
Memory Outcome in Prodromal and Mild Dementia with Lewy Bodies and Alzheimer’s Disease: A Longitudinal Study
Abstract
Background:
Dementia with Lewy bodies (DLB) and Alzheimer’s disease (AD) are likely to induce memory impairments from the prodromal stage but, to our knowledge, no longitudinal study of these patients’ memory profile has been conducted to date.
Objective:
The aim of our study was to describe the characteristics and the evolution of the long-term memory profile of patients with prodromal and mild DLB and AD.
Methods:
We collected verbal (RL/RI-16) and visual (DMS48) memory scores from 91 DLB patients, 28 AD patients, 15 patients with both conditions (DLB/AD), and 18 healthy control subjects at their inclusion visit and at 12, 24, and 48 months.
Results:
On the RL/RI-16, DLB patients performed better than AD patients in terms of total recall (p < 0.001), delayed total recall (p < 0.001), recognition (p = 0.031), and loss of information over time (p = 0.023). On the DMS48, differences between these two groups were not significant (p > 0.05). Longitudinally, the memory performance of DLB patients was stable over 48 months, unlike that of AD patients.
Conclusion:
Four indicators were relevant to distinguish between DLB and AD patients in terms of memory performance: DLB patients benefitted greatly from semantic cueing, their recognition and consolidation abilities were well-preserved, and both their verbal and visual memory performance remained remarkably stable over four years. However, no performance differences between DLB and AD patients were found regarding visual memory, either qualitatively (memory profile) or quantitatively (severity of impairment), indicating the lesser relevance of this test in distinguishing between these two diseases.
INTRODUCTION
Dementia with Lewy bodies (DLB) is the second most common form of neurodegenerative disease after Alzheimer’s disease (AD). DLB is one of the synucleinopathies, diseases which are characterized by the diffuse aggregation of abnormal α-synuclein, forming Lewy bodies. According to the revised DLB consensus criteria [1], a diagnosis of probable DLB can be made if two or more of the following manifestations are present: fluctuating cognition with pronounced variations in attention and alertness, recurrent visual hallucinations, spontaneous parkinsonian features, and rapid eye movement sleep behavior disorder (RBD). McKeith and colleagues [2] also developed criteria for prodromal DLB, including a mild cognitive impairment (MCI), a delirium-onset or a psychiatric-onset presentation. It should be noted that the presence of visual hallucinations and/or cognitive fluctuations is reported to be associated with an increased risk of transition from MCI to dementia [3].
From the prodromal stage of the disease, DLB patients also experience a cognitive decline, and especially deficits in executive and attentional functions [4–6], cognitive processing speed [5–8] as well as visuo-constructive and visuo-spatial abilities [7]. This cognitive decline worsens in the dementia stage, with greater executive, attentional, visuo-spatial, and visuo-perceptual difficulties [9–11]. As the disease progresses, memory impairment also usually appears [1]. Decreased performances on both DMS48 sets have been highlighted in patients with prodromal DLB [7], and significant impairments in visual recognition memory have also been demonstrated in the dementia stage of the disease [12]. Regarding verbal memory, patients rather experience, from the prodromal stage, dysfunction of retrieval strategies (accessing the information when needed), with pathological performances in free recall [7, 13], but a significant benefit from semantic cueing compared to AD patients [14]. This indicates executive rather than memory deficits. As a reminder, free recall consists in freely recalling words from a previously learned list, while semantic cueing consists in giving semantic cues to help the patient remember words not freely recalled. Besides, DLB patients also tend to perform better in verbal memory tests than in visual memory tests [15]. One must nevertheless bear in mind that a small percentage of patients seem to be genuinely impaired in verbal memorystorage [7].
AD, on the other hand, is the memory disease par excellence. Biologically, AD is characterized by an extraneuronal accumulation of amyloid-β protein (Aβ42) and an intraneuronal accumulation of phosphorylated tau protein (P-tau) leading to neurofibrillary degeneration. According to the National Institute on Aging – Alzheimer’s Association (NIA-AA) diagnostic criteria [16], the typical clinical presentation is characterized by an insidious and progressive onset with episodic memory impairments. These disorders are well described in the literature. Typically, AD patients present a so-called “hippocampal” memory profile, characterized by deficits in encoding, storing, and consolidating information in both verbal and visual modalities [17], although patients often show better performance in visual memory, at least in the prodromal stage [18]. These memory disorders are characteristic of AD [19] and have been associated many times with hippocampal damage [20–22]. However, it should be noted that memory disorders are likely to begin several years before diagnostic criteria are met and before hippocampal atrophy appears onMRI [23].
Although the symptoms and biological markers of DLB and AD have been relatively well identified, distinguishing DLB from AD remains difficult because of overlapping clinical and neuro-pathological features between the two conditions. In practice, two-thirds of patients with DLB would be misdiagnosed or not diagnosed at all [24]. Moreover, the co-occurrence of AD and DLB is frequent and complicates the diagnosis and management of the patient as well as the identification of each disease’s specific clinical signs. Consequently, it appears crucial to differentiate between DLB and AD in the early stages by means of appropriate clinical tools, since the diagnosis determines patients’ care.
Although several studies have already demonstrated memory deficits in patients with DLB and AD, to our knowledge, no study has provided an in-depth analysis of the memory profile and its evolution in DLB patients compared to AD patients. Therefore, the aim of the present study was to specify the characteristics and the evolution of these patients’ memory profile, in order to clarify the differential diagnosis between the two pathologies. On the one hand, we analyzed the patients’ memory profiles at their first visit, and on the other hand, we assessed the evolution of their verbal and visual memory scores over 48 months. DLB patients’ memory profiles were compared to those of AD patients, patients with both diseases (DLB/AD) and healthy control subjects (HCS).
In view of the existing literature data, we assumed that DLB patients show verbal memory retrieval impairments and deficits in visual recognition memory, both of which tend to worsen as the disease progresses, in line with the increase of executive, attentional, and neuro-visual disorders. Furthermore, we expected to find a bilateral hippocampal syndrome in AD patients that worsened with disease progression, as suggested in the literature. Finally, we hypothesized that patients with DLB/AD would have a mixed and more variable memory profile, worsening rapidly and progressing more clearly to a hippocampal syndrome.
METHODS
Study population
Ninety-one DLB patients, 28 AD patients, 15 DLB/AD patients, and 18 healthy control subjects (HCS), participating in two larger cohort studies (AlphaLewyMA, N° HUS: 5330; N°IDRCB: 2012-A00992-412020-2021; and MCL Visuoconstruction, N° HUS N°5565; N° IDRCB: 2013-A00554-41) were enrolled in the study. Patients and HCS were recruited from the tertiary memory clinic of Strasbourg University Hospital, France, including the geriatrics and neurology departments. All gave informed consent for their participation in this study. They were followed for 48 months, with annual clinical examinations, including complete neuropsychological assessments, evaluating memory, executive, attentional and instrumental functions (language, visuoperceptive, visuospatial, and visuoconstructive functions). Fluctuations were measured using the Mayo Clinic Fluctuations scale [25] and hallucinations using the Parkinson’s disease-associated psychotic symptoms questionnaire [26]. Features of parkinsonism were assessed with the Unified Parkinson’s Disease Rating Scale (UPDRS, part 3) [27]: akinesia, rigidity, and tremor at rest (rated from 0 for no symptoms to 4 for serious symptoms). RBD was evaluated using a sleep questionnaire on RBD from the publication by Gjerstad et al. [28], simplified into four questions for the patient and the caregiver: one concerning movements during sleep and the other concerning vivid dreams and nightmares.
Regarding inclusion criteria, the DLB group met the revised DLB consensus criteria for prodromal DLB [2] or probable DLB [1], the AD group met the Dubois criteria [29] and the DLB/AD group met both sets of disease criteria [1, 2, 29]. We also included cerebrospinal fluid (CSF) biomarker analyses to verify the presence of AD biomarkers and to clarify the characteristics of each group. Only patients in the prodromal/MCI or mild stages of the disease were selected. As a reminder, “prodromal stage” is defined as the presence of a cognitive decline that does not lead to a functional impact on the patient’s daily life (according to the DSM5). We operationalized this aspect by means of four questions concerning patient autonomy (Instrumental Activities of Daily Living (IADL) score). Patients who had difficulties in at least one of the following dimensions: medication, finances, telephone and transportation, were considered to have dementia. Patients who had no difficulties in these dimensions were considered to be at the prodromal stage. Additionally, we selected only patients with a Mini-Mental State Examination (MMSE) [30] score≥20. This is the cut-off used to differentiate between patients with mild dementia (MMSE score≥20) and those with moderate dementia (MMSE score < 20). Please note that of the 91 DLB patients, 60 patients were in the prodromal stage and 31 were in the mild dementia stage. Of the 28 AD patients, 22 were in the prodromal stage and 6 were in the mild dementia stage. Of the 15 DLB/AD patients, 8 were in the prodromal stage and 7 were in the mild dementia stage. There was no significant difference in the proportion of prodromal/dementia patients in these three groups (χ2 = 3.016, p = 0.221). Evidently, none of our control subjects showed any alteration in terms of autonomy.
