
Photobiomodulation for Hypertension and Alzheimer’s Disease
Abstract
Although the cause(s) of Alzheimer’s disease in the majority of cases remains elusive, it has long been associated with hypertension. In animal models of the disease, hypertension has been shown to exacerbate Alzheimer-like pathology and behavior, while in humans, hypertension during mid-life increases the risk of developing the disease later in life. Unfortunately, once individuals are diagnosed with the disease, there are few therapeutic options available. There is neither an effective symptomatic treatment, one that treats the debilitating cognitive and memory deficits, nor, more importantly, a neuroprotective treatment, one that stops the relentless progression of the pathology. Further, there is no specific preventative treatment that offsets the onset of the disease. A key factor or clue in this quest for an effective preventative and therapeutic treatment may lie in the contribution of hypertension to the disease. In this review, we explore the idea that photobiomodulation, the application of specific wavelengths of light onto body tissues, can reduce the neuropathology and behavioral deficits in Alzheimer’s disease by controlling hypertension. We suggest that treatment with photobiomodulation can be an effective preventative and therapeutic option for this neurodegenerative disease.
INTRODUCTION
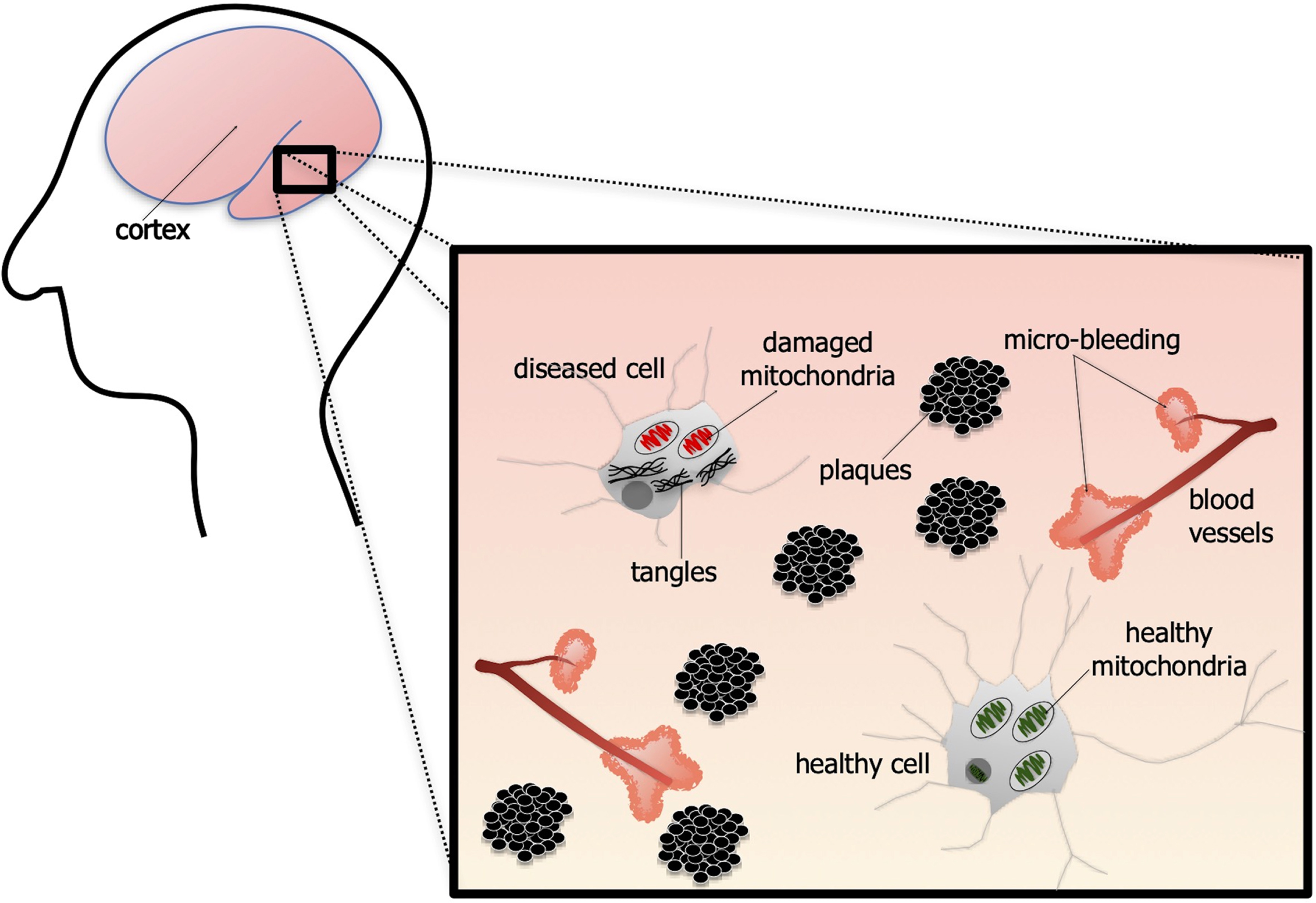
Alzheimer’s disease (AD) is a brain disorder that involves a progressive loss of memory, cognition, and self-control, the so-called executive brain functions. It affects mainly those entering older age (>65 years); in fact, age is the major risk factor of the disease [1, 2]. The devastating symptoms arise after a large number of neurons across the brain degenerate. These dying neurons have a number of distinct features (Fig. 1). Intracellularly, neurons develop neurofibrillary tangles, made up mainly of hyperphosphorylated tau protein, that disrupt normal cell function and survival. There are also problems with glucose metabolism that will eventually lead to damage and dysfunction of the “engine room” of the cells, namely the mitochondria [3]; further, there are deficits evident of the intracellular clearance system, for example of proteins and glucoconjugates that involve small organelles called lysosomes. In addition to these intracellular features, there are also many extracellular structures, made up of aggregations or plaques of amyloid-β (Aβ) protein, scattered across the brain, particularly within the memory areas [4–7]. Finally, there is evidence of vascular pathology. In particular, there are sites of micro-bleeding across the brain, many of which are associated with the Aβ plaques [8–12].
Fig. 1
Schematic diagram of the pathology associated with alzheimer’s disease. The brain is characterized by neurons containing intracellular neurofibrillary tangles, made up of tau protein. The mitochondria are damaged and neurons become dysfunctional. There are also many extracellular aggregations of amyloid-ß plaques. Finally, there is much vascular pathology, with many sites of micro-bleeding across the brain. Note that, although not depicted here, the majority of the plaques found across the brain are associated with sites of micro-bleeding.
In the sections that follow, we will examine briefly the suspected causes and mechanisms that underpin AD, focusing on the idea that hypertension and dysfunction of the vascular system may be central to the disease process. Next, we consider the current treatment options and preventative measures available for patients. We will then introduce the method of photobiomodulation, the use of red to near infrared light (∼λ= 600–1300 nm) on body tissues, and consider its beneficial effects on cells and on the vascular system and hypertension [13]. Finally, we will propose that photobiomodulation can form an effective preventative and therapeutic treatment option for patients by controlling hypertension.
THE CAUSES AND MECHANISMS: A FOCUS ON THE VASCULAR SYSTEM
Over the years, many hypotheses as to the causes and mechanisms underpinning the pathology associated with AD have been proposed and debated [1–7, 14]. Briefly, these include suggestions that the primary driver of the neuronal dysfunction and death, either by genetic mutation or by factors unknown, is either the accumulation of Aβ, the formation and self-propagation of tau protein and/or the dysfunction of mitochondria and/or lysosomes. Unfortunately, each one of these hypotheses has been associated with problems, in particular, in the development of a curative therapy [15, 16], with none being able to fully account for all the features of the disease [4–7].
