
Exercise Training for Mild Cognitive Impairment Adults Older Than 60: A Systematic Review and Meta-Analysis
Abstract
Background:
The prevalence of mild cognitive impairment (MCI) continues to increase due to population aging. Exercise has been a supporting health strategy that may elicit beneficial effects on cognitive function and prevent dementia.
Objective:
This study aimed to examine the effects of aerobic, resistance, and multimodal exercise training on cognition in adults aged > 60 years with MCI.
Methods:
We searched the Cochrane Library, PubMed, and Embase databases and ClinicalTrials.gov (https://clinicaltrials.gov) up to November 2021, with no language restrictions. We included all published randomized controlled trials (RCTs) comparing the effect of exercise programs on cognitive function with any other active intervention or no intervention in participants with MCI aged > 60 years.
Results:
Twelve RCTs were included in this review. Meta-analysis results revealed significant improvements in resistance training on measures of executive function (p < 0.05) and attention (p < 0.05); no significant differences were observed between aerobic exercise and controls on any of the cognitive comparisons.
Conclusion:
Exercise training had a small beneficial effect on executive function and attention in older adults with MCI. Larger studies are required to examine the effects of exercise and the possible moderators.
INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative disorder that is the most common cause of dementia [1]. In the initial stage of AD, the decline in cognitive function can be significantly subtle and is currently being clinically identified as degenerative mild cognitive impairment (MCI) [2]. There are three clinical subtypes of MCI: amnestic MCI, MCI involving various degrees of impairment in multiple cognitive domains, and MCI involving a single non-memory domain. Patients with MCI normally have self- or informant-reported cognitive complaints [3] and documented objective impairment in one or more cognitive domains that is greater than would be expected for the patient’s age or educational background [4], but still preserved the activities of daily living without significant impairment in social or occupational functions [5]. The prevalence of MCI increases with age (6.7% for ages 60–64 years, 65.2% in older adults aged > 60 years), and patients with MCI are at a higher risk of progressing to dementia than age-matched controls (progression to dementia at a rate of approximately 14.9% in MCI aged > 65 years followed by 2 years) [6]. To date, there is no pharmacologic management currently approved for MCI, and behavioral training, such as cognitive therapy and exercise training, has symptomatic cognitive benefits in MCI [7–9].
Considering the feasibility and acceptability of intervention training, exercise seems to be an available and economical therapeutic intervention for individuals at an earlier point of cognitive decline. Evidence indicates that exercise elicits cognition- and neurovascular oxygenation-promoting effects in rodents by reducing amyloid pathology [10–12]; enhancing hippocampal neurogenesis [13], oxidative stress [14–16], and intracranial energy metabolism [17]; and reducing neuroinflammation [18]. However, findings are mixed in human studies. Evidence suggests that exercise reduces vascular risk factors, such as hypertension [19], dyslipidemia [20], type 2 diabetes [21], obesity [22], subclinical atherosclerosis [23], and arrhythmias [24], which are associated with a greater risk of cognitive impairment and dementia [25]. Moreover, exercise may reduces the risk of stroke [26]. Recent meta-analyses showed that physical exercise may help preserve or even improve cognitive function [27–29] and peripheral brain-derived neurotrophic factor concentrations [30, 31] in healthy older adults. Exercise increases precentral cortical thickness and reduces neuroplasticity [32]; augments gray and white matter volumes [33], hippocampal volume [34–36], and systemic levels of glycosylphosphatidylinositol-specific phospholipase; and ameliorates age-related regenerative impairments [37].
Previous studies have reported a valid effect of exercise training on cognitive function in older adults with and without cognitive impairment [38–40] with a general effect of exercise training [41–43]. For instance, all levels of physical activity were reported to have a significant and consistent protective effects against the occurrence of cognitive decline [44]. Nevertheless, studies on the effects of physical exercise in older adults with MCI are insufficient and vary in efficacy owing to the large variability in exercise protocols, compliance, and complicated interpretation of the results [43]. This review involved patients with MCI aged > 60 years, when the global prevalence rates of dementia are exacerbated continuously. We compared the results with previous reviews by examining the effects of aerobic, resistance, mind–body, and multimodal exercise training on cognitive performance in patients with MCI. These results may be helpful in clarifying the efficacy of exercise interventions on cognitive function in older adults with MCI.
