
Dyadic Discrete Choice Experiments Enable Persons with Dementia and Informal Caregivers to Participate in Health Care Decision Making: A Mixed Methods Study
Abstract
Background:
Discrete choice experiments (DCEs) may facilitate persons with dementia and informal caregivers to state care preferences. DCEs can be cognitively challenging for persons with dementia.
Objective:
This study aims to design a dementia friendly dyadic DCE that enables persons with dementia and informal caregivers to provide input individually and jointly, by testing the number of attributes and choice tasks persons with dementia can complete and providing insight in their DCE decision-making process.
Methods:
This study included three DCE rounds: 1) persons with dementia, 2) informal caregivers, and 3) persons with dementia and informal caregivers together. A flexible DCE design was employed, with increasing choice task complexity to explore cognitive limitations in decision-making. Summary statistics and bivariate comparisons were calculated. A qualitative think-aloud approach was used to gain insight in the DCE decision-making processes. Transcripts were analyzed using thematic analysis.
Results:
Fifteen person with dementia, 15 informal caregiver, and 14 dyadic DCEs were conducted. In the individual DCE, persons with dementia completed six choice tasks (median), and 80% could complete a choice task with least three attributes. In the dyadic DCE persons with dementia completed eight choice tasks (median) and could handle slightly more attributes. Qualitative results included themes of core components in DCE decision-making such as: understanding the choice task, attribute and level perception, option attractiveness evaluation, decision rule selection, and preference adaptation.
Conclusion:
Persons with dementia can use simple DCE designs. The dyadic DCE was promising for dyads to identify overlapping and discrepant care preferences while reaching consensus.
INTRODUCTION
Discrete choice experiments (DCEs) are frequently used in health economics to identify preferences of patients in health care [1, 2]. Outcomes of DCE research can be used by policy makers, for example to select treatment options or build care packages. In DCEs, participants decide between two or more hypothetical options presented in multiple, sequential options (e.g., care packages). These options are described by a range of characteristics named attributes (e.g., types of care included in a care package), and corresponding attribute levels (e.g., care delivery frequency). The underlying theoretical framework of DCEs assumes tradeoffs between options are made based on the relative utility or attractiveness of attributes and attribute levels [3–6]. Participants are expected to understand the DCE information, weigh options of the given choice task and make the best choice selection [4]. However, overly complex choice tasks may lead to participants ignoring information and making simplified heuristic or random choices, which biases results vastly [7].
Most DCE studies that aim to identify the preferences of persons with dementia use proxy reporting by the public or informal caregivers [8, 9], despite known biases of proxy responses [10]. Recent evidence shows that persons with dementia can express their needs and preferences [11, 12]. The few DCE studies that included the preferences of persons with dementia indicated that DCE survey complexity was a serious challenge for participants [13–15]. Involving the person with dementia and the informal caregiver in individual and joint choice tasks may empower participants and provide a solution to this measurement dilemma. However, there are no official guidelines or consensus on enabling persons with dementia to participate in DCEs. Evidence is required to establish the feasibility of dyadic DCEs for persons with dementia and their informal caregivers. Furthermore, how individual and joint decision-making elicits the preferences of the person with dementia and informal caregivers accurately must be established. This mixed methods study aims to determine the best-in-practice dyadic DCE design to enable persons with dementia and informal caregivers to provide input individually and jointly on health care preferences, by testing the number of attributes and choice tasks persons with dementia can complete, and providing insight in their DCE decision-making process.
METHODS
Design
This mixed method study uses a triangulation design to corroborate the quantitative and qualitative data that is simultaneously collected [16]. Quantitative data aimed to identify the DCE choice task complexity participants could handle whereas qualitative data were used to provide insights in the DCE decision-making process. Three in-person DCE rounds were conducted with: 1) the person with dementia, 2) the informal caregiver, and 3) together. The individual interviews aimed to elicit individual preferences and the dyadic interviews their joint preferences. This study used the Checklist for Mixed Methods Research Manuscript Preparation and Review (Supplementary Material 1) [17], and followed the COREQ guidelines (Supplementary Material 2) to provide more details on the qualitative part of this study [18]. An ethical waiver was obtained from the ethics committee at the Amsterdam University Medical Centre (W20_001 #20.025).
Participants
Dyads of informal caregivers and persons with dementia were recruited through dementia care organizations from different regions of the Netherlands. Potential participants were approached by JW via telephone and informed about the study aims and procedures.
