
Real-World Use of Symptomatic Treatments in Early Alzheimer’s Disease
Abstract
Background:
Alzheimer’s disease (AD) is the most common type of dementia, causing progressive decline of memory, thinking, and behavior, impairing daily functioning. Early AD (eAD) includes mild cognitive impairment (MCI) due to AD and mild AD dementia.
Objective:
The aim of this study was to investigate symptomatic treatment prevalence and treatment patterns in eAD.
Methods:
Embase, MEDLINE, and EBM Reviews were searched in November 2021 for observational studies reporting symptomatic treatment patterns in eAD. The range of patients receiving treatment was collated. Risk of bias was assessed using the Joanna Briggs Institute (JBI) prevalence tool. Two independent reviewers screened the records, one performed data extraction and quality assessment while a second checked.
Results:
Twenty-one studies (prospective and retrospective cohorts, cross-sectional studies, and a survey) were included. Population size ranged from 23 to 2,028. Worldwide, 18 to 35% of patients diagnosed with MCI due to AD received any AChE inhibitor (three studies; n = 631), 7 to 8% memantine (two studies; n = 229), and 9% combination therapy (one study; n = 402). Patients receiving no treatment ranged from 41 to 54% (two studies; n = 733). Worldwide, in mild AD dementia patients, 13 to 89% received any AChE inhibitor (six studies; n = 3,715), 1 to 21% memantine (five studies, n = 3,527), and 0.4 to 39% combination therapy (four studies, n = 3,018). Patients receiving no treatment ranged from 9 to 26% (five studies, n = 4,073).
Conclusion:
Limitations in reporting led to unclear risk of bias. The results reveal a pattern of use of symptomatic treatment in eAD beyond approved labels and highlights the opportunity for new consensus guidelines to inform clinical practice.
INTRODUCTION
Alzheimer’s disease (AD) and other dementias are a major and increasing global health challenge, with an estimated 50 million people currently living with dementia [1]. AD is the most common cause of age-related dementia, accounting for an estimated two thirds of cases [2].
AD is characterized by cognitive deficits resulting in progressive decline in memory, reasoning, thinking, and behavioral symptoms that impair a person’s ability to function in daily life [2]. AD progresses along a continuum with three phases: preclinical disease, mild cognitive impairment (MCI), and clinically apparent dementia (mild, moderate, and severe AD dementia) [3]. Early clinical stages of AD, hereafter referred to as early AD (eAD), are defined as MCI due to AD (also referred to as prodromal AD) and mild AD dementia. The early indicators are decline in mental capabilities in the absence of impaired performance on objective cognitive testing. MCI describes the earliest symptomatic stage of cognitive impairment in which at least one cognitive domain is impaired to at least a mild extent whilst functional capacities are relatively preserved [4]. By contrast, dementia is defined as cognitive impairment of sufficient magnitude to impair independence and affect daily life. Symptoms evolve over time and the pace at which symptoms advance from mild to moderate to severe dementia differs between individuals. Short periods of memory loss characterize the early clinical stage of the disease with interference in some everyday activities as dementia progresses to a mild stage [2].
A meta-analysis featured in a 2018 North American practice guideline update reported that MCI due to AD affects 6.7% of 60–64-year-olds and 25.2% of 80–84-year-olds [5]. A study to characterize severity of AD amongst a primarily Caucasian population in the Framingham Heart study found 50.5% of people with AD had mild AD dementia [6].
Currently, no cure exists for AD, and until the recent approval of aducanumab in the US [7], no treatments existed to slow its progression. However, therapeutic interventions exist to temporarily slow symptoms and improve cognitive function. A summary of the current guidelines for the treatment of AD in the US, Canada, and Europe is presented in Supplementary Table 1. There are currently no recommendations for pharmacological management of MCI due to AD. For dementia due to AD, two classes of symptomatic treatments have existing approvals in Europe and the US, the acetylcholinesterase (AChE) inhibitors - donepezil, galantamine and rivastigmine, and the N-methyl-D-aspartate (NMDA) antagonist, memantine [7–9]. AChE inhibitors are considered as first line treatment for mild-moderate AD dementia, acting to increase acetylcholine and improve memory [9]. As AD dementia progresses to the moderate-severe stage, memantine is recommended as an add-on therapy.
Recent results from surveys on the clinical management of MCI due to AD and mild AD dementia suggest the use of symptomatic treatment in both patient populations [10, 11]; however, neither report actual patient data. Similarly, recent data from clinical trials in eAD report baseline use of AChE inhibitors and memantine which is not necessarily in line with current regulatory EU and US approvals or clinical guidelines [12–14]. Therefore, our review aims to describe the current real-world use of AD symptomatic treatments in patients with MCI due to AD and mild AD dementia, with an emphasis on understanding the extent of AD symptomatic treatment use beyond approved labels.
METHODS
The systematic review was pre-registered, and the protocol can be accessed at https://www.crd.york.ac.uk/prospero/ (ID: CRD42022296104). Reporting aligns to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline [15] and the checklists can be found in Supplementary Tables 2 and 3.
Search, study selection, and data extraction
Searches were conducted in Embase, MEDLINE, and EBM Reviews via Ovid on November 30, 2021, to identify studies reporting on symptomatic treatment prevalence and treatment patterns in the earlier clinical stages of AD dementia. Symptomatic treatments included were AChE inhibitors such as donepezil, galantamine, and rivastigmine and the NMDA antagonist, memantine. Searches were restricted to 2009 onwards to capture the most recent evidence from the last decade and reflect current practice. This was informed by a pragmatic review that found the earliest included study was from 2009 [16]. Searches were not restricted by language. A search filter was used to identify observational studies and real-world data studies and as such would also identify systematic reviews of observational studies and real word data studies. The full search strategies are presented in Supplementary Tables 4 to 6. Reference lists of included studies and relevant systematic reviews were searched to identify additional studies. The main Embase strategy was independently peer reviewed by a second analyst, based on the Peer Review of Electronic Search Strategies (PRESS) [17].
Two reviewers independently performed title and abstract screening, followed by full paper screening using the inclusion and exclusion criteria presented in Supplementary Table 7. To summarize, full publications of observational studies (prospective/retrospective observational studies, registries, medical record reviews, and surveys) were included if they reported pharmacological symptomatic treatment patterns of patients in the early clinical stages of AD. Studies that reported reasons for treatment outside guidelines were also included. Data extraction was performed by one reviewer, and all data were checked by a second reviewer. Any disagreements were resolved by consensus or discussion with a third reviewer.
Risk of bias assessment
Study quality assessment was performed by one reviewer and checked by a second reviewer using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Prevalence Studies [18]. Any disagreements were resolved by consensus or discussion with a third reviewer. The JBI Critical Checklist for prevalence data addresses important issues of internal and external validity to consider when assessing validity of prevalence (or frequency) of treatment use regardless of study design [19].
Data analysis
A formal narrative synthesis was planned based on the reporting guideline for Synthesis Without Meta-analysis (SWiM) in systematic reviews [20]. All included studies were summarized by country and grouped according to disease stage (MCI due to AD or mild AD dementia). A summary of study design, patient characteristics, treatment pattern, and risk of bias was presented. To capture treatment patterns, the range of treatment use was reported for ‘any AChE inhibitor monotherapy’ (donepezil, rivastigmine, or galantamine), memantine monotherapy, AChE inhibitor plus memantine combinations, other combined therapies, or no symptomatic treatment. To indicate the certainty of the evidence, the findings of the synthesis were reported alongside the risk of bias, number of studies, and the study size (or range). To summarize the best quality data, studies at high risk of bias were extracted (Supplementary Table 9 (Risk of bias assessment) and 10 (Study results)) but not considered further in the data ranges for analysis and synthesis. Studies that reported on drug dose only in populations receiving symptomatic treatment were reported separately as they were not directly comparable to treatment pattern data.