Vascular pathology and hypertension
One of the first hypotheses of the initial causes of dementia and AD, and a major focus of this review, centers on vascular pathology and cerebral hypoperfusion [17, 18]. This process may trigger the development of Aβ plaques, tau assemblies, mitochondrial and lysosome dysfunction, and ultimately neuronal death. There is evidence of cerebral micro-bleeding across the capillary-bed, together with damage to the capillary endothelium and blood-brain barrier [9, 19–21]. Further, from postmortem material, a majority of patients diagnosed with AD ( 90%) have been found to have considerable vascular pathology [18].
Hypertension has long been considered to be a major cause of this vascular pathology; it is also considered to be a strong risk factor for the development of AD [22–24]. Many studies have reported that systolic hypertension, as well as overall variability in blood pressure, is associated with memory impairment and development of AD [22, 25–30]. This increase in blood pressure leads to damage to the cerebral microcirculation and arterial stiffness [31], inducing ischemia, disruptions to the blood-brain barrier, loss of neuronal function and an increase in Aβ expression [32–35]. There are many factors that may contribute to hypertension, including alterations of the renin– angiotensin– aldosterone system or autonomic nervous system, an increase in salt intake, obesity, and insulin resistance [36–38]. The renin– angiotensin– aldosterone system is a key regulator of blood volume and systemic vascular resistance. Unlike the baroreceptor reflex that responds to acute changes in blood pressure, the renin– angiotensin– aldosterone is generates more chronic alterations. The major compounds, namely renin, angiotensin II, and aldosterone, work together to raise blood pressure in response to various factors, including low blood pressure and/or salt levels [39–41]. However, it should be noted that, as with most hypotheses associated with neurodegenerative disease, the link between cognitive decline and hypertension has been subject to some debate over the years. While many studies have indicated increased cognitive impairment risk with hypertension (see above), other studies have suggested less of an association [26, 42, 43]. The timeline of hypertension may explain this discrepancy; in general, subjects with chronic hypertension over a period greater than ten years appear to have a stronger risk of cognitive decline later in life [44, 45].
Further to this debate, many clinical studies have reported that medications aimed to reduce hypertension lead to a lower incidence of dementia and AD [46, 47]. A recent meta-analysis containing fourteen international studies have highlighted considerable cognitive enhancement with blood-brain barrier-crossing renin-angiotensin drugs [48]. In addition, there is evidence in transgenic mouse models of the disease (APP/PS1, 3xTgAD) that hypertension can exacerbate the behavioral deficits and neuropathology of AD. For example, hypertensive APP/PSI mice develop an earlier cognitive deficit, together with an increase in both Aβ plaques and levels of soluble Aβ in the brain and plasma when compared to normotensive APP/PSI mice. The hypertensive APP/PSI mice also have considerably more vascular pathology (e.g., reduced density of microvessels) than the normotensive APP/PSI mice [49]. In the 3xTgAD mouse model, similar patterns have been reported, with experimentally-induced hypertension triggering an acceleration of Alzheimer-like pathology, microglial activation and leakage of the blood-brain barrier [50]. In addition, several authors have tested the efficacy of various drugs, in particular RB150 [51], in controlling hypertension in the 3xTgAD mouse model, with some promisingoutcomes [52].
It should be noted that vascular pathology and hypertension have been found in other types of neurodegenerative disease, not just AD. For example, in patients with Parkinson’s disease, there are reports of damage to the capillary endothelium and blood-brain barrier in the basal ganglia together with some fluctuation in blood pressure, including nocturnal hypertension [53, 54].
Taken all together, hypertension can lead to vascular pathology, altering the structure and density of cerebral blood vessels. This process can be disruptive to the mechanisms that assure an adequate blood supply to the brain, leading to cerebral hypoperfusion and potentially dementia and AD [22].
CURRENT TREATMENT OPTIONS
There are few effective treatment options available for patients with AD [55]. Some patients appear to respond to a newly approved therapy that aims to remove the Aβ plaques from the brain, while others gain some benefit with the use of acetylcholinesterase inhibitors, that suppress the breakdown of acetylcholine, and N-methyl-d-aspartate receptor antagonists, that helps prevent neurotoxicity in the brain [15, 56]. However, a number of patients do not respond to these treatments, and many suffer severe side effects. In essence, there is no currently available, broad range treatment option that stops or even slows the neuronal death (i.e., a neuroprotective treatment), although several experimental therapies have been suggested [57, 58]. The disease progresses relentlessly, and neurons continue to degenerate across the brain. Further, there is no treatment that even treats effectively the symptoms of the disease, namely the decline in memory, cognition, and self-control [59]. Indeed, the greatest fear for most people entering older age is that they will be diagnosed with AD and that there would be nothing that can be done about it.
In terms of prevention, a number of measures, albeit largely not specific for AD, have been suggested over the years, including, to do more exercise, be cognitively active, eat a Mediterranean diet, reduce both alcohol intake and obesity, and stop smoking [1, 7]. These measures can also help maintain a healthy blood pressure, controlling hypertension. In addition, and relevant to this review, suggestions have been made, based on evidence from both humans and animal models, that controlling hypertension can be an effective means to offset the onset of the disease, together with limiting its severity (see above). Hence, a key to a better and more efficient treatment for AD may lie in addressing the control of hypertension.
PHOTOBIOMODULATION: THE LIGHT
In this context, there is a new treatment option that has been receiving considerable interest across the clinical, scientific, and wider community. This treatment is known as photobiomodulation, the use of red to near infrared light (∼λ= 600–1300 nm) on body tissues [60]. It has been shown to be beneficial in many animal models of disease, from Parkinson’s disease [61] to stroke [62] and from traumatic brain injury [63] to retinal disease [64] and multiple sclerosis [65], it has an impeccable safety record, with little or no evidence of side effects or toxicity on body cells and the devices are easy to use and inexpensive [60]. In the sections that follow, the mechanisms of photobiomodulation are considered, together with its impact on the vascular system, hypertension, and AD.