Persons with Alzheimer’s disease and other dementias (hereinafter referred to as persons with dementia) were eligible if they had a diagnosis from a medical specialist. We used the Dutch version of the Telephone-based Interview for Cognitive Screening (TICS) to screen the cognitive status of the person with dementia [19]. The TICS has a cutoff point of < 34 for mild cognitive impairment and < 28 for severe cognitive impairment [19]. Persons with dementia gave oral informed consent, informal caregivers signed written informed consent and proxy informed consent. Furthermore, informal caregivers completed a short questionnaire to obtain demographic information, completed the Zarit 6 Burden Interview to assess caregiver burden [20], and a proxy report of the Katz 6 Activities of Daily Living Scale for the person with dementia [21].
DCE choice tasks
We used a DCE to establish preferences of homecare and support that enable persons with dementia and their informal caregivers to extend their time living at home. Table 1 describes the attributes and levels that were used to describe hypothetical packages of homecare and support based on previously published focus groups [12]. All choice tasks consisted of two hypothetical options.
Table 1
Attribute description and corresponding levels
| Attribute | Description | Attribute levels |
| Homecare | I can get assistance at home with personal care such as showering, dressing, or medication. | •Daily on a fixed time•24/7 on demand |
| Help with daily activities | I can get assistance at home with household tasks such as groceries, laundry, cooking, cleaning, or help with doing my finances. | •Once per week•Multiple times per week |
| Social activities | I can participate in social activities that I like to do. | •At a daycare facility, once per week•At a daycare facility, multiple times per week•At home, once per week•At home, multiple times per week |
| Emotional support | I can talk to someone when I feel down or want to share my worries. | •Peer support group•Psychologist•Telephone helpline•Case manager |
| Information about dementia | I can get information about having dementia. | •Telephone helpline•Case manager•Peer support group |
| Navigating the healthcare system | I can get assistance with organizing care and help with insurances. | •Telephone helpline•Case manager |
| Home adaptations and tools | I can get home adaptations and tools such as a stair lift, grips in shower and toilet, or a personal alarm. | •No reimbursement•Full reimbursement |
We created easy-to-understand illustrations to describe each attribute including a simple written description (Supplementary Material 3). Attribute levels were presented by a simple written description. See Supplementary Material 4 for a choice task example. We designed a DCE template on which attribute and level cards could be placed to create the hypothetical scenarios. During the iterative process of designing the DCE, we piloted and consulted our expert group consisting of two informal caregivers, four geriatricians, two day-care professionals, and two DCE experts.
Interview design
A concurrent think-aloud approach was used to provide insights into the decision-making process of persons with dementia and informal caregivers [22]. In a think-aloud, participants perform tasks and are asked to say everything that crosses their mind. The interview started with an explanation of its purpose, followed by a general introduction about responding to DCEs. The interviewer explained each attribute card as objectively as possible with the use of the picture and the written description. A practice round helped participants understand the requirements of the choice task. We chose a flexible DCE design to test the boundaries of the cognitive abilities in decision-making of each participant. For persons with dementia, we started with the simplest design of two attributes. If four choice sets of two attributes were completed without difficulty, complexity was increased by adding an extra attribute to the next choice task. Complexity was increased following the same procedure until a maximum of six attributes. For informal caregivers, we followed the same procedure, but started with a choice set containing four attributes. We started with two attributes in the dyadic interviews.
Data collection
A total of 44 DCE interviews were conducted at participants’ homes: 15 with persons with dementia, 15 with informal caregivers, and 14 within sample dyadic interviews. Interviews were spaced at least two weeks apart to minimize mere exposure effects [23, 24]. All interviews were conducted by JW, an experienced qualitative interviewer. Interviews were audio-recorded and transcribed verbatim. Data saturation was reached after 44 interviews. Quantitative DCE survey data such as time on task and choice task complexity were collected during the interviews.
Data analysis
Transcripts were analyzed using thematic analysis based on the guideline of Braun and Clarke [25]. Inductive thematic analysis of the written data consisted of six phases: 1) familiarizing the data, 2) generating initial codes, 3) searching for themes, 4) reviewing potential themes, 5) defining and naming themes, and 6) producing the report [25]. JW analysed all transcripts while JMV and NL each independently analysed four transcripts. Coding schemes were discussed in the research group to enhance investigator triangulation. See final coding scheme in Supplementary Material 5. Qualitative data were analyzed using MAXQDA 2018 V.18.2.0. Furthermore, quantitative DCE survey data was analyzed by summary statistics and bivariate comparisons. Linear regression modelling was used to analyze the association between scores on the cognitive screening test of participants with dementia (TICS) and number of choice tasks completed, in addition to the association between scores on the cognitive screening test and the maximum attributes participant with dementia could handle within a choice task. Statistical significance was set at p < 0.05. Quantitative data was analyzed Using Stata V15.1 SE.