Patient and public involvement
This study did not have any direct patient or public involvement.
RESULTS
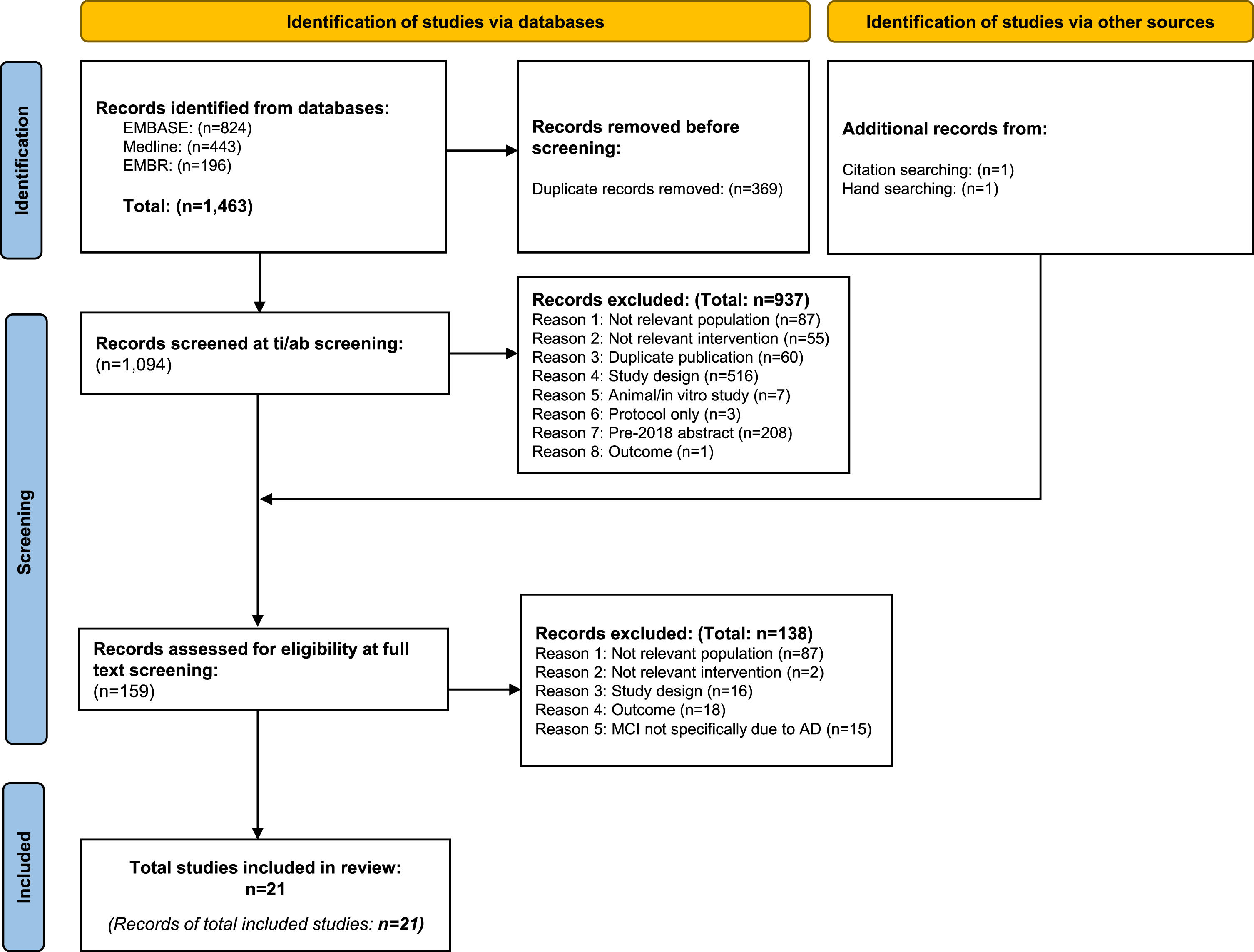
Following database searching, 1,463 records were retrieved: 369 duplicates removed and 1,094 screened at title and abstract. A total of 159 records were sought for full paper screening and of these, 21 met the criteria for inclusion in the review (Fig. 1). The 138 records excluded at full paper screening are listed together with the reason for exclusion in Supplementary Table 8. A summary of the characteristics of the included studies is presented in Table 1. Prospective and retrospective cohorts, cross-sectional studies, and a survey were all represented; however, most studies were prospective and focused on European populations. Nearly all the studies (86%) reported on mild AD dementia, four (19%) reported on MCI due to AD [21–24], and two reported on early AD (a mixed population of MCI due to AD and mild AD dementia) [25, 26]. AChE inhibitor monotherapies were the most frequently reported treatment (91% of studies) followed by AChE inhibitors and memantine (33%), memantine monotherapy (33%), or no treatment (33%). Population size ranged from 23 [27] to 2,028 [28] (IQR = 514.5). Patient characteristics were not widely reported. Where reported, mean age was broadly consistent across studies (70.8 [26] to 79.3 years [29]) whereas the proportions of gender were variable (4.4% [27] to 64.4% males [21]). Mean severity (MMSE) ranged from 22.6 [30] to 27.0 [21] with most studies reporting mean MMSE in the middle of the range for mild AD dementia (mean 23.2 [21, 31–35]). No studies reported on the reasons for discordance between guidelines and clinical practice.
Fig. 1
PRISMA diagram documenting the flow of studies during systematic review process.
Overall six studies were identified with low risk of bias [21, 23, 26, 29, 32, 36], eight were judged to have one or more ratings at high risk [25, 27, 30, 31, 34, 37–39], and seven were unclear [22, 24, 28, 33, 35, 40, 41] (summarized in Supplementary Tables 9 and 10). High risk of bias was associated with a low sample size (<100) [30, 31, 39] or having a population that may not represent the intended population (96% of study participants were female) [27]. Studies reporting the proportion of patients receiving different doses of a specific AChE inhibitor are recorded in Supplementary Table 11.