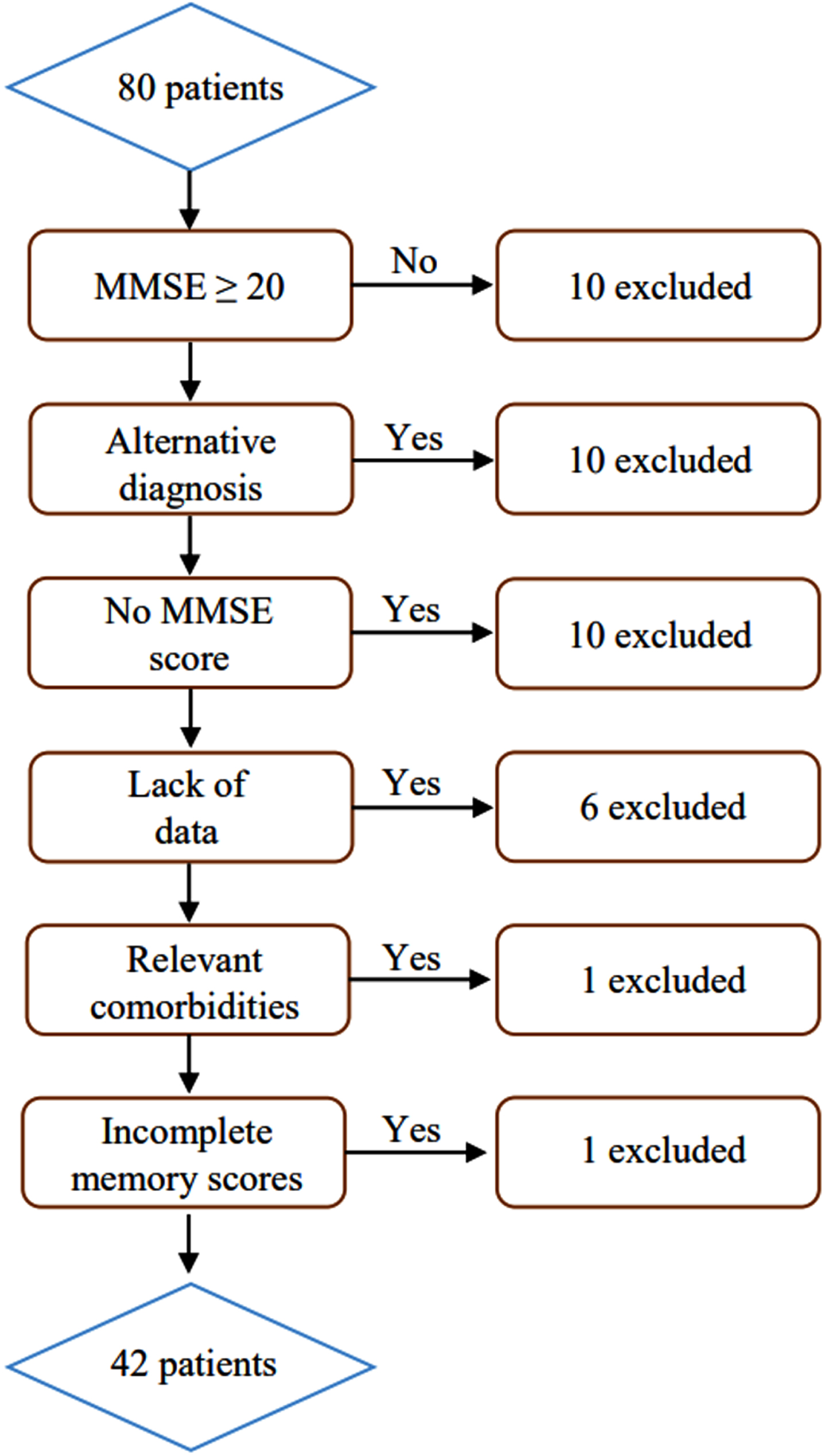
Initial exclusion criteria for all participants included in the two cohorts were as follows: contraindication to MRI; history of alcohol/substance abuse; sensory or motor deficits; relevant neurological or psychiatric comorbidities or the presence of other severe or unstable medical illnesses. In addition, some participants had to be excluded from the analyses due to a lack of data or because of the emergence of comorbidities that have an impact on memory abilities (see flowcharts in Figs. 1 and 2). A total of 130 subjects were included from the AlphaLewyMA cohort and 42 patients from the MCL Visuoconstruction cohort, of whom 20 were included in both cohorts.
Fig. 1
Inclusion of DLB, AD, and DLB/AD patients and HCS from the AlphaLewyMA cohort.
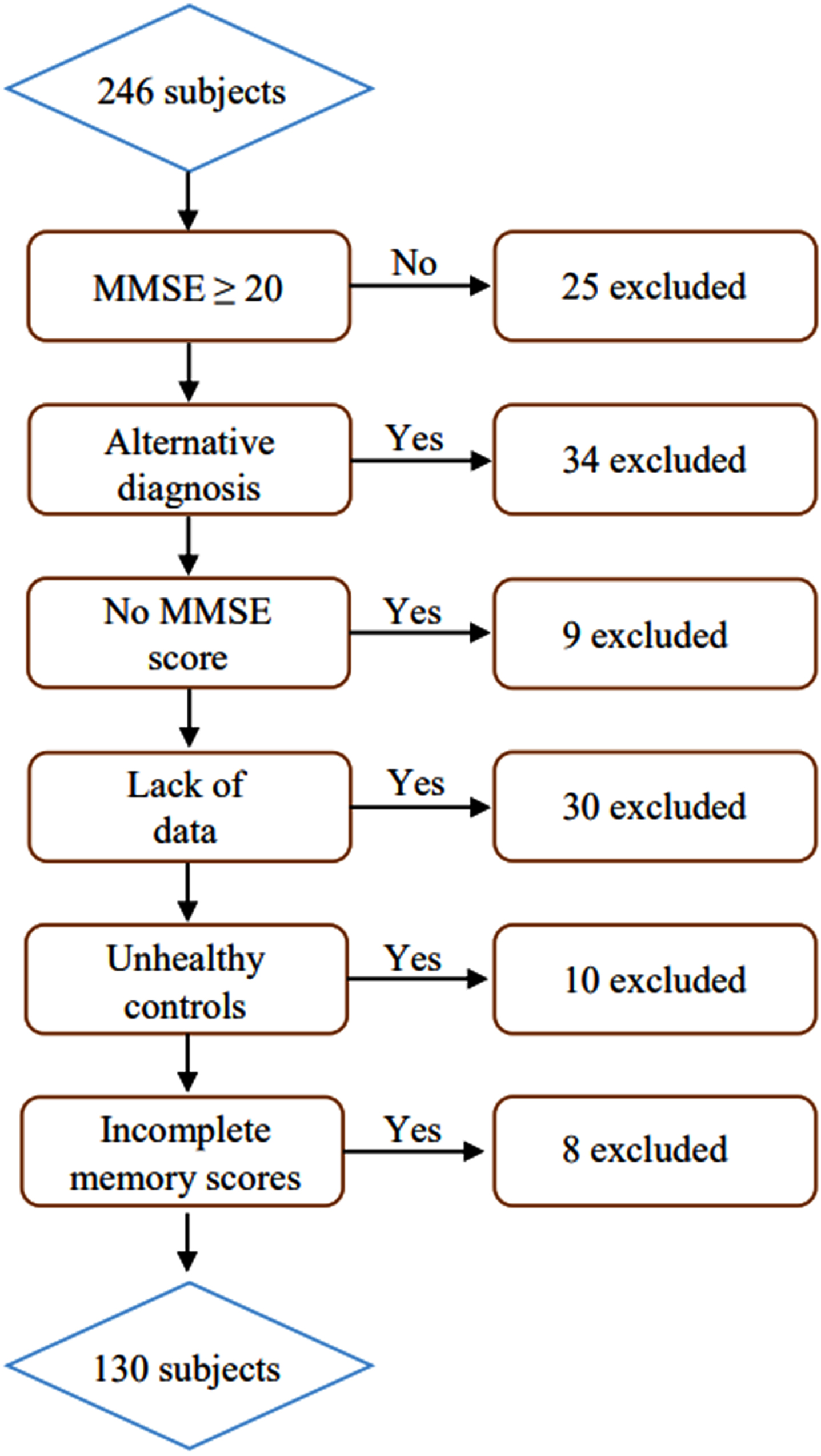
Fig. 2
Inclusion of DLB, AD, and DLB/AD patients from MCL Visuoconstruction cohort.
Cerebrospinal fluid analyses
Some of our patients underwent a lumbar puncture, in order to collect and analyze the CSF and evaluate the presence or absence of biomarkers indicative of AD (AD biomarkers). Each CSF sample was transported to the laboratory within 4 h after collection. Samples were then homogenized on receipt, centrifuged at 1700 g for 10 min at room temperature, transferred to 0.5-ml polypropylene tubes and stored at -80°C until analysis. As a second step, CSF T-tau (total tau), Aβ42 and P-tau concentrations were measured by sandwich enzyme-linked immunosorbent assay (ELISA) using commercially available kits (INNOTEST; Fujirebio Europe, Ghent, Belgium). All assays were performed according to the manufacturer’s instructions, and the methodology did not change during the period in which the analyses were performed. Please note that CSF biomarker measurements were run as clinical routine analyses by technicians at the biochemistry laboratory of University Hospital of Strasbourg. In the present study, patients were considered to have Alzheimer neuropathology if their CSF biomarker analysis showed the following results: decreased Aβ42 <700 ng/l plus increased p-Tau (>60 ng/l) and T-tau (>500 ng/l).
Mean CSF biomarker values are presented in Table 1. CSF T-tau, Aβ42, and P-tau values were available for 57% of DLB patients, 68% of AD patients, and 87% of DLB/AD patients. Table 1 highlights significant differences between the groups in terms of CSF biomarker values. DLB patients showed significantly lower levels of CSF T-tau and P-tau than AD and DLB/AD patients (p < 0.001), but also significantly higher levels of CSF Aβ42 (DLB > AD, p < 0.001; DLB > DLB/AD, p = 0.002) (Table 2). No significant differences in T-tau, Aβ42, and P-tau levels were found between AD and DLB/AD patients. Furthermore, according to our criteria, T-tau, Aβ42 and P-tau mean values were pathological in AD and DLB/AD patients, but not in DLB patients.
Table 1
Mean CSF biomarker values for DLB, AD, and DLB/AD patients
| Group | |||||
| Biomarker | DLB (n = 91) | AD (n = 28) | DLB/AD (n = 15) | Statistic test, p | Dunn post-hoc test |
| CSF T-tau | 276.35 (100.11) a | 635.11 (297.79) b | 652.85 (245.42) c | H=41.868, p < 0.001* | DLB<AD; DLB < DLB/AD |
| CSF Aβ42 | 908.8 (304.44) a | 609.68 (172) b | 641.92 (258.5) c | H=18.659, p < 0.001* | DLB>AD; DLB > DLB/AD |
| CSF P-tau | 43.33 (13.09) a | 88.11 (35.12) b | 91.23 (32.64) c | H= 46.609, p < 0.001* | DLB<AD; DLB < DLB/AD |
CSF, cerebrospinal fluid; T-tau, total tau; Aβ42, amyloid-β 42; P-tau, phosphorylated tau; AD, Alzheimer’s disease; DLB, dementia with Lewy bodies. Significant p values (p < 0.05) are in boldface type. Values are mean (SD). aData missing for 39 patients. bData missing for 9 patients. cData missing for 2 patients.