The light mechanisms: direct and indirect stimulation
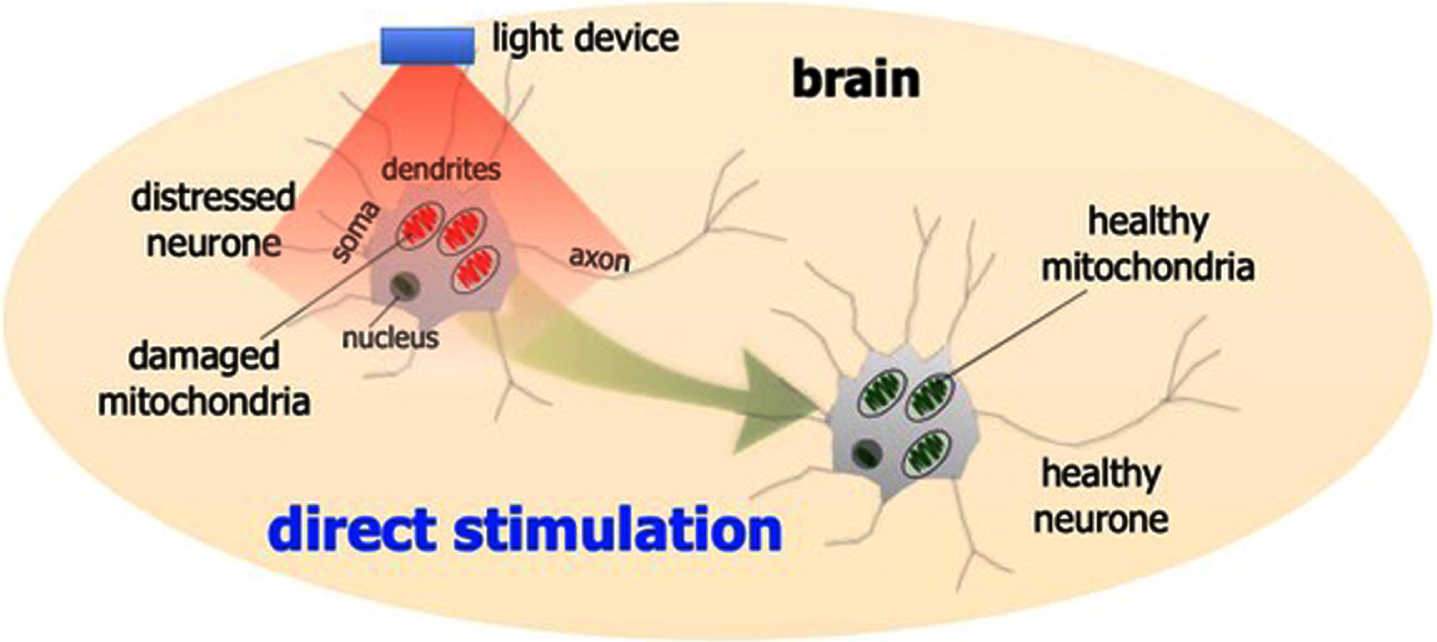
The precise mechanisms used by photobiomodulation to achieve beneficial outcomes are not entirely clear, but two have been suggested, namely direct and indirect stimulation [66, 67]. For direct stimulation, photobiomodulation has to fall directly on the neurons (Fig. 2). This stimulates the activity of the mitochondria, by being absorbed by a photoacceptor (e.g., cytochrome oxidase c and/or interfacial water), whose primary function is to provide energy for the cells that drive many intrinsic functions. This process leads to a healthier cell, with the expression of various functional and protective genes that make the cell not only function better, but make it more resistant to distress and disease [60]. Many studies have also reported that photobiomodulation promotes many other beneficial outcomes, such as triggering neurogenesis and synaptogenesis, as well as reducing inflammation [60, 68–72].
Fig. 2
Schematic diagram outlining the direct photobiomodulation stimulation. Photobiomodulation stimulates the mitochondria to produce more energy. This process leads to a healthier cell, with the expression of various functional and protective genes that make the cell not only function better, but make it more resistant to distress and disease.
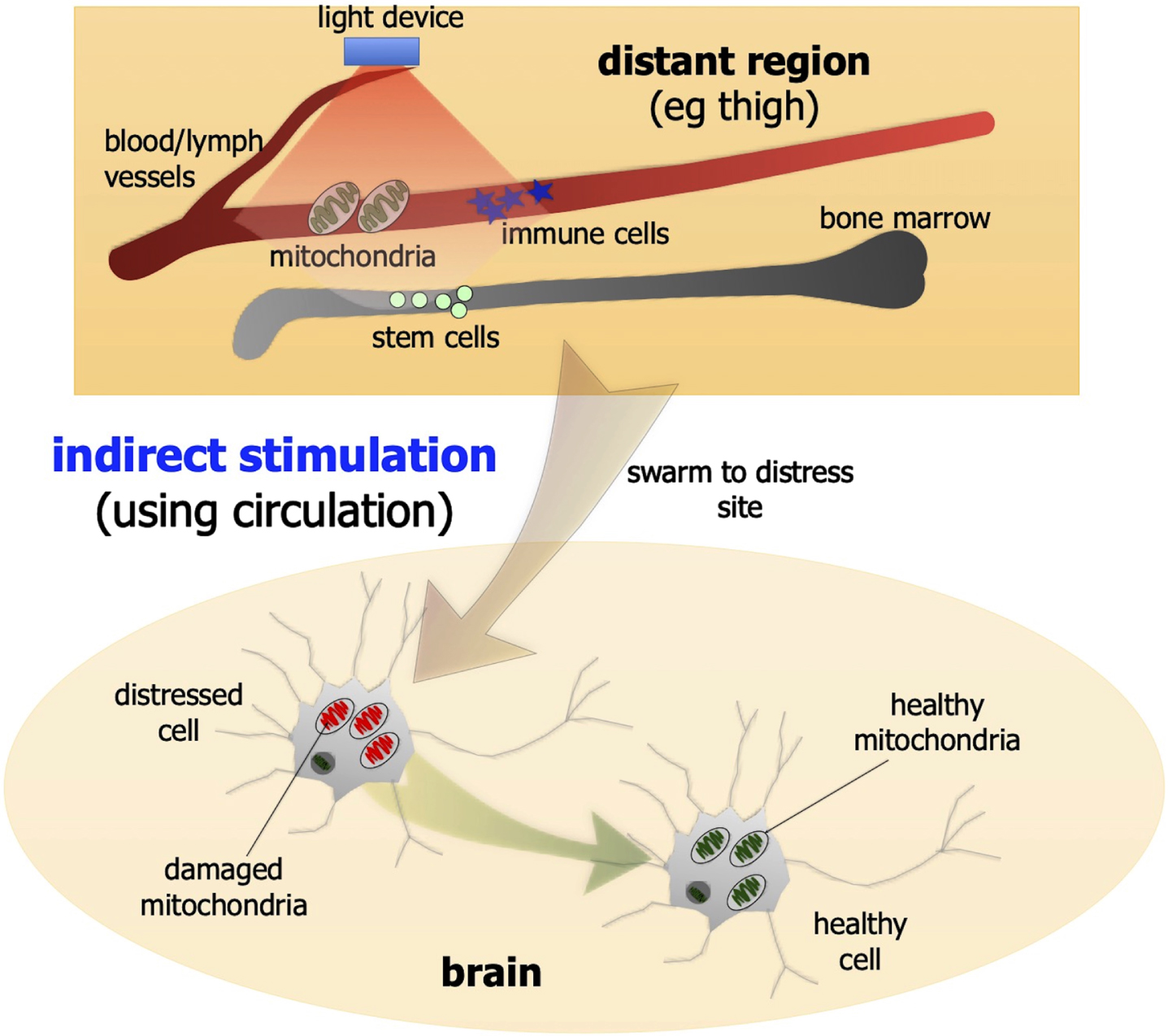
In addition to direct stimulation, photobiomodulation has been shown, quite remarkably, to be beneficial to neuronal function and survival even when it is applied to a more distant or remote location; that is, when it is not applied directly to the neurons (Fig. 3). This indirect stimulation is thought to activate circulating cells or molecules, or even free-floating mitochondria, within the cardiovascular or lymphatic systems that then leads to an increase in overall mitochondrial activity, in a similar fashion to the direct stimulation described above, in the distressed neurons located in the brain. The indirect stimulation, although offering neuroprotection, is less effective than direct application [66, 67].
Fig. 3
Schematic diagrams outlining the indirect photobiomodulation stimulation. Photobiomodulation has been shown to be beneficial to neurons when it is applied to a more distant or remote location. For example, when photobiomodulation is applied to the thigh, it may activate circulating cells, molecules, or free-floating mitochondria within the cardiovascular or lymphatic systems that then leads to an improved survival and function of distressed neurons located in the brain.