MATERIALS AND METHODS
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis. The study protocol was registered with the International Prospective Register of Systematic Reviews (CRD42021259555).
Search strategy
A librarian-led systematic search of Embase, PubMed, and Cochrane databases was performed using a strategy combining selected Medical Subject Headings terms (exercise, exercise therapy, resistance training, sports, physical fitness, circuit-based exercise, endurance training, Tai Ji, bicycling, yoga, walking, jogging, running, swimming, muscle stretching exercises, plyometric exercise, cognitive dysfunction, aged) and free-text terms (For full search strategy, see the Supplementary Material). No language or other limitations were imposed during the search process. Additionally, we searched ClinicalTrial.gov, reference lists of selected articles, and related review articles to screen for related clinical trials being conducted. The search terms regarding random control study design (randomized controlled trial [Publication Type] OR randomized [Title/Abstract] OR placebo [Title/Abstract]) were obtained from McMaster University Health Information’s website. The last search was performed on November 5, 2021.
Criteria for considering studies for this review
Types of studies
Human subject studies designed as randomized controlled trial (RCT) published in English were included without year restriction. Nonrandomized controlled studies, conference abstracts, reviews, protocols, and secondary analyses were excluded.
Types of participants
Participants diagnosed with MCI according to accepted criteria (Petersen, Winblad, Morris, Albert criteria) and aged > 60 years were included. We excluded healthy aging elderly adults, patients with any form of dementia, or those diagnosed with cognitive impairment due to definite etiologies, such as trauma or vascular or psychiatric diseases. Any clinical subtype of MCI was considered eligible. MCI defined by a single scale was considered insufficiently credible and unreliable.
Types of interventions
We included supervised structured exercises of any frequency, intensity, duration, or time directed at improving physical fitness. Combined exercise interventions with two or more types were included as multimodal training; however, studies involving exercise programs that combined cognitive training or other non-exercise activities (e.g., diets, drugs, and video games), not fully supervised or lasted < 4 weeks, were excluded.
Types of control groups
We included studies that involved comparators who engaged in a strength or balance tone, a program of social or mental activities, no treatment, or on the waiting list.
Types of outcomes
The primary outcome was cognitive function that was evaluated using a measurable cognitive screening instrument, whereas the secondary outcome was the dropout rate. Studies with no outcomes in specific domains of cognitive fields or studies that only involved the Mini-Mental State Examination (MMSE) or Montreal Cognitive Assessment (MoCA) were excluded. Two authors (WS and KH) initially excluded articles that did not meet the inclusion criteria, based on their titles and abstracts. After deduplication, the remaining articles were independently screened for eligibility by full-text assessment based on the defined inclusion criteria. Disagreements were resolved through discussions with expert HZ (study selection procedure, Fig. 1).
