
Physical Activity for Cognitive Health: A Model for Intervention Design for People Experiencing Cognitive Concerns and Symptoms of Depression or Anxiety
Abstract
Background:
People experiencing cognitive concerns and symptoms of depression or anxiety are at risk for Alzheimer’s disease and dementia. We know physical activity can benefit cognition but understanding how to best support engagement is an ongoing challenge. Evidence-based conceptual models of factors underpinning physical activity engagement in target populations can inform intervention tailoring to address this challenge.
Objective:
This study (part of a pragmatic physical activity implementation trial) aimed to develop a specified model of physical activity engagement in people experiencing depressive or anxiety symptoms and cognitive concerns, to enable optimized dementia risk reduction intervention tailoring.
Methods:
We employed a qualitative design, triangulating data from three sources: semi-structured individual interviews with people experiencing cognitive concerns and mild to moderate depressive or anxiety symptoms; review of published evidence; and the Capability, Opportunity and Motivation system of behavior, an existing behavioral science model. Findings were integrated to develop a contextualized model of mechanisms of action for optimizing engagement.
Results:
Twenty-one participants were interviewed, and 24 relevant papers included. Convergent and complementary themes extended understanding of intervention needs. Findings highlighted emotional regulation, capacities to enact intentions despite barriers, and confidence in existing skills as areas of population-specific need that have not previously been emphasized. The final model provides specificity, directionality, and linked approaches for intervention tailoring.
Conclusion:
This study demonstrated that people experiencing cognitive concerns and symptoms of depression or anxiety require different interventions to improve physical activity engagement. This novel model can enable more precise intervention tailoring, and, ultimately, benefits for a key at-risk population.
INTRODUCTION
As part of a comprehensive response to the public health challenge of dementia, higher-risk populations are key target groups for individual interventions to reduce modifiable dementia risk factors, such as physical inactivity, poor diets, social disengagement, and vascular diseases [1–3]. People in mid- or later-life who live with mild cognitive impairment (MCI) or subjective cognitive decline (SCD) (combined, referred to as cognitive concerns for this report) and who concurrently experience clinically significant symptoms of depression or anxiety are one at-risk population where greater research attention is required.
The specific relationships between dementia and cognitive concerns, depression and anxiety are complex, variable, and likely bi-directional. Each type of problem has been independently associated with increased dementia risk [1, 4–6], including a recent large meta-analysis that reported pooled ORs for all cause dementia of 1.91 (95% CI 1.72 –2.12) in depression and of 1.60 (95% CI 1.29–2.00) in anxiety [7]. Each is also associated with higher rates of other modifiable dementia risk factors, such as those described above [8], contributing to compounding risk of dementia and poor broader health and functional outcomes. Finally, depressive, anxiety, and cognitive symptoms very commonly overlap or co-occur [9–13]. Hence, targeting this pooled population could be a pragmatic, efficient approach to dementia risk reduction (DRR) that also optimizes intervention reach.
Adopting and maintaining regular physical activity (PA) in line with guidelines’ recommendations [14] (Fig. 1) may be a particularly beneficial approach to DRR for this population [15]. PA is one of the best supported DRR intervention types, including for people with cognitive concerns [1, 16, 17]. There is also strong evidence that PA can reduce symptoms of depression or anxiety [18–20] and benefit vascular health in people who are experiencing depression or anxiety [20–22]. Combined, these effects could substantially reduce individual dementia risk and improve mental and physical wellbeing.
Fig. 1
Summary physical activity recommendations for people with cognitive concerns, adapted from Australian general population guidelines [23], and from specific guidelines for older Australians living with mild cognitive impairment or subjective cognitive decline [24].
![Summary physical activity recommendations for people with cognitive concerns, adapted from Australian general population guidelines [23], and from specific guidelines for older Australians living with mild cognitive impairment or subjective cognitive decline [24].](https://ip.ios.semcs.net:443/media/jad/2023/94-2/jad-94-2-jad221216/jad-94-jad221216-g001.jpg)
A key ongoing challenge for DRR research is discovering how to better support target groups to adopt and maintain PA. Despite the well-known health benefits, only 44% of Australian adults currently achieve recommended aerobic PA levels, and less than a quarter meet strength-based activity guidelines, consistent with findings from other high-income countries [25]. Commonly reported barriers include shortage of time, cost, competing priorities, and over-estimating current activity level [25]. Behavior change interventions can help overcome barriers and address this public health challenge, with consistent evidence of efficacy and small to medium effect sizes for both PA adoption and maintenance (e.g., a recent large meta-analysis including 26 randomized controlled trials calculated effect sizes of d = 0.32, 95% CI 016–0.48 for adoption and d = 0.21, 95% CI 0.12–0.30 for maintenance for more than six months [26]).
Behavior change seems more challenging for people living with cognitive concerns and depression or anxiety. They likely experience additional and unique engagement barriers but identifying and addressing their specific needs have often been overlooked in trials to date. Depression and anxiety have been associated with reduced uptake, adherence, or effectiveness in PA behavior change interventions that were designed for the general population, including in DRR and wider health promotion contexts [8, 27, 28]. There is also some evidence that people living with cognitive concerns might experience more barriers to increasing PA, including low self-efficacy, reduced enjoyment, and greater stress with PA [29]. The recently completed Maintain Your Brain trial of an online multi-domain DRR intervention for people at risk of dementia partly addresses this issue by including more comprehensive depression treatment modules [30]. However, tailoring across the range of DRR interventions, including PA, has been limited. There is now an urgent need to better understand tailoring needs and to investigate new approaches and implementation pathways to enable this group, and others with multiple needs, to engage with PA and reduce their dementia risk.
The supports embedded within interventions to help participants change their behavior are termed behavior change techniques (BCTs) and the different processes through which they affect behavior are the intervention mechanisms of action (MoAs). Understanding which MoAs influence target behaviors is important as interventions may be more effective when they use MoAs that are known (or expected) to exert significant influence on target behavior patterns in target populations [31, 32]. A thematic synthesis of 50 qualitative studies reporting general population perspectives of DRR recently provided initial insights into potentially important MoAs for DRR, finding that knowledge, motivation, social processes, and volitional processes (through which motivation and intentions are turned into action) may all be important [33]. However, further data to support effective and efficient BCT selection in DRR remain limited and most clinical trials apply non-systematic and non-targeted approaches [34, 35].
Furthermore, the published synthesis did not explore the key issue of potential differences in influential MoAs for different DRR activities or individual target populations. Knowledge of the specific needs of people with cognitive concerns and depression or anxiety remains minimal, although some data is emerging for related groups. A recent qualitative follow-up of a PA program for older adults with cognitive concerns found several factors relating to motivation and context (including social and environmental factors) influenced PA engagement for DRR, while self-efficacy, habit formation and perceived benefits were important for PA maintenance [36]. The wider literature also suggests that key MoAs for PA engagement (for diverse health outcomes) in people experiencing depression or anxiety may be different [8, 37, 38].
These insights suggest inadequate BCT tailoring may contribute to the disappointing engagement seen for our target population with interventions to date. They highlight the need for more precise tailoring that is underpinned by detailed, contextually specified understanding of MoAs for PA engagement for DRR in this population [31, 32].
Triangulating new qualitative data specific to this target population with existing data from the large body of published literature regarding the adjacent context of PA for people with depression or anxiety and theoretical propositions from behavioral science is a new approach in this field that can help efficiently address the current knowledge gap and contextualize findings. The Capability, Opportunity and Motivation system of behavior (COM-B) [32] is one behavioral science model providing a pragmatic theoretical framework of internal mechanisms and environmental factors underpinning behavior and behavior change to support organization and interpretation of empirical data. It is well-established and has been applied in processes for behavior change intervention design, development and tailoring across diverse healthcare settings, including in mental health care [39, 40]. It describes three broad mechanistic constructs as influencing behavior, as shown in Fig. 2. These constructs align well with the key MoAs identified in published literature as important for DRR in people with cognitive concerns and in the general population [33, 36].
Fig. 2
The COM-B system of constructs underpinning behavior change, adapted from [41]. Each major model construct includes multiple individual mechanisms. Capability includes physical and psychological capabilities (including knowledge); Motivation includes automatic and reflective factors (e.g., habits and outcome expectancies); Opportunity includes both social and physical environmental factors. The system proposes that capabilities and opportunities both influence motivation and that each construct directly influences behavior. Finally, behaviors themselves reciprocally influence capabilities, motivation, and opportunities.
![The COM-B system of constructs underpinning behavior change, adapted from [41]. Each major model construct includes multiple individual mechanisms. Capability includes physical and psychological capabilities (including knowledge); Motivation includes automatic and reflective factors (e.g., habits and outcome expectancies); Opportunity includes both social and physical environmental factors. The system proposes that capabilities and opportunities both influence motivation and that each construct directly influences behavior. Finally, behaviors themselves reciprocally influence capabilities, motivation, and opportunities.](https://ip.ios.semcs.net:443/media/jad/2023/94-2/jad-94-2-jad221216/jad-94-jad221216-g002.jpg)
The Exercise for Cognitive Health (EXCEL) Study [42] is a multi-phase project that aimed to develop an evidence base for how to best support people living with cognitive concerns and depression or anxiety to meet guidelines for PA for DRR. The study reflects the first phase of EXCEL.
Our objective for this study was to develop an evidenced-informed model of PA for DRR interventions specific to people in mid- and later-life experiencing cognitive concerns and depression or anxiety. These findings contributed to subsequent design of a tailored intervention for pilot evaluation.
To achieve this objective, we aimed to:
• Examine the qualitative PA and DRR perspectives of people experiencing cognitive concerns and depression or anxiety.
• Contextualize interview findings within the existing evidence through a critical review of related literature.
• Map interview and literature review findings and existing theory to develop an integrated model of the MoAs underpinning successful adoption and maintenance of PA for DRR for our target population.
METHODS
Design and setting
This phase of the EXCEL Study comprised semi-structured qualitative interviews and a critical literature review, followed by a data mapping process to triangulate results with behavioral science theory to develop the specified model. The design was based on established recommendations for behavioral analysis and complex intervention design, with COM-B as an organizing framework [31, 32] (Fig. 2). Due to the COVID-19 pandemic, the original protocol was adapted so all study activities used video or voice calls via Information and Communications technology (ICT). The study was approved by University of Melbourne Human Ethics Committee (ID: 2057282.1).