Lights on the vascular system and hypertension
Photobiomodulation has also been shown to have a direct effect on the vascular system. There is evidence that photobiomodulation offsets the degeneration and leakage of retinal capillaries in animal models of diabetes [73] and in the striatum and brainstem of a mouse model of Parkinson’s disease [74]. Further, photobiomodulation has been reported to induce the release of nitric oxide from cells, which triggers the vasodilation of nearby blood vessels, increasing blood (and lymphatic) flow [60, 75]. In addition to these studies, several groups have indicated an effect of photobiomodulation on the vascular system and cerebral blood flow. Photobiomodulation has been shown to improve endothelial dysfunction [76], influence the levels of angiogenic protein (e.g., vascular endothelial growth factor), that prompts capillary-like structure formation [63, 68], together with cerebral hemodynamic and uric acid levels [77], both of which are risk factors for the development of hypertension. There are also indications that photobiomodulation can increase oxygenated hemoglobin and oxidized cytochrome c oxidase levels [78], as well as restoring capillary blood supply and stimulating the microcirculation in Parkinson’s disease [79]. In AD patients, and in a patient suffering persistent vegetative state, photobiomodulation has been reported to increase cerebral blood flow [80–82]. In patients with major depressive disorder, photobiomodulation induces an improvement in diastolic blood pressure and a better cerebral blood flow, together with reductions in anxiety and depressive scores [83, 84].
There is also recent evidence in various experimental animal models that photobiomodulation reduces hypertension. In one model, involving constriction of the renal artery, photobiomodulation generates a long-lasting hypotensive effect after a device was implanted within the abdominal aorta. This effect is thought to be prompted by a photobiomodulation-induced vasodilation after a release of nitric oxide [85]. In another model of hypertension, involving an implantation of a cannula into the femoral artery, photobiomodulation applied externally over the abdomen reduced blood pressure considerably, together increasing serum levels of nitric oxide [86, 87].
Lights on Alzheimer’s disease
There are many studies, mainly on animal models and but also on patients, reporting that photobiomodulation is effective in AD. In animal models, that include different types of transgenic or Aβ-induced models, photobiomodulation has been shown to reduce Aβ plaques and aggregations, neurofibrillary tangles of hyperphosphorylated tau protein, synaptic vulnerability, gliosis, inflammation and oxidative stress, and increase in neurogenesis, mitochondrial function, and ATP levels (APP/PS1 model [88–93]; TASTPM model [94]; K369I model [89, 90]; Tg2576 model [95]; Aβ-induced model [96–98]; 5xTg model [99]; hTau and 3xTg models [100]). In addition, after internalization of Aβ into human neuroblastoma cells, photobiomodulation has been shown to increase ATP levels and cell number, while reducing Aβ aggregates [101]. When applied to normal mice, photobiomodulation prompts a much faster clearance of Aβ out of the brain and into the lymphatic system [75]. Finally, there are also some very early, encouraging observations in AD patients that photobiomodulation improves cognition [81, 102–104] and the functional connectivity of different areas of the brain [82].
From these previous studies, there are two key and relevant issues worthy of further comment. First, in both the rodent models and patients, photobiomodulation was applied transcranially. Many previous studies have reported that light can penetrate up to 30–50 mm of body tissue; in general, the longer the wavelength then the greater the penetration [60, 67, 105, 106]. In rodents, where the distances between the scalp and the most ventral areas of the brain are relatively short (5–10 mm), photobiomodulation applied in this way can reach and influence all regions of the brain directly. In addition, transcranial photobiomodulation can reach the many cerebral and scalp blood and lymphatic vessels and hence influence circulatory mitochondria, cells, and molecules. In humans, where the distances are much greater (80–100 mm), transcranial photobiomodulation can still reach the superficial areas of the cerebrum where much of the AD pathology is located, namely the cortex (10–15 mm) [66, 67]. As with the rodents, transcranial photobiomodulation in humans can also reach the cerebral and scalp blood and lymphatic vasculature. Hence, in both rodents and humans, transcranial photobiomodulation, by reaching large areas of brain together with blood and lymph vessels, can impart beneficial outcomes by both direct and indirect stimulation (see above). It should be noted that in one study in mice, beneficial outcomes were achieved after photobiomodulation was applied across the abdomen only, indicating that indirect stimulation by itself can be effective in AD [96].
Second, in all of these previous studies on animal models, photobiomodulation was started either at the onset, or well after the onset, of the first behavioral deficits and/or pathology [88–100]. This approach is largely in line with the clinical reality of the disease, where patients are treated after the emergence of the first symptoms. However, for a preventative approach, it would be more instructive to treat animals well before the onset of pathology and behavioral signs. In one study, using a mouse model of ageing (CD1), a preventative approach was used and improvements were noted in working memory [107]. Although these findings are encouraging, this was not a model of AD.
PHOTOBIOMODULATION, HYPERTENSION, AND ALZHEIMER’S DISEASE: AN HYPOTHESIS AND A POSSIBLE TREATMENT APPROACH
When considering all this information, principally from animal models, we would like to highlight three key issues, that:
(1) photobiomodulation reduces the pathology and behavioral deficits in AD when applied directly onto the head or body;
(2) photobiomodulation can reduce hypertension and vascular pathology when applied to blood vessels, and;
(3) hypertension exacerbates the neuropathology and behavioral deficits of AD.
Taking these three key issues together, we hypothesize that photobiomodulation, by controlling hypertension, can be an effective therapy option for AD. If applied at very early stages, photobiomodulation may form a preventative therapy by helping to maintain low blood pressure, thereby offsetting the onset of vascular pathology and the disease process; if applied at later stages, it may help form an ongoing therapeutic treatment, by controlling the hypertension, thereby slowing the disease process.
One of the clear advantages for using photobiomodulation is that, unlike many pharmaceutical options, there are few or no side effects, no evidence for toxicity on body cells and because the devices are easy to use and inexpensive, many patients can afford the treatment and use it at home. In fact, it has been our experience with six Parkinson’s disease patients that compliance to using photobiomodulation is very high [108]; a major factor in this high compliance rate was that photobiomodulation is a non-pharmacological treatment and that the patients felt at ease with its use.
In terms of approach, we suggest that photobiomodulation could be applied transcranially, hence offering both mechanisms of direct and indirect stimulation (see above); in addition, using this approach, the access to both cerebral and scalp blood vessels would provide photobiomodulation the potential to influence hypertension. One could also have the additional approach of applying photobiomodulation across another part of the body, for example the abdomen, as to access more blood vessels and influence hypertension. There is evidence, particularly using the longer wavelengths, that transabdominal photobiomodulation can pierce through to the intestines and influence composition of the microbiome in humans [109]; hence, if it can penetrate through layers of abdominal fat, muscle, and connective tissue, it would certainly reach the rich array of major blood vessels that innervate the abdominal organs (e.g., aorta). It could also influence the composition of the microbiome by reducing systemic inflammation. As a starting point, we suggest using a transcranial helmet [82, 103, 108] and a transabdominal device [109] set at the parameters used by previous studies. There is also the option of using a whole body photobiomodulation bed.