Table 2
Demographic and clinical characteristics of patients and control subjects
| Group | ||||||
| Characteristics | DLB | AD | DLB/AD | HCS | Statistic test, p | Dunn Post-hoc test |
| (n = 91) | (n = 28) | (n = 15) | (n = 18) | |||
| Agea | 71.2 (9.38) | 74.95 (7.3) | 71.87 (7.67) | 67.78 (7.79) | F = 2.609, p = 0.054 | |
| Gender (M/F) | 32/59 | 13/15 | 7/8 | 9/9 | χ2 = 2.393, p = 0.495 | |
| Laterality (R/L) | 82/9 | 26/2 | 15/0 | 18/0 | χ2 = 3.787, p = 0.705 | |
| EL (y)a | 11.97 (4.02) | 12.5 (3.78) | 10.33 (2.55) | 13.67 (2.38) | F = 2.36, p = 0.074 | |
| Stage of disease (pro/dem) | 60/31 | 22/6 | 8/7 | χ2 = 3.016, p = 0.221 | ||
| MMSE score a | 26.19 (2.96) | 25.32 (2.61) | 25.00 (2.65) | 28.83 (1.04) | H = 25.795, p < 0.001* | HCS>DLB, AD, DLB/AD |
| Hallucinations (/9) a,b | 1.76 (1.86) | 0.15 (0.36) | 0.53 (0.74) | 0.25 (0.34) | H = 41.465, p < 0.001* | DLB>AD, DLB/AD, HCS |
| Fluctuationsc,j | 8/24/24/24/10g | 17/4/3/1/0f | 4/7/0/2/1g | 12/4/1/0/0g | H = 49.521, p < 0.001* | DLB>AD, DLB/AD, HCS DLB/AD>AD, HCS |
| Akinesiad,j | 33/46/7/2/0f | 24/1/0/0/0f | 10/3/1/0/0g | 17/1/0/0/0 | H = 39.195, p < 0.001* | DLB>AD, DLB/AD, HCS |
| Rigidityd,j | 33/50/5/0/0f | 21/4/0/0/0f | 7/6/1/0/0g | 17/1/0/0/0 | H = 30.084, p < 0.001* | DLB>AD, HCS DLB/AD>AD, HCS |
| Tremord,i,j | 79/9/0/0/0 | 22/1/0/0/0 | 13/1/0/0/0 | 18/0/0/0/0 | H = 0.679, p = 0.712 | |
| RBDe,k | 32/20/28h | 21/3/1f | 9/1/4g | 12/5/1 | H = 18.537, p < 0.001* | DLB>AD, HCS |
AD, Alzheimer’s disease; DLB, dementia with Lewy bodies; HCS, healthy control subjects; EL, educational level; pro, prodromal stage; dem, mild dementia stage; MMSE, Mini-Mental State Examination; RBD, rapid eye movement behavior disorder. Significant p values (p < 0.05) are in boldface type. aValues are mean (SD). bAccording to [26]. cAccording to [25]. dAccording to [27]. eAccording to [28]. fData missing for 3 patients. gData missing for 1 patient. hData missing for 11 patients. iHCS group not included in the analysis (variance equal to 0). jrating 0/1/2/3/4 (proportion of patients for each score). krating 0/1/2 (proportion of patients for each score).
Behavioral study
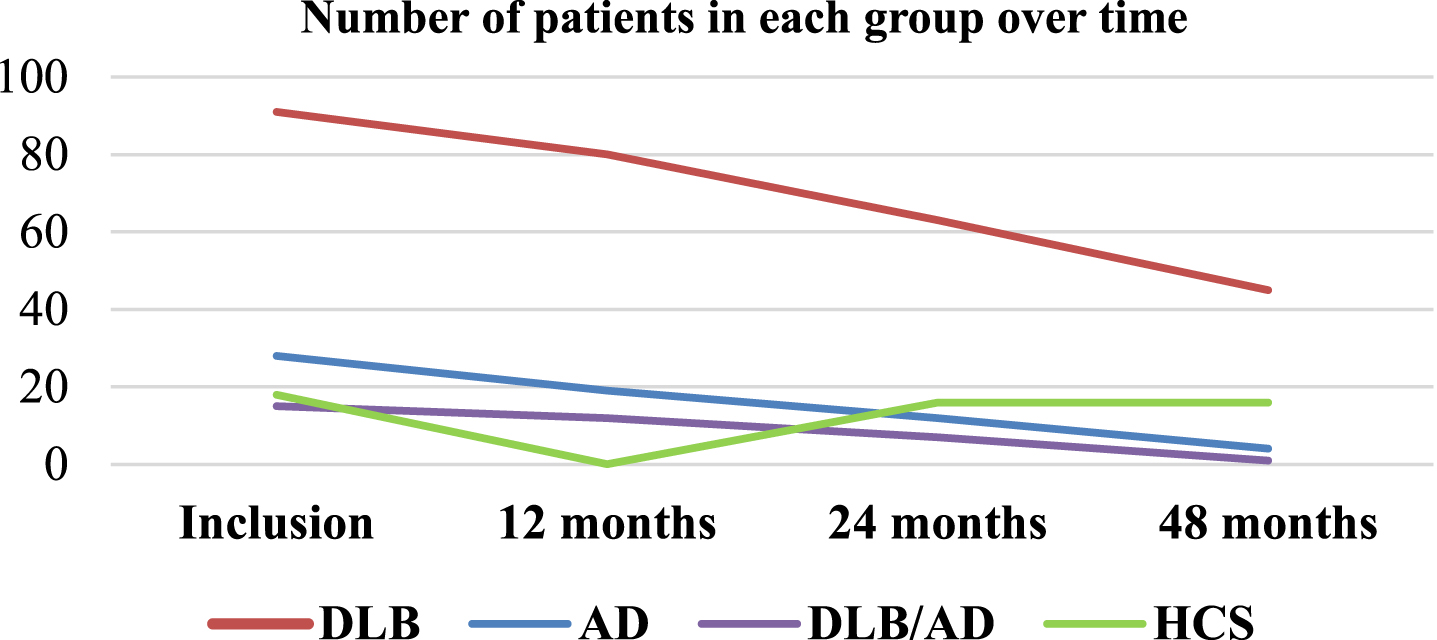
Patients’ memory performance on RL/RI-16 and DMS48 was collected at their inclusion visit and at 12 months, 24 months, and 48 months. However, there was a significant loss of data as the visits progressed, especially for AD and DLB/AD patients (Fig. 3).
Fig. 3
Number of patients in each group over time.
The RL/RI-16 (Rappel Libre/Rappel Indicé à 16 items) test [31], a French verbal episodic memory test similar to the FCSRT [32], consists in memorizing 16 words of different semantic categories. It allows a clear distinction between encoding, storage, and retrieval processes. During the immediate recall stage, the 16 words are presented to the participants, and they must associate each word with a category cue. An immediate recall score (IR: 0 to 16 points) is collected. Participants are then asked to recall the 16 words on three successive trials, each with a free recall and a cued recall for the words that were not spontaneously recalled. In this way, we obtain a total free recall score (TFR: 0 to 48 points) and a total recall score (TR: 0 to 48 points) corresponding respectively to the sum of the words recalled without cues and those recalled with cues. Following this phase, participants perform a recognition task, which consists in recognizing the 16 words of the initial list among 32 distractors. A recognition score (RS: 0 to 16 points) is noted. Twenty minutes later, delayed recalls are performed following the same procedure as for the first recalls. A delayed free recall score (DFR: 0 to 16 points) and a delayed total recall score (DTR: 0 to 16 points) are collected as well as a loss of information score (LIS = DTR - TR3) counting the number of items forgotten between the third total recall and the delayed total recall.
The test highlights a retrieval disorder if one or more free recalls are deficient but normalized with semantic cueing. There is a storage disorder if one or more total recalls are deficient, and the patient receives little or no help from cueing. Using the norms of Van der Linden et al. [31] which are widely used in current clinical practice, we compared each patient’s scores to those of a representative population (in terms of age and sociocultural level) in order to determine whether they were normal or deficient. In this way, we were able to obtain a detailed analysis of the memory profiles of our patients.
The DMS48 (Delayed Matching to Sample 48 items) test [33] is a visual recognition memory task evaluating visual encoding and storage abilities. Its procedure first includes an implicit encoding phase where subjects are asked to say whether they distinguish more or fewer than three colors on 48 consecutive target items. After this phase, an immediate and a 1-hour delayed recognition trial are performed with two different sets of distractors (Set 1 and Set 2). Two recognition scores are accordingly obtained, corresponding to Set 1 (0 to 48 points) and Set 2 (0 to 48 points). The test reveals an encoding disorder if only Set 1 is deficient, and a storage disorder if Set 2 is deficient. The loss of information (LIS) between Set 1 and Set 2 (Set 2 - Set 1) is also analyzed in order to assess consolidation abilities in visual memory. We chose to use the norms of the DMS48 authors [33], which offer several age categories and are very often used in clinical practice.
Statistical analyses
All statistical analyses were performed using JASP software (https://jasp-stats.org).
An ANOVA was used for age and educational level (EL) variables, as they were normally distributed. We used non-parametric Kruskal-Wallis tests and Dunn post-hoc tests for MMSE score, hallucinations, fluctuations, akinesia, rigidity, tremor, and RBD comparisons as well as for CSF biomarker analyses (T-tau, Aβ42, and P-tau). For categorical measures (gender and laterality), χ2 tests were applied.
In addition, ANOVA analyses and Tukey’s post-hoc tests were used to compare intergroup differences (DLB, AD, DLB/AD, and HCS) in terms of memory performance, based on the raw scores at inclusion (IR, TFR, TR, DFR, DTR, RS, and LIS on the RL/RI-16 test; Set 1, Set 2, and LIS on the DMS48 test). Effect sizes were calculated using eta squared (η2) for significant main effects. Longitudinal statistical analyses were performed to compare the raw scores at inclusion, at 12 months, at 24 months, and at 48 months (IR, TFR, TR, DFR, DTR, and LIS on the RL/RI-16 test; Set 1, Set 2, and LIS on the DMS48 test). For this purpose, repeated measures ANOVAs were performed, while non-parametric Friedman tests were applied for variables not following a normal distribution, in which case post-hoc tests were subsequently performed using the Holm method. Note that only data from patients with memory scores at 48 months were used here (DLB: n = 45; HCS: n = 16). A threshold of p < 0.05 was used to determine statistical significance.
RESULTS
Demographic and clinical characteristics
Table 2 presents the demographic and clinical characteristics of DLB, AD, and DLB/AD patients and healthy control subjects (HCS). Our four groups were matched in terms of age (p = 0.054), gender (p = 0.495), laterality (p = 0.705), and education level (p = 0.074). Concerning MMSE scores, all three patient groups had significantly lower mean MMSE scores than controls (p < 0.001). The mean MMSE score did not differ between the three groups of patients (p > 0.05).