RESULTS
Characteristics of participants
Table 2 describes characteristics of the participants.
Table 2
Characteristics of participants
| Person with dementia (n = 15) | Informal caregiver (n = 15) | |
| Age (mean,±SD) | 76.1 (6.2) | 70.2 (6.5) |
| Female (n, %) | 5 (30) | 12 (80) |
| Living situation (n, %) | ||
| Alone | 2 (13.3) | |
| With informal caregiver | 13 (86.7) | |
| TICS score* (mean, ±SD) | 22.6 (3.5) | |
| Multi morbidity† (n, %) | 9 (60.0) | |
| KATZ 6 score‡ (mean, ±SD) | 5.5 (0.5) | |
| Case manager involved (n, %) | 13 (86.7) | |
| Relation to person with Dementia (n, %) | ||
| Partner | 13 (86.7) | |
| Child | 1 (6.7) | |
| Sibling | 1 (6.7) | |
| Zarit Burden Interview score§ (mean, ±SD) | 7.8 (2.5) |
*Cut-off mild cognitive impairment < 34 points, dementia, or severe cognitive impairment < 28 points based on Telephone-based Interview for Cognitive Screening (TICS). †Two or more chronic conditions. ‡Score 0 = very dependent, score 6 = independent. §Score≥11 high caregiver burden.
Individual DCEs
Survey data
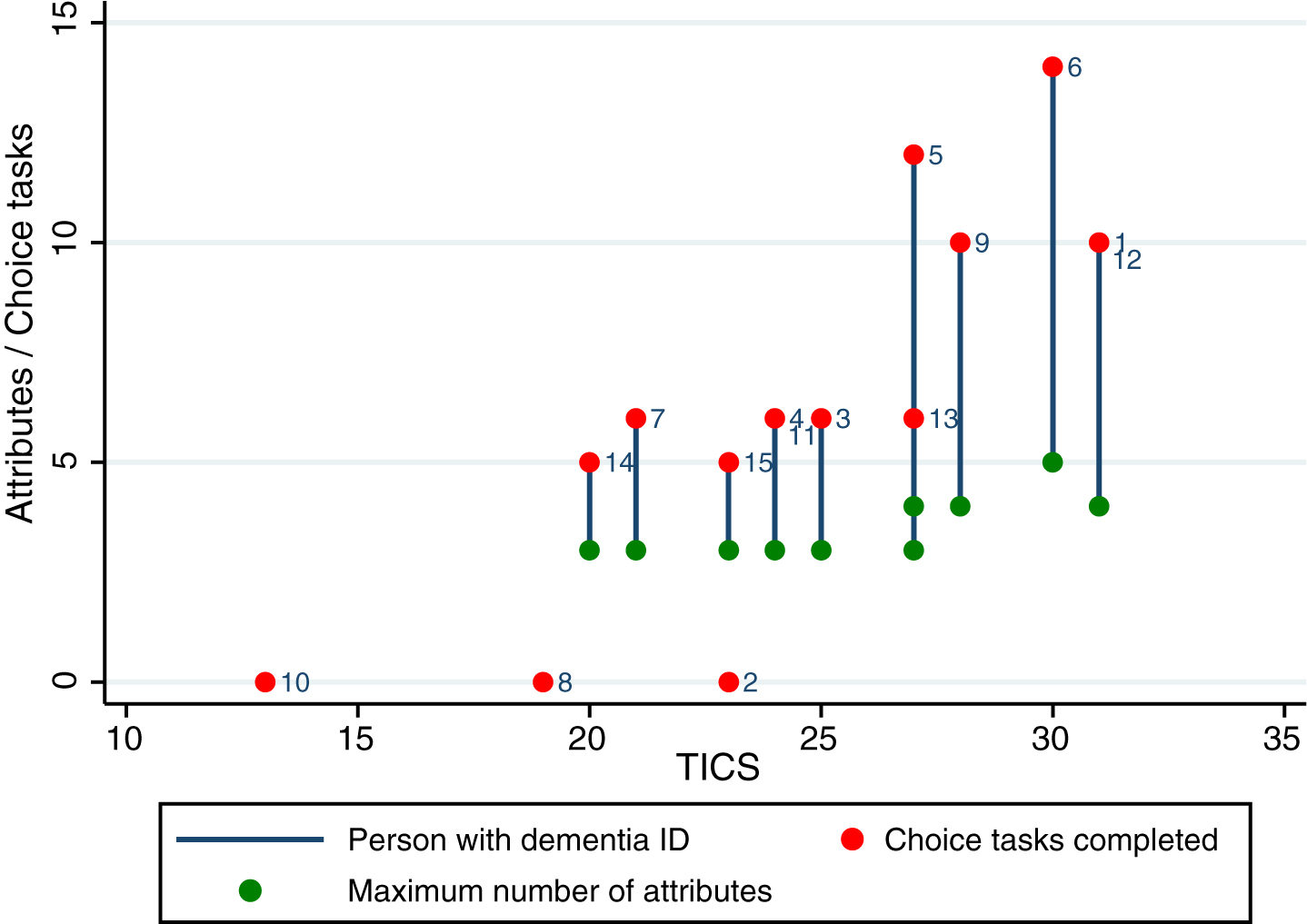
The DCE interviews with persons with dementia lasted between 20 to 70 min. Of the 15 persons with dementia participating, three were not able to complete the two-attribute choice task. The remaining 12 participants with dementia completed at least one choice task. The median number of choice tasks completed was six, while most participants with dementia (80.0%) completed choice tasks with three attributes (Table 3). Unadjusted bivariate comparisons show a positive association between cognitive screening test scores and the maximum number of attributes participant with dementia could handle within a choice task (β=0.251, 95% CI 0.133–0.368, p < 0.000), and between cognitive screening test scores and the maximum number of choice tasks completed (β=0.714, 95% CI 0.419–1.00, p < 0.000). Figure 1 illustrates the number of attributes and choice tasks completed by scores on the cognitive screening test for each participant with dementia.
Table 3
Maximum number of attributes and choice tasks completed
| Persons with dementia (n = 15) | Informal caregivers (n = 15) | Dyadic interviews (n = 14) | |
| Maximum choice tasks completed, Median (Interquartile range) | 6 (5) | 9 (1) | 8 (5) |
| Maximum number of attributes per choice task, n (%) | |||
| Did not complete the first | 3 (20.0) | – | 2 (14.3) |
| task of two attributes | |||
| 2 attributes* | 0 (0.0) | – | 1 (7.1) |
| 3 attributes | 8 (53.3) | – | 5 (35.7) |
| 4 attributes | 3 (20.0) | – | 4 (28.6) |
| 5 attributes | 1 (6.7) | 3 (20.0) | 2 (14.3) |
| 6 attributes | 0 (0.0) | 12 (80.0) | 0 (0.0) |