Semi-structured interviews
Individuals aged between 45 and 80 years, residing in the community, with cognitive concerns and mild to moderate depression and/or anxiety were invited to interviews. Recruitment was via advertisement in local community and university newsletters and community groups. All participants provided written informed consent.
In addition to inclusion and exclusion criteria developed for the parent EXCEL Study [42], we used purposive sampling techniques to ensure representation across genders and age groups.
Inclusion criteria comprised:
• Evidence of MCI, according to the Modified Telephone Interview for Cognitive Status (TICS-M) scale, or SCD. TICS-M is a tailored tool for telephone-based cognitive screening, with a maximum score of 50 and acceptable sensitivity and specificity for distinguishing MCI from normal cognition and dementia using upper and lower cut-off scores of 31 and 28, respectively [43]. SCD was identified through questionnaire items regarding subjective experiences of confusion or memory loss.
• Mild to moderate depressive and/or anxiety symptoms, as measured by the Depression Anxiety and Stress Scale (DASS-21). The DASS-21 measures depressive, anxiety, and stress symptoms, with total scoring between 0 and 63. Scores of 10–20 and 8–14 reflect mild to moderate symptoms on the depression and anxiety subscales, respectively [44].
• Adequate English language to engage in interviews and complete study documents.
Exclusion criteria comprised:
• Diagnosis of dementia or TICS-M score of less than 28.
• Severe depression (DASS-21 score > 20) or diagnosis of another severe mental illness (schizophrenia, bipolar affective disorder or eating disorder).
• Comorbid physical health problem that would preclude participation in an unsupervised moderate intensity PA program (such as significant cardiovascular or respiratory conditions).
• Inadequate English language to participate in interviews or complete study paperwork.
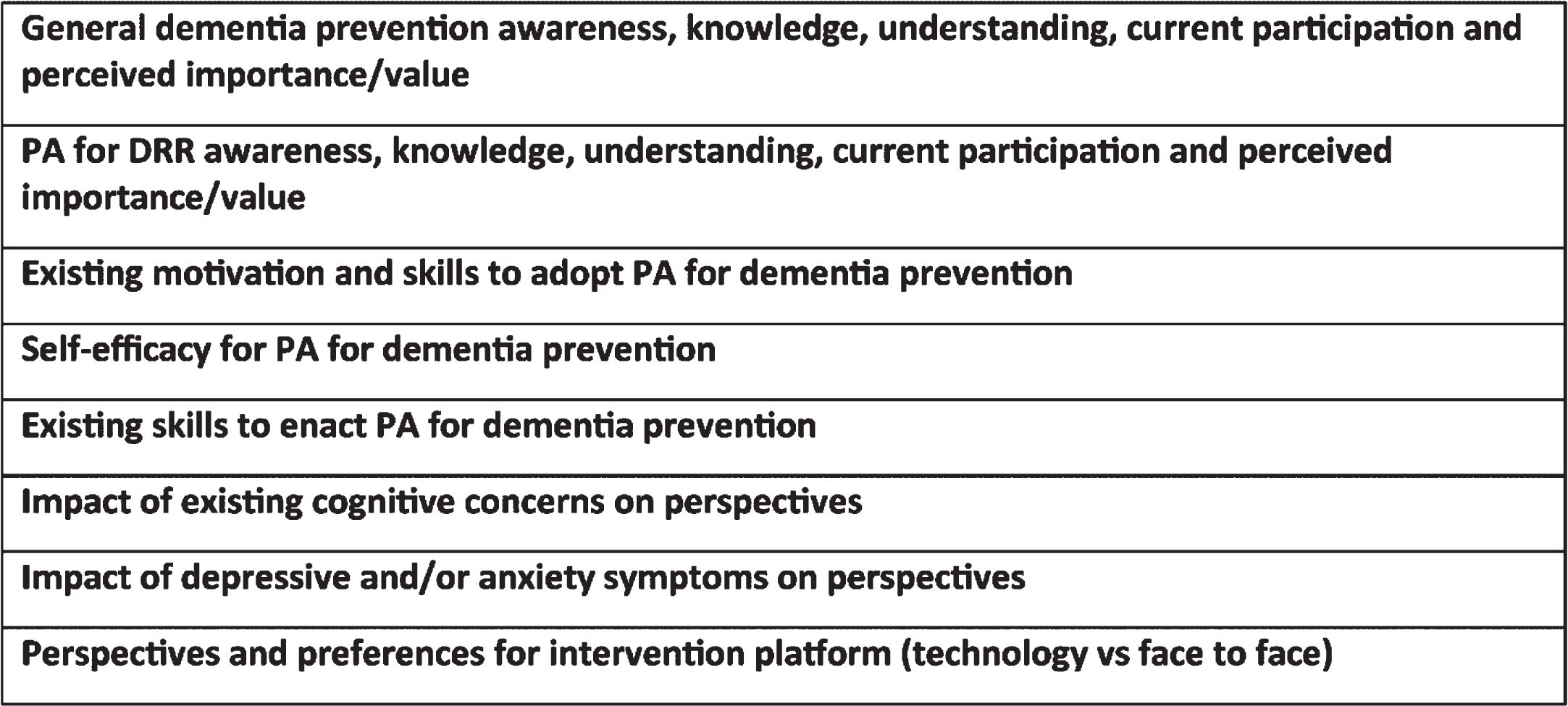
Interviews examined participant perspectives regarding DRR, PA and interventions to support engagement. Interview domains were developed by the study team based on the study framework and prior experience in both DRR and mental health research (Fig. 3). Self-reported current regular weekly physical activity (frequency, duration, and intensity) was assessed using a modified version of the Adult Pre-Exercise Screening System (APSS) tool [45]. Questions were piloted to establish face validity and ease of completion for participants. Researchers initially provided broad information about the objective of the EXCEL Study and encouraged participants to share their perspectives and current engagement in DRR and PA. Further information was then provided about PA for DRR, and participants were prompted to discuss influences on their current PA engagement, particularly factors they felt either helped or hindered this.
Fig. 3
Semi-structured interview domains.
Critical review of existing evidence
To contextualize themes identified from interviews, we critically reviewed the published literature regarding PA interventions for people living with cognitive concerns, depression, or anxiety. We sought evidence and insights about effective MoAs for these interventions, particularly in similar contexts to the EXCEL Study. Publications were identified through searches of Ovid MEDLINE and PubMed, hand searching reference lists of included studies and consultation with experts from the EXCEL investigator group were used to identify any additional studies.
We included review papers or reports of primary studies of interventions to increase PA, where PA behavior change was described in outcomes or adherence findings, published in English language peer-reviewed journals between 2010 and the end of 2021. We included both randomized controlled trials and quasi-experimental designs. Anticipating that few studies have directly examined MoAs, we included any reviews or intervention studies that demonstrated increased PA and included sufficient detail for identification of included BCTs, based on manual review of the full-texts of manuscripts.
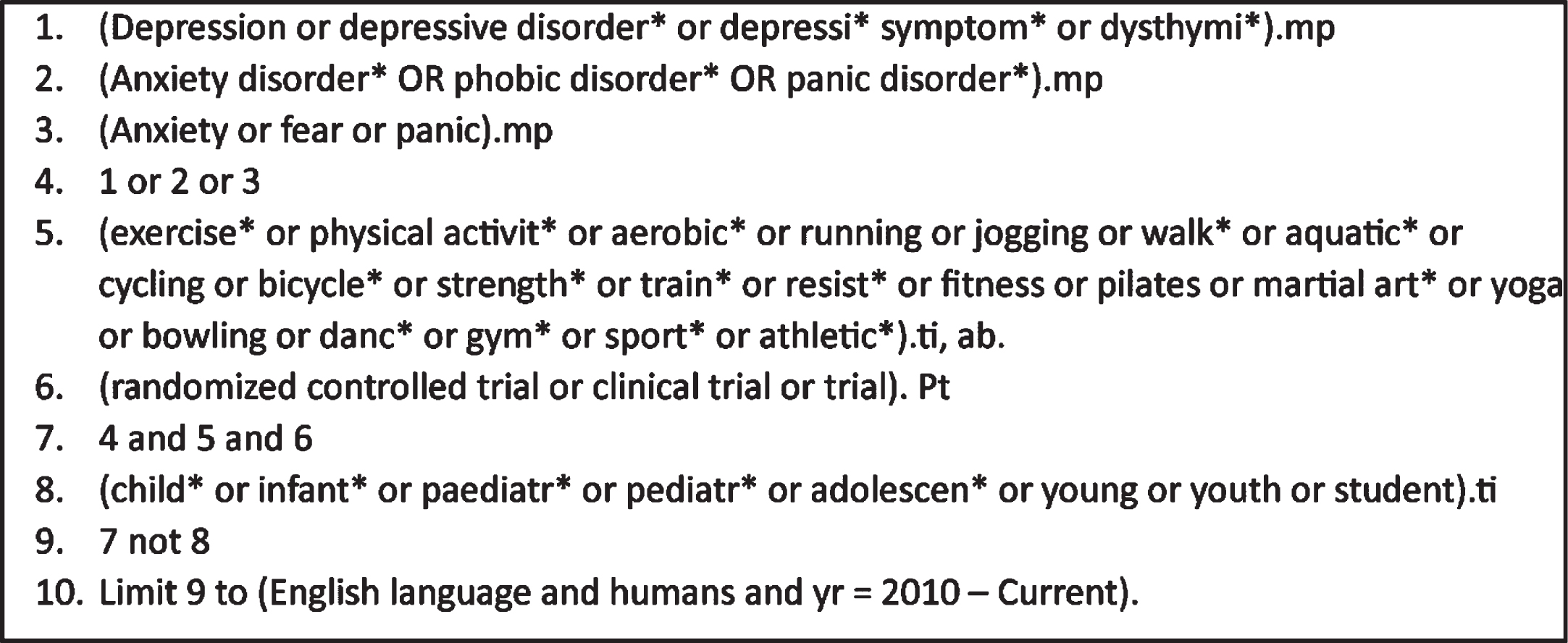
We applied stepped inclusion criteria to prioritize evidence relating to similar contexts to the EXCEL Study. We also maintained a focus on populations with depression or anxiety as we anticipated that these participant characteristics would be most associated with differential intervention MoAs. We initially sought studies investigating cognitive health promotion for middle-aged and/or older participants (aged 45 years and older) living with cognitive concerns and depression or anxiety. We then expanded inclusion criteria to studies with the same target population as EXCEL but set in other health contexts such as depression treatment. Finally, we progressively expanded included populations to people in mid- and later-life experiencing depression or anxiety but without cognitive concerns, then adults of any age experiencing depression or anxiety (see Fig. 4 for example search strategy developed for Medline).