Finally, regarding clinical symptoms, DLB patients presented significantly higher scores for fluctuations, hallucinations, akinesia, and rigidity compared to AD patients and HCS (p < 0.001). Similarly, we noted that the presence of RBD was significantly higher in DLB patients compared to AD patients (p < 0.001) and HCS (p = 0.007). Furthermore, DLB/AD patients presented more fluctuations than AD patients (p = 0.042) and HCS (p = 0.024) as well as higher levels of rigidity than AD patients (p = 0.017) and HCS (p = 0.006).
Verbal memory (RL/RI-16)
Memory profiles: inclusion visit
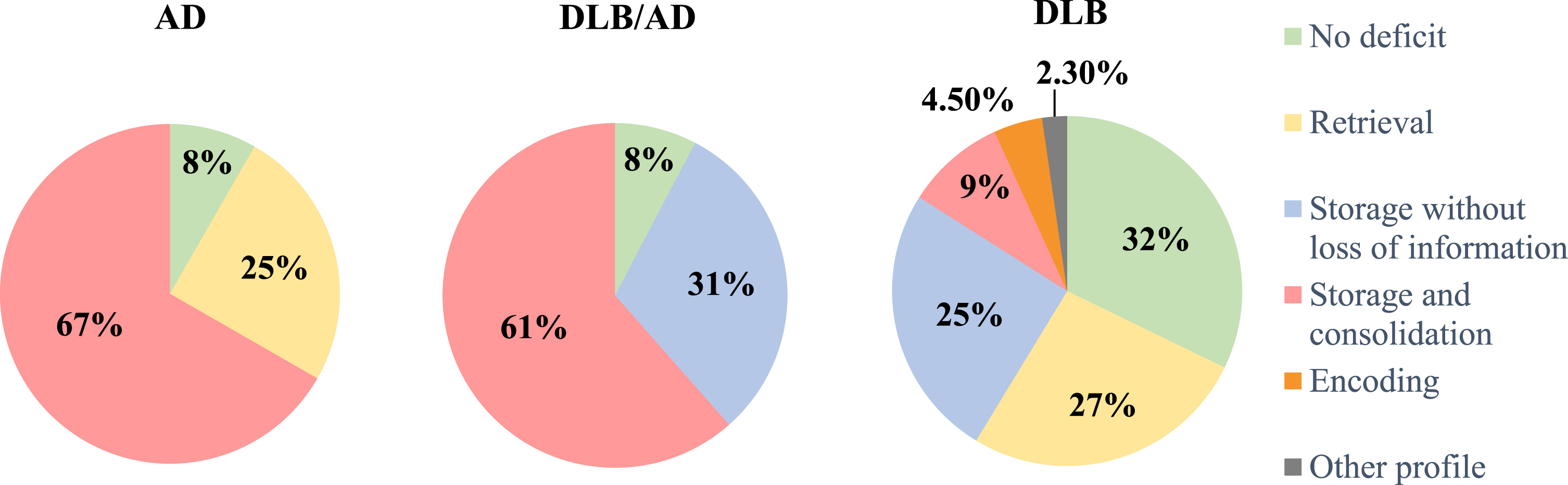
Of the 87 DLB patients with data at their inclusion visit, 32.2% showed no verbal anterograde memory deficit according to our standards. On the other hand, 26.5% of the patients showed a retrieval impairment, 25.3% a storage disorder without a loss of information over time, 9.2% a storage and consolidation disorder with a loss of information over time, 4.5% an isolated encoding disorder, and 2.3% had a single total recall deficit with no real storage disorder (see Fig. 4). Most of the AD patients showed a storage and consolidation disorder with a clear loss of information over time (66.7% of the 24 patients with data), 25% had a retrieval impairment and only 8.3% of patients had no deficit (see Fig. 4). Finally, our results indicated that almost all patients suffering from both pathologies (DLB/AD) had a storage disorder (92.3% of the 13 patients with data) with two-thirds of them losing information between the third total recall and the delayed total recall. Only 7.7% had no deficits (see Fig. 4).
Fig. 4
RL/RI-16 memory profiles of the three groups of patients at the inclusion visit. Retrieval disorder: one or more free recalls are deficient but normalized with semantic cueing Storage disorder: one or more total recalls are deficient, and the patient receives little or no help from cueing Consolidation disorder: loss of information between the third total recall and the delayed total recall Encoding disorder: immediate recall score is deficient.
Comparison of scores: inclusion visit
Immediate recall score (IR): behavioral statistical analyses at the inclusion visit (Tables 3 and 4) revealed that IR performance on the RL/RI-16 test differed between groups (p < 0.001). AD patients (p < 0.001), DLB patients (p = 0.029), and DLB/AD patients (p = 0.002) performed worse than HCS, but there was no significant difference between patient groups (p > 0.05).
Table 3
Mean RL/RI-16 test scores of the three groups of patients and control subjects
| Group | |||||
| AD (n = 28) | DLB/AD (n = 15) | DLB (n = 91) | HCS (n = 18) | Statistic test, p, η2 | |
| IR | 14.17 (1.71) | 14 (1.83) | 14.85 (1.42) | 15.89 (0.32) | F = 6.438, p < 0.001*, η2=0.123 |
| TFR | 13.5 (7.58) | 12.85 (7.2) | 20.55 (8.6) | 28.83 (5.7) | F = 16.251, p < 0.001*, η2=0.26 |
| TR | 33.04 (11.3) | 32.46 (8.1) | 41.01 (7.98) | 46.17 (3.3) | F = 12.964, p < 0.001*, η2=0.219 |
| DFR | 4.58 (4) | 4.15 (4.16) | 7.88 (4.04) | 12.17 (1.58) | F = 17.199, p < 0.001*, η2=0.274 |
| DTR | 10.58 (4.64) | 10.85 (3.18) | 14.41 (2.16) | 15.83 (0.38) | F = 20.825, p < 0.001*, η2=0.313 |
| LIS | -0.92 (1.79) | -0.92 (1.98) | 0 (1.26) | -0.11 (0.47) | F = 3.944, p = 0.010*, η2=0.079 |
| RS | 14.45 (1.79) | 15.18 (0.87) | 15.35 (1.31) | 15.81 (0.4) | F = 3.722, p = 0.013*, η2=0.084 |
RL/RI-16, Rappel Libre/Rappel Indicé à 16 items; AD, Alzheimer’s disease; DLB, dementia with Lewy bodies; HCS, healthy control subjects; IR, immediate recall; TFR, total free recall; TR, total recall; DFR, delayed free recall; DTR, delayed total recall; LIS, loss of information score; RS, recognition score. Significant p values (p < 0.05) are in boldface type. Values are mean (SD). Effect sizes were calculated using eta squared (η2) for significant main effects.
Table 4
Tukey post-hoc tests – mean RL/RI-16 test scores of the three groups of patients and healthy control subjects
| Group | |||||||
| DLB versus HCS | AD versus HCS | DLB/AD versus HCS | DLB versus AD | DLB versus DLB/AD | AD versus DLB/AD | ||
| IR | t=-2.804, p = 0.029* | t=-3.863, p < 0.001* | t=-3.629, p = 0.002* | t=-2.074, p = 0.167 | t=-2.0, p = 0.193 | t=0.338, p = 0.987 | |
| TFR | t=-4.019, p < 0.001* | t=-6.169, p < 0.001* | t=-5.51, p < 0.001* | t=-3.838, p = 0.001* | t=-3.251, p = 0.008* | t=0.238, p = 0.995 | |
| TR | t=-2.416, p = 0.079 | t=-5.104, p < 0.001* | t=-4.565, p < 0.001* | t=-4.196, p < 0.001* | t=-3.489, p = 0.004* | t=0.204, p = 0.997 | |
| DFR | t=-4.322, p < 0.001* | t=-6.361, p < 0.001* | t=-5.758, p < 0.001* | t=-3.739, p = 0.002* | t=-3.278, p = 0.007* | t=0.326, p = 0.988 | |
| DTR | t=-2.022, p = 0.185 | t=-6.187, p < 0.001* | t=-5.034, p < 0.001* | t=-6.086, p < 0.001* | t=-4.397, p < 0.001* | t=-0.28, p = 0.992 | |
| LIS | t=0.312, p = 0.989 | t=-1.88, p = 0.241 | t=-1.624, p = 0.369 | t=-2.893, p = 0.023* | t=-2.259, p = 0.113 | t=0.014, p = 1.000 | |
| RS | t=-1.289, p = 0.572 | t=-3.133, p = 0.011* | t=-1.242, p = 0.602 | t=-2.787, p = 0.031* | t=-0.414, p = 0.976 | t=-1.504, p = 0.439 | |
RL/RI-16, Rappel Libre/Rappel Indicé à 16 items; AD, Alzheimer’s disease; DLB, dementia with Lewy bodies; HCS, healthy control subjects; IR, immediate recall; TFR, total free recall; TR, total recall; DFR, delayed free recall; DTR, delayed total recall; LIS, loss of information score; RS, recognition score. Significant p values (p < 0.05) are in boldface type.
Total free recall score (TFR): significant differences were found between groups for TFR (p < 0.001). The AD group (p < 0.001), the DLB group (p < 0.001), and the DLB/AD group (p < 0.001) performed significantly worse than the HCS group. However, our analyses indicated that DLB patients performed better than AD (p = 0.001) and DLB/AD patients (p = 0.008). No differences were found between AD patients and DLB/AD patients (p = 0.995).
Total recall score (TR): TR performance differed between groups (p < 0.001). AD (p < 0.001) and DLB/AD (p < 0.001) patients showed a lower performance than controls. In contrast, no significant differences in performance between DLB patients and controls were found (p = 0.079). DLB patients performed better than AD (p < 0.001) and DLB/AD patients (p = 0.004), but there was no difference between the latter two groups (p = 0.997).
Delayed free recall score (DFR): we found a significant intergroup difference in DFR (p < 0.001). Our analyses revealed significantly lower DFR scores in DLB (p < 0.001), AD (p < 0.001) and DLB/AD patients (p < 0.001) compared to controls. However, DLB patients’ performance was still higher than that of AD patients (p = 0.002) and DLB/AD patients (p = 0.007). We found no difference between the latter two groups (p = 0.988).
Delayed total recall score (DTR): DTR performance also differed between groups (p < 0.001). The performance of AD (p < 0.001) and DLB/AD patients (p < 0.001) was lower than that of HCS. In contrast, we found no significant difference between the performance of DLB patients and that of HCS (p = 0.185). Furthermore, DLB patients performed better than AD (p < 0.001) and DLB/AD patients (p < 0.001). No difference was found between the latter two groups (p = 0.992).