*The starting number of attributes was 2 for the individual DCE with persons with dementia and joint DCE for persons with dementia and informal caregivers, and 4 was the starting number of attributes for the individual DCE with informal caregivers. Three persons with dementia were not able to complete the first task.
Fig. 1
Number of attributes and choice tasks completed by individual scores on the Telephone Interview Cognitive Screening in participants with dementia.
The interviews with the informal caregiver lasted between 50 to 90 min. The mean number of choice tasks completed was nine and most informal caregivers (80.0%) completed choice tasks with six attributes.
Understanding the choice task
After the practice round, few participants with dementia (2/15) could directly comprehend the choice task, and understood they had to make tradeoffs based on the options presented (as assessed by the interviewer). Although participants with dementia showed a clear learning curve in understanding the choice tasks, most needed reminders throughout all choice tasks. Informal caregivers required minimal guidance after the practice round.
The most common decision-making strategy was going over the choice task from top to bottom, expressing their preference for package A or B per attribute, followed by valuing the total attractiveness of the options. Others seemed to choose the most important attribute of the choice task and used it to evaluate the attractiveness of the other attributes.
Person with dementia (ID#4): You want the best options from the package. This is not possible because they are in both A and B. Both packages have their advantageous, which makes it difficult to choose.
3.4Attribute perception
Several participants with dementia (5/15), and all informal caregivers were able to understand the attributes presented by the illustration and text. Participants with dementia generally needed additional explanations. Some participants with dementia needed a new explanation each time an attribute reoccurred in a choice task. Also, their perceptions about attributes appeared to be temporally inconsistent as they forgot or changed their understanding of what the attribute entailed. The attribute illustrations seemed helpful in decreasing cognitive burden of the choice tasks because many participants with dementia and informal caregivers remembered the illustrations.
Most participants with dementia were able to express differences in attractiveness across attributes and could evaluate multiple attributes given in a single choice task (quote below). However, when an attribute was not understood well, participants with dementia were likely to ignore the attribute.