Fig. 4
Search strategy for Ovid Medline.
One researcher conducted all searches and initial screening (EC). Included studies were independently assessed for eligibility by another researcher (TC or TR) and any disagreements were resolved by group discussion. BCTs in each included study were identified and grouped according to an established taxonomy [46]. BCTs for each study were independently identified by two researchers from the group (EC, TC, TR), and a final consensus list was produced through a workshop with all three researchers. MoAs potentially engaged by each BCT were then identified using the ‘Theory and Techniques Tool’, developed by an international collaboration for behavior change intervention research [47]. This tool links 74 BCTs to 26 identified MoAs, based on expert consensus and a published literature synthesis [47, 48]. Acknowledging that BCTs can link to multiple MoAs, we took a pragmatic approach for this study context and reported all linked MoAs.
Data analysis
Data analysis for interviews occurred concurrently with data collection and interviews continued until no new themes were identified, indicating saturation.
Interviews were recorded and fully transcribed. Transcripts were imported into NVivo 12 [49] for data management and manual coding within the program. A thematic analysis was conducted following Braun and Clarke’s approach [50, 51]. This allowed for a generally inductive approach that accommodated both descriptive and interpretive aspects in identified themes. Theoretical flexibility meant latter stages of analysis could be informed by the COM-B system. The first six interview transcripts were independently coded by two researchers (EC, AW). Discussion of coding differences and similarities was used to generate initial agreed codes. The remaining interviews were divided and each coded by one researcher with discussion, revision and addition of further codes as required, then grouping into themes and development of a preliminary model of important MoAs.
For triangulation, we examined for convergence between themes from interviews, MoAs identified as prominent in the existing literature and the key constructs predicted by the COM-B system. We also identified complementary findings that were evident only in one data source but helped create a fuller picture of key MoAs for this context. Following discussion and refinement among the whole team, this produced a tailored and evidence-based model of potentially influential MoAs to inform intervention design.
RESULTS
Participants
Fifty-three people completed consent and screening processes. Twenty-three (43%) were eligible and 21 completed interviews. Twenty-one individuals were ineligible because DASS-21 subscale scores did not reach threshold for clinically significant symptoms; five individuals reported severe depressive or anxiety symptoms; two individuals had cognitive impairment consistent with dementia on TICS-M; and two individuals had co-morbid physical health conditions that deemed them ineligible. Two eligible participants withdrew prior to interviews, due to other commitments and preferring to participate in an intervention study, respectively.
Most (19) of the 21 participants were female, highly educated, lived in an urban area, and aged 60 years or older. The majority had subjective but not objective cognitive impairment, experienced mild mood or anxiety symptoms and already engaged in primarily aerobic PA (Table 1). Two participants (8.7%) did not currently engage in any PA.
Table 1
Participant characteristics and PA levels
| Demographics | |
| Age, y, mean (SD), [range] | 66 (9.2), [49–80] |
| Female, n (%) | 19 (90%) |
| Completed post-secondary education, n (%) | 19 (90%) |
| Currently employed (full-time, part-time or casual), n (%) | 10 (48%) |
| Retired, n (%) | 9 (43%) |
| Living in metropolitan area, n (%) | 19 (90%) |
| Cognition | |
| TICS-M score, mean (SD) | 37.4 (2.74) |
| DASS-21 sub-scale scores | |
| Depressive subscale score, mean (SD) | 11.0 (5.2) |
| Anxiety subscale score, mean (SD) | 5.1 (4.8) |
| Baseline PA | |
| Weekly minutes of at least moderate aerobic PA, mean (SD) | 178.6 (161.7) |
| Meeting aerobic PA guidelines, n (%) | 12 (52.2) |
| Meeting strength PA guidelines, n (%) | 5 (21.7) |
| Meeting balance PA guidelines (older adults only), n (%) | 4 (22.2) |
| Meeting complete relevant PA guidelines, n (%) | 2 (8.7) |
TICS-M, modified telephone interview for cognitive status; DASS-21, depression, anxiety and stress scale; PA, calculated from APSS tool (modified) responses.
Interview themes
Five main themes were identified from the interview data, with participants in both mid- and later-life contributing to all themes. Each main theme is summarized below, with representative quotations in Table 2. For more detailed description of themes and all supportive quotations, see Supplementary Material 1.
Table 2
Supportive quotations for interview themes
| Theme | Example supportive quotations |
| Being informed to enable change | I guess I realize that [to prevent] dementia you need to, it needs to be care of your body, physical, mental, spiritual, anything that can assist to keep abreast of what’s happening. Just keeping a good wellbeing. I guess that’s as far as I’ve got. (F, 73) I think the things that would help with dementia would be things not just aerobic or strength, I suppose they do, but like dancing where your brain is involved kind of. I don’t know, maybe your brain is involved in other stuff as well. (F, 72) Trying to find out more about it, watching television programs that have dealt with dementia. (F, 73) I use it [the internet] all the time for everything . . . always googling something. (F, 53) I guess if I knew that there was a certain amount of exercise would have a positive impact on dementia prevention and what sort of exercise, maybe it’s any exercise. More education about that might motivate me. (F, 51) |
| Skills and confidence to make and enact intentions are vital | So I don’t know what can get me from the willingness to the doing. (F, 51) The anxiety thing of starting something new can be incredibly overwhelming. (F, 65) It [depressive symptoms] sort of paints a negative wash in your brain, and you think, ‘Well, I know I ought to be doing this,’ or, ‘I ought to be eating that way,’ or, ‘I ought to be exercising today,’ but when one gets into such a frame of mind, you know you can go for help, you know what to do in order to help these things, but there’s something about that period of time that thinks, ‘Well, you know, fair enough, let other people do it’. (F, 72) What I need to try and do more is where I actually can’t do activity for reason of injury or something like that, I need to just go and have a walk or something. I’m not very good at gentle exercise, put it that way. (M, 55) Planning and helping me gain some sort of control over my life, now that I don’t have a lot of control over my life [with depression]. (F, 78) |
| Individual attitudes can support urgency for change | I think I’d be more concerned about dementia and my memory . . . if I wasn’t able to compare notes with other people, and virtually everyone I know has different levels of memory problems. (F, 80) I’d say nine and a half, nine and three-quarters, ten out of ten. Yes, pretty important [to prevent dementia]. (F, 60) Enjoyment, if I enjoy something, there’s no question, I seek enjoyment. And there are things I do in my life that I really enjoy, and there’s no trouble motivating me at all if I really enjoy it. (M, 62) Short-term would be like that quick fix, quick hit, of endorphins if you go and do some exercise, and then longer-term, your physical and mental health. (F, 53) I was just so unbalanced on the bike that I was too scared of falling over and, you know, smashing my knee on a concrete kerb or something and ending up more disabled than I already was. (F, 60) |
| Access to reliable, flexible resources can help overcome barriers | I’m very keen, I’m happy to read stuff, I’m happy to look things up on the internet, I’m happy to watch stuff if it was available, all of the above . . . If I was thinking that I wanted to particularly save something which may be a set of instructions, “Do this to improve your mental health,” I would just save it and go print it. (F, 71) A program where I can, that you check in and go righto. You could do this last week, can you do two more this week? . . . You know if you’ve got guidelines to set that pushes you, yeah. Okay I’ll do it. And if someone’s going to check on you, oh. (M, 55) I guess, finding the right place to do it as well. Somewhere comfortable with the right program. So, having to do a bit of footwork or research to find what’s right for me. (F, 62) I think another barrier is getting ready in the cold for half an hour and then coming home, that’s a barrier (F, 51) |
| Access to social opportunities for accountability and support | Yeah that’s it, that’s that commitment to others. Someone else is relying on you to come yeah. (F, 62) I do prefer to walk by myself to be honest. I mean, one, when my husband comes, he walks slower than I do and I just find it irritating having someone walking behind me, but I always feel like I’ve got to ask, do you want to come. Maybe I just shouldn’t ask, but then if he’s around, I don’t tend to go. (F, 60) I would be encouraged by family for sure. If I said I was hoping to make these changes, I’d have a lot of support with family. (F, 62) I do a lot of walking with friends at lunch time, so that sort of thing would make it easier, the support of others. (F, 53) |
Being informed to enable change
Participants indicated having at least some awareness or understanding that engaging in PA can reduce dementia risk, but detailed views indicated significant knowledge gaps regarding the concept, the need for change, specific changes required and how to ‘do’ recommended activities.
Existing knowledge derived from diverse sources, particularly personal social networks, media (especially news media, hospital or public health consumer information, and television) or health professionals.
Some believed the DRR benefits of PA were only secondary to broader health benefits or to the cognitive challenge of PA. Most were aware of benefits for depressive and anxiety symptoms, but no participants linked these with cognitive health. More specific procedural knowledge was lacking. There was no awareness of guidelines’ recommendations and there were diverse perspectives regarding the best type, amount, and intensity of PA. Several participants believed that incidental PA was sufficient, and others acknowledged not knowing ‘how’ to do strength exercises. These gaps highlight the importance of specific knowledge for effective behavior change.
In several interviews, information seeking was prominent and knowledge appeared linked to a sense of empowerment to make effective changes and impact cognitive health. Participants wished to improve their conceptual and procedural knowledge. Some believed that awareness of benefits would directly enable them to adopt PA, but more implied that knowledge alone was inadequate. Procedural knowledge was emphasized by some because it provided clarity. Some also highlighted procedural knowledge and/or clearer research findings as increasing confidence in expected outcomes, indicating pathways between knowledge and expectations as helping enable change.
Skills and confidence to make and enact intentions are vital
Several participants expressed prominent beliefs that difficulties ‘controlling’ emotions and behaviors impeded PA uptake. They described these as barriers to turning PA intentions and motivation into action. ’Poor self-control’ was used by participants to describe difficulties monitoring their behavior, acting on intentions and being distracted or put off by barriers. Several emphasized this as central to unhelpful habits and difficulty maintaining PA. A few specifically linked these difficulties to negative emotions, describing emotions as so overwhelming that they lost track of behavior. Other participants described avoidance or withdrawal as something they habitually did to specifically regulate negative emotions. Both descriptions implied direct links between difficulty regulating negative emotions and difficulty regulating behavior.