Table 1
Summary of study characteristics
| World region | Country (ies) | Study | Number of centers | Population details | Study design | Data source | Recruitment | Source of diagnosis | Source of treatment information | Guideline available* |
| MCI due to AD | ||||||||||
| North America | USA | Besser 2016 [23] | Multi-center: 31 | N = 191% Male = 95 (49.7) Mean age (SD) = 79.1 (10.3) Diagnostic criteria: MCI (according to the Petersen criteria) Mean age of onset (SD) = 76.5 (10.8)≥1 APOE ɛ4 allele = 64 (41.8%) | Case series | NACC UDSSeptember 2005 to March 2015 | Data from NACC UDS that studies participants at 31 past and present USA ADC | From NACC UDS | Self-reported | ✓ [44, 45] |
| Mild AD dementia | ||||||||||
| Asia | Taiwan | Chiu 2009 [40] | Multi-center: 22 | N = 264 Diagnostic criteria: CDR score: 1 | Prospective cohort | Non-interventional post-marketing surveillance study December 2004 to December 2006 | Outpatients with AD were recruited from 22 centers | Routine visit to institution or chart review | Routine visit to institution or chart review | NR |
| Asia | Thailand | Kongpak-watta 2019 [30] | Single center | N = 35% Male = 17 (48.6) Mean age (SD) = 77.6 (6.3) Diagnostic criteria: MMSE score: ≥20 Mean MMSE (SD) = 22.6 (2.0) | Cross-sectional study | Study conducted in a tertiary hospital in Thailand November 2017 to April 2018 | Recruited from a university affiliated tertiary hospital | Medical records | Structured interview | NR |
| Europe | Finland | Tormalehto 2015 [41] | Multi-center: 3 | N = 236% Male = 115 (48.7) Mean age (SD) = 75.7 (6.5) Diagnostic criteria: CDR: 0.5 to 1 | Prospective cohort | Study conducted over three hospital districts in middle and eastern Finland 2002 to 2006 | Newly diagnosed patients were recruited from three hospitals | Unclear | Annual interviews (reported by family care-givers) | ✓ [49] |
| Europe | Italy | Bruno 2018 [31] | Multi-center: 19 | N = 29% Male = 15 (51.7) Mean age (SD) = 76.2 (7.12) Diagnostic criteria: Diagnosis of probable AD and a MMSE score of ≤26 Mean MMSE (SD) = 23.0 | Prospective cohort | GERAS II (a prospective, multicenter, observational study) April 2013 to January 2014 | Community-dwelling patients attending secondary care centers and their primary informal caregivers were recruited | Recruiting physician | Obtained using the RUD instrument through interview with the caregiver | ✓ [49, 52] |
| Europe | Multina-tional: France, Germany, UK | Reed 2018 [32] | Multi-center: NR | N = 566% Male = 295 (52.1) Mean age (SD) = 77.3 (6.9) Diagnostic criteria: MMSE score: 20–26 Mean MMSE (SD) = 23.3 (1.6) | Prospective cohort | GERAS (an 18-month, prospective, observational study) October 2010 to September 2011 | Community-dwelling patients with AD were recruited | Recruiting physician | Obtained using the RUD instrument through interview with the caregiver | ✓ [49–51, 53, 58] |
| Europe | Multina-tional: France, Germany, UK | Wimo 2013 [29] | Multi-center: NR | N = 567% Male = 296 (52.2) Mean age (SD) = 77.3 (6.97) | Prospective cohort | GERASOctober 2010 to September 2011 | Community-dwelling patients with AD were recruited | Recruiting physician | Obtained using the RUD instrument through interview with the caregiver | ✓ [49–51, 53, 58] |
| Europe | Netherlands | Droogsma 2015 [33] | Single center | N = 335% Male = 122 (36.4) Mean age (SD) = Median: 80, IQR: 75.0–83.0 Diagnostic criteria: MMSE: ≥21–26 Mean MMSE (SD) = 23.0 | Retro-spective cohort | Memory clinic of the medical center Leeuwarden 2002 to 2012 | Community-dwelling AD patients at a large memory clinic were recruited | Data from patients attending memory clinic | Recorded at outpatient visit | ✓ [49] |
| Europe | Spain | Calvo-Perxas 2017 [28] | Multi-center: 7 | N = 2028Diagnostic criteria: CDR score: 1 | Retro-spective cohort | ReDeGi Pharmacy Unit Database -Public Health Catalan Healthcare Service 2007 to 2014 | Data from ReDeGi which records incident cases of AD diagnosed in seven hospitals | Data from HRG Pharmacy Unit database from the PCHS | Data from ReDeGi | ✓ [49, 54] |
| Europe | Spain | Martinez-Moreno 2016 [38] | Multi-center: 2 | N = 60% Male = 25 (42) Mean age (SD) = 75.1 (6.35) Diagnostic criteria: Diagnosis of mild AD dementia and a MMSE score of ≥20 | Retro-spective cohort | Retrospective observational study conducted at an outpatient clinic. May 2004 to March 2012 | Patients attending a CS program at two outpatients’ clinics | Unclear | Interview with patients performed by clinical neuropsychologist | ✓ [49, 54] |
| Europe | Spain | Olazaran 2017 [36] | Multi-center | N = 116% Male = 53 (45.7) Mean age (SD) = 74.7 (7.9) Diagnostic criteria: MMSE 21–26 | Prospective cohort | GERASIIApril 2013 to December 2013 | Community-dwelling patients attending secondary care centers and their primary informal caregivers were recruited | Recruiting physician | Obtained using the RUD instrument through interview with the caregiver | ✓ [49, 54] |
| Europe | Spain | Vinuela 2021 [37] | Single center | N = 60% Male = 23 (38.3) Mean age (SD) = 75.8 (9.0) Diagnostic criteria: Mild AD dementia and an MMSE >20 | Prospective cohort | Single center, prospective, non-interventional study May 2017 to June 2018 | Consecutive patients with diagnosis of mild AD dementia were recruited from one center | Unclear | Unclear – likely determined as part of the study | ✓ [49, 54] |
| Europe | Sweden | Mesterton 2010 [34] | Multi-center | N = 91% Male = 45 (49) Mean age (SD) = 76.8 (7.4) Diagnostic criteria: MMSE 20–26 Mean MMSE (SD) = 23.7 (2.6) | Cross-sectional study | Medical records, interviews, self administered questionnaires August 2007 | Investigators at 16 study centers screened their patient lists for patients who met the inclusion criteria | Medical records, interviews, self administered questionnaires | Medical records, interviews, self administered questionnaires | ✓ [49] |
| Europe | Sweden | Wattmo 2016 [35] | Multi-center: 14 | N = 734% Male = 261 (36) Mean age (SD) = 75.2 (6.8) Diagnostic criteria: MMSE score: 20–26 Mean MMSE (SD) = 23.4 (2.0) Mean age of onset (SD) = 72.3 (7.1) APOE ɛ4 carrier = 241 (31) | Prospective cohort | SATS: a 3- year, prospective, open, non-randomized multicenter study to assess long-term AChEi treatment in routine clinical practice | Community dwelling out-patients with or without home-help services at AD diagnosis were recruited | Unclear | Recorded as part of the study – no further information | ✓ [49] |
| South America | Argentina | Chaves 2014 [27] | Single center | N = 23% Male = 1 (4.4) Diagnostic criteria: CDR: 1Mean age of onset (SD) = 82.4 (4.9) | Retrospective cohort | Computerized medical records of Hospital Italiano de Buenos Aires January 2002 to January 2010 | Data from computerized medical records of Hospital Italiano de Buenos Aires. | Computerized medical records of Hospital Italiano de Buenos Aires. | Computerized medical records of Hospital Italiano de Buenos Aires. | NR |
| South America | Argentina | Rojas 2010 [39] | Single center | N = 38% Male = 16 (42.1) Mean age (SD) = 71.0 (9.83) Diagnostic criteria: CDR: 1 | Prospective cohort | Non-interventional, uncontrolled, open-label, longitudinal study at the Memory Laboratory at Hospital Zubizarreta March 2008 to March 2009 | Patients attending the Memory Laboratory at Hospital Zubizarreta were recruited | Unclear | Recorded as part of the study – no further information | NR |
| Early AD | ||||||||||
| Europe | France | Epelbaum 2019 [26] | Multi-center: 458 | N = 195% Male = 87 (44.9) Mean age (SD) = 70.8 (0.6) Diagnostic criteria: MMSE ≥20 Mean MMSE (SD) = 24.7 (0.2) | Retro-spective cohort | Electronic clinical records database from 11 memory research and resource centers | Data from electronic clinical records from 11 memory research and resource centers | Electronic clinical records database | Electronic clinical records database | ✓ [49, 58] |