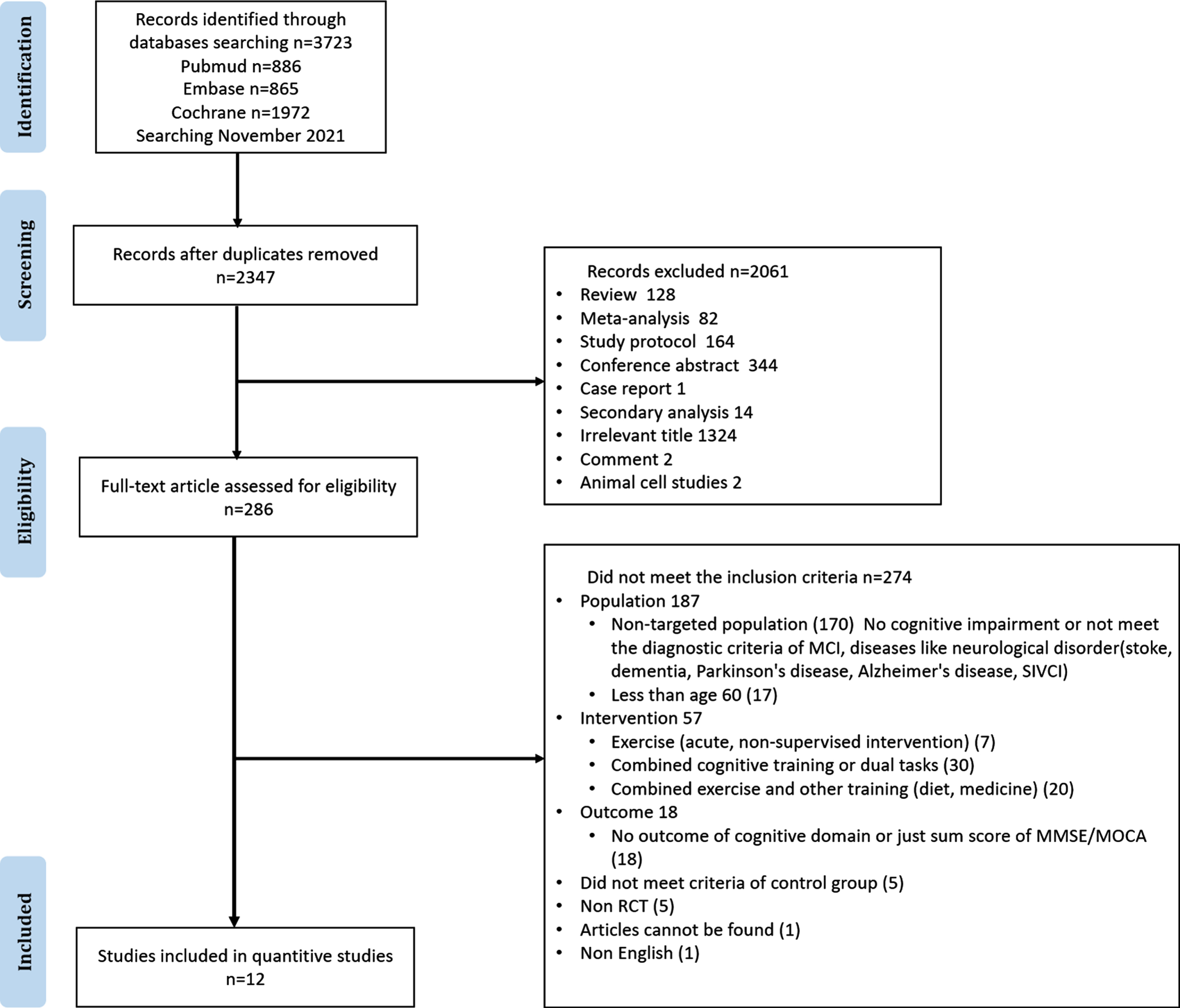
Fig. 1
PRISMA flow diagram of the literature selection process.
Quality assessment and data extraction
We extracted types of data from the full-text articles, including study characteristics of author; published year; country; RCT design, including grouping, sample size, sex ratio, mean age, MMSE score before the intervention, and diagnostic criteria; characteristics of the exercise intervention group, including type, intensity, frequency, duration, and time; and outcome neuropsychological tool used for measuring cognitive function. If the full text or data were incomplete, the author was contacted via email. The protocol of each included study was examined to verify reporting bias. The quality of individual study was assessed using the Cochrane Risk of Bias Tool (Fig. 2) [45]. Risk was assessed to be “low,” “high,” or “unclear.” Two independent authors (HL and HD) assessed the risk of bias. Disagreements were resolved by discussion with a third author.