CONCLUSIONS
There is a real need for an effective, broad range therapeutic treatment option for patients suffering AD, one that treats the symptoms and offers neuroprotection. Further, is a need for a preventative treatment, one that can offset the development of the disease later in life. In this context, many previous studies have reported that photobiomodulation reduces the pathology and behavioral deficits in animal models of AD; there are also reports that photobiomodulation can reduce hypertension and limit the vascular pathology, a factor that has been reported to increase the risk of developing the disease. When taking all these findings together, we suggest that photobiomodulation, by controlling hypertension, could form an effective therapy for AD. We propose that early treatment may help maintain low blood pressure and offset the vascular pathology and development of the disease (preventative treatment), while later treatment may help control hypertension and slow the ongoing disease process (therapeutic treatment). The stage is set for a series of pre-clinical experiments using a combined hypertensive-AD animal model, translating to a large-scale clinical trial inhumans.
ACKNOWLEDGMENTS
We thank Fonds de Dotation Clinatec and COVEA France for supporting our work.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0632r2).
REFERENCES
[1] | Ballard C , Gauthier S , Corbett A , Brayne C , Aarsland D , Jones E ((2011) ) Alzheimer’s disease. Lancet 377: , 1019–1031. |
[2] | Selkoe DJ , Hardy J ((2016) ) The amyloid hypothesis of Alzheimer’s disease at 25 years. EMBO Mol Med 8: , 595–608. |
[3] | Abolhassani N , Leon J , Sheng Z , Oka S , Hamasaki H , Iwaki T , Nakabeppu Y ((2017) ) Molecular pathophysiology of impaired glucose metabolism, mitochondrial dysfunction, and oxidative DNA damage in Alzheimer’s disease brain. Mech Ageing Dev 161: , 95–104. |
[4] | Brettschneider J , Tredici KD , Lee VM-Y , Trojanowski JQ ((2015) ) Spreading of pathology in neurodegenerative diseases: A focus on human studies. Nat Rev Neurosci 16: , 109–120. |
[5] | Goedert M ((2015) ) Alzheimer’s and Parkinson’s diseases: The prion concept in relation to assembled Aβ, tau, and α-synuclein. Science 349: , 1255555. |
[6] | Karran E , De Strooper B ((2016) ) The amyloid cascade hypothesis: Are we poised for success or failure? J Neurochem 139: Suppl 2, 237–252. |
[7] | Scheltens P , Blennow K , Breteler MMB , de Strooper B , Frisoni GB , Salloway S , Van der Flier WM ((2016) ) Alzheimer’s disease. Lancet 388: , 505–517. |
[8] | Weller RO , Cohen NR , Nicoll JAR ((2004) ) Cerebrovascular disease and the pathophysiology of Alzheimer’s disease. Implications for therapy. Panminerva Med 46: , 239–251. |
[9] | Stone J ((2008) ) What initiates the formation of senile plaques? The origin of Alzheimer-like dementias in capillary haemorrhages. Med Hypotheses 71: , 347–359. |
[10] | Nelson L , Tabet N ((2015) ) Slowing the progression of Alzheimer’s disease; what works? Ageing Res Rev 23: , 193–209. |
[11] | Charidimou A , Boulouis G , Gurol ME , Ayata C , Bacskai BJ , Frosch MP , Viswanathan A , Greenberg SM ((2017) ) Emerging concepts in sporadic cerebral amyloid angiopathy. Brain 140: , 1829–1850. |
[12] | Crous-Bou M , Minguillón C , Gramunt N , Molinuevo JL ((2017) ) Alzheimer’s disease prevention: From risk factors to early intervention. Alzheimers Res Ther 9: , 71. |
[13] | de la Torre JC , Olmo A del , Valles S ((2020) ) Can mild cognitive impairment be stabilized by showering brain mitochondria with laser photons? Neuropharmacology 171: , 107841. |
[14] | Hardy J , Selkoe DJ ((2002) ) The amyloid hypothesis of Alzheimer’s disease: Progress and problems on the road to therapeutics. Science 297: , 353–356. |
[15] | Cummings J , Lee G , Mortsdorf T , Ritter A , Zhong K ((2017) ) Alzheimer’s disease drug development pipeline: 2017. Alzheimers Dement (N Y) 3: , 367–384. |
[16] | Cummings J , Feldman HH , Scheltens P ((2019) ) The “rights” of precision drug development for Alzheimer’s disease. Alzheimers Res Ther 11: , 76. |
[17] | de la Torre JC ((2002) ) Vascular basis of Alzheimer’s pathogenesis. Ann N Y Acad Sci 977: , 196–215. |
[18] | de la Torre JC ((2004) ) Is Alzheimer’s disease a neurodegenerative or a vascular disorder? Data, dogma, and dialectics. Lancet Neurol 3: , 184–190. |
[19] | Cullen KM , Kócsi Z , Stone J ((2005) ) Pericapillary haem-rich deposits: Evidence for microhaemorrhages in aging human cerebral cortex. J Cereb Blood Flow Metab 25: , 1656–1667. |
[20] | Pimentel-Coelho PM , Rivest S ((2012) ) The early contribution of cerebrovascular factors to the pathogenesis of Alzheimer’s disease: The contribution of cerebrovascular factors to AD. Eur J Neurosci 35: , 1917–1937. |
[21] | Stone J , Johnstone DM , Mitrofanis J , O’Rourke M ((2015) ) The mechanical cause of age-related dementia (Alzheimer’s disease): The brain is destroyed by the pulse. J Alzheimers Dis 44: , 355–373. |
[22] | Iadecola C , Davisson RL ((2009) ) Hypertension and cerebrovascular dysfunction. Cell Metab 7: , 476–484. |
[23] | Tini G , Scagliola R , Monacelli F , La Malfa G , Porto I , Brunelli C , Rosa GM ((2020) ) Alzheimer’s disease and cardiovascular disease: A particular association. Cardiol Res Practice 2020: , 1–10. |
[24] | Omura JD , McGuire LC , Patel R , Baumgart M , Lamb R , Jeffers EM , Olivari BS , Croft JB , Thomas CW , Hacker K ((2022) ) Modifiable risk factors for Alzheimer disease and related dementias among adults aged ≥45 years — United States, 2019. MMWR Morb Mortal Wkly Rep 71: , 680–685. |
[25] | DeCarli C ((2021) ) The link between blood pressure and Alzheimer’s disease. Lancet Neurol 20: , 878–879. |
[26] | Lennon MJ , Makkar SR , Crawford JD , Sachdev PS ((2019) ) Midlife hypertension and Alzheimer’s disease: A systematic review and meta-analysis. J Alzheimers Dis 71: , 307–316. |
[27] | Shih Y-H , Tsai S-F , Huang S-H , Chiang Y-T , Hughes MW , Wu S-Y , Lee C-W , Yang T-T , Kuo Y-M ((2016) ) Hypertension impairs hippocampus-related adult neurogenesis, CA1 neuron dendritic arborization and long-term memory. Neuroscience 322: , 346–357. |
[28] | Barthold D , Joyce G , Diaz Brinton R , Wharton W , Kehoe PG , Zissimopoulos J ((2020) ) Association of combination statin and antihypertensive therapy with reduced Alzheimer’s disease and related dementia risk. PLoS One 15: , e0229541. |