Person with dementia (ID#4): I think personal in-home care becomes more important than help with daily activities. You can ask your children to do groceries and those sorts of things, however you cannot expect them to come to help you shower every morning.
Attribute level perception
Most participants with dementia (8/15) directly understood the attribute levels presented without further explanation and could explain the attractiveness of levels (quote below). Sometimes participants with dementia and informal caregivers interpreted the attribute levels differently from the original intension. For example, the telephone helpline was perceived as having the option to call their own case manager. Some attribute levels, like social activities organized at the daycare center, seemed to be a dominant preference, leading to screening of alternatives without that level.
Person with dementia (ID#9): At the daycare center you are out for a day and there are other people you can talk to; it is like going on an outing. That is different from somebody coming to my home.
Option attractiveness evaluation
Most participants with dementia (12/15) were able to process all information from the options given in the choice task and could make tradeoffs across all aspects of the choice task presented. During each choice task the interviewer frequently prompted participants to express how they were doing. This gave participants the opportunity to express their difficulties and opt out if they were not able to come to a decision. Too many attributes and fatigue were the main reasons mentioned for not being able to process all information from the given choice task.
Person with dementia (ID#1): I do not know; it is a lot. Yes, combining the cards [attributes and levels]. I try to do it card by card. Then if I read the next, this one was B, the other I had A, then I do not know what to do.
Decision rule selection
The interviewer prompted participants to explain their preferences. Sometimes participants with dementia did not provide any explanation, choosing a care package at random. Moreover, when explaining their preferences, some lacked insight that they had dementia or might need care or assistance. Others used simplified decision rules such as motivating their preferences by counting the number of favorable attribute levels per care package.
Person with dementia (ID#3): Well, I think I choose for . . . let see, one, two, three for this package. That is three out of four, so I choose that one.
Often participants with dementia and informal caregivers used their present situation as an anchor point (i.e., their present situation constitutes a reference alternative). Care that they were already using seemed to predominate over the ones they were less familiar with (i.e., there may be attribute level-based inertia). Also, participants with dementia and informal caregivers indicated that they found it difficult to envision what their future care needs might be that could enable them to live at home, since the course of dementia is unpredictable. This may have led to decision avoidance, ultimately leading to random choice.
Person with dementia (ID#6): I try to consider that in the future I might worsen. It is a shame, at this moment I’m doing quite ok, however I will do less and less. Now I must think about what I still might be able to do in the future and what not, that is very difficult.
Sometimes participants with dementia made decisions influenced by outside considerations, refusing to keep within the boundaries set by the two options presented. This phenomenon happened often when a similar level option was in both care packages of the choice task but related to different attributes. For example, when the level case manager was in option A for emotional support, but also in option B for information about dementia. Also, decisions from previous choice tasks were sometimes included in decisions of the present choice task. Participants with dementia stated that they already could receive this care as they chose for this option in a previous choice task. The latter phenomenon could translate into a lack of independence between tasks, which is an almost universally adopted assumption in statistical procedures used to analyse DCE responses.
Dyadic DCEs
Survey data
The dyadic interviews lasted between 50 min to 80 min. The median number of choice tasks completed was nine, and 78.6% of the dyads were able to complete choice tasks with a maximum of three attributes (see Table 3). Some participants with dementia (21.4%) were able to complete choice tasks with more attributes in the dyadic DCE compared to the individual DCE.
Informal caregivers assisting with choice task
During the dyadic interviews, informal caregivers helped the person with dementia in understanding the choice tasks. They explained in their own words what was expected of them completing the choice task. Furthermore, they suggested methods for making tradeoffs.
Informal Caregiver: You also must consider the other cards.
Person with dementia (ID#3): You mean I cannot pick both?
Informal care Caregiver: No, you must choose between package A or B. So, if you prefer to have the home adaptations reimbursed, you can only contact the telephone helpline for assistance with organizing care and not the case manager.
Person with dementia (ID#3): Ok, now I remember. I cannot take both, I must choose between these two.
Furthermore, informal caregivers helped elicit preferences from persons with dementia and indicated whether these were not realistic in their present situation, making operative choice constraints and contextual considerations apparent (quote below). Also, it enabled persons with dementia and informal caregivers to understand each other’s motivations, thus taking both preferences into consideration. Both frequently did not know each other’s’ preference.
Person with dementia (ID#5): I do not need help with doing groceries. This is something I can still do myself.
Caregiver: No, you cannot do this by yourself.
Person with dementia (ID#5): Why not?
Caregiver: How? You have not done this for years.
Person with dementia (ID#5): I just go there by bike.
Caregiver: I do not think that is a good idea. Sometimes we ask our children to do that.