Low confidence in behavioral and emotional regulation abilities was also prominent. Some participants believed they were ‘incapable’ of PA because they anticipated standard recommendations would cause pain or exacerbate injuries or health complaints. Such comments were sometimes linked to low confidence in abilities to (safely) adapt PA to accommodate physical issues. A few participants described demoralization and low general self-efficacy as core to both their mental health problems and physical inactivity. Others highlighted a vicious cycle in which physical inactivity and lack of confidence in capacities to change this exacerbated general demoralization, which they also felt unable to control.
Conversely, several participants who were already physically active believed their skills to carry out intentions and to navigate other barriers were key to their subjective success. Skills emphasized included: capacities both to make PA a habit and to identify and break other unhelpful habits; capacities to monitor PA behavior and notice immediate emotional/physical benefits; and capacities to persist and adapt when faced with frustrating changes to physical health or injury. Capacity and confidence to adapt PA in response to injury was sometimes directly attributed to prior professional advice on the topic.
Individual attitudes can influence a sense of urgency for change
A distinction between general attitudes to PA and more specific attitudes towards personally adopting recommended PA for DRR was notable. Aversion to dementia was universal and almost all participants valued avoiding, delaying, or slowing dementia. Most participants believed that reducing dementia risk would make PA worthwhile, although some were skeptical about likely effectiveness.
Personal salience perspectives were more varied, including about the need to reduce one’s own dementia risk and about the likely individual benefits of PA. Many participants either clearly or seemingly under-estimated individual dementia risk. Under-estimated risk often appeared linked to a lower commitment or urgency to reducing risk. In contrast, while a few participants (all of whom had limited DRR knowledge) linked awareness of being ‘at risk’ to hopelessness, it was described by others as motivating, including prompting formation of more urgent and specific intentions.
Some participants strongly linked personal attitudes to expectations for benefits other than DRR, particularly improving physical and mental health and opportunities for social connections, describing these as prompting more specific and urgent PA intentions, although potentially still insufficient to generate sustained behavior change on their own. Many participants also anticipated negative outcomes. These included discomfort; pain; injury; fatigue; embarrassment; or failure. These expectations were linked by many to diminished motivation and personal commitment. Some also linked these to fears of exacerbating mood or anxiety symptoms.
Finally, participants appeared to link both inaccurate personal risk appraisals and pessimistic outcome expectations to multiple factors, including past experiences; concern regarding research evidence gaps; generalizing the experiences of family and friends; and misunderstandings regarding the relative impact of genetic and modifiable risk factors.
Access to reliable, flexible resources can help overcome barriers
Many participants shared a wish for information and resources to support self-regulation. There was a strong preference for accessible and reliable information. Many described online sources as preferred, a notable difference to the previously emphasized sources of existing knowledge. Several also expressed caution about the reliability of online sources, such as only visiting news media or well-established government or health institution sites or seeking health professional confirmation and personalization for online-sourced recommendations. Participants described wanting: more information about research findings; guidance such as programs, picture, and video demonstrations; and specific information about how to adapt activities to accommodate physical health problems or disability.
Most participants sought tools to improve and support perceived accountability, describing a variety of potentially useful tools to improve self-monitoring of behavior and progress, and to feel accountable for enacting intentions. These all spoke to abilities to understand, monitor, and regulate individual behavior. Several mentioned the benefits of structured programs, but opinions were more mixed regarding tools for feedback: some felt they might help motivation or enacting intentions, but others suggested they would cause embarrassment and could prompt avoidance, appearing to link to themes highlighting emotional regulation and self-efficacy. Most participants referenced technology-based tools, including check-in or diary apps, email and SMS reminders, and regular or asynchronously accessed online classes. However, several noted that they would also like hard-copy versions of technology tools to be available.
Participants also sought strategies to help navigate barriers (or remove barriers that participants felt were too difficult to independently navigate). They identified needing help to adapt PA to accommodate injury or health problems, competing work and carer roles, bad weather, limited financial resources and COVID-19 restrictions. Access to adequate appropriate spaces and equipment, such as gyms, were sought by some participants. Others preferred PA at home, which, for a few, appeared linked to concerns about embarrassment and convenience.
Access to social opportunities for accountability and support
As with access to physical resources, the perceived benefits of a sense of social accountability were a prominent topic for participants. Several noted that group activities, support or supervision from a trusted health or exercise professional could generate a sense of accountability that helped overcome difficulties with initiation, self-monitoring and navigating barriers or competing roles. Some participants used social norms to both measure their own PA, and to subjectively appraise their dementia risk. The importance of social opportunities was also highlighted by comments from a few participants that sedentary behavior in social networks tended to, conversely, diminish individual motivation.
In addition to increasing perceived accountability, many participants described social interactions themselves as an important valued outcome of PA, and ‘social’ encouragement from peers or health professionals as helpful. This was linked by some to overcoming low confidence, anxiety, or fears of embarrassment. Support from health and exercise professionals was more specifically linked to overcoming both fears of exacerbating health problems or injury and uncertainty about adapting activities. A few participants explicitly differentiated between this support and health professional support for accountability.
Findings from literature review
From searches and consultation with relevant experts in the study team, we identified seven review papers [19, 20, 37, 52–55] and 17 primary studies [56–72] that reported adequate information to identify some or all BCT and PA intervention delivery modes used. Only three primary studies were specific to older adults [56, 64, 67] and only one review [19] and one primary study related to anxiety [72]. Few studies provided detailed information regarding BCTs used and fewer explicitly identified target MoAs. All studies described multiple BCTs.
Two review papers and two primary studies explicitly applied a theory or model [37, 52, 57, 59]. These were the Transtheoretical Model of Change (including motivational interviewing), Coleman’s Model (or Coleman’s Boat) and Self-Determination Theory.
BCTs reported across all studies linked to 18 out of the 26 different MoAs outlined in the Theory and Techniques Tool. These are summarized in Table 3 (see Supplementary Material 2 for all included BCTs and linked MoAs). Of these, knowledge, social influences, and beliefs about capabilities were targeted MoAs in all included studies. Skills, intentions, general attitudes, and goals were the next most commonly targeted MoAs. Specific attitudes towards the target behavior, motivation, feedback processes, behavioral regulation and environmental context and resources were also targeted by a majority of studies.
Table 3
Target MoAs of BCTs described by included studies
| Mechanism of Action (MoA) | Number of studies applying/recommending MoA | Studies |
| Knowledge | 24 | [19, 20, 37, 52–72] |
| Social influences | 24 | [19, 20, 37, 52–72] |
| Beliefs about capabilities | 24 | [19, 20, 37, 52–72] |
| Skills | 23 | [19, 20, 37, 52–67, 69–72] |
| Intentions | 23 | [19, 20, 37, 52–71] |
| General attitudes/beliefs | 23 | [19, 20, 37, 52–67, 69–72] |
| Goals | 22 | [19, 20, 37, 52–54, 56–71] |
| Attitude towards the behavior | 21 | [19, 20, 37, 52–66, 68, 69, 72] |
| Feedback processes | 20 | [19, 20, 37, 52, 53, 54–58, 60–64, 68–70, 72] |
| Motivation | 20 | [19, 20, 37, 52–58, 60, 62–64, 66–70, 72] |
| Behavioral regulation | 18 | [19, 20, 37, 52, 53, 56–59, 61, 64–70, 72] |
| Environmental context and resources | 18 | [19, 20, 37, 52–55, 57–60, 63–67, 70–72] |
| Norms/Subjective norms | 11 | [19, 37, 53, 54, 56–58, 60, 61, 65, 71] |
| Behavioral cueing | 11 | [37, 52, 54, 55, 58, 60, 63, 66, 67, 69, 70] |
| Beliefs about consequences | 10 | [19, 20, 37, 52, 53, 57, 66, 67–69] |
| Perceived susceptibility/vulnerability | 5 | [37, 52, 57, 68, 69] |
| Memory, attention, and decision processes | 4 | [37, 52, 66, 70] |
Knowledge: an awareness of the existence of something; social influences: interpersonal processes that can cause oneself to change one’s thoughts, feelings or behaviors; beliefs about capabilities: beliefs about one’s ability to successfully carry out a behavior; skills: an ability or proficiency acquired through practice; general attitudes/beliefs: evaluations of an object, person, group, issue or concept on a scale ranging from negative to positive; goals: mental representations of outcomes or end states that an individual wants to achieve; attitude towards the behavior: the general evaluations of the behavior on a scale ranging from negative to positive; feedback processes: processes through which current behavior is compared against a particular standard; motivation: processes relating to the impetus that gives purpose or direction to behavior and operates at a conscious or unconscious level; behavioral regulation: behavioral, cognitive and/or emotional skills for managing or changing behavior; environmental context and resources: aspects of a person’s situation or environment that discourage or encourage the behavior; norms: the attitudes held and behaviors exhibited by other people within a social group; subjective norms: one’s perceptions of what most other people within a social group believe and do; behavioral cueing: processes by which behavior is triggered from either the external environment, the performance of another behavior, or from ideas appearing in consciousness; beliefs about consequences: beliefs about the consequences of the behavior, including about what will be achieved and/or lost by undertaking a behavior; perceived susceptibility/vulnerability: perceptions of the likelihood that one is vulnerable to a threat; memory, attention and decision processes: ability to retain information, focus on aspects of the environment and choose between two or more alternatives.
Mapping and model development
There was strong convergence between interview themes, existing published findings, and COM-B system constructs. Most MoAs identified in the published literature mapped to a single interview theme and COM-B domain (Table 4), supporting the validity of identified themes.