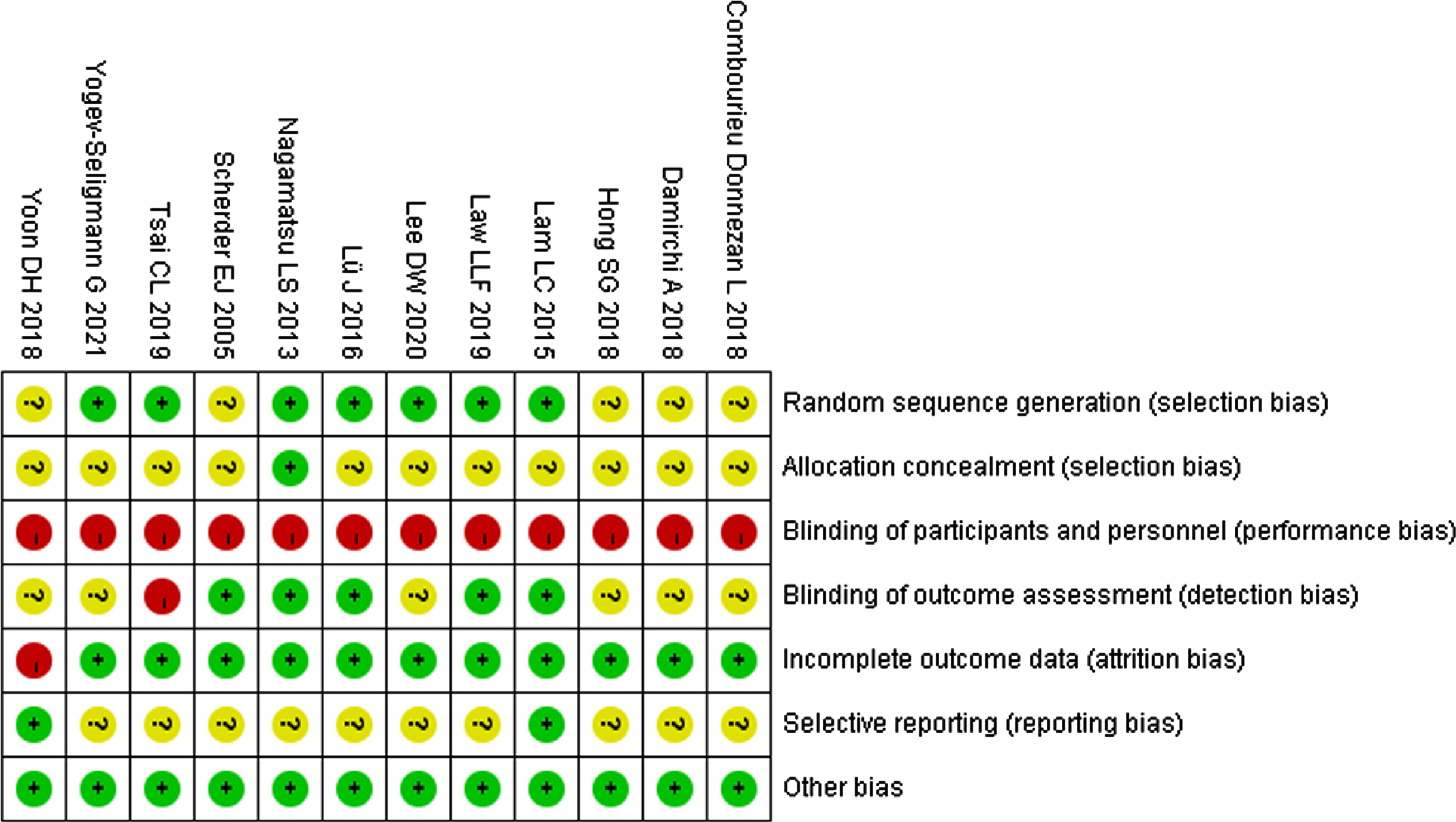
Fig. 2
Cochrane’s Quality Assessment: summary of risk of bias for each quality item for each included study.
