
Dysphagia Profiles Among Inpatients with Dementia Referred for Swallow Evaluation
Abstract
Background:
Alzheimer’s disease and related dementias (ADRD) patients who are hospitalized often develop oropharyngeal dysphagia, increasing risk for adverse outcomes, such as aspiration pneumonia. However, prevalence estimates of dysphagia are highly variable and often based on patient report or clinical testing rather than visualization of the swallow.
Objective:
The aims of this study were to determine prevalence and severity of dysphagia among inpatients with ADRD referred for swallowing evaluation.
Methods:
Electronic health record (EHR) abstraction of ADRD diagnosis and presence and severity of clinically-determined dysphagia on bedside swallow evaluation (BSE) and videofluoroscopic swallow study (VFSS).
Results:
16% (n = 268) had an ADRD diagnosis or were taking dementia-specific medication based on the EHR. 75% (n = 202) were diagnosed with dysphagia on the BSE. 60% subsequently underwent VFSS (n = 122) with dysphagia confirmation in 92% (n = 112). ADRD inpatients were significantly more likely to be diagnosed with dysphagia based on the BSE (p < 0.0001) than those without ADRD. Additionally, dysphagia on the VFSS was more severe in the ADRD group (p < 0.03).
Discussion:
ADRD individuals may be vulnerable to developing or worsening dysphagia during hospitalization. Results underscore the importance of evaluating swallowing function in hospitalized patients with ADRD in order to facilitate targeted intervention.
INTRODUCTION
Oropharyngeal dysphagia, or swallowing dysfunction, is a condition that affects more than 16 million individuals in the United States [1] and results in serious health consequences, including pneumonia, malnutrition, and death [2–4]. Alzheimer’s disease and related dementias (ADRD) commonly lead to oropharyngeal dysphagia. In fact, pneumonia, due to dysphagia-related aspiration [5], is the most commonly cited complication leading to death in older individuals with ADRD [6, 7]. Hospitalized patients with ADRD are particularly vulnerable to developing comorbid dysphagia as a result of their diagnosis. One study observed that patients with comorbid ADRD and dysphagia are at increased risk for malnutrition, aspiration pneumonia, mechanical ventilation, and increased length of hospital stay compared to those without dysphagia [8].
Despite the serious consequences of dysphagia, prevalence estimates for its occurrence in individuals with ADRD range widely across studies from 7 to 87% [9–19]. These differences are due to variations in the method of dysphagia measurement (e.g., patient-reported outcome measures (PROs), screening tools, bedside clinical evaluations, instrumental assessments), definition of dysphagia, dementia subtype (e.g., Alzheimer’s disease, vascular dementia), stage of dementia progression, and study setting (home, hospital, institution) [2]. Despite the serious consequences of dysphagia in hospitalized patients, these variations in prevalence estimates limit understanding of dysphagia and development of optimal treatment for patients with ADRD compared to other populations.
Additionally, the majority of prevalence studies in this population have relied on PROs or bedside evaluation procedures to determine presence of dysphagia [15, 17, 19]. These approaches have lower diagnostic accuracy for identifying dysphagia [20] as compared to instrumental assessments (videofluoroscopic swallow study (VFSS) and fiberoptic endoscopic evaluation of swallowing (FEES)) that allow for direct visualization of the swallow [12].
Unfortunately, depending upon the clinical practice setting, instrumental assessments are not always available. When they are available, clinicians may not recommend them for patients with ADRD as frequently due to the perception that they will not be well-tolerated [4, 12, 21–23].
Therefore, the aim of this study was two-fold: 1) to identify the presence and severity of dysphagia in a cohort of inpatients with ADRD referred for dysphagia evaluation and 2) to characterize practice patterns specific to dysphagia evaluation in ADRD inpatients. We hypothesized that dysphagia would be more prevalent in patients with ADRD compared to those without ADRD and that instrumental assessments following a BSE would be recommended less frequently for inpatients with ADRD.