Loss of information over time: our results indicated a significant difference between groups regarding the loss of information between TR3 and DTR (p = 0.01) with less loss of information in DLB patients compared to AD patients (p = 0.023). We showed no other significant differences betweengroups.
Recognition score (RS): we found a significant difference between groups in terms of the recognition score (RS) (p = 0.013). Our analyses indicated significantly lower scores in AD patients, compared to DLB patients (p = 0.031) and HCS (p = 0.011). No other significant differences between groups were found.
Longitudinal analysis from the inclusion visit to the 48-month visit
Longitudinal statistical analyses comparing the evolution of memory scores across the inclusion and 12-, 24-, and 48-month visits (Table 5) showed no significant difference in DLB patients for IR (p = 0.741), TFR (p = 0.543), TR (p = 0.238), DFR (p = 0.309), DTR (p = 0.763), and loss of information (p = 0.906).
Table 5
Evolution of the mean RL/RI-16 test scores in DLB patients (n = 45)
| Visit | |||||
| Inclusion | 12 months | 24 months | 48 months | Statistic test, p | |
| IR | 15.12 (1.31) | 15.02 (1.08) | 15.12 (1.19) | 15.05 (1.21) | F = 0.417, p = 0.741 |
| TFR | 23.16 (8.7) | 24.07 (7.87) | 22.76 (9.47) | 24.79 (8.01) | F = 0.719, p = 0.543 |
| TR | 41.98 (6.8) | 42.4 (5.75) | 42.74 (5.2) | 43.41 (4.36) | χ2 = 4.229, p = 0.238 |
| DFR | 8.93 (4.04) | 9.52 (4.00) | 8.93 (3.94) | 8.85 (4.00) | F = 1.213, p = 0.309 |
| DTR | 14.64 (2.18) | 14.86 (1.76) | 14.33 (2.63) | 14.95 (1.62) | χ2 = 1.160, p = 0.763 |
| LIS | 0.05 (1.29) | 0.02 (0.86) | -0.4 (1.52) | -0.13 (1.13) | F = 0.186, p = 0.906 |
RL/RI-16, Rappel Libre/Rappel Indicé à 16 items; IR, immediate recall; TFR, total free recall; TR, total recall; DFR, delayed free recall; DTR, delayed total recall; LIS, loss of information score. Values are mean (SD).
However, our results indicated a significant decrease in DTR score between the inclusion and 48-month visits in HCS (p = 0.039) (Table 6), but no significant difference for IR (p = 0.554), TFR (p = 0.189), TR (p = 0.895), DFR (p = 0.650), and loss of information (p = 0.135).
Table 6
Evolution of the mean RL/RI-16 scores in healthy control subjects (n = 16)
| Visit | ||||
| Inclusion | 24 months | 48 months | Statistic test, p | |
| IR | 15.88 (0.34) | 15.63 (0.81) | 15.56 (1.09) | F = 0.602, p = 0.554 |
| TFR | 28.81 (5.31) | 30.38 (3.14) | 31.13 (4.13) | F = 1.761, p = 0.189 |
| TR | 46.63 (2.53) | 46.38 (2.00) | 46.69 (2.12) | F = 0.111, p = 0.895 |
| DFR | 12.25 (1.65) | 12.19 (1.52) | 12.63 (1.45) | F = 0.437, p = 0.650 |
| DTR | 15.94 (0.25) | 15.88 (0.34) | 15.63 (0.81) | χ2 = 6.5, p = 0.039* |
| LIS | 0.00 (0.37) | -0.13 (0.34) | -0.25 (0.58) | F = 2.143, p = 0.135 |
RL/RI-16, Rappel Libre/Rappel Indicé à 16 items; IR, immediate recall; TFR, total free recall; TR, total recall; DFR, delayed free recall; DTR, delayed total recall; LIS, loss of information score. Significant p values (p < 0.05) are in boldface type. Values are mean (SD).
Concerning AD and DLB/AD patients, the RL/RI-16 test was no longer feasible for 57% of AD patients and 67% of DLB/AD patients at 12 months; for 79% of AD patients and 80% of DLB/AD patients at 24 months; and for 100% of AD patients and 93% of DLB/AD patients at 48 months (see Fig. 3). We were unable to carry out statistical analyses for these two groups, which were already too impaired in terms of memory.
Visual memory (DMS48)
Memory profiles: inclusion visit
At the inclusion visit, out of the 86 DLB patients with data, 46.5% showed no visual recognition memory deficit according to our standards. On the other hand, 29% of DLB patients showed a storage disorder with a loss of information between Set 1 and Set 2 (Set 1 > Set 2) and 44% of them had an associated encoding disorder; 15.2% of DLB patients had an encoding and storage disorder with no loss of information over time and 9.3% had an isolated encoding disorder (Set 1) (see Fig. 5).
Half of the 24 AD patients for whom data were available had an encoding and storage disorder, with more than half (57%) of them showing a loss of information between the two sets. On the other hand, 43% showed no deficit and 7% had an isolated encoding deficit in Set 1 with a normalization of performance in Set 2 (see Fig. 5).
Fig. 5
DMS48 memory profiles of the three groups of patients at the inclusion visit. Encoding disorder: Set 1 is deficient but Set 2 is within the norms Storage disorder: Set 2 is deficient Loss of information/consolidation disorder: loss of information between Set 1 and Set 2.
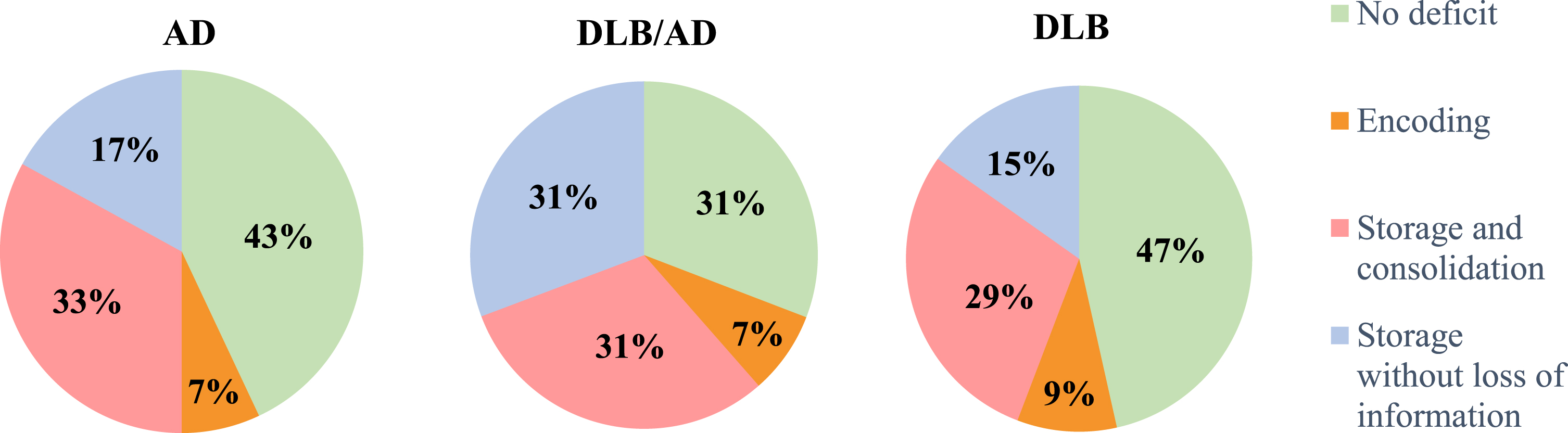
In patients with both pathologies (DLB/AD), 61.5% of the 13 patients with data showed an encoding and storage disorder, half of them with a loss of information between Set 1 and Set 2. On the other hand, 30.8% of the patients had no deficits and 7.7% of DLB/AD patients had an isolated encoding disorder (see Fig. 5).
Comparison of scores: inclusion visit
Set 1: statistical analyses at the inclusion visit (Tables 7 and 8) demonstrated a significant difference between groups at Set 1 of the DMS48 (p < 0.001). We found no difference between control subjects’ and DLB patients’ performance (p = 0.099), but AD (p < 0.001) and DLB/AD (p = 0.009) patients showed a significantly poorer performance than controls. DLB patients tended to perform better than AD patients (p = 0.051). However, no differences were found between the DLB and DLB/AD groups (p = 0.251) or between the AD and DLB/AD groups (p = 0.999).
Table 7
Mean DMS48 scores
| Group | |||||
| AD (n = 28) | DLB/AD (n = 15) | DLB (n = 91) | HCS (n = 18) | Statistic test, p, η2 | |
| Set 1 | 40.64 (6.05) | 40.87 (7.08) | 43.58 (5.09) | 46.72 (1.64) | F = 6.071, p < 0.001*, η2=0.111 |
| Set 2 | 40.04 (7.02) | 40.00 (5.45) | 43.00 (5.62) | 47.33 (0.69) | F = 7.384, p < 0.001*, η2=0.136 |
| LIS | –0.61 (3.27) | 0.15 (4.69) | -0.65 (2.73) | 0.61 (1.46) | F = 1.113, p = 0.346 |
DMS48, Delayed Matching to Sample 48 items; AD, Alzheimer’s disease; DLB, dementia with Lewy bodies; HCS, healthy control subjects; LIS, loss of information score. Significant p values (p < 0.05) are in boldface type. Values are mean (SD). Effect sizes were calculated using eta squared (η2) for significant main effects.
Table 8
Tukey post-hoc tests – Mean DMS48 scores
| Group | ||||||
| DLB versus HCS | AD versus HCS | DLB/AD versus HCS | DLB versus AD | DLB versus DLB/AD | AD versus DLB/AD | |
| Set 1 | t=-2.316, p = 0.099 | t=-3.838, p < 0.001* | t=-3.195, p = 0.009* | t=-2.589, p = 0.051 | t=-1.857, p = 0.251 | t=-0.133, p = 0.999 |
| Set 2 | t=-3.001, p = 0.017* | t=-4.336, p < 0.001* | t=-3.616, p = 0.002* | t=-2.445, p = 0.073 | t=-1.809, p = 0.273 | t=0.019, p = 1.000 |
DMS48, Delayed Matching to Sample 48 items; AD, Alzheimer’s disease; DLB, dementia with Lewy bodies; HCS, healthy control subjects. Significant p values (p < 0.05) are in boldface type.