Data synthesis and statistical analyses
Review Manager (RevMan) version 5.3 was used for all analyses. The summary statistics required for each assessment for continuous data were the post-intervention mean scores, standard deviation, and number of participants in each group (several studies did not provide change scores). The mean was entered as negative when a higher score indicated worse performance (e.g., reaction time, trail making test). Cognitive function is normally assessed using both global and individual cognitive tests. There are general cognitive tests (MMSE, MoCA) and specific tests that cover cognitive domains, including memory, attention, visuospatial processing, language, executive function, and social comportment. We classified the cognitive outcomes assessed using various neuropsychological tests into seven domains: (1) immediate memory, (2) working memory, (3) delayed memory, (4) processing speed, (5) attention, (6) executive function, and (7) recognition [27]. For each domain, we included only one test from a single trial that was used more frequently or closer to the domain. For dichotomous data, we extracted the number of participants in each group for each trial. Statistical analyses were performed if more than one study could be grouped into cognitive domains according to intervention (e.g., aerobic or resistance exercise). When only one study involved a category, the statistics from that single study were reported, but not analyzed. For continuous variables measured on different scales, standardized mean differences (SMDs) and 95% confidence interval (CI) were calculated; for dichotomous variables, risk ratios and 95% CIs were calculated.
The I2 statistic was calculated to describe the proportion of true heterogeneity in the observed variance across studies. Cochrane’s handbook recommends heterogeneity as not important (0–40%), moderate heterogeneity (30–60%), substantial heterogeneity (50–90%), and considerable heterogeneity (75–100%). Sensitivity analysis was performed when I2 was > 50% [46]. For which data were available, meta-analyses were performed using the inverse-variance method. A random-effects model was used to assess the cognitive outcomes and dropout rates. Given the small number of included studies, we did not perform a funnel plot visual test to investigate publication bias [9, 47].
RESULTS
Included studies
The initial database search identified 3,723 records (PubMed, n = 886; Embase, n = 865; Cochrane, n = 1,972) (Fig. 1). After duplicates were removed and screened, the full texts of 286 articles were assessed for eligibility, of which 12 met the eligibility criteria (Tables 1–3). A total of 708 participants were included and assessed in this systematic review. Seven trials of 122 participants assessed the treatment effects of aerobic exercise, including bicycle or motor-driven treadmill training [48–51] (n = 66) and walking [52–54] (n = 56); six trials of 116 participants reported on resistance exercise, including elastic band training [55–57] (n = 48), circuit exercise [51, 53] (n = 46), and dumbbell training group [58] (n = 22). Moreover, one trial researched on multimodal exercise [59] (n = 147). In total, 112 participants with MCI in the control groups were compared to the aerobic training group, who received a waiting list, a maintaining lifestyle routine, a strength or balance tone, muscle-stretching exercises, or social visits; 126 participants in the control groups were compared to the resistance training group, who received a regular lifestyle routine, a strength or balance tone, stretching exercises, or lecture counseling classes; and 131 participants in the control groups were compared with the multimodal exercise group. Three mind–body training studies were excluded because their exercise protocol involved home-based exercise and lacked supervision [60–62]. No further articles were found by searching the reference lists of reviews identified during the initial search or in the included articles.