| North America | USA | Wang 2014 [25] | Single center | N = 44 Diagnostic criteria: Very mild or mild AD dementia (CDR 0.5 and CDR 1) | Retro-spective study | Community dwelling volunteers enrolled in studies of ageing and memory at Washington University in St Louis. | Community dwelling volunteers with mild or very mild AD dementia who were enrolled in studies of ageing and memory at Washington University in St Louis were recruited | Study clinician | Unclear – likely determined as part of the study | ✓ [44, 45] |
| Both MCI due to AD and mild AD dementia | ||||||||||
| Europe | Germany | Hessmann 2018 [22] | Multi-center: 5 | MCI due to AD: N = 51 Diagnostic criteria: MMSE score: 27–30 Mild AD dementia: N = 130 Diagnostic criteria: MMSE: 20–26 | Cross-sectional | Cross-sectional study including patients from five study sites in Marburg-Biedenkopf, a rural region in Hessen, Germany | Patients with mild cognitive effects and AD dementia were consecutively recruited with their primary carers from five study sites | Unclear | Standardized questionnaire | ✓ [49, 51] |
| North America | Multina-tional: Canada, USA | Schneider 2011 [21] | Multi-center: 59 | MCI due to AD: N = 402% Male = 259 (64.4%) Mean age (SD) = 74.8 (7.42) Diagnostic criteria: MMSE score: 24–30 Mean MMSE (SD) = 27.0 (1.78)APOE ɛ4 genotype carriers, 1 or 2 alleles = 215 (53.5%) Mild AD dementia: N = 188% Male = 99 (52.7%) Mean age (SD) = 75.3 (7.56) Diagnostic criteria: MMSE score: 21–26 Mean MMSE (SD) = 23.3 (2.04)APOE ɛ4 genotype carriers, 1 or 2 alleles = 124 (66.0%) | Prospective cohort | ADNI database | Data from ADNI database that recruited a community sample of MCI and AD patients from 59 sites | Unclear | Data from ADNI database | ✓ [44, 45, 48] |
| Worldwide | Multina-tional: France, Germany, Japan, the UK and the USA | Podhorna 2020 [24] | Multi-center | MCI due to AD/prodromal AD: N = 331 Mild AD dementia: N = 1175 | Survey of online questionnaires and patient record forms from a survey of physicians | Online questionnaires and patient record forms from a survey of physicians | Physicians were instructed to startwith surname letters H, M or K and select the first patient with a diagnosis of MCI/prodromalAD, mild or moderate AD dementia | Study physician | Participating physicians completed online questionnaires and patient record forms | ✓ [44, 45, 49–51, 53, 58] |
AChEi, acetylcholinesterase inhibitor; ADC, Alzheimer’s Disease Centers; AD, Alzheimer’s disease; ADNI, Alzheimer’s Disease Neuroimaging Initiative; APOE, apolipoprotein E; CDR, Clinical Dementia Rating; CS, cognitive stimulation; HRG, health region of Girona; IQR, interquartile range; MCI, mild cognitive impairment; MMSE, Mini-Mental State Exam; N, number; NACC, National Alzheimer’s Coordinating Center; NR, not recorded; PCHS, Public Health Catalan Healthcare Service; ReDeGi, Registry of Dementias of Girona; RUD, resource utilization in dementia; SATS, the Swedish Alzheimer treatment study; SD, standard deviation; UDS, uniform data set; UK, United Kingdom; USA, United States of America. *In Supplementary Table 1.
There were multiple sources of bias in the constituent studies. Some studies were limited due to their retrospective nature [25–28, 33, 38] and many studies used medical records [26, 27, 34] or databases as their source of data [21, 23, 28, 29, 31, 32, 36]. Retrospective studies of medical records or databases are prone to bias as they are designed to assess pre-existing data which may be subject to recall bias or misclassification bias and data on confounding factors may be missing. The information on diagnosis was often established by the recruiting physician [24, 25, 29, 31, 32, 36] or from medical records [27, 30, 34, 40] or databases [23, 26, 28]. Diagnostic criteria were reported but with no additional methodological details [21, 22, 35, 37–39, 41]. A validated tool (Resource Utilization in Dementia (RUD)) was used to determine treatment records in four studies, [29, 31, 32, 36] while others used questionnaires or interviews with patients and/or carers [22–24, 30, 34, 38, 41] or databases [21, 26, 28]. The use of a validated tool is considered a more robust method as the tool has been tested for reliability and is considered fit for purpose. The study population is likely to be representative of real-world practice as community dwelling patients were recruited in seven studies [25, 29, 32, 33, 35–37] and the majority of studies were multicenter [21–24, 26, 28, 29, 31, 32, 34–36, 38, 40, 41].
Table 2 summarizes prevalence data for symptomatic treatment patterns in MCI due to AD from four studies across six countries with low or unclear risk of bias. In Germany and North America, 18% [22] to 35% [21] of patients received any AChE inhibitors (including individual AChE inhibitors (three studies; n = 631 [21, 23, 42]), 7% [23] to 8% [22] received memantine (two studies; n = 229), and 9% [21] received combination treatment (one study; n = 402). Of the population receiving symptomatic treatment, 9% to 87% had AChE inhibitors, 10% had memantine, and 4% had combined treatment (one study; n = 331) [24]. Patients receiving no treatment ranged from 41 [24] to 54% [21] (two studies; n = 733).
Table 2
Summary of symptomatic treatment patterns in MCI due to AD by country
| Study details | Symptomatic treatment patterns (n/N (%), range) | ||||||
| Region | Country (ROB, author, study design and size) | Definition | Any AChEi monotherapy | Memantine monotherapy | AChEi + Memantine | Other | No symptomatic treatment |
| Europe | Germany••Hessmann 2018 [22] Cross-sectional study N = 51 | Treatment use /Total MCI due to AD population | 9/51 (17.6%) – 16/51 (31.4%) | 4/51 (7.8%) | NR | NR | NR |
| North America | Canada & USA•Schneider 2011 [21] Prospective cohort N = 402 | Treatment use /Total MCI due to AD population | 141/402 (35.1%) | 46/402 (11.4%)** | 36/402 (9.0%) | AChEi monotherapy or in combination with memantine: 177/402 (44.0%) | 215/402 (53.5%) |
| Treatment at baseline/ MCI due to AD patients receiving AChEi | NR | NR | NR | AChEi monotherapy or in combination with memantine: 9/177 (5.1%) – 150/177 (84.7%) | NR | ||
| USA••Besser 2016 [23] Case series N = 178 | Treatment use /Total MCI due to AD population | 33/178 (18.5%) | 12/178 (6.7%) | NR | NR | NR | |
| Worldwide | France, Germany, Japan, UK & USA••Podhorna 2020 [24] Survey N = 331 | Prescription rates of treatments/MCI due to AD patients receiving AD treatment | NR/128 (9%) – NR/128 (87%) | NR/128 (10%) | NR/128 (4%) | NR | NR |
| Treatment use /Total MCI due to AD population | NR | NR | NR | NR | NR/331 (41%) | ||
AChEi, acetylcholinesterase inhibitor; AD, Alzheimer’s disease; MCI, mild cognitive impairment; NR, not recorded; UK, United Kingdom; USA, United States of America. *Any or an individual AChEi. **Likely to report mixed population of monotherapy and combination therapy. • low risk of bias; •• unclear risk of bias.
Table 3 summarizes the prevalence data for symptomatic treatment patterns in mild AD dementia from ten studies across ten different countries with low or unclear risk of bias. In mild AD dementia patients from Europe or North America, 13 [22] to 89% [41] (IQR = 32.8) received any AChE inhibitor (46% [21] to 89% [41] received multiple AChE inhibitors) (6 studies; n = 3,715 [21, 22, 28, 29, 32, 41]), 1 [29] to 21% [22] (IQR = 15.6) received memantine (5 studies, n = 3,527 [21, 28, 29, 32, 41]), and 0.4 [24] to 39% [21] (IQR = 29.8) received a combination of both (four studies, n = 3018 [21, 28, 32, 41]). There was insufficient data to demonstrate any differences by region. Of the population receiving symptomatic treatment, 10% [36] to 88% [24] received AChE inhibitors, 7% [24] to 10% [36] received memantine, and 3% [24] to 12% [36] received combined therapy (two studies; n = 1271). Patients not treated ranged from 9% [21] to 26% [28] (IQR = 10.4) (five studies, n = 4073 [21, 24, 28, 32, 36]).