Preference adaptation
Many informal caregivers let the person with dementia choose first. However, when informal caregivers shared their opinion, persons with dementia were likely to follow their decision. When persons with dementia found it difficult to state their preference, they asked their informal caregiver for confirmation of their choice or refrained completely from choosing by asking for the informal caregiver’s opinion. Clearly, different degrees of agency delegation can occur in these joint decisions.
In total 15 identical choice tasks were completed during the individual DCE by the person with dementia, by the informal caregiver, and by both during the dyadic DCE. In 66.7% of those choice tasks there was full agreement on the decision throughout all three DCEs. In 13.3% the preference of the persons with dementia from the individual DCE was dominant in the dyadic DCE, in 20.0% the preference of the informal caregiver was dominant in the dyadic DCE, indicating that in 33.3% of the dyadic tasks the chosen alternative arose through some degree of preference balancing.
DISCUSSION
This study found that most persons with dementia in the individual DCE round were able to complete a median of six choice tasks that included two illustrated scenarios using a maximum of three attributes. The informal caregiver DCE round was helpful to identify their individual preferences, in which they experienced minimal difficulties with completing the choice tasks. In the dyadic DCE round, persons with dementia were able to complete more choice tasks and handle an increased number of attributes. Informal caregivers had a meaningful role in helping the persons with dementia complete the dyadic DCE. A surprising finding was the dyadic DCE enabled communication on care preferences between the persons with dementia and their informal caregiver.
Study results suggest that the number of attributes and choice tasks are decisive factors in establishing cognitive burden for persons with dementia. In this small sample we found a positive unadjusted association between cognitive screening test scores and maximum number of attributes within a choice task, and a positive unadjusted association between cognitive screening test scores and maximum number of choice tasks completed. In addition, we found that two options described by three attributes, and six choice tasks, was the limit for most participants with dementia. Longer and more complex surveys could lead to participants making simplified choices. Study participants adopted for example the single-attribute lexicographic rule, making decisions based on only the most important attribute [26]. Also, participant adopted the majority of confirming dimensions decision rule, making decisions based on the number of favorable attributes instead of maximizing the total attractiveness of the attributes [27]. Both decision rules do not include making trade-offs among the other attributes, which is essential in DCE decision-making [26, 27]. This type of adaptive behavior is not limited to populations with dementia but are widely recognized impacts of exceeding bearable cognitive burdens [26, 27]. Cognitive screening tests such as the TICS are recommended for respondent inclusion.
A recent DCE study that included persons with mild cognitive impairments showed that using pictures and simplified language helped participants increase attribute understanding [28]. This is consistent with our study findings that show illustrations improved understanding the attributes and therefore may reduce cognitive burden. Piloting illustrations in survey designs with its end-users is recommended.
The face-to-face interview combined with the concurrent think-aloud approach appeared to help the persons with dementia with the DCE tasks. Results of this study showed that most persons with dementia benefited from frequent reminders on the rules of the choice tasks. This consistent with two previous studies [15, 28] that found interviewers could check if persons with dementia were able to understand the DCE choice task through the think aloud approach. Although the added strain of thinking aloud when performing a task is discussed in literature [29], in our study it helped persons with dementia focus on the task. Like Ratcliffe et al. [15], our study found that attribute and level perceptions, and reading difficulties, are a common concern. In addition, this study found that persons with dementia sometimes made choices influenced by outside considerations or decisions from previous choice tasks. These results suggest that persons with dementia need extra guidance and feedback when using DCEs. By letting participants think aloud, the interviewer can observe the above-mentioned issues and help overcome them in real time. Moreover, the interviewer can elicit the decision rules of participants to avoid simplified decision-making.
There are limited studies that included both the preferences of persons with dementia and informal caregivers [13, 14]. However, choices are commonly made by more than one individual [30, 31]. The dyadic DCE from this study created an opportunity for both members of the dyad to explore, learn, and discuss each other’s preference, together formulating joint preferences. An advantage of joint choice experiments found in this study was that it made it possible for informal caregivers to assist persons with dementia in completing the choice tasks. Informal caregivers helped explain the choice task, elicited justifications, made constraints of the choice task salient, and provided a reality check. Consequently, this might have enabled persons with dementia to complete surveys that were more complex.