[29] | Burke GL , Hughes TM ((2021) ) Arterial changes connecting hypertension to Alzheimer’s disease and related dementias. JACC Cardiovasc Imaging 14: , 186–188. |
[30] | de Heus RAA , Olde Rikkert MGM , Tully PJ , Lawlor BA , Claassen JAHR ;NILVAD Study Group ((2019) ) Blood pressure variability and progression of clinical Alzheimer disease. Hypertension 74: , 1172–1180. |
[31] | Pase MP , Beiser A , Himali JJ , Tsao C , Satizabal CL , Vasan RS , Seshadri S , Mitchell GF ((2016) ) Aortic stiffness and the risk of incident mild cognitive impairment and dementia. Stroke 47: , 2256–2261. |
[32] | Mitchell GF , van Buchem MA , Sigurdsson S , Gotal JD , Jonsdottir MK , Kjartansson Ó , Garcia M , Aspelund T , Harris TB , Gudnason V , Launer LJ ((2011) ) Arterial stiffness, pressure and flow pulsatility and brain structure and function: The Age, Gene/Environment Susceptibility–Reykjavik study. Brain 134: , 3398–3407. |
[33] | Gupta A , Iadecola C ((2015) ) Impaired Aβ clearance: A potential link between atherosclerosis and Alzheimer’s disease. Front Aging Neurosci 7: , 115. |
[34] | Carrano A , Hoozemans JJM , van der Vies SM , Rozemuller AJM , van Horssen J , de Vries HE ((2011) ) Amyloid Beta induces oxidative stress-mediated blood-brain barrier changes in capillary amyloid angiopathy. Antioxid Redox Signal 15: , 1167–1178. |
[35] | Montagne A , Barnes SR , Sweeney MD , Halliday MR , Sagare AP , Zhao Z , Toga AW , Jacobs RE , Liu CY , Amezcua L , Harrington MG , Chui HC , Law M , Zlokovic BV ((2015) ) Blood-brain barrier breakdown in the aging human hippocampus. Neuron 85: , 296–302. |
[36] | Iulita MF , Vallerand D , Beauvillier M , Haupert N , A. Ulysse C , Gagné A , Vernoux N , Duchemin S , Boily M , Tremblay M-È , Girouard H ((2018) ) Differential effect of angiotensin II and blood pressure on hippocampal inflammation in mice. J Neuroinflammation 15: , 62. |
[37] | Shi P , Diez-Freire C , Jun JY , Qi Y , Katovich MJ , Li Q , Sriramula S , Francis J , Sumners C , Raizada MK ((2010) ) Brain microglial cytokines in neurogenic hypertension. Hypertension 56: , 297–303. |
[38] | Bailey DM , Bain AR , Hoiland RL , Barak OF , Drvis I , Hirtz C , Lehmann S , Marchi N , Janigro D , MacLeod DB , Ainslie PN , Dujic Z ((2022) ) Hypoxemia increases blood-brain barrier permeability during extreme apnea in humans. J Cereb Blood Flow Metab 42: , 1120–1135. |
[39] | Beevers G , Lip GYH , O’Brien E ((2001) ) The pathophysiology of hypertension. BMJ 322: , 912–916. |
[40] | Ren L , Lu X , Danser AHJ ((2019) ) Revisiting the brain renin-angiotensin system— focus on novel therapies. Curr Hypertens Rep 21: , 28. |
[41] | Fountain JH , Lappin SL ((2021) ) Physiology, Renin Angiotensin System, StatPearls Publishing. |
[42] | Farron MR , Kabeto MU , Dey AB , Banerjee J , Levine DA , Langa KM ((2020) ) Hypertension and cognitive health among older adults in India, J Am Geriatr Soc 68: Suppl 3, S29–S35. |
[43] | Hughes D , Judge C , Murphy R , Loughlin E , Costello M , Whiteley W , Bosch J , O’Donnell MJ , Canavan M ((2020) ) Association of blood pressure lowering with incident dementia or cognitive impairment: A systematic review and meta-analysis. JAMA 323: , 1934–1944. |
[44] | Lennon MJ , Koncz R , Sachdev PS ((2021) ) Hypertension and Alzheimer’s disease: Is the picture any clearer? Curr Opin Psychiatry 34: , 142–148. |
[45] | Sanchez Hoffmann S , Winkler A , Weimar C , Müller-Gerards D , Abramowski J , Moebus S , Jöckel K-H , Erbel R , Jokisch M ((2021) ) Blood pressure and cognitive decline - the impact of hypertension over one decade. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 28: , 528–542. |
[46] | de Jong DLK , de Heus RAA , Rijpma A , Donders R , Olde Rikkert MGM , Günther M , Lawlor BA , van Osch MJP , Claassen JAHR ((2019) ) Effects of nilvadipine on cerebral blood flow in patients with Alzheimer disease: A randomized trial. Hypertension 74: , 413–420. |
[47] | Ding H , Hashem M , Wiehler WB , Lau W , Martin J , Reid J , Triggle C ((2005) ) Endothelial dysfunction in the streptozotocin-induced diabetic apoE-deficient mouse: EDHF in diabetic apoE-deficient mice. Br J Pharmacol 146: , 1110–1118. |
[48] | Ho JK , Moriarty F , Manly JJ , Larson EB , Evans DA , Rajan KB ((2021) ) Blood-brain barrier crossing renin-angiotensin drugs and cognition in the elderly: A meta-analysis. Hypertension 78: , 629–643. |
[49] | Cifuentes D , Poittevin M , Dere E , Broquères-You D , Bonnin P , Benessiano J , Pocard M , Mariani J , Kubis N , Merkulova-Rainon T , Lévy BI ((2015) ) Hypertension accelerates the progression of Alzheimer-like pathology in a mouse model of the disease. Hypertension 65: , 218–224. |
[50] | Shih Y-H , Wu S-Y , Yu M , Huang S-H , Lee C-W , Jiang M-J , Lin P-Y , Yang T-T , Kuo Y-M ((2018) ) Hypertension accelerates Alzheimer’s disease-related pathologies in pigs and 3xTg mice. Front Aging Neurosci 10: , 73. |
[51] | Marc Y , Boitard SE , Balavoine F , Azizi M , Llorens-Cortes C ((2020) ) Targeting brain aminopeptidase A: A new strategy for the treatment of hypertension and heart failure. Can J Cardiol 36: , 721–731. |
[52] | Valverde A , Dunys J , Lorivel T , Debayle D , Gay A-S , Lacas-Gervais S , Roques Bernard P , Chami M , Checler F ((2021) ) Aminopeptidase A contributes to biochemical, anatomical and cognitive defects in Alzheimer’s disease (AD) mouse model and is increased at early stage in sporadic AD brain. Acta Neuropathol 141: , 823–839. |
[53] | Kummer BR , Diaz I , Wu X , Aaroe AE , Chen ML , Iadecola C , Kamel H , Navi BB ((2019) ) Associations between cerebrovascular risk factors and Parkinson disease. Ann Neurol 86: , 572–581. |
[54] | Tsukamoto T , Kitano Y , Kuno S ((2013) ) Blood pressure fluctuation and hypertension in patients with Parkinson’s disease. Brain Behav 3: , 710–714. |
[55] | Xie J , Liang R , Wang Y , Huang J , Cao X , Niu B ((2020) ) Progress in target drug molecules for Alzheimer’s disease. Curr Top Med Chem 20: , 4–36. |
[56] | Hampel H , Mesulam M-M , Cuello AC , Farlow MR , Giacobini E , Grossberg GT , Khachaturian AS , Vergallo A , Cavedo E , Snyder PJ , Khachaturian ZS ((2018) ) The cholinergic system in the pathophysiology and treatment of Alzheimer’s disease. Brain 141: , 1917–1933. |