Table 3
Summary of symptomatic treatment patterns in mild AD dementia by country
| Study details | Symptomatic treatment patterns | |||||||
| Region | Country (ROB, author, study design and size) | Definition | Any AChEi monotherapy* | Memantine monotherapy | AChEi + Memantine | Other | No symptomatic treatment | |
| Europe | Finland••Tormalehto 2015 [41] Prospective cohort N = 236 | Treatment use /Total AD population | 210/236 (89.0%) | 16/236 (7.0%) | 1/236 (0.4%) | NR | NR | |
| France•Wimo 2013 [29] Prospective observational study N = 138 | Treatment use /Total AD population | NR/138 (81.9%) | NR/138 (13.8%) | NR | NR | NR | ||
| Germany••Hessmann 2018 [22] Cross-sectional study N = 130 •Wimo 2013 [29] Prospective observational study N = 228 | Treatment use /Total AD population | 17/130 (13.1%) – NR/228 (73.7%) | NR/228 (19.7%) – 27/130 (20.8%) | NR | NR | NR | ||
| Netherlands••Droogsma 2015 [33] Retrospective cohort N = 335 | Treatment at baseline/AD patients receiving AChEi treatment | 8/335 (2.4%) – 327/335 (97.6%) | NR | NR | NR | NR | ||
| Spain••Calvo-Perxas 2017 [28] Retrospective cohort N = 2,028 •Olazaran 2017 [36] Prospective observational study N = 116 (N = 96 received AD treatment) | ||||||||
| Treatment use /Total AD population | 1249/2028 (61.6%) | 83/2028 (4.1%) | 170/2028 (8.4%) | NR | 20/116 (17.2%) – 526/2028 (25.9%) | |||
| Treatment at baseline/AD patients receiving treatment | 10/96 (10.4%) – 71/96 (74%) | 10/96 (10.4%) | 11/96 (11.5%) | NR | NR | |||
| Sweden••Wattmo 2016 [35] Prospective open non-randomised study N = 734 | Treatment use /AD patients receiving AChEi treatment | NR/734 (22.0%) – NR/734 (48%) | NR | NR | NR | NR | ||
| UK •Wimo 2013 [29] Prospective observational study N = 201 | Treatment use /Total AD population | NR/201 (82.6%) | NR/201 (1.0%) | NR | NR | NR | NR | |
| Multinational (France, Germany, UK)•Reed 2018 [32] Prospective observational study N = 566 | Treatment use /Total AD population | 411/566 (72.6%) | 41/566 (7.2%) | 26/566 (4.6%) | NR | 88/566 (15.5%) | ||
| North America | Multinational (Canada & USA)•Schneider 2011 [21] Prospective cohort N = 188 | Treatment use /Total AD population | 86/188 (45.7%) | 86/188 (45.7%)** | 73/188 (38.8%) | AChEi monotherapy or in combination with memantine: 159/188 (84.6%) | 16/188 (8.5%) | |
| Worldwide | Multinational (France, Germany, Japan, UK & USA)••Podhorna 2020 [24] Survey N = 1,175 | Treatment at baseline/AD patients receiving treatment | NR/809 (7%) – NR/809 (88%) | NR/809 (7%) | NR/809 (3%) | NR | NR | |
| Treatment use /Total AD population | NR | NR | NR | NR | NR/1175 (19%) |
AChEi, acetylcholinesterase inhibitor; AD, Alzheimer’s disease; MCI, mild cognitive impairment; NR, not recorded; UK, United Kingdom; USA, United States of America. Denominator is the population with mild AD. *Any or an individual AChEi. **Likely to report mixed population of monotherapy and combination therapy. • low risk of bias; •• unclear risk of bias.
Table 4 summarizes symptomatic treatment patterns in early AD, a mixed population of MCI due to AD and mild AD dementia). Of patients treated for early AD, 15% to 80% received any AChE inhibitor while 70% received no symptomatic treatment (one French study; n = 195) [26].
Table 4
Summary of symptomatic treatment patterns in early AD by country
| Study details | Symptomatic treatment patterns (%, range) | ||||||
| Region | Country (ROB, author, study design and size) | Definition | Any AChEi monotherapy* | Memantine monotherapy | AChEi + Memantine | Other | No symptomatic treatment |
| Europe | •FranceRetrospective cohort Epelbaum 2019 [26] N = 195 | Treatment at baseline/eAD treatment | 9/60 (15%) – 48/60 (80%) | NR | NR | NR | NR |
| Treatment use /Total eAD population | NR | NR | NR | NR | 135/195 (69.2%) | ||
AChEi, acetylcholinesterase inhibitor; eAD, early Alzheimer’s disease; MCI, mild cognitive impairment; NR, not recorded; UK, United Kingdom; USA, United States of America. Denominator is the population with early AD. *Any or an individual AchEi. • low risk of bias.
DISCUSSION
Summary of findings
Twenty-one studies were included in this review of symptomatic treatment patterns in the early clinical stages of AD. Findings confirm that patients being treated primarily with AChE inhibitors and to a lesser extent memantine and combination therapy. A proportion of patients remain untreated. Studies that reported on drug dose only in populations receiving symptomatic treatment were reported separately as they were not directly comparable to treatment pattern data.
Worldwide, 18 to 35% of patients diagnosed with MCI due to AD received any AChE inhibitor (three studies; n = 631 [21, 23, 42]), 7 to 8% memantine (two studies; n = 229 [22, 23]), and 9% combination therapy (one study; n = 402 [21]). Patients receiving no treatment ranged from 41 to 54% (two studies; n = 733 [21, 24]). Worldwide, in mild AD dementia patients, 13 to 89% received any AChE inhibitor (six studies; n = 3,715 [21, 22, 28, 29, 32, 41]), 1 to 21% memantine (five studies, n = 3,527), and 0.4 to 39% combination therapy (four studies, n = 3018, [21, 28, 32, 41]). Patients receiving no treatment ranged from 9 to 26% (five studies, n = 4073 [21, 24, 28, 32, 36]).
Treatment patterns for MCI due to AD were broadly similar in Europe and North America. AChE inhibitor use in Europe was 31% [22] and North America ranged from 19 to 35% [21, 23]. Use of memantine was lower in Europe (8%) [22] and North America (7%) [23]. Use of combination therapy was 9% in North America [21] and not reported in Europe [22]. Patients receiving no symptomatic treatment ranged from 41% (Internationally) to 54% (North America).
For mild AD dementia, use of AChE inhibitor was higher in Europe (up to 89% [41]) than in North America (46%) [21]. Use of memantine was low in Europe ranging from 7% [41] to 21% [22] and not clearly reported in North America. Combination therapy was low across Europe (0.4% [41] to 8% [28] but higher in North America (39%) [21]. The proportion of patients not treated was low in North America (9%) [21] and slightly higher in Europe (16% [32] to 26% [28]), and internationally (19%) [24].
The observed variations between regions may be explained by differences in the reimbursement status of the symptomatic treatments as well as differences in access to treatment (e.g., availability of generic medicines) and healthcare funding mechanisms (public and/or private).
Comparison to other reviews
To our knowledge, this is the first systematic review to investigate treatment patterns in MCI due to AD and mild AD dementia without geographical restrictions. A similar review was published in 2018 and focused on Japanese data but found no studies that reported on treatment or prescribing patterns in the management of cognitive function among patients with AD dementia in Japan [43]. Our study supports this view, and we included only one study, published in 2020, presenting Japanese data combined with France, Germany, UK, and US [24]. In a European survey of clinicians, a small proportion of the respondents routinely prescribed AChE inhibitor (21%) and memantine (13%) to patients with MCI due to AD [11]. In a Delphi survey of German clinical experts, the consensus reached was that most mild AD dementia patients were likely to receive AChE inhibitor, followed by memantine and 53% of patients are expected to receive no symptomatic treatment [10]. Our review is broadly in line with these surveys; however, we reported lower rates for ‘no treatment use’ in Europe (14% [36] to 26% [28]); no data was identified for ‘no treatment use’ in Germany. This disparity may be due to differences in the methodology and data reported, i.e., these surveys report the proportion of physicians prescribing treatments [11] or the clinical expert opinion of what patients are likely to receive, rather than actual proportion of patients receiving treatment or no treatment [10].