Set 2: On the DMS48 Set 2, our results indicated a difference between groups (p < 0.001). The performance of DLB (p = 0.017), AD (p < 0.001), and DLB/AD (p = 0.002) patients was lower compared to that of controls. On the other hand, DLB patients tended to perform better than AD patients, although the difference was not significant (p = 0.073). No differences were found between the DLB/AD and DLB groups (p = 0.273) or between the DLB/AD and AD groups (p = 1.000).
Loss of information: our analyses showed no significant difference between the groups regarding the loss of information between Set 1 and Set 2 at the DMS48 (p = 0.346).
Longitudinal analysis from the inclusion visit to the 48-month visit
Longitudinally, and similar to the results found for verbal memory, no difference in performance was found in DLB patients (Table 9) between the inclusion visit, the 12-month visit, the 24-month visit, and the 48-month visit for DMS48 Set 1 (p = 0.361), Set 2 (p = 0.565), and the loss of information between these two sets (p = 0.392).
Table 9
Evolution of the mean DMS48 test scores in DLB patients (n = 45)
| Visit | |||||
| Inclusion | 12 months | 24 months | 48 months | Statistic test, p | |
| Set 1 | 44.77 (4.06) | 44.7 (4.29) | 45.14 (3.34) | 44.75 (4.75) | χ2 = 3.208, p = 0.361 |
| Set 2 | 45.14 (4.15) | 44.11 (4.32) | 44.37 (4.63) | 44.57 (4.51) | χ2 = 2.038, p = 0.565 |
| LIS | 0.12 (2.11) | -0.59 (2.14) | -0.77 (2.94) | -0.4 (1.9) | F = 1.007, p = 0.392 |
DMS48, Delayed Matching to Sample 48 items; LIS, loss of information score. Values are mean (SD).
On the other hand, control subjects (Table 10) improved their performance in Set 1 over time (p = 0.015), but their performance declined in terms of loss of information (p = 0.035). Their performance in Set 2 remained stable over time (p = 0.645).
Table 10
Evolution of the mean DMS48 test scores in healthy control subjects (n = 16)
| Visit | ||||
| Inclusion | 24 months | 48 months | Statistic test, p | |
| Set 1 | 46.63 (1.71) | 47.06 (1.06) | 47.69 (0.6) | χ2 = 8.359 , p = 0.015* |
| Set 2 | 47.31 (0.7) | 47.06 (1.18) | 47.19 (1.17) | F = 0.446, p = 0.645 |
| LIS | 0.69 (1.54) | 0 (1.1) | -0.5 (1.1) | F = 3.767, p = 0.035* |
DMS48, Delayed Matching to Sample 48 items; LIS, loss of information score. Significant p values (p < 0.05) are in boldface type. Values are mean (SD).
Concerning AD and DLB/AD patients, the DMS48 test was no longer feasible for 32% of AD patients and 20% of DLB/AD patients at 12 months; for 57% of AD patients and 53% of DLB/AD patients at 24 months; and for 86% of AD patients and 93% of DLB/AD patients at 48 months (see Fig. 3). We therefore did not carry out statistical analyses due to the smaller number of patients in each group.
DISCUSSION
The aim of this study was to shed light on the memory profile of DLB, AD, and DLB/AD patients at a prodromal to mild stage (MMSE≥20) in the context of a longitudinal follow-up over 48 months. To our knowledge, this is the first study to use such an approach, and compare these patients’ memory profiles. For this purpose, we disposed of a unique cohort that enabled us to collect information on the verbal and visual memory performances of DLB, AD, and DLB/AD patients, and healthy control subjects at several intervals over 48 months.
We hypothesized that DLB patients would show impairments in verbal memory retrieval and deficits in visual recognition memory, both of which worsen with the disease progression. In addition, we expected to find a bilateral hippocampal syndrome in AD patients that would worsen with the progression of the disease. Finally, we hypothesized that DLB/AD patients would have a mixed and more variable memory profile, worsening rapidly and progressing more clearly towards a hippocampal syndrome.
Our hypotheses were partially confirmed. The memory profiles of DLB and AD patients were indeed different, in terms of deficits and evolution. However, DLB patients’ performances did not decline over time, contrary to what we had initially assumed.
CSF biomarkers
It should be noted that none of the DLB patients for whom CSF was available had associated AD and they therefore presented biologically pure DLB profiles. For these patients, T-tau, Aβ42, and P-tau values were indeed within the norm and were significantly different from those of AD and DLB/AD patients. On the contrary, our results confirm that most of our AD and DLB/AD patients had pathological CSF biomarkers (decreased Aβ42 and increased T-tau and P-tau).
Memory profiles
In terms of verbal memory, DLB patients showed a better memory performance than AD patients on all measures, in line with previous reports, both in the prodromal stage [6] and in the dementia stage [34, 35]. Although DLB patients’ performance remained inferior to that of controls in free recall (immediate and delayed), these patients showed a comparable performance to HCS in total recall (immediate and delayed), highlighting a substantial benefit of semantic cueing. Thus, DLB patients would present executive difficulties in retrieving information from memory rather than purely memory impairments, in accordance with the literature [7, 13, 14]. Nevertheless, it should be emphasized that a marked percentage of DLB patients (34.5%) showed several total recall deficits, indicating an insufficient benefit of cueing and a memory storage impairment. This result is in line with the results of a study by Kemp et al. [7], conducted on a smaller cohort of patients with prodromal DLB, in which 21.6% of patients had a storage disorder. Furthermore, a small number of our patients (2.3%) had a single total recall deficit, suggesting a potential impact of attentional fluctuations on memory abilities.
The majority of AD patients had impairments in the storage and consolidation of information in verbal memory (66.7%). The performance in terms of free recall and total recall was significantly lower than that of DLB patients and control subjects, indicating the lesser benefit from semantic cueing in normalizing TR performances. These results are in favor of defective hippocampal functioning, in line with a well-supported literature on the subject [23, 34, 36]. Furthermore, our study provides an interesting finding: the performance of patients with both diseases (DLB/AD) was statistically comparable to that of AD patients for all sub-scores of the RL/RI-16, suggesting a similar memory profile and hence a hippocampal syndrome.
Therefore, DLB, AD, and DLB/AD patients are more or less likely to develop verbal memory storage disorders from the prodromal stage. However, several indicators could help to distinguish between these conditions. First, DLB patients had better consolidation abilities (i.e., less loss of information over time) than AD and DLB/AD patients. This result is consistent with a study by Bussè et al. [37], who found less information loss in DLB patients compared to AD patients on the Rey Auditory Verbal Learning Test (RAVLT). Second, the recognition performance of DLB patients was significantly better than that of AD patients, and even comparable to that of controls, suggesting better memory efficiency.
We also highlight the relevance of a third indicator: the performance of DLB patients did not deteriorate over time, unlike that of AD and DLB/AD patients, who experience a rapid and major worsening, given the considerable loss of data between the inclusion visit and the 48-month visit. Our clinicians reported that the latter patients were not able to take the RL/RI-16 test due to excessive memory impairments. The use of easier tests, such as the Dubois’ five words [38], was most often preferred in this case.
Lastly, we note that the memory performance of control subjects tended to decline in terms of delayed total recall, although it remained within the norm. This result may reflect a slight decline in memory efficiency with age, as already noted in previous studies [39–41].
In terms of visual memory, the performance of DLB patients in Set 1 was comparable to that of controls and tended to be superior to that of AD and DLB/AD patients, underlining a relative efficiency of the visual information encoding process. In Set 2, 29% of DLB patients nevertheless showed a deficit score, and the performance of all DLB patients was significantly lower than that of controls. This indicates a possible impairment of visual information storage, especially as the performance of DLB patients did not differ significantly from that of AD and DLB/AD patients. These results are consistent with several studies [7, 12] which demonstrated a deficit in DMS48 performance in DLB patients.
Concerning AD patients, half of them presented an encoding and storage disorder, with 57% of these presenting a loss of information between Set 1 and Set 2, indicating a consolidation deficit, in line with the literature [17]. We also found a similar though more impaired memory profile in DLB/AD patients: 61.5% of them showed both encoding and storage disorders, half of them with a loss of information between Set 1 and Set 2, and only 30.8% had no deficits.
In terms of evolution, the performance of DLB patients on the DMS48 was stable over time, unlike AD and DLB/AD patients’ performances, which deteriorated significantly, with a major loss of data between the inclusion and 48-month visits. As with the verbal memory test, the clinicians in our team reported excessive memory impairment in these patients, and therefore the use of simpler tests, such as the five drawings test [42].
Interestingly, control subjects tended to improve their performance from year to year in Set 1 of the DMS48, highlighting a probable learning effect. Also, the loss of information increased year on year, indicating a potential effect of aging on patients’ memory performance.
In line with the literature [15, 37], our study highlights that visual memory is in general more affected than verbal memory in DLB patients, although their performances are stable over time for both modalities. However, we question here the sensitivity of the DMS48 test in DLB patients, many of whom have attentional and/or visuoperceptual impairments. Indeed, these disorders are likely to disrupt performance on the test, without the deficit being attributable to a real memory impairment. This point had already been raised by a recent study [43], suggesting that recognition memory tests involving a single trial might not be sensitive enough to reveal a medial temporal lobe dysfunction because they do not allow a distinction to be made between a memory deficit and a visuoperceptual or attentional deficit. While the DMS48 authors [33] underlined the relevance of the using the FCSRT and DMS48 tests in combination for the assessment of dominant (verbal) and non-dominant (visual) hemispheres’ storage abilities in the context of insidious onset memory disorders, the combined use of these two tests does not seem to present the same interest in DLB patients. Furthermore, although DLB patients tended to present better memory performance on the DMS48 than AD patients and DLB/AD patients, the difference between these groups was much less pronounced than in the RL/RI-16, both qualitatively (memory profile) and quantitatively (severity of impairment). Thus, although the DMS48 can highlight a few deficits in AD and DLB patients, it does not seem to be a sufficiently sensitive tool to differentiate between these two pathologies.
Taken together, our findings may have important clinical implications as they suggest that the RL/RI-16 test is a relevant tool to distinguish between DLB and AD patients as well as a good indicator of the longitudinal evolution of their memory performance.
Interestingly, the stability of memory performance in DLB patients is in line with the dysfunctional nature of the disease. We suppose that Lewy bodies aggregation first leads to neuronal dysfunction and consequently to relatively stable cognitive impairment, as found in the DLB group. Thus, pure DLB without AD biomarkers would rather be a functional disease with little or no neuronal loss, at least at the early stages. This hypothesis is supported by published data showing that prodromal DLB is associated with less cortical thinning than prodromal AD [44]. On the contrary, the presence of AD biomarkers such as pathological levels of tau, phospho-tau, and Aβ42 would result in neuronal loss and greater cognitive deficits, as found in AD and DLB/AD groups. This assumption is in line with a recent study [45], in which DLB patients with neurofibrillary tangles (due to tau and phosphotau accumulation) had comparable memory-naming impairment compared to AD patients, while DLB patients without neurofibrillary tangles performed better than AD patients.