METHODS
This retrospective cohort study consists of all inpatients who were referred to the University of Wisconsin Hospital and Clinic’s Swallow Service in the calendar year 2014. The inpatient list for those who received a clinical swallowing evaluation was procured through billing data for CPT code 92610. Patients under the age of 50 were excluded and patients above the age of 89 were designated as 89 to protect privacy in accordance with the IRB protocol. In-depth abstractions of patient medical records were conducted by abstractors who were trained using a standardized protocol. Abstracted information included basic demographics (age, sex, race), presence of ADRD, and dysphagia severity ratings from the bedside and instrumental swallowing evaluations. If a patient received more than one evaluation during the index hospitalization, severity ratings from the first evaluation were used. Additionally, in those with ADRD, the primary diagnosis from the hospital discharge summary was recorded.
It has been shown that the majority of patients diagnosed with ADRD by their primary care providers are correctly diagnosed and that the use of electronic medical records can be a reliable way to identify patients with ADRD [24, 25]. In this study, the diagnosis of ADRD was determined by either of the following criteria: a) patient has a documented ADRD diagnosis by a healthcare provider or any mention of a previous ADRD diagnosis by a healthcare worker prior to the swallow evaluation, or b) patient was taking any medication commonly prescribed for ADRD (donepezil, memantine, rivastigmine, or galantamine) before the swallow evaluation. This involved reviewing the problem list and past medical history at time of admission, hospital admission history and physical, and hospital admission pharmacist medicine list, as well as using the electronic medical record (Epic HealthLink) search feature [26].
Dysphagia severity ratings were abstracted independently from the Speech-Language Pathologist’s (SLP) bedside swallow evaluation (BSE) and VFSS reports. The BSE is a commonly used clinical assessment, performed at the patient’s bedside, that includes a cranial nerve examination as well as administration of liquids and foods in various sizes and consistencies. If dysphagia is suspected, the SLP will typically recommend an instrumental swallowing examination (VFSS or FEES) to allow for visualization of the swallow. The VFSS is a dynamic radiographic imaging procedure which allows for real-time assessment of the presence and severity of aspiration as well as biomechanical aspects of the oropharyngeal swallow through administration of barium. It is a valid and reliable tool, used as the reference standard for dysphagia diagnosis [27].
In routine clinical practice at the study hospital, dysphagia severity ratings based on the BSE and VFSS are based on the American Speech-Language-Hearing Association (ASHA) Functional Communication Measures (FCM) and characterized as no dysphagia, mild, mild-moderate, moderate, moderate-severe, or severe oropharyngeal dysphagia [28]. If the evaluation note did not include either a dysphagia diagnosis or severity rating, a clinical SLP on the study team reviewed the note and assigned one of two ratings: “not mentioned” to cases in which it was unclear if the patient had dysphagia, or “dysphagia without mention of severity” when the note clearly indicated dysphagia but a severity rating was not assigned by the treating clinician.
Statistical analysis
Baseline demographics were summarized using descriptive statistics. Differences between the ADRD and non-ADRD groups were analyzed using chi-square tests for categorical variables and t-tests for continuous variables. We conducted a sensitivity analysis with receiver operating characteristics (ROC) using the ROCTAB package in STATA. The positive predictive value (PPV) was calculated using column and row percentages of true and false positives. Specificity and negative predictive value were not calculated because patients who tested negative on the BSE did not undergo a VFSS. Accuracy of the BSE for diagnosis of dysphagia (present or absent) when compared to the VFSS was also calculated. Accuracy was defined as the number of accurate dysphagia diagnoses over the total number of dysphagia diagnoses from the BSE. All statistical analyses were conducted using STATA version SE and a p-value of 0.05 was considered statistically significant.
RESULTS
Demographics
This retrospective cohort study included all inpatients ≥50 years of age who received a BSE swallowing evaluation over one full calendar year at a large university hospital (n = 1,691). A total of 268 (16%) of these patients were found to have a diagnosis of ADRD. Of these patients identified as having a diagnosis of ADRD, 147 (54.9%) were identified solely based on the presence of a clinically documented ADRD diagnosis and 121 (45.1%) patients were identified as having a diagnosis of ADRD and taking ADRD medication. Those with ADRD were older (M = 78 years, SD = 8.2 years) than those without (M = 68 years, SD = 10.2 years).