Table 4
Map of interview themes, MoA identified from literature and COM-B components
| Interview themes | MoA from literature | COM-B component |
| Being informed to enable change | Knowledge Skills | Capability and Motivation |
| Individual attitudes and urgency for change | Beliefs about consequences General attitudes/beliefs Attitudes to the behavior Perceived susceptibility/vulnerability Motivation Intentions | |
| Skills and confidence to make and enact intentions | Beliefs about capabilities Skills Behavioral regulation Goals Memory, attention and decision-making processes Behavioral cueing | |
| Access to reliable, flexible resources | Environmental context and resources | Opportunity |
| Access to social opportunities | Social influences Norms Subjective norms |
Knowledge appeared key in both interviews and existing evidence. Required knowledge included conceptual knowledge about DRR and procedural knowledge (i.e., type, amount and ‘how to do’ the required activities). ‘Knowledge’ as a MoA from existing literature mapped clearly to the interview theme of being informed to enable change. We also mapped the ‘skills’ MoA from the literature review to this theme (in addition to skills and confidence to make and enact intentions) as it aligned with the emphasis on procedural knowledge from interview data.
Skills, attitudes, behavioral regulation, and resources (including social) were emphasized in both interviews and the published literature. Emotional regulation was not independently emphasized in the literature, in contrast to its prominence in interviews. This is notable as it appeared to have important links to PA self-efficacy and enacting intentions. Similarly, feedback processes were prominent in the literature reviewed but there were mixed perspectives regarding their benefits in interviews that again linked to emotional regulation and self-efficacy. The prominence of both highlight that these interacting constructs reflect key experiential factors of depression and anxiety.
Findings were notably complementary to COM-B in relation to self-efficacy and emotions. In interviews, both appeared linked to capabilities in addition to motivation (as described in the original model). Negative emotions, difficulties with emotional regulation and low confidence in psychological skills (to regulate emotions, to monitor behavior, and to break unhelpful habits in particular) were described as strongly influencing capabilities to turn intentions into action, particularly when engagement needed to adapt to health problems or other distractions and even when subjective knowledge and motivation were high.
Final model
Our final model comprised key MoAs for interventions to support people in mid- and later-life with both cognitive concerns and depression or anxiety to adopt PA. This is represented in Fig. 5 and described further below. The model illustrates key findings and specific targets for intervention relevant to each theme. COM-B constructs provided organization for themes, with the model demonstrating that MoAs related to capabilities, motivation, and opportunities all influence each other and, combined, contribute to behavior change.
Fig. 5
Integrated model of mechanisms of action for interventions to support adoption and maintenance of physical activity for cognitive health by middle-aged and older people living with cognitive concerns and depressive or anxiety symptoms.
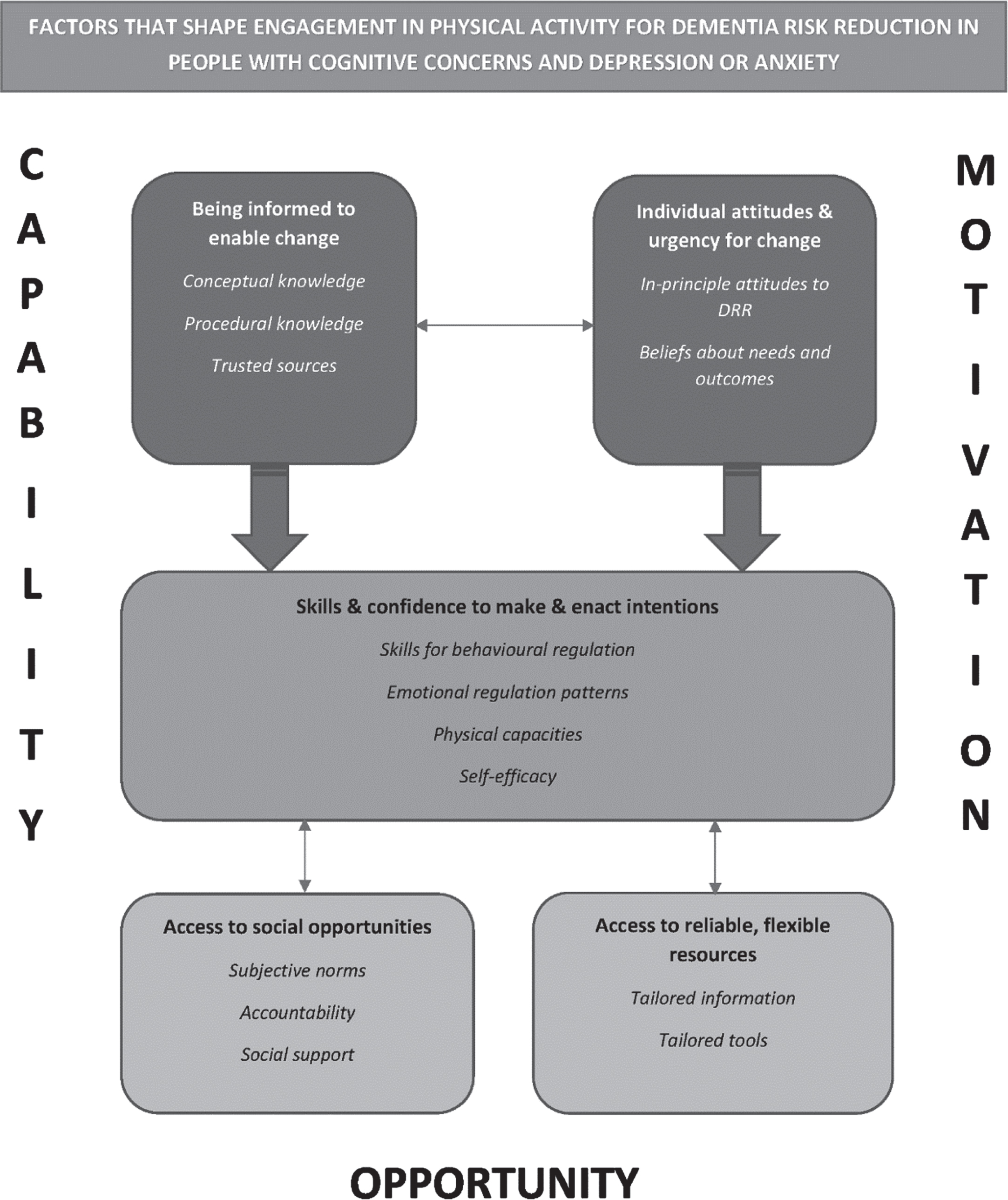
First, optimizing knowledge through trusted information will be key. This includes supporting both conceptual knowledge to enhance motivation and procedural knowledge to support effective change. While improved knowledge may be sufficient for behavior change in some, it is more likely that other change interventions will need to build on knowledge.
Second, general attitudes can support the formation of general intentions, but beliefs about both being at risk and being able to benefit from PA are important to facilitate specific intentions reflective of greater commitment to action. Further, addressing beliefs or fears of negative physical and mental health consequences may be particularly influential for generating specific intentions in this population.
Third, successful behavior change may be better supported when BCTs and technologies for improving knowledge and attitudes are complemented by others that focus on enacting intentions and social and physical resources. Skills in behavioral and emotional regulation could be vital to taking the steps to enacting and maintaining intentions, and to re-enacting them after periods of ‘relapse’. Strengthening confidence in the skills that individuals possess and supporting them through tools to mitigate impacts of cognitive difficulties (due to cognitive concerns or depressive or anxiety symptoms) may be key to leveraging their potential benefits.
For our target population, effective emotional regulation may be particularly crucial. Impaired emotional regulation and low confidence in emotional regulation could help explain how depression and anxiety can lead to poor uptake and maintenance of PA, including habitual inactivity, despite motivation and strong intentions. Emotional regulation and broader self-regulation skills also appear to be crucial to overcoming the physical and cognitive concerns that are common in this population and more difficult to modify. Finally, both social and physical resources can support emotional regulation. Social opportunities and resources to either build capacity and confidence, or to compensate for difficulties, may be particularly helpful. It is also important to note that, while the scope of this study means we refer largely to social opportunities and resources that can currently be accessed or developed, this aspect of the model has scope to be expanded to incorporate higher-level approaches addressing structural barriers and social determinants of health.
DISCUSSION
This study has developed a model to describe important MoAs through which PA interventions for cognitive health can effectively promote behavior change in people aged 45 years and older who already experience both cognitive concerns and depression or anxiety. Triangulating data sources and types in the development process supported validity and contextualized specific findings to optimally inform intervention development.
We found prominent convergent themes across each source of evidence. DRR understanding remains limited amongst this population, and increasing specific knowledge is vital for improved uptake. Further, we found that positive attitudes, based on beliefs about the salience and likely outcomes of individual behavior change, can help individuals to develop intentions and commit to change. The relatively high subjective reports of current levels of aerobic PA in participants also highlights the importance of knowledge and beliefs about salience. Given individuals commonly over-estimate PA levels [73], enabling more realistic appraisal of current PA may improve assessment of current risk and increase the personal salience of risk reduction. Importantly, we identified that capacities to regulate behavior and emotion, and confidence in these capacities may be particular vulnerabilities for this population. These may contribute to challenges converting intentions into action in the context of barriers such as physical health issues, but they could also be intervention targets that may enable individuals to realize intentions despite cognitive, emotional, and physical symptoms and changing contextual barriers. Finally, we found that access to appropriate social or physical resources can help individuals to overcome or accommodate capability gaps and that technology-based resources are also valued by this older population.