Dyadic preferences are expected to be different from individual preferences, as persons with dementia and informal caregivers have distinctive care needs and preferences [12]. In this study, frequently they did not know each other’s care preferences, which is consistent with previous literature [32]. Differences between individual and joint preferences are also reported by DCE studies in other fields, and they suggest that joint preferences should be cautiously interpreted as they could be yielding the preference of the stronger agent [30, 33]. Our study found full agreement in 66.7% throughout all three DCEs. In 13.3% the preference of the persons with dementia from the individual DCE was dominant in the dyadic DCE while in 20.0% the preference of the informal caregiver was dominant in the dyadic DCE. It appeared that especially the choice tasks that were difficult for the persons with dementia promoted agency transfer by the person with dementia to the informal caregiver. This shows the importance of interviewing the informal caregiver separately to obtain their individual preference, followed by the individual DCE of the persons with dementia, with the informal caregiver merely having an assisting role, and on a later occasion with sufficient time interval conducting the joint DCE round.
Policy makers can use the preference outcomes of both individual and joint DCEs for health policy decisions based on their relevancy. There are valid reasons for including the preference outcomes of person with dementia, as they are the recipients of most care and can provide their own opinions while informal caregivers provide most of the care and have their own needs [12, 34]. Outcomes of joint DCEs might identify preferences that are shared by persons with dementia and informal caregivers. Future DCE research with larger sample sizes should determine what their preferences are.
Strengths of this study include participation of informal caregivers and persons with dementia in a previous qualitative study prioritizing characteristics of homecare and support to ensure attributes used in this study were relevant to participants [12]. While the sample size in this study is small, we did three in-depth rounds of qualitative interviews and achieved saturation on the themes we sought to explore. This study is a starting point for larger scale studies to explore other DCE survey designs that can be utilized by persons with dementia.
In conclusion, this study provided evidence that persons with dementia can participate in DCEs with low choice task complexity. Including the informal caregiver and persons with dementia in dyadic DCEs can enable greater empowerment of the person with dementia while enabling joint decision-making.
ACKNOWLEDGMENTS
This work was supported by the Netherlands Organization for Health Research and Development (NWO-ZonMw Veni, 091.619.060).
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0604r1).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-220604.
REFERENCES
[1] | de Bekker-Grob EW , Ryan M , Gerard K ((2012) ) Discrete choice experiments in health economics: A review of the literature. Health Econ 21: , 145–172. |
[2] | Soekhai V , de Bekker-Grob EW , Ellis AR , Vass CM ((2019) ) Discrete choice experiments in health economics: Past, present and future. Pharmacoeconomics 37: , 201–226. |
[3] | Hensher DA , Rose JM , Greene WH ((2005) ) Applied Choice Analysis: A Primer. Cambridge University Press. |
[4] | Louviere J , Hensher DA , Swait JD ((2000) ) Stated Choice Methods: Analysis and Application. Cambridge University Press. |
[5] | Lancsar E , Louviere J ((2008) ) Conducting discrete choice experiments to inform healthcare decision making: A user’s guide. Pharmacoeconomics 26: , 661–677. |
[6] | Ryan M , Gerard K , Amaya-Amaya M ((2008) ) Using Discrete Choice Experiments to Value Health and Health Care, Springer, Dordrecht, The Netherlands. |
[7] | Heidenreich S , Watson V , Ryan M , Phimister E ((2018) ) Decision heuristic or preference? Attribute non-attendance in discrete choice problems. Health Econ 27: , 157–171. |
[8] | Walsh S , O’Shea E , Pierse T , Kennelly B , Keogh F , Doherty E ((2020) ) Public preferences for home care services for people with dementia: A discrete choice experiment on personhood. Soc Sci Med 245: , 112675. |
[9] | Kampanellou E , Chester H , Davies L , Davies S , Giebel C , Hughes J , Challis D , Clarkson P , Members of the HOST-D (Home Support in Dementia) Programme Management Group ((2019) ) Carer preferences for home support services in later stage dementia. Aging Ment Health 23: , 60–68. |
[10] | Bryan S , Hardyman W , Bentham P , Buckley A , Laight A ((2005) ) Proxy completion of EQ-5D in patients with dementia. Qual Life Res 14: , 107–118. |