Table 1
Characteristics of patients evaluated for dysphagia
| Overall (N = 1,691) | No ADRD (N = 1,423) | ADRD (N = 268) | |
| Age, n (%) | |||
| 50–59 y | 330 (19.5) | 324 (22.8) | 6 (2.2) |
| 60–69 y | 486 (28.7) | 455 (32) | 31 (11.6) |
| 70–79 y | 426 (25.2) | 352 (24.7) | 74 (27.6) |
| 80–88 y | 324 (19.2) | 225 (15.8) | 99 (36.9) |
| 89+ y | 125 (7.4) | 67 (4.7) | 58 (21.6) |
| Sex, n (%) | |||
| Female | 767 (45.4) | 633 (44.5) | 134 (50) |
| Male | 924 (54.6) | 790 (55.5) | 134 (50) |
| Race, n (%) | |||
| Black | 67 (4) | 56 (3.9) | 11 (4.1) |
| White | 1566 (92.6) | 1317 (92.6) | 249 (92.9) |
| Other | 58 (3.4) | 50 (3.5) | 8 (3) |
In patients with ADRD, the diagnosis from the hospital discharge summary was recorded and categorized. Stroke or intracerebral hemorrhage was the most common diagnosis at discharge (16.8%), followed by altered mental status or delirium (14.2%).
Table 2
Diagnosis at hospital discharge in patients with ADRD
| Category | N (268) | % |
| Stroke/Hemorrhage | 45 | 16.8 |
| Altered Mental Status/Delirium/Dementia | 38 | 14.2 |
| Aspiration/Dysphagia/Pneumonia | 33 | 12.3 |
| Falls/Fractures | 33 | 12.3 |
| Cardiac Conditions | 21 | 7.8 |
| Other | 19 | 7.1 |
| Gastrointestinal/Gall Bladder | 17 | 6.3 |
| Sepsis | 13 | 4.8 |
| Respiratory Conditions | 12 | 4.4 |
| Trauma | 9 | 3.5 |
| Seizure | 8 | 2.9 |
| Wound/Cellulitis/Ulcer | 5 | 1.8 |
| Urinary Tract Infection | 5 | 1.8 |
| Kidney Disease | 4 | 1.5 |
| Cancer | 4 | 1.5 |
| Spinal Injuries | 2 | <1 |
Evaluation type
Slightly over half of inpatients who received a BSE also underwent an instrumental evaluation (60%). There was no significant difference in the frequency of instrumental evaluations following the BSE between the ADRD and non-ADRD cohorts (p < 0.416).
Table 3
Type of dysphagia evaluation completed during hospital admission
| Overall (N = 1,691) | No ADRD (N = 1,423) | ADRD (N = 268) | p | |
| BSE Only (%) | 928 (54.88) | 787 (55.31) | 141 (52.61) | 0.416 |
| FEES Only (%) | 95 (5.62) | 90 (6.32) | 5 (1.87) | |
| VFSS Only (%) | 589 (34.83) | 472 (33.17) | 117 (43.65) | |
| VFSS + FEES (%) | 79 (4.67) | 74 (5.20) | 5 (1.87) |
Dysphagia diagnosis and characterization
Licensed SLPs completed consultations as part of routine care that included a BSE with each patient, documented their findings from the assessment, and determined if further evaluation with a VFSS or FEES was warranted. The BSE documentation indicated one of the following: functional oropharyngeal swallowing abilities or an absence of dysphagia (no dysphagia; n = 565), dysphagia with a severity characterization (mild, mild-moderate, moderate, moderate-severe, severe; n = 650), dysphagia without a severity rating (n = 414), or no information related to dysphagia status (not mentioned; n = 62).