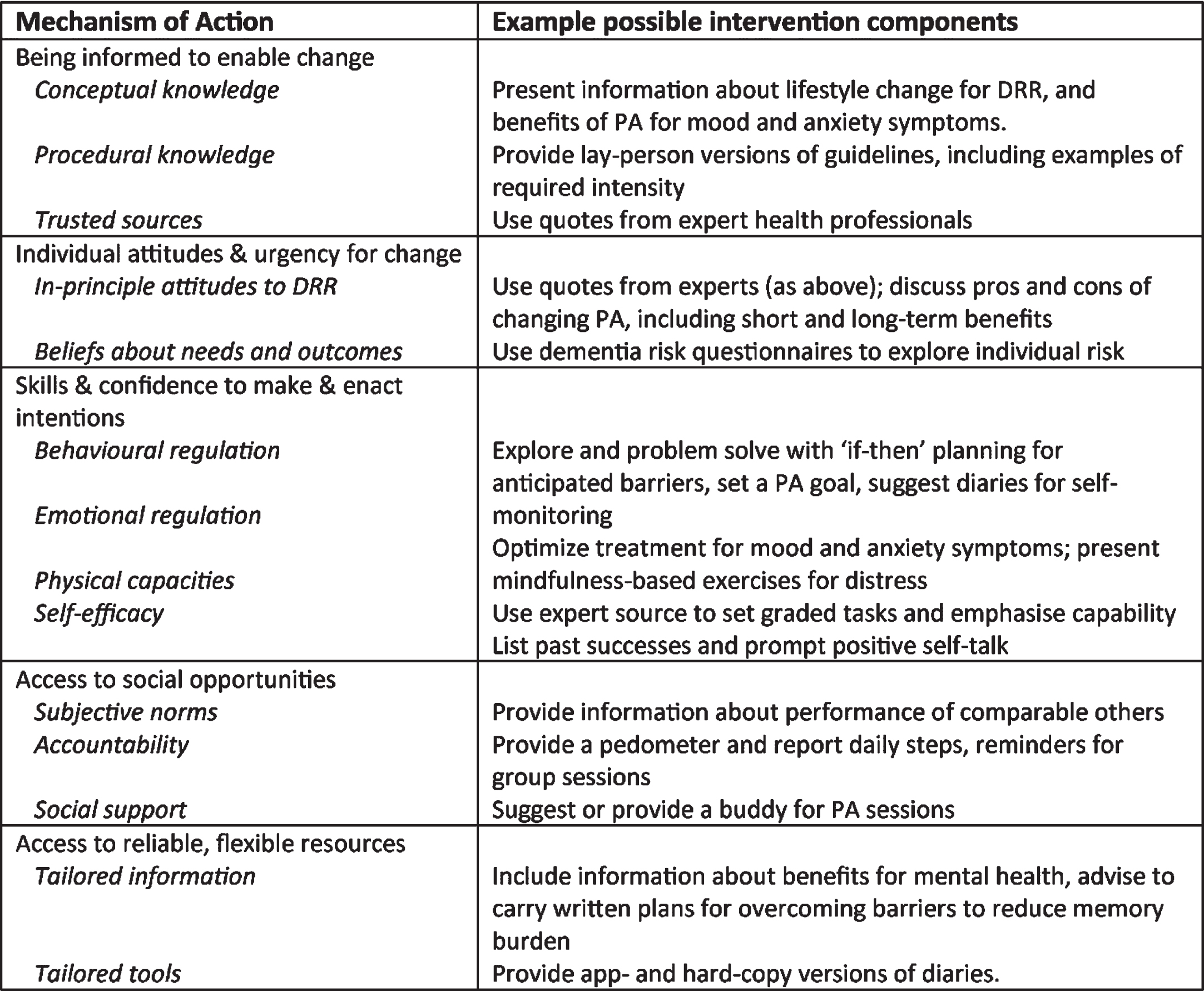
This model provides insights to inform, rather than direct, real-world intervention design. There are numerous ways of engaging individual MoAs and the most appropriate will depend upon intervention context. With these caveats in mind, some possible BCTs addressing the identified MoAs are shown in Fig. 6. Importantly, our findings also suggest that MoAs interact and build on each other. Hence, including complementary intervention components addressing multiple areas may substantially increase PA intervention engagement and effectiveness for DRR.
Fig. 6
Examples of possible intervention components addressing each identified MoA.
This study is the first to identify important MoAs for PA for DRR intervention specifically in this target population. Our findings build on existing evidence that people living with cognitive concerns, depression, and anxiety can all experience significant barriers to PA behavior change [8, 19, 27, 29]. Findings also extend existing knowledge by providing insights into the experiential factors involved in depression and anxiety combined with cognitive concerns, how these could contribute to barriers, and key MoAs for interventions to overcome barriers. Similar to models already published for DRR in the general population [33] and for PA in people with memory concerns alone [14, 36], we identified knowledge, attitudes, self-regulation, and social processes as important, but the current model placed greater emphasis on the roles of emotional regulation and confidence in capabilities for behavioral regulation. Identification of these specific MoAs is key to the delivery of tailored approaches in DRR.
Importantly, some MoAs (such as emotional regulation, planning, and adaptation capabilities) emphasized by our model have not previously been targeted or highlighted in general population DRR trials. Prior studies have tended to focus on increasing knowledge, goal setting, graded tasks, feedback, and social support [34, 35, 74]. Hence, the more specified understanding provided by our findings may help explain disappointing engagement for some groups in the past, reinforces calls for DRR intervention tailoring to target group needs, and provides critical support for optimizing tailoring and outcomes for our target population. This knowledge may also have broader future application in PA intervention design for diverse physical and mental health outcomes in people living with depression and anxiety, although additional data specific to different contexts will still be crucial.
While the purpose of this study was not to test the COM-B system or its constructs, our findings do indicate it is an appropriate model to support intervention design in this context. We found it provided an organizational framework without prompting analytic foreclosure. This was aided by our use of expert input for SSI domains, an initially inductive approach to thematic analysis, triangulation with diverse existing data and researcher reflexivity. Similarly, the main assumptions of COM-B were not likely to have undermined methodological integrity. In particular, the central assumption that engaging identified mechanisms underpinning behavior patterns can enable behavior change and the implied emphasis on individuals rather than broad socio-cultural-political contexts were in conceptual alignment with the context and objective of the study, namely, to inform design processes for a PA intervention focused on individuals [51]. We identified areas where our findings were subtly different to COM-B organization. Our findings also emphasized a relatively smaller number of MoAs within the main constructs. Both outcomes demonstrate the importance of in-depth and contextualized understanding to enable effective and efficient application of COM-B (and other theory) in real world intervention design and implementation.
The strengths of this study include the use of systematic methodology that balanced rigor and pragmatism. This means findings can be immediately applied to intervention design, iteratively developed, and incorporated into future research findings. Qualitative perspectives of individuals who are usually hard to reach for research work, in particular, facilitated nuanced findings that allowed more in-depth conceptual understanding.
While statistical representativeness and generalizability is not expected in qualitative research, it is notable that most interview participants were female, older (rather than middle-aged), highly educated, residing in a urban area and did not have significant objective cognitive impairment, despite subjective concerns. These characteristics may have inflected our findings as each could plausibly influence both pre-existing beliefs about PA and experiences of depression or anxiety that may impact on PA engagement, such as symptom patterns [75] or the extent of symptom response with PA [76]. Additional themes relevant to subgroups with low representation may not have been identified. However, this did not prohibit the study objective of developing nuanced insights regarding this complex topic. Importantly, the study did include some participants of different demographics, thematic saturation was reached and middle-aged and male participant responses contributed to all themes, supporting their validity. Further, triangulation of data with a large body of existing quantitative research is a well-established method to support validity. These methods also support the transferability of findings to the EXCEL intervention design or similar settings, although the sample characteristics may limit broader model generalizability.
A key limitation is that interviewer prompting may have directed some areas of emphasis. Again, the semi-structured nature of interviews was aligned with the pragmatic objective of the study and interviewer training mitigated risks of excessive direction, but other themes may have emerged with different qualitative methods. It is possible that new MoAs will be identified and needed for different contexts. Finally, while we used a rigorous approach to identifying BCTs and target MoAs from previous studies, reporting in included studies often lacked detail and we may not have identified all relevant BCTs or target MoAs.
This model can now be applied to support important future research in this field, particularly addressing similar gaps in understanding how to best tailor intervention design for key target groups with multiple needs. In particular, the model can be adapted to generate contextually specified understanding for individuals from culturally and linguistically diverse backgrounds and different healthcare contexts. Our critical review findings also support the need for future intervention trial reports to include mechanistic and behavioral outcomes to better understand how and why interventions do or do not work and support more efficient cumulative knowledge development in the field.
This study has developed the first model of important MoAs for PA intervention with specificity for people in mid- and later-life experiencing cognitive concerns and depression or anxiety, and for a DRR context. This can support the necessary intervention tailoring to optimize intervention outcomes for an important and overlooked at-risk group. It will help better direct intervention design efforts toward the needs of target populations. The model can also be easily and immediately incorporated into clinical settings to provide direction for clinicians, and for services considering program or resource development. Given the extensive established benefits of PA for people living with cognitive concerns and depression or anxiety, employing models such as this can better support individuals to capitalize on the potential it offers.
ACKNOWLEDGMENTS
We gratefully acknowledge the generous contribution of all study participants.
FUNDING
The EXCEL study was supported by the Australian Government’s Medical Research Future Fund (MRFF) as part of the Rapid Applied Research Translation program in conjunction with the Melbourne Academic Centre for Health, and the National Health and Medical Research Council Centre for Research Excellence in Cognitive Health (CRE 110579). EC was supported by a PhD Fellowship with the Maintain Your Brain Study. This study was funded by a National Health and Medical Research Council of Australia Dementia Research Team Grant (APP1095097). Participants in MYB were recruited from the 45 and Up Study (http://www.saxinstitute.org.au). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW; and partners: the National Heart Foundation of Australia (NSW Division); NSW Ministry of Health; NSW Government Family & Community Services –Ageing, Carers and the Disability Council NSW; and the Australian Red Cross Blood Service. The funding bodies had no role in the study.
CONFLICT OF INTEREST
Professor Kaarin Anstey, Dr. Terence Chong, and Assistant Professor Kay Cox are Editorial Board Members of this journal but were not involved in the peer-review process nor had access to any information regarding its peer-review.
All other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-221216.