Implications
The review highlights that MCI due to AD patients are receiving treatment with AChE inhibitor, memantine, or combination therapy not reflected in the current guidelines and approvals [7–9]. Similarly, mild AD dementia patients are being treated with AChE inhibitors, memantine, or combination of AChE inhibitor with memantine where only AChE inhibitor is recommended and memantine is approved for moderate and severe AD treatments only [7–9]) In addition, up to 26% of mild AD dementia patients received no treatment [28], which is discordant with current guidelines [44–54]. Recent clinical trials report similar findings, where baseline data reported patients were receiving symptomatic treatment [12–14]. The current review aimed to capture reasons for non-compliance with guidelines; however, no reasons were explicitly reported, which could indicate limited evidence to support the recommendation and use of treatment options. The lack of approved treatments for MCI due to AD as well as limited evidence are likely to be the main reasons for no treatment in this population. Although there are approved treatments for mild AD dementia, potential reasons for no treatment may include lack of treatment availability, affordability issues, or patient refusal. Broadly, in psychiatry and more specifically in the treatment of dementia, prescribing patterns outside the approved drug labels are not uncommon and is mainly due to limitations of the evidence. Although some divergence was expected between guidelines and clinical practice due to their interpretation, the guidelines appear completely discordant with practice rather than just not ideally aligned. The differences between current guidelines and clinical practice, together with the recent approval of aducanumab in the US and the ongoing late-stage development of other disease modifying treatments presents a new opportunity for a consensus review of current guidelines [55].
Limitations
Our searches were restricted to 2009 onwards to reflect current practice, but it is important to acknowledge that there may be missing evidence. Furthermore, our supplementary searches were limited to reference checking and conference proceedings.
Data on the included patient characteristics, study methodology, or treatment dosage details were not widely reported by the included studies and therefore did not allow a closer interrogation of the data. Limited information was reported on missing data or timing of diagnosis and prescription such that changes in diagnosis or treatment may not be adequately captured. Such findings are common in real-world data, and a recent report [56] found that a third of all real-world evidence studies had limited reporting reflecting the challenges of meta-research of observational data. The GERAS [29, 32] and GERAS II [31, 36] databases featured quite heavily in our review focusing on different countries or timeframes. It is likely there is some overlap in the patients in these studies. The variance in the denominator population description highlights the challenge of heterogeneity: ‘mild AD dementia’, ‘mild AD dementia receiving treatment’, or ‘mild AD dementia receiving AChE inhibitors’; this variation limits comparisons across studies and countries/regions. A proportion of studies had low sample size (<100) but overall, the majority were in large studies with no overall concerns for risk of bias.
In our review, we found limited numbers of publications on MCI due to AD. Very few used the term prodromal AD [11, 24]. Although treatment patterns are reported, this is likely to be an under-representation of the population as MCI due to AD is inadequately identified in affected patients [57].
No reasons for the use of symptomatic AD treatments outside of their approved labels were identified. Future research should be designed to understand why clinicians are prescribing treatments outside of the current guidelines to patients with MCI due to AD and mild AD dementia.
Conclusions
Our systematic review demonstrates that while as per approved treatment labels and treatment guidelines, the use of symptomatic treatment is not recommended in MCI due to AD and only limited treatment is recommended in mild AD dementia, there is widespread real-world clinical use. These findings confirm the unmet medical need in early AD and together with the emergence of disease modifying treatments presents an opportunity to revise AD clinical treatment guidelines to accurately reflect current practice.
ACKNOWLEDGMENTS
Mtech Access were funded by F. Hoffmann-La Roche Ltd. to conduct this systematic review.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0471r2).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-220471.
REFERENCES
[1] | Nichols E , Szoeke CEI , Vollset SE , Abbasi N , Abd-Allah F , Abdela J , Aichour MTE , Akinyemi RO , Alahdab F , Asgedom SW , Awasthi A , Barker-Collo SL , Baune BT , Béjot Y , Belachew AB , Bennett DA , Biadgo B , Bijani A , Bin Sayeed MS , Brayne C , Carpenter DO , Carvalho F , Catalá-López F , Cerin E , Choi J-YJ , Dang AK , Degefa MG , Djalalinia S , Dubey M , Duken EE , Edvardsson D , Endres M , Eskandarieh S , Faro A , Farzadfar F , Fereshtehnejad S-M , Fernandes E , Filip I , Fischer F , Gebre AK , Geremew D , Ghasemi-Kasman M , Gnedovskaya EV , Gupta R , Hachinski V , Hagos TB , Hamidi S , Hankey GJ , Haro JM , Hay SI , Irvani SSN , Jha RP , Jonas JB , Kalani R , Karch A , Kasaeian A , Khader YS , Khalil IA , Khan EA , Khanna T , Khoja TAM , Khubchandani J , Kisa A , Kissimova-Skarbek K , Kivimäki M , Koyanagi A , Krohn KJ , Logroscino G , Lorkowski S , Majdan M , Malekzadeh R , März W , Massano J , Mengistu G , Meretoja A , Mohammadi M , Mohammadi-Khanaposhtani M , Mokdad AH , Mondello S , Moradi G , Nagel G , Naghavi M , Naik G , Nguyen LH , Nguyen TH , Nirayo YL , Nixon MR , Ofori-Asenso R , Ogbo FA , Olagunju AT , Owolabi MO , Panda-Jonas S , Passos VMdA , Pereira DM , Pinilla-Monsalve GD , Piradov MA , Pond CD , Poustchi H , Qorbani M , Radfar A , Reiner RC Jr. , Robinson SR , Roshandel G , Rostami A , Russ TC , Sachdev PS , Safari H , Safiri S , Sahathevan R , Salimi Y , Satpathy M , Sawhney M , Saylan M , Sepanlou SG , Shafieesabet A , Shaikh MA , Sahraian MA , Shigematsu M , Shiri R , Shiue I , Silva JP , Smith M , Sobhani S , Stein DJ , Tabarés-Seisdedos R , Tovani-Palone MR , Tran BX , Tran TT , Tsegay AT , Ullah I , Venketasubramanian N , Vlassov V , Wang Y-P , Weiss J , Westerman R , Wijeratne T , Wyper GMA , Yano Y , Yimer EM , Yonemoto N , Yousefifard M , Zaidi Z , Zare Z , Vos T , Feigin VL , Murray CJL ((2019) ) Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 18: , 88–106. |
[2] | Alzheimer’s Association ((2020) ) 2020 Alzheimer’s disease facts and figures. Alzheimers Dement 16: , 391–460. |
[3] | Marasco RA ((2020) ) Current and evolving treatment strategies for the Alzheimer disease continuum. Am J Manag Care 26: , S167–s176. |
[4] | Knopman DS , Amieva H , Petersen RC , Chételat G , Holtzman DM , Hyman BT , Nixon RA , Jones DT ((2021) ) Alzheimer disease. Nat Rev Dis Primers 7: , 33. |