Reasons for the “not mentioned” designation were the following: 1) information from the bedside and instrumental examinations were combined into one evaluation note with no BSE specific results delineated; 2) the BSE exam was limited due to high risk for silent aspiration (e.g., tracheostomy present), altered mental status or reduced alertness, or a history of known severe dysphagia; or 3) the patient demonstrated baseline coughing or throat clearing (prior to administration of liquid/food) that warranted further evaluation but the clinician did not indicate a diagnosis of dysphagia.
For 24.5% of patients, a dysphagia severity rating was not given (“dysphagia without severity”). This occurred when either 1) there was not enough information from the BSE to assign a dysphagia severity level, typically in cases in which the patient was not able to participate in a full evaluation due to altered mental status or current medical condition or 2) the clinician performed an instrumental evaluation following the bedside examination and assigned one severity rating based on the instrumental. Of note, the practice pattern utilized by clinicians at this facility is to designate a severity level after a valid assessment is performed, which is either after a complete, comprehensive bedside evaluation or an instrumental assessment.
Based on the BSE, 60.6% (862) of patients without ADRD had oropharyngeal dysphagia, while 75.4% (202) of patients with ADRD were diagnosed with dysphagia. Descriptive statistics, utilizing the chi-squared test, showed a significant difference (p < 0.0001) for individuals with ADRD compared to those without ADRD. The proportion of dysphagia occurred at a higher rate in ADRD patients, suggesting dysphagia varies by dementia status. Overall, 667 patients in the cohort (39.4%) had a VFSS. Of those, 122 (18.3%) were patients with ADRD. In contrast to the BSE results, there was no statistically significant difference in frequency of dysphagia diagnosis based on the VFSS between the ADRD and non-ADRD cohorts (p = 0.360).
Table 4
Dysphagia severity ratings from BSE in patients with and without ADRD
| Bedside Swallow Evaluation | Overall (N = 1,691) | No ADRD (N = 1,423) | ADRD (N = 268) | p |
| Dysphagia Severity | ||||
| Mild | 266 (15.7) | 213 (15) | 53 (19.8) | 0.25 |
| Mild-Moderate | 122 (7.2) | 87 (6.1) | 35 (13.1) | |
| Moderate | 85 (5) | 67 (4.7) | 18 (6.7) | |
| Moderate-Severe | 36 (2) | 28 (2) | 8 (3) | |
| Severe | 141 (8.3) | 116 (8.2) | 25 (9.3) | |
| Dysphagia without Severity | 414 (24.5) | 351 (24.7) | 63 (23.5) | 0.09 |
| Total Dysphagia Diagnoses | 1,064 | 862 (60.6) | 202 (75.4) | <0.00 |
Table 5
VFSS dysphagia severity ratings in patients with and without ADRD
| Videofluoroscopic Swallow Study | Overall (N = 667) | No ADRD (N = 545) | ADRD (N = 122) | p |
| Dysphagia Severity | ||||
| Mild | 227 (34) | 197 (36.2) | 30 (24.6) | <0.03 |