REFERENCES
[1] | Livingston G , Huntley J , Sommerlad A , Ames D , Ballard C , Banerjee S , Brayne C , Burns A , Cohen-Mansfield J , Cooper C , Costafreda SG , Dias A , Fox N , Gitlin LN , Howard R , Kales HC , Kivimäki M , Larson EB , Ogunniyi A , Orgeta V , Ritchie K , Rockwood K , Sampson EL , Samus Q , Schneider LS , Selbæk G , Teri L , Mukadam N ((2020) ) Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 396: , 413–446. |
[2] | World Health Organization ((2019) ) Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines. World Health Organization, Geneva, Switzerland. |
[3] | Chong TW , Macpherson H , Schaumberg MA , Brown BM , Naismith SL , Steiner GZ , Nhmrc National Institute for Dementia Research DPSIG ((2021) ) Dementia prevention: The time to act is now. Med J Aust 214: , 302–304 e301. |
[4] | Santabarbara J , Lipnicki DM , Olaya B , Villagrasa B , Bueno-Notivol J , Nuez L , Lopez-Anton R , Gracia-Garcia P ((2020) ) Does anxiety increase the risk of all-cause dementia? An updated meta-analysis of prospective cohort studies. J Clin Med 9: , 1791. |
[5] | Wang SM , Han KD , Kim NY , Um YH , Kang DW , Na HR , Lee CU , Lim HK ((2021) ) Late-life depression, subjective cognitive decline, and their additive risk in incidence of dementia: A nationwide longitudinal study. PLoS One 16: , e0254639. |
[6] | Liew TM ((2019) ) Depression, subjective cognitive decline, and the risk of neurocognitive disorders. Alzheimers Res Ther 11: , 70. |
[7] | Kuring JK , Mathias JL , Ward L ((2020) ) Risk of dementia in persons who have previously experienced clinically-significant depression, anxiety, or PTSD: A systematic review and meta-analysis. J Affect Disord 274: , 247–261. |
[8] | Firth J , Siddiqi N , Koyanagi A , Siskind D , Rosenbaum S , Galletly C , Allan S , Caneo C , Carney R , Carvalho AF , Chatterton ML , Correll CU , Curtis J , Gaughran F , Heald A , Hoare E , Jackson SE , Kisely S , Lovell K , Maj M , McGorry PD , Mihalopoulos C , Myles H , O’Donoghue B , Pillinger T , Sarris J , Schuch FB , Shiers D , Smith L , Solmi M , Suetani S , Taylor J , Teasdale SB , Thornicroft G , Torous J , Usherwood T , Vancampfort D , Veronese N , Ward PB , Yung AR , Killackey E , Stubbs B ((2019) ) The Lancet Psychiatry Commission: A blueprint for protecting physical health in people with mental illness. Lancet Psychiatry 6: , 675–712. |
[9] | Burmester B , Leathem J , Merrick P ((2016) ) Subjective cognitive complaints and objective cognitive function in aging: A systematic review and meta-analysis of recent cross-sectional findings. Neuropsychol Rev 26: , 376–393. |
[10] | Chen C , Hu Z , Jiang Z , Zhou F ((2018) ) Prevalence of anxiety in patients with mild cognitive impairment: A systematic review and meta-analysis. J Affect Disord 236: , 211–221. |
[11] | Ismail Z , Elbayoumi H , Fischer CE , Hogan DB , Millikin CP , Schweizer T , Mortby ME , Smith EE , Patten SB , Fiest KM ((2017) ) Prevalence of depression in patients with mild cognitive impairment: A systematic review and meta-analysis. JAMA Psychiatry 74: , 58–67. |
[12] | Ma L ((2020) ) Depression, anxiety, and apathy in mild cognitive impairment: Current perspectives. Front Aging Neurosci 12: , 9. |
[13] | Martin E , Velayudhan L ((2020) ) Neuropsychiatric symptoms in mild cognitive impairment: A literature review. Dement Geriatr Cogn Disord 49: , 146–155. |
[14] | Chong TWH , Curran E , Ellis KA , Southam J , You E , Cox KL , Hill KD , Pond D , Dow B , Anstey KJ , Hosking D , Cyarto E , Lautenschlager NT ((2020) ) Physical activity for older Australians with mild cognitive impairment or subjective cognitive decline - A narrative review to support guideline development. J Sci Med Sport 23: , 913–920. |
[15] | Freberg E , Taglialatela G ((2022) ) Exercise as a potential therapeutic strategy to target the clinical link between depression and Alzheimer’s disease: A narrative review. J Alzheimers Dis 89: , 759–767. |
[16] | Anstey KJ , Ee N , Eramudugolla R , Jagger C , Peters R ((2019) ) A systematic review of meta-analyses that evaluate risk factors for dementia to evaluate the quantity, quality, and global representativeness of evidence. J Alzheimers Dis 70: , S165–S186. |
[17] | Yu JT , Xu W , Tan CC , Andrieu S , Suckling J , Evangelou E , Pan A , Zhang C , Jia J , Feng L , Kua EH , Wang YJ , Wang HF , Tan MS , Li JQ , Hou XH , Wan Y , Tan L , Mok V , Tan L , Dong Q , Touchon J , Gauthier S , Aisen PS , Vellas B ((2020) ) Evidence-based prevention of Alzheimer’s disease: Systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry 91: , 1201–1209. |
[18] | Ashdown-Franks G , Sabiston CM , Stubbs B ((2019) ) The evidence for physical activity in the management of major mental illnesses: A concise overview to inform busy clinicians’ practice and guide policy. Curr Opin Psychiatry 32: , 375–380. |
[19] | Chong TWH , Kootar S , Wilding H , Berriman S , Curran E , Cox KL , Bahar-Fuchs A , Peters R , Anstey KJ , Bryant C , Lautenschlager NT ((2022) ) Exercise interventions to reduce anxiety in mid-life and late-life anxiety disorders and subthreshold anxiety disorder: A systematic review. Ther Adv Psychopharmacol 12: , 20451253221104958. |
[20] | Schuch FB , Stubbs B ((2019) ) The role of exercise in preventing and treating depression. Curr Sports Med Rep 18: , 299–304. |
[21] | Stubbs B , Rosenbaum S , Vancampfort D , Ward PB , Schuch FB ((2016) ) Exercise improves cardiorespiratory fitness in people with depression: A meta-analysis of randomized control trials. J Affect Disord 190: , 249–253. |
[22] | Kandola A , Stubbs B (2020) Exercise and anxiety. In Physical exercise for human health, Xiao J, ed. Springer Nature, Singapore. |
[23] | Brown WJ , Moorhead GE , Marshall AL (2008) Choose Health: Be Active: A Physical Activity Guide for Older Australians. Commonwealth of Australia, Canberra, Australia. |
[24] | Lautenschlager NT , Cox K , Hill KD , Pond D , Ellis KA , Dow B , Hosking D , Chong T , You E , Curran E , Cyarto E , Southam J , Anstey KJ (2018) Physical Activity Guidelines for Older Australians with Mild Cognitive Impairment or Subjective Cognitive Decline. Dementia Collaborative Research Centres, Melbourne, Australia. |
[25] | Australian Institute of Health and Welfare (2018) Physical Activity Across the Life Stages. AIHW, Canberra. |
[26] | Howlett N , Trivedi D , Troop NA , Chater AM ((2019) ) Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl Behav Med 9: , 147–157. |
[27] | Coley N , Ngandu T , Lehtisalo J , Soininen H , Vellas B , Richard E , Kivipelto M , Andrieu S , Hatice F , HATICE, FINGER, and MAPT/DSA groups ((2019) ) Adherence to multidomain interventions for dementia prevention: Data from the FINGER and MAPT trials. Alzheimers Dement 15: , 729–741. |
[28] | Kulmala J , Rosenberg A , Ngandu T , Hemio K , Tenkula T , Hyytia A , Vienola M , Huhtamaki-Kuoppala M , Saarinen A , Korkki S , Laatikainen T , Solomon A , Kivipelto M ((2021) ) Facilitators and barriers to implementing lifestyle intervention programme to prevent cognitive decline. Eur J Public Health 31: , 816–822. |
[29] | Lautenschlager NT , Cox KL , Ellis KA ((2022) ) Physical activity forcognitive health: What advice can we give to older adults with subjective cognitive decline and mild cognitive impairment? Dialogues Clin Neurosci 21: , 61–68. |
[30] | Heffernan M , Andrews G , Fiatarone Singh MA , Valenzuela M , Anstey KJ , Maeder AJ , McNeil J , Jorm L , Lautenschlager NT , Sachdev PS , Ginige JA , Hobbs MJ , Boulamatsis C , Chau T , Cobiac L , Cox KL , Daniel K , Flood VM , Guerrero Y , Gunn J , Jain N , Kochan NA , Lampit A , Mavros Y , Meiklejohn J , Noble Y , O’Leary F , Radd-Vagenas S , Walton CC , Maintain Your Brain Collaborative T , Brodaty H ((2019) ) Maintain Your Brain: Protocol of a 3-year randomized controlled trial of a personalized multi-modal digital health intervention to prevent cognitive decline among community dwelling 55 to 77 year olds. J Alzheimers Dis 70: , S221–S237. |
[31] | Abraham C , Denford S ((2020) ) Design, implementation and evaluation of behavior change interventions: A ten-task guide. In The Handbook of Behavior Change, Hagger MS, Cameron LD, Hamilton K, Hanoken N, Lintunen T, eds. Cambridge University Press, UK. |
[32] | Michie S , Atkins L , West R (2014) The Behaviour Change Wheel: A Guide to Designing Interventions, Silverback Publishing, UK. |
[33] | Curran E , Chong TWH , Godbee K , Abraham C , Lautenschlager NT , Palmer VJ ((2021) ) General population perspectives of dementia risk reduction and the implications for intervention: A systematic review and thematic synthesis of qualitative evidence. PLoS One 16: , e0257540. |
[34] | Ngandu T , Lehtisalo J , Solomon A , Levälahti E , Ahtiluoto S , Antikainen R , Bäckman L , Hänninen T , Jula A , Laatikainen T , Lindström J , Mangialasche F , Paajanen T , Pajala S , Peltonen M , Rauramaa R , Stigsdotter-Neely A , Strandberg T , Tuomilehto J , Soininen H , Kivipelto M ((2015) ) A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 385: , 2255–2263. |
[35] | Richard E , Moll van Charante EP , Hoevenaar-Blom MP , Coley N , Barbera M , van der Groep A , Meiller Y , Mangialasche F , Beishuizen CB , Jongstra S , van Middelaar T , Van Wanrooij LL , Ngandu T , Guillemont J , Andrieu S , Brayne C , Kivipelto M , Soininen H , Van Gool WA ((2019) ) Healthy ageing through internet counselling in the elderly (HATICE): A multinational, randomised controlled trial. Lancet Digital Health 1: , e424–e434. |
[36] | Chong TWH , Curran E , Southam J , Cox KL , Bryant C , Goh AMY , You E , Ellis KA , Lautenschlager NT ((2022) ) Factors influencing long-termphysical activity maintenance: A qualitative evaluation of aphysical activity program for inactive older adults at risk ofcognitive decline: The INDIGO Follow-Up Study. J AlzheimersDis 89: , 1025–1037. |