Table 1
Characteristics of studies –aerobic exercise versus control group
| Study | RCT design | Country | Group (N) | Sex (male/female) | Mean age | MMSE | Diagnosis criteria | Exercise | Outcome |
| Tsai et al. [51] | Parallel | China | Aerobic exercise (AE) n = 19 Resistance exercise (RE) n = 18 Static stretching exercises (CO) n = 18 | 5/14 (AE) 7/11 (RE) 5/13 (CO) | 66.00 (AE) 65.44 (RE) 65.17 (CO) | 27.16±1.26 (AE) 26.56±1.34 (RE) 27.00±1.65 (CO) | Gauthier 2006, Petersen 2004, Winblad 2004 | AE: Type: Bicycle ergometer or motor-driven treadmill Intensity: 70–75% of the target heart rate reserve (HRR) Frequency: 3 sessions/week Duration: 40 min Time: 16 weeks CO: Type: Static stretching exercises Intensity: No load Frequency, duration, and time: same to AE group | Working memory: Digit span of Wechsler-IV Adult intelligence test |
| Yogev-Seligmann et al. [50] | Parallel | Israel | AE n = 13 Balance and tone (BAT) n = 14 | 8/5 (AE) 7/7 (BAT) | 70.84 (AE) 71.92 (BAT) | Not mentioned | Albert 2011 | AE: Type: Stationary bicycles Intensity: 70% to 80% HRR; Frequency: 3 sessions/week Duration: 40 min Time: 16 weeks BAT: Type: balance, gross motor coordination, and light toning exercises Intensity: maintaining heart rate below 30% of HRR Frequency, duration, and time: same to AE group | Immediate and delayed memory: The Rey Auditory Verbal Learning Test Working memory: Digit span component of the Wechsler memory test Processing speed: The color version of the trail making test 1 Execution function: The verbal fluency test Attention: The color version of the trail making test 2 Recognition: Faces/houses recognition test |
| Scherder et al. [52] | Parallel | America | AE n = 15 Hand and face exercises Control (CO) n = 15 | 2/13 (AE) 1/14 (CO) | 84 (AE) 86 (CO) | 9.73±1.94 (AE) 9.87±1.41 (CO) | Petersen 1999 | AE: Type: Self-paced slow walking with an aid Frequency: 3 sessions/week Duration:30 mins Time:6 weeks CO: One subgroup eight subjects received social visits as a ‘treatment’, while in the other subgroup the remaining seven subjects continued their normal social activities. | Executive function: Retrieve familiar information from semantic memory (Category Naming); Processing speed: Trail-making A + B Working memory: Digit span from the Wechsler Memory Scale— Revised Memory: Visual Memory Span, The Verbal Learning and Memory Test, Direct Recall; Rivermead Behavioural Memory Test (faces, pictures) Delayed memory and recognition: The Verbal Learning and Memory Test, delayed recall and recognition. |
| Nagamatsu et al. [53] | Parallel | Canada | AE n = 30 RE n = 28 BAT n = 28 | 27.4±1.5 (AE) 27.0±1.8 (RE) 27.1±1.7 (CO) | All female | 75.6 (AE) 73.9 (RE) 75.1 (CO) | Petersen2004 | AE: Type: Outdoor walking Intensity: 70% to 80% of HRR, 13–15 on the RPE scale Frequency: 2 sessions/week Duration: 60 min Time: 26 weeks BAT: Type: Stretching exercises, range of motion exercises, balance exercises functional and relaxation techniques Intensity: No loading Duration and time: same with RE group | Verbal memory and learning: The Rey Auditory Verbal Learning Test, delayed recall; Spatial Memory: recall the spatial location of dots presented on a screen; Processing speed: Choice Reaction Time |
| Law et al. [48] | Parallel | China | AE n = 16 Waitlist control group (CO) n = 14 | 8/8 5/9 | 77.94 (AE) 75.14 (CO) | Not mentioned | Albert 2011 | AE: Type: Structured whole body movement exercise, bicycle, and arm ergometry Intensity: Moderate intensity aerobic exercise, at 4–5/10 on rate of perceived exertion Frequency: 12 sessions Duration: 60-min Time: 8 weeks | Memory: Chinese Version Verbal Learning Test; Processing speed: Trail Making Test A Attention: Trail Making Test B |