[5] | Petersen RC , Lopez O , Armstrong MJ , Getchius TSD , Ganguli M , Gloss D , Gronseth GS , Marson D , Pringsheim T , Day GS , Sager M , Stevens J , Rae-Grant A ((2018) ) Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 90: , 126–135. |
[6] | Yuan J , Maserejian N , Liu Y , Devine S , Gillis C , Massaro J , Au R ((2021) ) Severity distribution of Alzheimer’s disease dementia and mild cognitive impairment in the Framingham Heart Study. J Alzheimers Dis 79: , 807–817. |
[7] | Alzheimer’s Association, FDA-approved treatments for Alzheimer’s, https://www.alz.org/media/documents/fda-approved-treatments-alzheimers-ts.pdf, Accessed February 2, 2022. |
[8] | Alzheimer Europe, Alzheimer’s Dementia, https://www.alzheimer-europe.org/dementia/alzheimers-dementia, Accessed February 16, 2022. |
[9] | Winslow BT , Onysko MK , Stob CM , Hazlewood KA ((2011) ) Treatment of Alzheimer disease. Am Fam Physician 83: , 1403–1412. |
[10] | Kohlscheen KM , Jacob C , Braun S , Mittendorf T ((2018) ) Pharmaceutical treatment of mild Alzheimer’s disease in Germany - results from a delphi panel. Value Health 21: (Suppl 3), S331. |
[11] | Bertens D , Vos S , Kehoe P , Wolf H , Nobili F , Mendonca A , Van Rossum I , Hort J , Molinuevo JL , Heneka M , Petersen R , Scheltens P , Visser PJ ((2019) ) Use of mild cognitive impairment and prodromal AD/MCI due to AD in clinical care: A European survey. Alzheimers Res Ther 11: , 74. |
[12] | Lin H , Ostrowitzki KM , Sink M , Millar L , Warren F , Smith D , Clayton T , Bittner R , Fuji RN , Quartino A , Mackey H , Rabbia M , Yule S , Fontoura P , Doody R ((2018) ) Baseline characteristics from a phase III trial of crenezumab in early (prodromal-to-mild) Alzheimer’s disease. Presented at Alzheimer’s Association International Conference (AAIC), Chicago, IL. |
[13] | Swanson CJ , Zhang Y , Dhadda S , Wang J , Kaplow J , Lai RYK , Lannfelt L , Bradley H , Rabe M , Koyama A , Reyderman L , Berry DA , Berry S , Gordon R , Kramer LD , Cummings JL ((2021) ) A randomized, double-blind, phase 2b proof-of-concept clinical trial in early Alzheimer’s disease with lecanemab, an anti-Aβ protofibril antibody. Alzheimers Res Ther 13: , 80. |
[14] | Cohen S, Murphy J, Harrison J, Jaeger J, Yang L, Wu S, Ping H, Castrillo-Viguera C, Budd Haeberlein S, Heterogeneity in symptom progression and treatment response: An analysis of participants with early Alzheimer’s disease from the EMERGE Aducanumab trial, https://biogen.gcs-web.com/static-files/41808e3a-b261-4f75-ab66-fe4a401ef4ec, Accessed March 30, 2022. |
[15] | PRISMA Group, PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [Internet], https://prisma-statement.org/, Accessed November 1, 2022. |
[16] | Joao Garcia M ((2021) ) Pragmatic literature review: Pharmacological treatment patterns in early Alzheimer’s disease [Unpublished Work]. F. Hoffmann-La Roche Ltd 25. |
[17] | McGowan J , Sampson M , Salzwedel DM , Cogo E , Foerster V , Lefebvre C ((2016) ) PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol 75: , 40–46. |
[18] | The Joanna Briggs Institute, The Joanna Briggs Institute critical appraisal tools for use in JBI Systematic Reviews: Checklist for prevalence studies, https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Prevalence_Studies2017_0.pdf, Accessed November 1, 2022. |
[19] | Munn Z , Moola S , Riitano D , Lisy K ((2014) ) The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag 3: , 123–128. |
[20] | Campbell M , McKenzie JE , Sowden A , Katikireddi SV , Brennan SE , Ellis S , Hartmann-Boyce J , Ryan R , Shepperd S , Thomas J , Welch V , Thomson H ((2020) ) Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline, BMJ 368: , l6890. |
[21] | Schneider LS , Insel PS , Weiner MW ((2011) ) Treatment with cholinesterase inhibitors and memantine of patients in the Alzheimer’s disease neuroimaging initiative. Arch Neurol 68: , 58–66. |
[22] | Hessmann P , Dodel R , Baum E , Muller MJ , Paschke G , Kis B , Zeidler J , Klora M , Reese JP , Balzer-Geldsetzer M ((2018) ) Use of antidementia drugs in German patients with Alzheimer’s disease. Int Clin Psychopharmacol 33: , 103–110. |
[23] | Besser LM , Litvan I , Monsell SE , Mock C , Weintraub S , Zhou XH , Kukull W ((2016) ) Mild cognitive impairment in Parkinson’s disease versus Alzheimer’s disease. Parkinsonism Relat Disord 27: , 54–60. |
[24] | Podhorna J , Winter N , Zoebelein H , Perkins T ((2020) ) Alzheimer’s treatment: Real-world physician behavior across countries. Adv Ther 37: , 894–905. |
[25] | Wang L , Day J , Roe CM , Brier MR , Thomas JB , Benzinger TL , Morris JC , Ances BM ((2014) ) The effect of APOE epsilon4 allele on cholinesterase inhibitors in patients with Alzheimer disease: Evaluation of the feasibility of resting state functional connectivity magnetic resonance imaging. Alzheimer Dis Assoc Disord 28: , 122–127. |
[26] | Epelbaum S , Paquet C , Hugon J , Dumurgier J , Wallon D , Hannequin D , Jonveaux T , Besozzi A , Pouponneau S , Hommet C , Blanc F , Berly L , Julian A , Paccalin M , Pasquier F , Bellet J , Boutoleau-Bretonniere C , Charriau T , Rouaud O , Madec O , Mouton A , David R , Bekadar S , Fabre R , Liegey E , Deberdt W , Robert P , Dubois B ((2019) ) How many patients are eligible for disease-modifying treatment in Alzheimer’s disease? A French national observational study over 5 years, BMJ Open 9: , e029663. |
[27] | Chaves M , Toral A , Bisonni A , Rojas JI , Fernandez C , Garcia Basalo MJ , Matusevich D , Cristiano E , Golimstok A ((2014) ) Treatment with vitamin D and slowing of progression to severe stage of Alzheimer’s disease. Rev Argent Neurol Psiquiatr 25: , 85–91. |
[28] | Calvo-Perxas L , Turro-Garriga O , Lozano-Gallego M , Marquez F , Garre-Olmo J , Gich J , Molins A , Ramio L , Serena J , Silva Y , Robles R , Hernandez M , Lozano M , Pericot I , Vilalta-Franch J , Estrada AT , Llinas J , Lopez-Pousa S , Solano B , Terceno M , Alsina E , de Eugenio R , Hernandez E , Flaque M , Carmona O , Cullell M , Osuna T , del Mar Fernandez M , Bisbe J , Linares M , Daniel FM , Vallmajo N , Perkal H , Vinas M , Casas I , Turbau J , Cuy JM , Manzano A , Roig AM , Coromina J , Soto MP ((2017) ) Trends in the prescription and long-term utilization of antidementia drugs among patients with Alzheimer’s disease in Spain: A cohort study using the registry of dementias of Girona. Drugs Aging 34: , 303–310 . |
[29] | Wimo A , Reed CC , Dodel R , Belger M , Jones RW , Happich M , Argimon JM , Bruno G , Novick D , Vellas B , Haro JM ((2013) ) The GERAS study: A prospective observational study of costs and resource use in community dwellers with Alzheimer’s disease in three European countries - study design and baseline findings. J Alzheimers Dis 36: , 385–399. |
[30] | Kongpakwattana K , Dejthevaporn C , Krairit O , Dilokthornsakul P , Mohan D , Chaiyakunapruk N ((2019) ) A real-world evidence analysis of associations among costs, quality of life, and disease-severity indicators of Alzheimer’s disease in Thailand. Value Health 22: , 1137–1145. |