| Mild-Moderate | 190 (28.5) | 143 (26.2) | 47 (38.5) | |
| Moderate | 93 (13.9) | 71 (13) | 22 (18) | |
| Moderate-Severe | 39 (5.8) | 33 (6.1) | 6 (4.9) | |
| Severe | 46 (6.9) | 39 (7.2) | 7 (5.7) | |
| Dysphagia without Severity | 2 (0.3) | 2 (0.4) | 0 (0) | 0.49 |
| Total Dysphagia Diagnoses | 597 (89.5) | 485 (89.9) | 112 (91.8) | 0.36 |
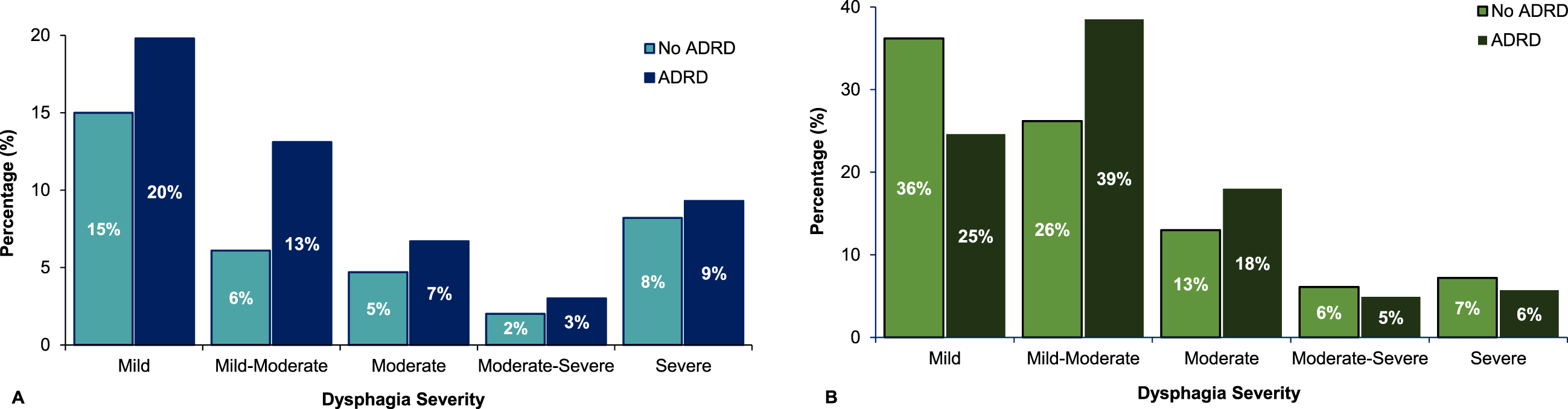
When dysphagia was identified during a BSE and a severity rating was assigned, mild dysphagia was diagnosed more often than more severe forms of dysphagia in both the non-ADRD cohort (15%) and the ADRD cohort (19.8%). In both groups, moderate-severe dysphagia was the severity of dysphagia diagnosed the least often (2% and 3%, respectively) on the BSE. Severe dysphagia was only diagnosed in 9% of those patients with ADRD and 8% of those without ADRD, upon bedside examination. For VFSS studies that resulted in a dysphagia diagnosis, the most common dysphagia severity was mild-moderate dysphagia (38.5%) in those with ADRD and mild dysphagia (36%) in those without ADRD, consistent with the BSE results. Diagnosis of severe dysphagia following the VFSS also mirrored that of the BSE, with 6% of patients with ADRD and 7% of patients without ADRD demonstrating this degree of impairment. For both the BSE and the VFSS, more severe ratings of dysphagia occurred in the ADRD group compared to the non-ADRD group, with this difference reaching significance based on the VFSS results only (p < 0.03) (see Fig. 1).
Fig. 1
Dysphagia Severity Ratings for the BSE and VFSS.
Accuracy of the BSE
A total of 668 inpatients underwent both BSE and VFSS. Patients were excluded from this analysis if their dysphagia diagnosis was not mentioned in the bedside note (n = 40), resulting in 628 patients.
In the full cohort of 628 patients, accuracy was 91%. There were 120 patients with an ADRD diagnosis; for this sub-group, BSE accuracy was 92%. In the 508 individuals who did not have an ADRD diagnosis, BSE accuracy was 90%. Sensitivity, specificity, PPV, and negative predictive value (NPV) could not be determined as not everyone with a BSE underwent instrumental evaluation. Individuals who tested negative on the BSE were often referred for a VFSS by their SLP to assess further due to clinical concerns undetermined by screening.
In the 120 patients with ADRD who received both a BSE and VFSS, dysphagia severity ratings were compared across the two evaluations. In 21 cases (17.2%), there was exact agreement in the dysphagia severity level, with the highest agreement seen in those with mild-moderate dysphagia. In 23 cases (19%), dysphagia was deemed to be more impaired following the VFSS than noted at the BSE; similarly, 25 patients (21%) were found to have less severe dysphagia at the VFSS, in comparison to their BSE. Of note, in 51 cases (42.5%) the SLP diagnosed dysphagia at the BSE but did not assign a severity rating to the impairment until the VFSS.