Limitations
One of the limitations of our study is the inclusion of patients with comorbidities (n = 18). Although they were an exclusion criterion at the time patients were included in both cohorts, neurological (such as stroke) or psychiatric comorbidities (such as depression) emerged in a few patients in the months or years after inclusion. It should be noted that comorbidities are quite common in neurodegenerative diseases. Also, despite the fact that their presence may bias memory profiles, we chose to include patients with neurological or psychiatric comorbidities (n = 18) to gather a larger number of DLB patients (n = 91) and thus potentially increase the robustness of our statistical tests. It also made sense because we conducted longitudinal analyses and our sample size became smaller over time (see Fig. 3). To control for the influence of this variable on our results, we nevertheless performed a qualitative analysis of the memory profile of patients with comorbidities: it did not show any difference compared to other patients.
Additionally, while we managed to select a relatively large sample of DLB patients, our other groups of patients (AD: n = 28; DLB/AD: n = 15) and controls (n = 18) were smaller. However, our study was principally aimed at describing the memory profile of DLB patients, as the literature is already robust regarding AD patients. Besides, we were unfortunately unable to present longitudinal changes in memory performance for both the AD and DLB/AD groups. Although we were not able to administer the memory tests to these patients because of major memory impairments, we nevertheless measured a clear degradation of performance in AD and DLB/AD groups with the MMSE test in a longitudinal study published a few years ago [46]. In that study, our team also showed that patients with DLB reached the stage of severe dementia in 10 years, while those with DLB/AD reached it in 4 years. This last point is in line with the study by Ferman [45], which demonstrated that the dementia trajectory was slowest for autopsy-confirmed transitional Lewy body disease without neocortical tangles, and fastest for diffuse DLB with neurofibrillary tangles.
Fluctuations are also likely to have an impact on memory performance in DLB patients. Attentional fluctuations could impact verbal and visual memory subscores, and fluctuations in performance between visits may have influenced the longitudinal analyses. However, as these fluctuations are recurrent in the clinical presentation of DLB, it seems difficult to control them, especially as we rather consider them as potential factors of memory disturbance than as biases.
Finally, the pharmacological treatment and overall management of the patients may have influenced our results. Some of our patients were in fact receiving medication acting on the nervous system, such as anticholinergic treatment, memantine, anti-depressant, anti-epileptic, neuroleptic, benzodiazepine or anti-parkinsonian treatment. However, we were faced with a major problem in assessing the effect of this variable on our longitudinal analyses as the patients’ medication was constantly changing over time. Moreover, the effect of medication on patients’ cognition merits a comprehensive study, and will be the subject of a future study.
Conclusion
Our study highlights the relevance of four indicators that help to distinguish between DLB and AD patients in terms of verbal memory in the RL/RI-16 test: DLB patients benefit more from semantic cueing, present good recognition and consolidation abilities, and show no deterioration in performance over four years. These clinical elements indicate relatively stable deficits, more executive (i.e., information retrieval) than memory-related, in contrast to AD and DLB/AD patients, most of whom have a bimodal hippocampal syndrome that worsens over time. We also conclude that the DMS48 test would not be a sufficiently sensitive tool, either to highlight the altered processes in DLB patients, or to distinguish them from AD patients.
To assess the impact of executive, attentional and visuoperceptual difficulties on the memory performance of DLB patients, an interesting perspective would be to study the relationship between memory, executive, attentional, and visuoperceptual performances, in order to disentangle the influential relationships between the functions they measure.
Lastly, we believe that future studies on DLB should focus on studying a pure DLB population, with particular attention to the dysfunctional nature of the disease.
ACKNOWLEDGMENTS
We are grateful to the patients and their relatives and the healthy control subjects and their relatives who took part in the study. The authors thank the medical doctors of the Memory Center of Strasbourg (CM2 R), Pierre Anthony, Catherine Martin-Hunyadi, Alix Ravier and Benoît Schorr, the Neuropsychologists, Timothée Albasser, Mathias Bilger, Laure Di Bitonto, Emmanuelle Epp-Ehrhard, Guillaume Jung, Jennifer Kemp, Catherine Kleitz, Jeanne Mérignac, Laetitia Monjoin and Clélie Phillipps, the Research Clinical Assistants, Lucie Rauch, and Lea Sanna as well as the secretary, Gabrielle Huck, for the essential collection of the clinical data. We also thank Olivier Després for his precious advice on our statistical analysis.
FUNDING
This study was funded by Projet Hospitalier de Recherche Clinique (PHRC) inter-régional (IDRCB 2012-A00992-41).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data is not publicly available due to privacy and ethical restrictions.
REFERENCES
[1] | McKeith IG , Boeve BF , Dickson DW , Halliday G , Taylor JP , Weintraub D , Aarsland D , Galvin J , Attems A , Ballard CG , Bayston A , Beach TG , Blanc F , Bohnen N , Bonanni L , Bras J , Brundin P , Burn D , Chen-Plotkin A , Duda JE , El-Agnaf O , Feldman H , Ferman TJ , Ffytche D , Fujishiro H , Galasko D , Goldman JG , Gomperts SN , Graff-Radford NR , Honig LS , Iranzo A , Kantarci K , Kaufer D , Kukull W , Lee VMY , Leverenz JB , Lewis S. , Lippa C , Lunde A , Masellis M , Masliah E , McLean P , Mollenhauer B , Montine TJ , Moreno E , Mori E , Murray M , O’Brien JT , Orimo S , Postuma RB , Ramaswamy S , Ross OA , Salmon DP , Singleton A , Taylor A , Thomas A , Tiraboschi P , Toledo JB , Trojanowski JQ , Tsuang D , Walker Z , Yamada M , Kosaka K ((2017) ) Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology 89: , 88–100. |
[2] | McKeith IG , Ferman TJ , Thomas AJ , Blanc F , Boeve BF , Fujishiro H , Kantarci K , Muscio C , O’Brien JT , Postuma RB , Aarsland D , Ballard C , Bonanni L , Donaghy P , Emre M. , Galvin JE , Galasko D , Goldman JG , Gomperts SN , Honig LS , Ikeda M , Leverenz JB , Lewis SJG , Marder KS , Masellis M , David P , Salmon DP , Taylor JP , Tsuang DW , Walker Z , Tiraboschi P; prodromal DLB Diagnostic Study Group ((2020) ) Research criteria for the diagnosis of prodromal dementia with Lewy bodies. Neurology 94: , 743–755. |
[3] | Hamilton CA , Matthews FE , Donaghy PC , Taylor JP , O’Brien JT , Barnett N , Olsen K , Durcan R , Roberts G , Ciafone J , Barker SAH , Firbank M , McKeith IG , Thomas AJ ((2021) ) Progression to dementia in mild cognitive impairment with Lewy bodies or Alzheimer disease. Neurology 96: , 2685–2693. |
[4] | Cagnin A , Bussè C , Jelcic N , Gnoato F , Mitolo M , Caf-farra P ((2015) ) High specificity of MMSE pentagon scoring for diagnosis of prodromal dementia with Lewy bodies. Parkinsonism Relat Dis 21: , 303–305. |
[5] | Botzung A , Philippi N , Noblet V , Loureiro de Sousa P , Blanc F ((2019) ) Pay attention to the basal ganglia: A volumetric study in early dementia with Lewy bodies. Alzheimers Res Ther 11: , 108. |
[6] | Ciafone J , Thomas A , Durcan R , Donaghy PC , Hamilton CA , Lawley S , Roberts G , Colloby S , Firbank MJ , Allan L , Petrides G , Taylor JP , O’Brien JT , Gallagher P ((2022) ) Neuropsychological impairments and their cognitive architecture in mild cognitive impairment (MCI) with Lewy bodies and MCI-Alzheimer’s disease. J Int Neuropsychol Soc 28: , 963–973. |
[7] | Kemp J , Philippi N , Phillipps C , Demuynck C , Albasser T , Martin-Hunyadi C , Schmidt-Mutter C , Cretin C and Blanc F ((2017) ) Cognitive profile in prodromal dementia with Lewy bodies. Alzheimers Res Ther 9: , 19. |
[8] | Blanc F , Bouteloup V , Paquet C , Chupin M , Pasquier F , Gabelle A , Ceccaldi M , de Sousa PL , Krolak-Salmon P , David R , Fischer C , Dartigues JF , Wallon D , Moreaud O , Sauvée M , Belin C , Harston S , Botzung A , Albasser T , Demuynck C , Namer I , Habert MO , Kremer S , Bousiges O , Verny M , Muller C , Philippi N , Chene G , Cretin B , Mangin JF , Dufouil C ((2022) ) Prodromal characteristics of dementia with Lewybodies: Baseline results of the MEMENTO memory clinics nationwidecohort. Alzheimers Res Ther 14: , 96. |
[9] | Martini A , Weis L , Schifano R , Pistonesi F , Fiorenzato E , Antonini A , Biundo R ((2020) ) Differences in cognitive profiles between Lewy body and Parkinson’s disease dementia. J Neural Transm (Vienna) 127: , 323–330. |
[10] | Gurnani AS , Gavett BE ((2017) ) The differential effects of Alzheimer’s disease and Lewy body pathology on cognitive performance: A meta-analysis. Neuropsychol Rev 27: , 1–17. |