[37] | Machaczek KK , Allmark P , Goyder E , Grant G , Ricketts T , Pollard N , Booth A , Harrop D , de-la Haye S , Collins K , Green G ((2018) ) A scoping study of interventions to increase the uptake of physical activity (PA) amongst individuals with mild-to-moderate depression (MMD). BMC Public Health 18: , 392. |
[38] | Wheeler AJ , Roennfeldt H , Slattery M , Krinks R , Stewart V ((2018) ) Codesigned recommendations for increasing engagement in structured physical activity for people with serious mental health problems in Australia. Health Soc Care Community 26: , 860–870. |
[39] | Avery N , Patterson S ((2020) ) Physical health in public mental health care: A qualitative study employing the COM-B model of behaviour to describe views and practices of Australian psychologists. Aust Psychol 53: , 302–312. |
[40] | Carney R , Bradshaw T , Yung AR ((2016) ) Physical health promotion for young people at ultra-high risk for psychosis: An application of the COM-B model and behaviour-change wheel. Int J Ment Health Nurs 25: , 536–545. |
[41] | Michie S , van Stralen MM , West R ((2011) ) The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement Sci 6: , 42. |
[42] | Ellis KA , Curran E , Cox KL , Chong TWH , Palmer VJ , Anstey KJ , Southam J , Coulson B , Moss F , Lautenschlager NT ((2020) ) Protocol of a clinical trial to implement physical activity for cognitive health in two aged persons’ mental health services in Melbourne: The EXCEL study. Alzheimers Dement 16: (Supp 10), e040704. |
[43] | Knopman DS , Roberts RO , Geda YE , Pankratz VS , Christianson TJ , Petersen RC , Rocca WA ((2010) ) Validation of the telephone interviewfor cognitive status-modified in subjects with normal cognition,mild cognitive impairment, or dementia. Neuroepidemiology 34: , 34–42. |
[44] | Lovibond SH , Lovibond PF (1995) Manual for the Depression Anxiety Stress Scales 2nd Edn, Psychology Foundation, Sydney, Australia. |
[45] | Norton K , Coombes J , Parker R , Williams A , Hobson-Powell A ((2012) ) New Australian standard for adult pre-exercise screening. Sport Health 30: , 12–18. |
[46] | Michie S , Richardson M , Johnston M , Abraham C , Francis J , Hardeman W , Eccles MP , Cane J , Wood CE ((2013) ) The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann Behav Med 46: , 81–95. |
[47] | Johnston M , Carey RN , Connell Bohlen LE , Johnston DW , Rothman AJ , de Bruin M , Kelly MP , Groarke H , Michie S ((2021) ) Development of an online tool for linking behavior change techniques and mechanisms of action based on triangulation of findings from literature synthesis and expert consensus. Transl Behav Med 11: , 1049–1065. |
[48] | Carey RN , Connell LE , Johnston M , Rothman AJ , de Bruin M , Kelly MP , Michie S ((2019) ) Behavior change techniques and their mechanisms of action: A synthesis of links described in published intervention literature. Ann Behav Med 53: , 693–707. |
[49] | QSR International Pty Ltd (2018) NVivo (Version 12), https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home |
[50] | Braun V , Clarke V ((2006) ) Using thematic analysis in psychology. Qual Res Psychol 3: , 77–101. |
[51] | Braun V , Clarke V ((2021) ) Thematic Analysis: A Practical Guide, Sage Publications Ltd, UK. |
[52] | Knapen J , Vancampfort D , Moriën Y , Marchal Y ((2015) ) Exercise therapy improves both mental and physical health in patients with major depression. Disabil Rehabil 37: , 1490–1495. |
[53] | Murri MB , Ekkekakis P , Menchetti M , Neviani F , Trevisani F , Tedeschi S , Latessa PM , Nerozzi E , Ermini G , Zocchi D , Squatrito S , Toni G , Cabassi A , Neri M , Zanetidou S , Amore M ((2018) ) Physical exercise for late-life depression: Effects on symptom dimensions and time course. J Affect Disord 230: , 65–70. |
[54] | Stanton R , Reaburn P ((2014) ) Exercise and the treatment of depression: A review of the exercise program variables. J Sci Med Sport 17: , 177–182. |
[55] | Stubbs B , Vancampfort D , Rosenbaum S , Ward PB , Richards J , Soundy A , Veronese N , Solmi M , Schuch FB ((2016) ) Dropout from exercise randomized controlled trials among people with depression: A meta-analysis and meta regression. J Affect Disord 190: , 457–466. |
[56] | Belvederi Murri M , Amore M , Menchetti M , Toni G , Neviani F , Cerri M , Rocchi MB , Zocchi D , Bagnoli L , Tam E , Buffa A , Ferrara S , Neri M , Alexopoulos GS , Zanetidou S ((2015) ) Physical exercise for late-life major depression. Br J Psychiatry 207: , 235–242. |
[57] | Callaghan P , Khalil E , Morres I , Carter T ((2011) ) Pragmatic randomised controlled trial of preferred intensity exercise in women living with depression. BMC Public Health 11: , 465. |
[58] | Carneiro LS , Fonseca AM , Vieira-Coelho MA , Mota MP , Vasconcelos-Raposo J ((2015) ) Effects of structured exercise and pharmacotherapy vs. pharmacotherapy for adults with depressive symptoms: A randomized clinical trial. J Psychiatr Res 71: , 48–55. |
[59] | Chalder M , Wiles NJ , Campbell J , Hollinghurst SP , Haase AM , Taylor AH , Fox KR , Costelloe C , Searle A , Baxter H , Winder R , Wright C , Turner KM , Calnan M , Lawlor DA , Peters TJ , Sharp DJ , Montgomery AA , Lewis G ((2012) ) Facilitated physical activity as a treatment for depressed adults: Randomised controlled trial. BMJ 344: , e2758. |
[60] | Danielsson L , Papoulias I , Petersson EL , Carlsson J , Waern M ((2014) ) Exercise or basic body awareness therapy as add-on treatment for major depression: A controlled study. J Affect Disord 168: , 98–106. |
[61] | Doose M , Ziegenbein M , Hoos O , Reim D , Stengert W , Hoffer N , Vogel C , Ziert Y , Sieberer M ((2015) ) Self-selected intensity exercise in the treatment of major depression: A pragmatic RCT. Int J Psychiatry Clin Pract 19: , 266–275. |
[62] | Gujral S , Aizenstein H , Reynolds CF , 3rd, Butters MA , Grove G , Karp JF , Erickson KI ((2019) ) Exercise for depression: A feasibility trial exploring neural mechanisms. Am J Geriatr Psychiatry 27: , 611–616. |
[63] | Kerling A , Tegtbur U , Gützlaff E , Kück M , Borchert L , Ates Z , von Bohlen A , Frieling H , Hüper K , Hartung D , Schweiger U , Kahl KG ((2015) ) Effects of adjunctive exercise on physiological and psychological parameters in depression: A randomized pilot trial. J Affect Disord 177: , 1–6. |
[64] | Kerse N , Hayman KJ , Moyes SA , Peri K , Robinson E , Dowell A , Kolt GS , Elley CR , Hatcher S , Kiata L , Wiles J , Keeling S , Parsons J , Arroll B ((2010) ) Home-based activity program for older people with depressive symptoms: DeLLITE–a randomized controlled trial. Ann Fam Med 8: , 214–223. |
[65] | La Rocque CL , Mazurka R , Stuckless TJR , Pyke K , Harkness KL ((2021) ) Randomized controlled trial of bikram yoga and aerobic exercise for depression in women: Efficacy and stress-based mechanisms. J Affect Disord 280: , 457–466. |
[66] | Mota-Pereira J , Silverio J , Carvalho S , Ribeiro JC , Fonte D , Ramos J ((2011) ) Moderate exercise improves depression parameters in treatment-resistant patients with major depressive disorder. J Psychiatr Res 45: , 1005–1011. |
[67] | Pfaff JJ , Alfonso H , Newton RU , Sim M , Flicker L , Almeida OP ((2014) ) ACTIVEDEP: A randomised, controlled trial of a home-based exercise intervention to alleviate depression in middle-aged and older adults. Br J Sports Med 48: , 226–232. |
[68] | Soucy I , Provencher M , Fortier M , McFadden T ((2017) ) Efficacy of guided self-help behavioural activation and physical activity for depression: A randomized controlled trial. Cogn Behav Ther 46: , 493–506. |
[69] | Szuhany KL , Otto MW ((2020) ) Efficacy evaluation of exercise as an augmentation strategy to brief behavioral activation treatment for depression: A randomized pilot trial. Cogn Behav Ther 49: , 228–241. |
[70] | Trivedi MH , Greer TL , Church TS , Carmody TJ , Grannemann BD , Galper DI , Dunn AL , Earnest CP , Sunderajan P , Henley SS , Blair SN ((2011) ) Exercise as an augmentation treatment for nonremitted major depressive disorder: A randomized, parallel dose comparison. J Clin Psychiatry 72: , 677–684. |
[71] | Uebelacker LA , Kraines M , Broughton MK , Tremont G , Gillette LT , Epstein-Lubow G , Abrantes AM , Battle C , Miller IW ((2017) ) Perceptions of hatha yoga amongst persistently depressed individuals enrolled in a trial of yoga for depression. Complement Ther Med 34: , 149–155. |
[72] | Gordon BR , McDowell CP , Lyons M , Herring MP ((2020) ) Resistance exercise training for anxiety and worry symptoms among young adults: A randomized controlled trial. Sci Rep 10: , 17548. |
[73] | Prince SA , Adamo KB , Hamel M , Hardt J , Connor Gorber S , Tremblay M ((2008) ) A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int J Behav Nutr Phys Activity 5: , 56–70. |
[74] | van Charante EPM , Richard E , Eurelings LS , van Dalen J-W , Ligthart SA , van Bussel EF , Hoevenaar-Blom MP , Vermeulen M , van Gool WA ((2016) ) Effectiveness of a 6-year multidomain vascular care intervention to prevent dementia (preDIVA): A cluster-randomised controlled trial. Lancet 388: , 797–805. |
[75] | Marcus SM , Kerber KB , Rush AJ , Wisniewski SR , Nierenberg A , Balasubramani GK , Ritz L , Kornstein S , Young EA , Trivedi MH ((2008) ) Sex differences in depression symptoms in treatment-seeking adults: Confirmatory analyses from the Sequenced Treatment Alternatives to Relieve Depression study. Compr Psychiatry 49: , 238–246. |
[76] | Zhang J , Yen ST ((2015) ) Physical activity, gender difference, and depressive symptoms. Health Serv Res 50: , 1550–1573. |