DISCUSSION
This study represents the largest structured review ever performed of dysphagia prevalence and severity in hospitalized patients with ADRD. In this cohort referred for swallow evaluation, approximately 16% were identified as having ADRD. Patients with ADRD had a higher likelihood of dysphagia, and, when diagnosed with dysphagia, experienced more severe cases than those without ADRD.
The prevalence of dysphagia diagnosed by clinical examination in those with ADRD was roughly 30% higher in this study than in prior studies [19, 29–31], likely because the population was comprised of hospitalized patients referred for a swallowing evaluation. 75% of inpatients with ADRD referred for swallowing evaluation were diagnosed with a swallowing disorder based on a clinical examination, which was significantly higher than those without ADRD. These differences may be due to issues unique to the ADRD population that affect evaluation of eating and swallowing (e.g., cognitive and behavioral changes).
Although more patients in the ADRD cohort were diagnosed with dysphagia during a BSE, they received instrumental evaluations at the same rate as those without ADRD. This finding suggests that clinicians are making recommendations for dysphagia management based on the BSE alone more often for patients with ADRD. This could be due to differences in goals of care for patients with ADRD in that patients and/or caregivers of those with ADRD may opt to forego additional testing. Additionally, it could be that patients with ADRD decline participation in an instrumental assessment that involves barium or insertion of a nasoendoscope at higher rates or that SLP clinicians perceive more potential barriers to completing an instrumental assessment with this population due to cognitive and/or behavioral issues. Another possibility is that more patients with ADRD demonstrated concern for oral phase dysphagia which can be assessed based on the bedside evaluation alone compared to pharyngeal phase dysphagia which requires visualization of the swallow to accurately assess.
Dysphagia was evident in the majority of those in the non-ADRD cohort who received a VFSS (90%). This high rate of dysphagia in those receiving a VFSS or FEES was not surprising given that the instrumental assessment was recommended by the SLP based on concerns for dysphagia on the BSE. High accuracy or PPV between the BSE and instrumental evaluations has been previously reported in the literature. A systematic review examined twelve studies for BSE diagnostic accuracy compared to instrumental evaluation in post-stroke survivors [30]. Four studies included PPV in dysphagic patients [30]. The PPV across these studies ranged between 71% –79% for BSE accuracy compared to a VFSS or MASA [30].
Of note, almost 40% of inpatients were not assigned a severity rating from the BSE, whereas all were given a severity rating following the VFSS. This highlights best practice in use of an instrumental exam to accurately characterize dysphagia. The BSE appears to provide adequate information regarding the suspected presence or absence of dysphagia, but the instrumental exam is needed for in-depth understanding of swallowing biomechanics that leads to the designation of severity.
For those patients with dysphagia severity ratings, mild to moderate dysphagia was more common than severe dysphagia. However, the higher proportion of more severe ratings in the ADRD group compared to the non-ADRD cohort indicates that, when it occurs, dysphagia may be more severe for the ADRD population. Published studies characterizing dysphagia in patients with ADRD are cross-sectional with small sample sizes. Future studies with longitudinal follow-up of dysphagia and in-depth characterization of dementia are needed.
Limitations and future directions
As this was a retrospective cohort study focused on inpatients specifically referred for swallow evaluation, the prevalence of ADRD among referred patients for swallowing consultation is most likely disproportionally higher than a cohort of all patients admitted to the hospital (regardless of swallow evaluation referral). Reliability of clinically determined dysphagia severity ratings among various providers is also unknown which could influence results. Additionally, we were unable to calculate the specificity of the BSE in those that were identified as having functional oropharyngeal swallowing abilities and did not receive an instrumental evaluation. Finally, differences in the biomechanical aspects of the swallow as well as safety and efficiency profiles based on ADRD stage, subtype, and A/T/N classification were not detailed and will be the focus of future work. Future research will also investigate dysphagia prevalence in those without ADRD based on age and hospital admission diagnosis as well as associations amongst comorbid conditions and dysphagia in those both with and without ADRD.