| Combourieu Donnezan et al. [49] | Parallel | France | AE n = 18 Cognitive training; Combined training; Control group (CO) n = 14 | Not mentioned | 77.1 (AE) 79.2 (CO) | 28.2±0.43; 27.3±0.5 | Petersen 2004 | AE: Type: Bikes training Intensity: moderate intensity (i.e., 60% HR) Frequency: 2 sessions/week Duration: 60 min Time: 12 weeks | Executive function: The Matrix Reasoning test Attention: The flexibility part of the Stroop Color Word test, The Digit Span Forward test Working memory: The Digit Span Backward test |
| Damirchi et al. [54] | Parallel | Iran | AE n = 11 Mental training; Exercise + mental; Control group (CO) n = 9 | All female | 68.81 (AE) 69.11 (CO) | 23.18±2.18; 23.44±2.06 | Petersen 2004 | Type: Walking with muscular strength training Intensity: Walking from 55% to 75% heart rate reserve, muscle strength rating of perceived exertion within the desired 13 to 15 range; Frequency: 3 sessions/week; Duration: 60 min; Time: 8 weeks | Processing speed: Reaction time, Digit Symbol Coding test Attention: Modified Stroop color word test error number, Digit span forward subtests of the Wechsler Adult Intelligence Scale |
Table 2
Characteristics of studies –resistance exercise versus control group
| Study | RCT design | Country | Group (N) | Sex (male/female) | Mean age | MMSE | Diagnosis criteria | Exercise | Outcome |
| Tsai et al. [51] | Parallel | China | Resistance exercise (RE) n = 18 Static stretching exercises (CO) n = 18 | 7/11 (RE) 5/13 (CO) | 65.44 (RE) 65.17 (CO) | 26.56±1.34 (RE) 27.00±1.65 (CO) | Gauthier 2006, Petersen 2004, Winblad 2004 | RE: Type: Circuit-exercise use free weights and bodybuilding machines Intensity: 75% of their target 1-RM Frequency: 3 sessions/week Duration: 40 min Time: 16 weeks CO: Type: Static stretching exercises Intensity: No load Frequency, duration, and time: same to RE group | Working memory: Digit span of Wechsler-IV Adult intelligence test |
| Hong et al. [55] | Parallel | Korea | RE n = 10 CO n = 12 | 3/7 (RE) 3/9 (CO) | Male 78.33 Female 77.71 (RE) Male 78.33 Female 75.11 (CO) | Not mentioned | Petersen 1999 | Type: Elastic band Frequency: 2 sessions/week Intensity: 15-repetition maximum (15RM, about 65% of maximum) Duration: 60 min Time: 12 weeks CO: maintain current lifestyle | Execution function: Category/Semantic fluency test, Letter/Phonemic fluency test; Attention and working memory: The digit span test; Stroop test; Immediate Memory and recognition: Short-term and recognition memory, Rey 15-Item Memory Test |
| Yoon et al. [57] | Parallel | Korea | RE n = 22 CO n = 23 | 6/14 (RE) 7/16 (CO) | 73.82 (RE) 74.03 (CO) | 24.23±2.89 (RE) 24.22±1.86 (CO) | CDR, Kelaiditi 2013 | RE: Type: High-speed resistance training Intensity: blue elastic bands, at a perceived exertion rate of 12–13; 2–3 sets of 12–15 repetitions Frequency: 3 sessions/week Duration: 60 min Time: 16 weeks CO: Type: Balance and resistance band stretching Frequency: 2 sessions/week Duration and time: same with RE group | Memory: Rey 15-Item memory test; Processing speed and attention: Trail Making A&B Test, Working memory: Digit Span (both forward and backward) test; Executive functions: Frontal assessment battery |
| Nagamatsu et al. [53] | Parallel | Canada | Aerobic Training (AE) n = 30 RE n = 28 Balance and Tone (BAT) n = 28 | All female | 75.6 (AE) 73.9 (RE) 75.1 (CO) | 27.4±1.5 (AE) 27.0±1.8 (RE) 27.1±1.7 (CO) | Petersen 2004 | Type: Keiser Pressurized Air system Intensity: 6–8 repetitions (two sets), 13–15 on the Borg’s Rating of Perceived Exertion Frequency: 2 sessions/week Duration: 60 min Time: 26 weeks BAT: Type: Stretching exercises, range of motion exercises, balance exercises functional and relaxation techniques Intensity: No load Duration and time: same with RE group | Verbal memory and learning: The Rey Auditory Verbal Learning Test, delayed recall; Spatial Memory: recall the spatial location of dots presented on a screen; Processing speed: Choice Reaction Time |