[31] | Bruno G , Mancini M , Bruti G , Dell’Agnello G , Reed C ((2018) ) Costs and resource use associated with Alzheimer’s disease in Italy: Results from an observational study. J Prev Alzheimers Dis 5: , 55–64. |
[32] | Reed C , Belger M , Dell’Agnello G , Kahle-Wrobleski K , Sethuraman G , Hake A , Raskin J , Henley D ((2018) ) Representativeness of European clinical trial populations in mild Alzheimer’s disease dementia: A comparison of 18-month outcomes with real-world data from the GERAS observational study. Alzheimers Res Ther 10: , 36. |
[33] | Droogsma E , Van Asselt D , Diekhuis M , Veeger N , Van Der Hooft C , De Deyn PP ((2015) ) Initial cognitive response to cholinesterase inhibitors and subsequent long-term course in patients with mild Alzheimer’s disease. Int Psychogeriatr 27: , 1323–1333. |
[34] | Mesterton J , Wimo A , By A , Langworth S , Winblad B , Jonsson L ((2010) ) Cross sectional observational study on the societal costs of Alzheimer’s disease. Curr Alzheimer Res 7: , 358–367. |
[35] | Wattmo C , Minthon L , Wallin AK ((2016) ) Mild versus moderate stages of Alzheimer’s disease: Three-year outcomes in a routine clinical setting of cholinesterase inhibitor therapy. Alzheimers Res Ther 8: , 7. |
[36] | Olazaran J , Aguera-Ortiz L , Josep MA , Reed C , Ciudad A , Andrade P ((2017) ) Costs and quality of life in community-dwelling patients with Alzheimer’s disease in Spain: Results from the GERAS II observational study. Int Psychogeriatr 29: , 2081–2093 . |
[37] | Vinuela F , Barro A ((2021) ) Assessment of a potential synergistic effect of Souvenaid R in mild Alzheimer’s disease patients on treatment with acetylcholinesterase inhibitors: An observational, non-interventional study. J Alzheimers Dis 80: , 1377–1382. |
[38] | Martinez-Moreno M , Cerulla N , Chico G , Quintana M , Garolera M ((2016) ) Comparison of neuropsychological and functional outcomes in Alzheimer’s disease patients with good or bad response to a cognitive stimulation treatment: A retrospective analysis. Int Psychogeriatr 28: , 1821–1833. |
[39] | Rojas G , Bartoloni L , Serrano C , Dillon C , Allegri R ((2010) ) [Naturalist observational study on effectiveness of drug treatment of a cohort of patients with Alzheimer type dementia]. Neurologia Argentina 2: , 21–28. |
[40] | Chiu PY , Dai DE , Hsu HP , Lee C , Lin JJ , Kuo HC , Huang YC , Liu YC , Tsai CP ((2009) ) Safety/Tolerability and efficacy of rivastigmine in Taiwanese patients with Alzheimer’s disease: A prospective post-marketing surveillance study. Clin Drug Investig 29: , 729–738. |
[41] | Tormalehto SM , Martikainen JA , Vaatainen ST , Hallikainen IT , Hallikainen M , Bell JS , Koivisto AM ((2015) ) Use of anti-dementia drugs in relation to change in cognition, behavior, and functioning in Alzheimer’s disease over a three-year period: Kuopio ALSOVA study. J Alzheimers Dis 48: , 1033–1041. |
[42] | Chow TW , Varpetian A , Moss T , Vinters HV , Marquez S , Miller C ((2010) ) Alzheimer’s disease neuropathologic changes in semantic dementia. Neurocase 16: , 15–22. |
[43] | Montgomery W , Ueda K , Jorgensen M , Stathis S , Cheng Y , Nakamura T ((2018) ) Epidemiology, associated burden, and current clinical practice for the diagnosis and management of Alzheimer’s disease in Japan. Clinicoecon Outcomes Res 10: , 13–28. |
[44] | Qaseem A , Snow V , Cross JT Jr. , Forciea MA , Hopkins R Jr. , Shekelle P , Adelman A , Mehr D , Schellhase K , Campos-Outcalt D , Santaguida P , Owens DK ((2008) ) Current pharmacologic treatment of dementia: A clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med 148: , 370–378. |
[45] | American Psychiatric Association, American Psychiatric Association practice guideline for the treatment of patients with Alzheimer’s disease and other dementias. Second edition, https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/alzheimers.pdf, Accessed March 3, 2022. |
[46] | California Workgroup on Guidelines for Alzheimer’s Disease Management, Guideline for Alzheimer’s disease management: final report, https://www.alzheimersla.org/wp-content/uploads/2016/01/Professionals-Guideline-FullReport-CA.pdf, Accessed March 3, 2022. |
[47] | Segal-Gidan F , Cherry D , Jones R , Williams B , Hewett L , Chodosh J ((2011) ) Alzheimer’s disease management guideline: Update 2008 , Alzheimers Dement 7: , e51–59. |
[48] | Ismail Z , Black SE , Camicioli R , Chertkow H , Herrmann N , Laforce R Jr , Montero-Odasso M , Rockwood K , Rosa-Neto P , Seitz D , Sivananthan S , Smith EE , Soucy JP , Vedel I , Gauthier S ((2020) ) Recommendations of the 5th Canadian Consensus Conference on the diagnosis and treatment of dementia. Alzheimers Dement 16: , 1182–1195. |
[49] | Hort J , O’Brien JT , Gainotti G , Pirttila T , Popescu BO , Rektorova I , Sorbi S , Scheltens P ((2010) ) EFNS guidelines for the diagnosis and management of Alzheimer’s disease. Eur J Neurol 17: , 1236–1248. |
[50] | O’Brien JT , Holmes C , Jones M , Jones R , Livingston G , McKeith I , Mittler P , Passmore P , Ritchie C , Robinson L , Sampson EL , Taylor JP , Thomas A , Burns A ((2017) ) Clinical practice with anti-dementia drugs: A revised (third) consensus statement from the British Association for Psychopharmacology. J Psychopharmacol 31: , 147–168. |
[51] | Deutsche Gesellschaft für Neurologie (DGN), Guidelines for diagnostics and therapy in neurology: Dementia - version 2, https://dgn.org/leitlinien/leitlinie-diagnose-und-therapie-von-demenzen-2016/Accessed March 3, 2022. |
[52] | Caltagirone C , Bianchetti A , Di Luca M , Mecocci P , Padovani A , Pirfo E , Scapicchio P , Senin U , Trabucchi M , Musicco M ((2005) ) Guidelines for the treatment of Alzheimer’s disease from the Italian Association of Psychogeriatrics. Drugs Aging 22: (Suppl 1), 1–26. |
[53] | National Institute for Health and Care Excellence (NICE), Dementia: Assessment, management and support for people living with dementia and their carers [NG97], https://www.nice.org.uk/guidance/ng97, Accessed March 3, 2022. |
[54] | Ministerio de Sanidade Política Social e Igualdad, Clinical practice guideline on the comprehensive care of people with Alzheimer’s disease and other dementias, https://portal.guiasalud.es/wp-content/uploads/2018/12/GPC_484_Alzheimer_AIAQS_comp_eng.pdf, Accessed March 3, 2022. |
[55] | Cummings J , Lee G , Zhong K , Fonseca J , Taghva K ((2021) ) Alzheimer’s disease drug development pipeline: 2021, Alzheimers Dement (N Y) 7: , e12179. |
[56] | Nguyen VT , Engleton M , Davison M , Ravaud P , Porcher R , Boutron I ((2021) ) Risk of bias in observational studies using routinely collected data of comparative effectiveness research: A meta-research study. BMC Med 19: , 279. |
[57] | Cook L, Souris H, Isaacs J, The 2019 national memory service audit, NHS london Clinical Networks, https://www.england.nhs.uk//wp-content/uploads/sites/8/2020/04/The-2019-national-memory-service-audit.pdf, Accessed March 8, 2022. |
[58] | Haute Autorité de Santé, Care pathway guide for patients with a disorder neurocognitive associated with Alzheimer’s disease or related disease, https://www.has-sante.fr/upload/docs/application/pdf/2018-05/pursarco_de_soins_alzheimer.pdf, Accessed March 3, 2022. |