Conclusions
Hospitalized patients with ADRD are more likely to be diagnosed with dysphagia than those without ADRD and, when diagnosed, experience more severe cases. A VFSS following the BSE confirms the presence of dysphagia in patients both with and without ADRD, providing evidence that the presence of dysphagia can be adequately recognized through clinical evaluation. However, instrumentation is necessary for further characterization of the swallow.
ACKNOWLEDGMENTS
This work was supported by National Institutes of Health (NIH) Grant 1K76AG068590 (awarded to N.R.P.). The article was partially prepared at the William S. Middleton Veteran Affairs Hospital in Madison, WI; GRECC manuscript 007-2022. The views and content expressed in this article are solely the responsibility of the authors and do not necessarily reflect the position, policy, or official views of the Department of Veteran Affairs, the U.S. government, or the NIH.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0402r1).
REFERENCES
[1] | Bhattacharyya N ((2014) ) The prevalence of dysphagia among adults in the United States. Otolaryngol Head Neck Surg 151: , 765–769. |
[2] | Takizawa C , Gemmell E , Kenworthy J , Speyer R ((2016) ) A systematic review of the prevalence of oropharyngeal dysphagia in stroke, Parkinson’s disease, Alzheimer’s disease, head injury, and pneumonia. Dysphagia 31: , 434–441. |
[3] | Kuroda Y ((2016) ) Factors associated with the level of oral intake in hospitalized older adults with dysphagia: The importance of mental activity. Clin Nutr ESPEN 13: , 52–54. |
[4] | Payne M , Morley JE ((2018) ) Editorial: Dysphagia, ADRD and frailty. J Nutr Health Aging 22: , 562–565. |
[5] | Manabe T , Mizukami K , Akatsu H , Hashizume Y , Ohkubo T , Kudo K , Hizawa N ((2017) ) Factors associated with pneumonia-caused death in older adults with autopsy-confirmed ADRD. Intern Med 56: , 907–914. |
[6] | Burns A , Jacoby R , Luthert P , Levy R ((1990) ) Cause of death in Alzheimer’s disease. Age Ageing 19: , 341–344. |
[7] | Brunnstrom HR , Englund EM ((2009) ) Cause of death in patients with ADRD disorders.. Eur J Neurol 16: , 488–492. |
[8] | Paranji S , Paranji N , Wright S , Chandra S ((2017) ) A nationwide study of the impact of dysphagia on hospital outcomes among patients with ADRD. Am J Alzheimers Dis Other Demen 32: , 5–11. |
[9] | Horner J , Alberts MJ , Dawson DV , Cook GM ((1994) ) Swallowing in Alzheimer’s disease. Alzheimer Dis Assoc Disord 8: , 177–189. |
[10] | Rosler A , Pfeil S , Lessmann H , Hoder J , Befahr A , von Renteln-Kruse W ((2015) ) Dysphagia in ADRD: Influence of ADRD severity and food texture on the prevalence of aspiration and latency to swallow in hospitalized geriatric patients. J Am Med Dir Assoc 16: , 697–701. |
[11] | Miarons M , Clave P , Wijngaard R , Ortega O , Arreola V , Nascimento W , Rofes L ((2018) ) Pathophysiology of oropharyngeal dysphagia assessed by videofluoroscopy in patients with ADRD taking antipsychotics.. J Am Med Dir Assoc 19: , 812.e1–812.e. |
[12] | Michel A , Verin E , Gbaguidi X , Druesne L , Roca F , Chassagne P ((2018) ) Oropharyngeal dysphagia in community-dwelling older patients with ADRD: Prevalence and relationship with geriatric parameters. J Am Med Dir Assoc 19: , 770–774. |
[13] | Goes VF , Mello-Carpes PB , de Oliveira LO , Hack J , Magro M , Bonini JS ((2014) ) Evaluation of dysphagia risk, nutritional status and caloric intake in elderly patients with Alzheimer’s. Rev Lat Am Enfermagem 22: , 317–324. |