[11] | Vullings I , Labrie N , Wammes JD , de Bekker-Grob EW , MacNeil-Vroomen J ((2020) ) Important components for Dutch in-home care based on qualitative interviews with persons with dementia and informal caregivers. Health Expect 23: , 1412–1419. |
[12] | Wammes JD , Labrie NHM , Agogo GO , Monin JK , de Bekker-Grob EW , MacNeil Vroomen JL ((2021) ) Persons with dementia and informal caregivers prioritizing care: A mixed-methods study. Alzheimers Dement (N Y) 7: , e12193. |
[13] | O’Philbin L , Woods B , Holmes E ((2020) ) People with dementia and caregiver preferences for digital life story work service interventions. A discrete choice experiment and digital survey. Aging Ment Health 24: , 353–361. |
[14] | Chester H , Clarkson P , Davies L , Sutcliffe C , Davies S , Feast A , Hughes J , Challis D , Members of the HOST-D (Home Support in Dementia) Programme Management Group ((2018) ) People with dementia and carer preferences for home support services in early-stage dementia. Aging Ment Health 22: , 270–279. |
[15] | Ratcliffe J , Hutchinson C , Milte R , Nguyen KH , Welch A , Caporale T , Corlis M , Comans T ((2019) ) How do people with dementia and family carers value dementia-specific quality of life states? An explorative “Think Aloud” study. Australas J Ageing 38 Suppl 2: , 75–82. |
[16] | Doyle L , Brady A , Byrne G ((2009) ) An overview of mixed methods research. J Res Nurs 14: , 175–185. |
[17] | Lee SD , Iott B , Banaszak-Holl J , Shih SF , Raj M , Johnson KE , Kiessling K , Moore-Petinak N ((2022) ) Application of mixed methods in health services management research: A systematic review. Med Care Res Rev 79: , 331–344. |
[18] | Tong A , Sainsbury P , Craig J ((2007) ) Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int J Qual Health Care 19: , 349–357. |
[19] | Kempen GI , Meier AJ , Bouwens SF , van Deursen J , Verhey FR ((2007) ) The psychometric properties of the Dutch version of the Telephone Interview Cognitive Status (TICS). Tijdschr Gerontol Geriatr 38: , 38–45. |
[20] | Higginson IJ , Gao W , Jackson D , Murray J , Harding R ((2010) ) Short-form Zarit Caregiver Burden Interviews were valid in advanced conditions. J Clin Epidemiol 63: , 535–542. |
[21] | Katz S , Ford AB , Moskowitz RW , Jackson BA , Jaffe MW ((1963) ) Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychosocial function. JAMA 185: , 914–919. |
[22] | Jääskeläinen R (2010) Handbook of Translation Studies, pp. 371-374. |
[23] | Montoya RM , Horton RS , Vevea JL , Citkowicz M , Lauber EA ((2017) ) A re-examination of the mere exposure effect: The influence of repeated exposure on recognition, familiarity, and liking. Psychol Bull 143: , 459–498. |
[24] | Soga N (2018) The relationship between the anchoring effect and the mere exposure effect in commodity selection. Proceedings of the 5th Multidisciplinary International Social Networks, pp. 1-4. |
[25] | Braun V , Clarke V ((2012) ) APA Handbook of Research Methods in Psychology, American Psychological Association. |
[26] | Scott A ((2002) ) Identifying and analysing dominant preferences in discrete choice experiments: An application in health care. J Econ Psychol 23: , 383–398. |
[27] | Russo JE , Dosher BA ((1983) ) Strategies for multiattribute binary choice. J Exp Psychol Learn Mem Cogn 9: , 676–696. |
[28] | Hutchinson C , Milte R , Stanley M , Duff G , Ratcliffe J ((2022) ) Using discrete choice experiments to elicit the service preferences of people with mild intellectual disability: An exploratory study. Health Soc Care Community 30: , e1396–e1405. |
[29] | Nielsen J , Clemmensen T , Yssing C (2002) Getting access to what goes on in people’s heads? Reflections on the think-aloud technique Proceedings of the second Nordic conference on Human-computer interaction, pp. 101-110. |
[30] | Hensher DA , Beck MJ , Rose JM ((2011) ) Accounting for preference and scale heterogeneity in establishing whether it matters who is interviewed to reveal household automobile purchase preferences. Environ Resource Econ 49: , 1–22. |
[31] | Corfman KP , Lehmann DR ((1987) ) Models of cooperative group decision-making and relative influence: An experimental investigation of family purchase decisions. J Consum Res 14: , 1–13. |
[32] | Whitlatch C ((2008) ) Informal caregivers: Communciation and decision making . J Soc Work Educ 44: , 73–77. |
[33] | Beharry-Borg N , Hensher DA , Scarpa R ((2009) ) An analytical framework for joint vs separate decisions by couples in choice experiments: The case of coastal water quality in Tobago. Environ Resour Econ 43: , 95–117. |
[34] | Cantarero-Prieto D , Leon PL , Blazquez-Fernandez C , Juan PS , Cobo CS ((2020) ) The economic cost of dementia: A systematic review. Dementia (London) 19: , 2637–2657. |