[11] | Ota K , Murayama N , Kasanuki K , Kondo D , Fujishiro H , Arai H , Sato K , Iseki E ((2015) ) Visuoperceptual assessments for differentiating dementia with Lewy bodies and Alzheimer’s disease: Illusory contours and other neuropsychological examinations. Arch Clin Neuropsychol 30: , 256–263. |
[12] | Mondon K , Gochard A , Marque' A , Armand A , Beauchamp D , Prunier C , Jacobi D , de Toffol B , Autret A , Camus V , Hommet C ((2007) ) Visual recognition memory differentiates dementia with Lewy bodies and Parkinson’s disease dementia. J Neurol Neurosurg Psychiatry 78: , 738–741. |
[13] | Petrova M , Mehrabian-Spasova S , Aarsland D , Raycheva M , Traykov L ((2015) ) Clinical and neuropsychological differences between mild Parkinson’s disease dementia and dementia with Lewy bodies. Dement Geriatr Cogn Disord Extra 5: , 212–220. |
[14] | Bussè C , Caffarrac P , Rossia A , Zorzia G , Fragiacomoa F , Camporesea GG , Pompanina S , Di Bernardoe GA , Cagnin A ((2018) ) Testing hippocampal memory in prodromal dementia with Lewy bodies. J Alzheimers Dis 64: , 349–353. |
[15] | Noe E , Marder K , Bell KL , Jacobs DM , Manly JJ , Stern Y ((2004) ) Comparison of dementia with Lewy bodies to Alzheimer’s disease and Parkinson’s disease with dementia. Mov Disord 19: , 60–67. |
[16] | McKhann G M , Knopmanc D S , Chertkowd H , Hymanf B T , Clifford R Jack Jr , Kawash CH , Klunkk WE , Koroshetzl WJ , Manlym JJ , Mayeuxm R , Mohsp RC , Morrisq JC , Rossorr MN , Scheltenss P , Carrillot MC , Thiest B , Weintraubu S , Phelps CH ((2011) ) The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging – Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7: , 263–269. |
[17] | Sánchez-Benavides G , Peña-Casanova J , Casals-Coll M , Gramunt N , Molinuevo JL , Gómez-Ansón B , Aguilar M , Robles A , Antúnez C , Martínez-Parra C , Frank-García A , Fernández-Martínez M , Blesa R. NEURONORMA Study Team ((2014) ) Cognitive and neuroimaging profiles in mild cognitive impairment and Alzheimer’s disease: Data from the Spanish Multicenter Normative Studies (NEURONORMA Project). J Alzheimers Dis 41: , 887–901. |
[18] | Delgado C , Muñoz-Neira C , Soto A , Martinez M , Henriquez F , Flores P , Slachevsky A ((2016) ) Comparison of the psychometricproperties of the “Word” and “Picture” versions of the Free andCued Selective Reminding Test in a Spanish-speaking cohort ofpatients with mild Alzheimer’s disease and cognitively healthycontrols. Arch Clin Neuropsychol 31: , 165–175. |
[19] | Braak H , Braak E ((1995) ) Staging of Alzheimer’s disease-related neurofibrillary changes. Neurobiol Aging 16: , 271–284. |
[20] | Jack CR Jr , Petersen RC , Xu YC , O’Brien PC , Smith GE , Ivnik RJ , Boeve BF , Waring SC , Tangalos EG , Kokmen E ((1999) ) Prediction of AD with MRI-based hippocampal volume in mild cognitive impairment. Neurology 52: , 1397–1403. |
[21] | Mungas D , Jagust WJ , Reed BR , Kramer JH , Weiner MW , Schuff N , Norman D , Mack WJ , Willis L , Chui HC ((2001) ) MRI predictors of cognition in subcortical ischemic vascular disease and Alzheimer’s disease. Neurology 57: , 2229–2235. |
[22] | Petersen RC , Jack CR Jr , Xu YC , Waring SC , O’Brien PC , Smith GE , Ivnik RJ , Tangalos EG , Boeve BF , Kokmen E ((2000) ) Memory and MRI-based hippocampal volumes in aging and AD. Neurology 54: , 581–587. |
[23] | Grober E , Hall CB , Lipton RB , Zonderman AB , Resnick SM , Kawas C ((2008) ) Memory impairment, executive dysfunction, and intellectual decline in preclinical Alzheimer’s disease. J Int Neuropsychol Soc 14: , 266–278. |
[24] | Bousiges O , Blanc F ((2022) ) Biomarkers of dementia with Lewy bodies: Differential diagnostic with Alzheimer’s disease. Int J Mol Sci. 23: , 6371. |
[25] | Ferman TJ , Smith GE , Boeve BF , Ivnik RJ , Petersen RC , Knopman D , Graff-Radfort N , Parisi J , Dickson DW ((2004) ) DLB fluctuations specific features that reliably differentiate DLB from AD and normal aging. Neurology 62: , 181–187. |
[26] | Fenelon G , Soulas T , Zenasni F , Cleret de Langavant L ((2010) ) The changing face of Parkinson’s disease-associated psychosis: A cross-sectional study based on the new NINDS-NIMH criteria. Mov Disord 25: , 763–766. |
[27] | The Unified Parkinson’s Disease Rating Scale (UPDRS): Status and recommendations ((2003) ) Mov Disord 18: , 738–750. |
[28] | Gjerstad MD , Boeve B , Wentzel-Larsen T , Aarsland D , Larsen JP ((2008) ) Occurrence and clinical correlates of REM sleep behaviour disorder in patients with Parkinson’s disease over time. J Neurol Neurosurg Psychiatry 79: , 387–391. |
[29] | Dubois B , Feldman HH , Jacova C , Dekosky ST , Barberger-Gateau P , Cummings J , Delacourte A , Galasko D , Gauthier S , Jicha G , Meguro K , O’Brien J , Pasquier F , Robert P , Rossor M , Salloway S , Stern Y , Visser PJ , Scheltens P ((2007) ) Research criteria for the diagnosis of Alzheimer’s disease: Revising the NINCDS-ADRDA criteria. Lancet Neurol 6: , 734–746. |
[30] | Folstein MF , Folstein SE , McHugh PR ((1975) ) Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: , 189–198. |
[31] | Van der Linden, M , Coyette, F , Poitrenaud, J , Kalafat, M , Calacis, F , Wyns, C , Adam, S , et les membres du GREMEM ((2004) ) L’épreuve de rappel libre/rappel indicé à 16 items (RL/RI-16). In L’évaluation des troubles de la mémoire: Présentation de quatre tests de mémoire épisodique (avec leur étalonnage), Van der Linden M, Adam S, Agniel A, Baisset Mouly C, ed. Solal, Marseille, pp. 1–19. |
[32] | Grober E , Buschke H ((1987) ) Genuine memory deficit in dementia. Dev Neuropsychol 56: , 303–308. |
[33] | Barbeau E , Tramoni E , Joubert S , Mancini J , Ceccaldi M , Poncet M ((2004) ) Evaluation de la mémoire de reconnaissance visuelle:Normalisation d’une nouvelle épreuve en choix forcé (DMS 48)et utilité en neuropsychologie clinique. L’évaluation des troubles de la mémoire: Présentation de quatre tests de mémoire épisodique (avec leur étalonnage), Van derLinden M, Adam S, Agniel A, Baisset Mouly C, ed. Solal, Marseille, pp. 85–101. |
[34] | Vogel A , Mellergaard C , Waldemar G , Frederiksen KS ((2021) ) Impaired performances on the category cued memory test in mild Alzheimer’s disease and dementia with Lewy bodies: A comparative validity study. Appl Neuropsychol Adult 27: , 1–6. |
[35] | Nagahama Y ((2016) ) Clinical neuropsychology of dementia with Lewy bodies. Brain Nerve 68: , 165–174. |
[36] | Sarazin M , Chauvire V , Gerardin E , Colliot O , Kinkingnéhun S , DeSouza LC , Hugonot-Diener L , Garnero L , Lehericy S , Chupin M , Dubois B ((2010) ) The amnestic syndrome of hippocampal type in Alzheimer’sdisease: An MRI study. J Alzheimers Dis 22: , 285–294. |
[37] | Bussè C , Anselmi P , Pompanin S , Zorzi G , Fragiacomo F , Camporese G , Di Bernardo GA , Semenza C , Caffarra P , Cagnin A ((2017) ) Specific verbal memory measures may distinguish Alzheimer’s disease from dementia with Lewy bodies. J Alzheimers Dis 59: , 1009–1015. |
[38] | Dubois B , Touchon J , Portet F , Ousset PJ , Vellas B , Michel B ((2002) ) The 5 words: A simple and sensitive test for the diagnosis of Alzheimer’s disease. Presse Med 31: , 1696–1699. |
[39] | Cabeza R ((2002) ) Hemispheric asymmetry reduction in older adults: The HAROLD model. Psychol Aging 17: , 85–100. |
[40] | Rönnlund M , Nyberg L , Bäckman L , Nilsson LG ((2005) ) Stability, growth, and decline in adult life span development of declarative memory: Cross-sectional and longitudinal data from a population-based study. Psychol Aging 20: , 3–18. |
[41] | Der G , Allerhand M , Starr JM , Hofer SM , Deary IJ ((2010) ) Age-related changes in memory and fluid reasoning in a sample of healthy old people. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 17: , 55–70. |
[42] | Croisile B , Milliery M , Collomb K , Colombe C , Mollion H ((2009) ) Le Test des 5 dessins: Un test de mémoire visuo-spatiale àutiliser dans la maladie d’Alzheimer. Rev Gériatr 34: , 495–503. |
[43] | Philippi N , Noblet V , Duron E , Cretin B , Boully C , Wisniewski I , Seux ML , Martin-Hunyadi C , Chaussade E , Demuynck C , Kremer S , Lehéricy S , Gounot D , Armspach JP , Hanon O , Blanc F ((2016) ) Exploring anterograde memory: A volumetric MRI study in patientswith mild cognitive impairment. Alzheimers Res Ther 8: , 26. |
[44] | Blanc F , Colloby SJ , Philippi N , de Pétigny X , Jung B , Demuynck C , Phillipps C , Anthony P , Thomas A , Bing F , Lamy J , Martin-Hunyadi C , O’Brien JT , Cretin B , McKeith I , Armspach JP , Taylor JP ((2015) ) Cortical thickness in dementia with Lewy bodies and Alzheimer’sdisease: A comparison of prodromal and dementia stages. PLoS One 10: , 0127396. |
[45] | Ferman TJ , Aoki N , Boeve BF , Aakre JA , Kantarci K , Graff-Radford J , Parisi JE , Van Gerpen JA , Graff-Radford NR , Uitti RJ , Pedraza O , Murray ME , Wszolek ZK , Reichard RR , Fields JA , Ross OA , Knopman DS , Petersen RC , Dickson DW ((2020) ) Subtypes of dementia with Lewy bodies are associated with α-synuclein and tau distribution. Neurology 95: , 155–165. |
[46] | Blanc F , Mahmoudi R , Jonveaux T , Galmiche J , Chopard G , Cretin B , Demuynck C , Martin-Hunyadi C , Philippi N , Sellal F , Michel JM , Tio G , Stackfleth M , Vandel P , Magnin E , Novella JL , Kaltenbach G , Benetos A , Sauleau EA ((2017) ) Long-term cognitive outcome of Alzheimer’s disease and dementia with Lewy bodies: Dual disease is worse. Alzheimers Res Ther 9: , 47. |