[57] | Jadhav S , Avila J , Schöll M , Kovacs GG , Kövari E , Skrabana R , Evans LD , Kontsekova E , Malawska B , de Silva R , Buee L , Zilka N ((2019) ) A walk through tau therapeutic strategies. Acta Neuropathol Commun 7: , 22. |
[58] | Yang J , Yun Y , Miao Y , Sun J , Wang X ((2020) ) Synthesis and biological evaluation of 3-arylbenzofuranone derivatives as potential anti-Alzheimer’s disease agents. J Enzyme Inhib Med Chem 35: , 805–814. |
[59] | Folch J , Ettcheto M , Petrov D , Abad S , Pedrós I , Marin M , Olloquequi J , Camins A ((2018) ) Una revisión de los avances en la terapéutica de la enfermedad de Alzheimer: Estrategia frente a la proteína β-amiloide. Neurología 33: , 47–58. |
[60] | Hamblin MR ((2016) ) Shining light on the head: Photobiomodulation for brain disorders. BBA Clin 6: , 113–124. |
[61] | Shaw VE , Spana S , Ashkan K , Benabid A-L , Stone J , Baker GE , Mitrofanis J ((2010) ) Neuroprotection of midbrain dopaminergic cells in MPTP-treated mice after near-infrared light treatment. J Comp Neurol 518: , 25–40. |
[62] | Lapchak PA , Wei J , Zivin JA ((2004) ) Transcranial infrared laser therapy improves clinical rating scores after embolic strokes in rabbits. Stroke 35: , 1985–1988. |
[63] | Ando T , Xuan W , Xu T , Dai T , Sharma SK , Kharkwal GB , Huang Y-Y , Wu Q , Whalen MJ , Sato S , Obara M , Hamblin MR ((2011) ) Comparison of therapeutic effects between pulsed and continuous wave 810-nm wavelength laser irradiation for traumatic brain injury in mice, PLoS One 6: , e26212. |
[64] | Eells JT , Wong-Riley MTT , VerHoeve J , Henry M , Buchman EV , Kane MP , Gould LJ , Das R , Jett M , Hodgson BD , Margolis D , Whelan HT ((2004) ) Mitochondrial signal transduction in accelerated wound and retinalhealing by near-infrared light therapy. Mitochondrion 4: , 559–567. |
[65] | Muili KA , Gopalakrishnan S , Meyer SL , Eells JT , Lyons J-A ((2012) ) Amelioration of experimental autoimmune encephalomyelitis in C57BL/6 mice by photobiomodulation induced by 670 nm light, PLoS One 7: , e30655. |
[66] | Johnstone DM , Moro C , Stone J , Benabid A-L , Mitrofanis J ((2016) ) Turning on lights to stop neurodegeneration: The potential of near infrared light therapy in Alzheimer’s and Parkinson’s disease. Front Neurosci 9: , 500. |
[67] | Mitrofanis J ((2019) ) Run in the Light: Exploring exercise and photobiomodulation in Parkinson’s disease, Morgan & Claypool Publishers. |
[68] | Wang X , Li X , Zuo X , Liang Z , Ding T , Li K ((2021) ) Photobiomodulation inhibits the activation of neurotoxic microglia and astrocytes by inhibiting Lcn2/JAK2-STAT3 crosstalk after spinal cord injury in male rats. Neuroinflammation 18: , 256. |
[69] | El Massri N , Weinrich TW , Kam JH , Jeffery G , Mitrofanis J ((2018) ) Photobiomodulation reduces gliosis in the basal ganglia of aged mice. Neurobiol Aging 66: , 131–137. |
[70] | Martins DO , Marques DP , Venega RG , Chacur M ((2020) ) Photobiomodulation and B vitamins administration produces antinociception in an orofacial pain model through the modulation of glial cells and cytokines expression, Health 2: , 100040. |
[71] | Yang L , Tucker D , Dong Y , Wu C , Lu Y , Li Y ((2018) ) Photobiomodulation therapy promotes neurogenesis by improving post-stroke local microenvironment and stimulating neuroprogenitor cells. Exp Neurol 299: , 86–96. |
[72] | Guo S , Wang R , Hu J , Sun L , Zhao X , Zhao Y ((2021) ) Photobiomodulation promotes hippocampal CA1 NSC differentiation toward neurons and facilitates cognitive function recovery involving NLRP3 inflammasome mitigation following global cerebral ischemia. Front Cell Neurosci 15: , 731855. |
[73] | Cheng Y , Du Y , Liu H , Tang J , Veenstra A , Kern TS ((2018) ) Photobiomodulation inhibits long-term structural and functional lesions of diabetic retinopathy. Diabetes 67: , 291–298. |
[74] | San Miguel M , Martin KL , Stone J , Johnstone DM ((2019) ) Photobiomodulation mitigates cerebrovascular leakage induced by the parkinsonian neurotoxin MPTP. Biomolecules 9: , 564. |
[75] | Semyachkina-Glushkovskaya O , Abdurashitov A , Dubrovsky A , Klimova M , Agranovich I , Terskov A , Shirokov A , Vinnik V , Kuzmina A , Lezhnev N , Blokhina I , Shnitenkova A , Tuchin V , Rafailov E , Kurths J ((2020) ) Photobiomodulation of lymphatic drainage and clearance: Perspective strategy for augmentation of meningeal lymphatic functions. Biomed Opt Express 11: , 725. |
[76] | Colombo E , Signore A , Aicardi S , Zekiy A , Utyuzh A , Benedicenti S , Amaroli A ((2021) ) Experimental and clinical applications of red and near-infrared photobiomodulation on endothelial dysfunction: A review. Biomedicines 9: , 274. |
[77] | Kovalenko YL , Rudenko LA , Melekhovets OK , Chepeliuk AD , Melekhovets IV ((2018) ) Efficiency of hyperuricemia correction by low level laser therapy in the treatment of arterial hypertension. Wiad Lek 71: , 1310–1315. |
[78] | Saucedo CL , Courtois EC , Wade ZS , Kelley MN , Kheradbin N , Barrett DW , Gonzalez-Lima F ((2021) ) Transcranial laser stimulation: Mitochondrial and cerebrovascular effects in younger and older healthy adults. Brain Stim 14: , 440–449. |
[79] | Maksimovich IV ((2019) ) Intracerebral transcatheter laser photobiomodulation therapy in the treatment of Binswanger’s disease and vascular parkinsonism: Research and clinical experience. Photobiomodul Photomed Laser Surg 37: , 606–614. |
[80] | Nawashiro H , Wada K , Nakai K , Sato S ((2012) ) Focal increase in cerebral blood flow after treatment with near-infrared light to the forehead in a patient in a persistent vegetative state. Photomed Laser Surg 30: , 231–233. |
[81] | Baik JS , Lee TY , Kim NG , Pak K , Ko S-H , Min JH , Shin Y-I ((2021) ) Effects of photobiomodulation on changes in cognitive function and regional cerebral blood flow in patients with mild cognitive impairment: A pilot uncontrolled trial. J Alzheimers Dis 83: , 1513–1519. |
[82] | Chao LL ((2019) ) Effects of home photobiomodulation treatments on cognitive and behavioral function, cerebral perfusion, and resting-state functional connectivity in patients with dementia: A pilot trial. Photobiomodul Photomed Laser Surg 37: , 133–141. |
[83] | Cassano P , Caldieraro MA , Norton R , Mischoulon D , Trinh N-H , Nyer M , Dording C , Hamblin MR , Campbell B , Iosifescu DV ((2019) ) Reported side effects, weight and blood pressure, after repeated sessions of transcranial photobiomodulation. Photobiomodul Photomed Laser Surg 37: , 651–656. |