[14] | Londos E , Hanxsson O , Alm Hirsch I , Janneskog A , Bulow M , PalmkvistS ((2013) ) Dysphagia in Lewy body ADRD - a clinical observationalstudy of swallowing function by videofluoroscopic examination. BMC Neurol 13: , 140. |
[15] | Priefer BA , Robbins J ((1997) ) Eating changes in mild-stage Alzheimer’s disease: A pilot study. Dysphagia 12: , 212–221. |
[16] | Suh MK , Kim H , Na DL ((2009) ) Dysphagia in patients with ADRD: Alzheimer versus vascular. Alzheimer Dis Assoc Disord 23: , 178–184. |
[17] | Ikeda M , Brown J , Holland AJ , Fukuhara R , Hodges JR ((2002) ) Changes in appetite, food preference, and eating habits in frontotemporal ADRD and Alzheimer’s disease. J Neurol Neurosurg Psychiatry 73: , 371–376. |
[18] | Langmore SE , Olney RK , Lomen-Hoerth C , Miller BL ((2007) ) Dysphagia in patients with frontotemporal lobar ADRD. Arch Neurol 64: , 58–62. |
[19] | Alagiakrishnan K , Bhanji RA , Kurian M ((2013) ) Evaluation and management of oropharyngeal dysphagia in different types of ADRD: A systematic review. Arch Gerontol Geriatr 56: , 1–9. |
[20] | O’Horo JC , Rogus-Pulia N , Garcia-Arguello L , Robbins J , Safdar N ((2015) ) Bedside diagnosis of dysphagia: A systematic review. J Hosp Med 10: , 256–65. |
[21] | Correia SdM , Morillo LS , Filho WJ , Mansur LL ((2010) ) Swallowing in moderate and severe phases of Alzheimer’s disease. Arq Neuropsiquiatr 68: , 855–861. |
[22] | Egan A , Andrews C , Lowit A ((2020) ) Dysphagia and mealtime difficulties in dementia: Speech and language therapists’ practices and perspectives. Int J Lang Commun Disord 55: , 777–792. |
[23] | Desai RV , Namasivayam-MacDonald A ((2020) ) Practice patterns of speech-language pathologists managing dysphagia in dementia: A cross-sectional survey in the United States. Perspect ASHA Spec Interest Groups 5: , 1631–1646. |
[24] | Bradford A , Kunik ME , Schulz P , Williams SP , Singh H ((2009) ) Missed and delayed diagnosis of ADRD in primary care: Prevalence and contributing factors. Alzheimer Dis Assoc Disord 23: , 306–314. |
[25] | Wilkinson T , Ly A , Schnier C , Schnier C , Rannikmae K , Bush K , Brayne C , Quinn TJ , Sudlow CLM , UK Biobank Neurodegenerative Outcomes Group and Dementias Platform UK ((2018) ) Identifying ADRD cases with routinely collected health data: A systematic review. Alzheimers Dement 14: , 1038–1051. |
[26] | Epic HealthLink (2022) Epic Systems Corporation, Verona, Wisconsin. |
[27] | Lof GL , Robbins J ((1990) ) Test-retest variability in normal swallowing. Dysphagia 4: , 236–242. |
[28] | American Speech-Language-Hearing Association (1998) National Outcomes Measurement System (NOMS). Rockville, MD. |
[29] | Sura L , Madhavan A , Carnaby G , Crary M ((2012) ) Dysphagia in the elderly: Management and nutritional considerations. Clin Interv Aging 7: , 287–298. |
[30] | Virvidaki IE , Nasios G , Kosmidou M , Giannopoulos S , Milionis H ((2018) ) Swallowing and aspiration risk: A critical review of non instrumental bedside screening tests. J Clin Neurol 14: , 265–274. |
[31] | Espinosa-Val MC , Martín-Martínez A , Graupera M , Arias O , Elvira A , Cabré M , Palomera E , Bolívar-Prados M , Clavé P , Ortega O ((2020) ) Prevalence, risk factors, and complications oforopharyngeal dysphagia in older patients with ADRD. Nutrients 12: , 863. |