[84] | Schiffer F , Johnston AL , Ravichandran C , Polcari A , Teicher MH , Webb RH , Hamblin MR ((2009) ) Psychological benefits 2 and 4 weeks after a single treatment with near infrared light to the forehead: A pilot study of 10 patients with major depression and anxiety. Behav Brain Funct 5: , 46. |
[85] | Oishi JC , De Moraes TF , Buzinari TC , Cárnio EC , Parizotto NA , Rodrigues GJ ((2017) ) Hypotensive acute effect of photobiomodulation therapy on hypertensive rats. Life Sci 178: , 56–60. |
[86] | Buzinari TC , de Moraes TF , Cárnio EC , Lopes LA , Salgado HC , Rodrigues GJ ((2020) ) Photobiomodulation induces hypotensive effect in spontaneously hypertensive rats. Lasers Med Sci 35: , 567–572. |
[87] | De Moraes TF , Filho JCC , Oishi JC , Almeida-Lopes L , Parizotto NA , Rodrigues GJ ((2020) ) Energy-dependent effect trial of photobiomodulation on blood pressure in hypertensive rats. Lasers Med Sci 35: , 1041–1046. |
[88] | DeTaboada L , Yu J , El-Amouri S , Gattoni-Celli S , Richieri S , McCarthy T , Streeter J , Kindy MS ((2011) ) Transcranial laser therapy attenuates amyloid-β peptide neuropathology in amyloid-β protein precursor transgenic mice. J Alzheimers Dis 23: , 521–535. |
[89] | Purushothuman S , Johnstone DM , Nandasena C , Mitrofanis J , Stone J ((2014) ) Photobiomodulation with near infrared light mitigates Alzheimer’s disease-related pathology in cerebral cortex - evidence from two transgenic mouse models. Ther 6: , 2. |
[90] | Purushothuman S , Johnstone DM , Nandasena C , Eersel J van , Ittner LM , Mitrofanis J , Stone J ((2015) ) Near infrared light mitigates cerebellar pathology in transgenic mouse models of dementia. Neurosci Lett 591: , 155–159. |
[91] | Yue X , Mei Y , Zhang Y , Tong Z , Cui D , Yang J , Wang A , Wang R , Fei X , Ai L , Di Y , Luo H , Li H , Luo W , Lu Y , Li R , Duan C , Gao G , Yang H , Sun B , He R , Song W , Han H , Tong Z ((2019) ) New insight into Alzheimer’s disease: Light reverses Aβ-obstructed interstitial fluid flow and ameliorates memory decline in APP/PS1 mice. Alzheimers Dement (N Y) 5: , 671–684. |
[92] | Wu X , Shen Q , Zhang Z , Zhang D , Gu Y , Xing D ((2021) ) Photoactivation of TGFβ/SMAD signaling pathway ameliorates adult hippocampal neurogenesis in Alzheimer’s disease model. Stem Cell Res Ther 12: , 345. |
[93] | Wang M , Cao J , Amakye WK , Gong C , Li Q , Ren J ((2020) ) Mid infrared light treatment attenuates cognitive decline and alters the gut microbiota community in APP/PS1 mouse model. Biochem Biophys Res Commun 523: , 60–65. |
[94] | Grillo SL , Duggett NA , Ennaceur A , Chazot PL ((2013) ) Non-invasive infra-red therapy (1072 nm) reduces β-amyloid protein levels in the brain of an Alzheimer’s disease mouse model, TASTPM. J Photochem Photobiol B Biol 123: , 13–22. |
[95] | Comerota MM , Krishnan B , Taglialatela G ((2017) ) Near infrared light decreases synaptic vulnerability to amyloid beta oligomers. Sci Rep 7: , 15012. |
[96] | Blivet G , Meunier J , Roman FJ , Touchon J ((2018) ) Neuroprotective effect of a new photobiomodulation technique against Aβ25–35 peptide–induced toxicity in mice: Novel hypothesis for therapeutic approach of Alzheimer’s disease suggested. Alzheimers Dement (N Y) 4: , 54–63. |
[97] | da Luz Eltchechem C , Salgado ASI , Zângaro RA , da Silva Pereira MC , Kerppers II , da Silva LA , Parreira RB ((2017) ) Transcranial LED therapy on amyloid-β toxin 25–35 in the hippocampal region of rats. Lasers Med Sci 32: , 749–756. |
[98] | Lu Y , Wang R , Dong Y , Tucker D , Zhao N , Ahmed ME , Zhu L , Liu TC-Y , Cohen RM , Zhang Q ((2017) ) Low-level laser therapy for beta amyloid toxicity in rat hippocampus. Neurobiol Aging 49: , 165–182. |
[99] | Cho GM , Lee S-Y , Park JH , Kim MJ , Park K-J , Choi BT , Shin Y-I , Kim NG , Shin HK ((2018) ) Photobiomodulation using a low-level light-emitting diode improves cognitive dysfunction in the 5XFAD mouse model of Alzheimer’s disease, J Gerontol A Biol Sci Med Sci 5: 631–639. |
[100] | Comerota MM , Tumurbaatar B , Krishnan B , Kayed R , Taglialatela G ((2019) ) Near infrared light treatment reduces synaptic levels of toxic tau oligomers in two transgenic mouse models of human tauopathies. Mol Neurobiol 56: , 3341–3355. |
[101] | Sommer AP , Bieschke J , Friedrich RP , Zhu D , Wanker EE , Fecht HJ , Mereles D , Hunstein W ((2012) ) 670 nm laser light and EGCG complementarily reduce amyloid-β aggregates in human neuroblastoma cells: Basis for treatment of Alzheimer’s disease? Photomed Laser Surg 30: , 54–60. |
[102] | Nizamutdinov D , Qi X , Berman MH , Dougal G , Wu E , Yi SS , Stevens AB , Huang JH ((2021) ) Transcranial near infrared light stimulations improve cognition in patients with dementia. Aging Dis 12: , 10. |
[103] | Saltmarche AE , Naeser MA , Ho KF , Hamblin MR , Lim L ((2017) ) Significant improvement in cognition in mild to moderately severe dementia cases treated with transcranial plus intranasal photobiomodulation: Case series report. Photomed Laser Surg 35: , 432–441. |
[104] | Berman MH , Halper JP , Nichols TW , Jarrett H , Lundy A , Huang JH ((2017) ) Photobiomodulation with near infrared light helmet in a pilot, placebo controlled clinical trial in dementia patients testing memory and cognition. J Neurol Neurosci 8: , 176. |
[105] | Pitzschke A , Lovisa B , Seydoux O , Zellweger M , Pfleiderer M , Tardy Y , Wagnières G ((2015) ) Red and NIR light dosimetry in the human deep brain. Phys Med Biol 60: , 2921. |
[106] | Yuan Y , Cassano P , Pias M , Fang Q ((2020) ) Transcranial photobiomodulation with near-infrared light from childhood to elderliness: Simulation of dosimetry. Neurophotonics 7: , 015009. |
[107] | Michalikova S , Ennaceur A , van Rensburg R , Chazot PL ((2008) ) Emotional responses and memory performance of middle-aged CD1 mice in a 3D maze: Effects of low infrared light. Neurobiol Learn Mem 89: , 480–488. |
[108] | Hamilton C , El Khoury H , Hamilton D , Nicklason F , Mitrofanis J ((2019) ) The “buckets”: The use of red and infrared light helmets in Parkinson’s disease patients. Photobiomodul Photomed Laser Surg 37: , 615–622. |
[109] | Bicknell B , Liebert A , McLachlan CS , Kiat H ((2022) ) Microbiome changes in humans with Parkinson’s disease after photobiomodulation therapy: A retrospective study. J Pers Med 12: , 49. |