| Lee et al. [56] | Parallel | Korea | RE n = 18 Control: lecture consultation (CO) n = 22 | 7/11 9/13 | 73.7 (RE) 74.2 (CO) | 23.8±2.9; 23.4±1.3 | CDR Morris 1993 | RE: Type: High speed elastic band Frequency:3 sessions/week Intensity:10–12 repetitions of two to three sets, perceived exertion index ranging from 12 to 13 Duration: 50 min Time: 8 weeks | Executive function: Frontal Assessment Battery |
| Lü et al. [58] | Parallel | China | RE n = 22 CO n = 23 | 6/16 7/23 | 69.00 (RE) 70.43 (CO) | 7.23±1.63; 26.43±2.00 | Petersen, 1999 | RE: Type: Momentum based dumbbell-training Intensity: Each individual spinning exercise lasted 1–2 minutes with repetitions set at 4–5 minutes. Frequency: 3 sessions/week Duration: 60 min Time:12-week | Attention: The Trail Making Test B; The Digit Span Test forward Working memory: The Digit Span Test backward |
Table 3
Characteristics of studies –Multimodal exercise versus control group
| Study | RCT design | Country | Group (N) | Sex (male/female) | Mean age | MMSE | Diagnosis criteria | Exercise | Outcome |
| Lam et al. [59] | Parallel | China | Multimodal motion exercise (ME) n = 147; Cognitive group; Integrated cognitive-physical Group; Social group (S) n = 131 | 34/113 (ME) 29/101 (S) | 75.5 (ME) 75.4 (S) | 25.8±2.3 (ME); 25.6±2.4 (S) | Winblad 2004 | AE: Type: One stretching &toning exercise, one mind body exercise and one aerobic exercise session Frequency: 3 sessions/week Duration: 60 min Time: 12 months S: Attending in social activities | Episodic memory: The list learning delayed recall test Executive function: Category verbal fluency test; Subjective Cognitive complaints: Memory Inventory for Chinese |
Risk of bias
Studies without a statement of random sequence generation or allocation concealment in sufficient detail were judged to have an “unclear” risk of bias [45]. Most of the studies did not report protocols; therefore, it was not possible to determine if there was a selection bias. In all the assessed studies, it was not feasible to blind the participants to exercise training interventions. Therefore, the included studies all showed “high risk” of blinding for participants and personnel (performance bias). Half of the included studies stated that non-blind or without details of blinding of outcome assessors. It was judged non-blind as a “high-risk” bias and “not clear” for that without details of the detection bias. Studies were assessed as having a high risk of bias for incomplete outcome data (attrition bias) if they had a relatively high and unbalanced missing rate between groups or did not account for dropout. All other sectors had a low risk of bias (Fig. 2).
Aerobic exercise intervention versus control group
Seven studies including 234 participants with MCI relative to aerobic exercise intervention and any active or no intervention control groups were pooled for meta-analyses, which contributed data to no less than one cognitive domain [48–54]. The grouping of cognitive scales and studies over specific domains of cognitive function is shown in Table 4. We were able to perform meta-analyses at all seven of our pre-specified cognitive domains (Supplementary Material, Outcome 1.1 to Outcome 1.7). The results revealed no heterogeneity (I2 = 0%) across studies investigating processing speed and recognition, low heterogeneity in immediate memory (I2 = 24%), moderate heterogeneity in working memory (I2 = 47%), delayed memory (I2 = 36%), and attention (I2 = 42%). However, studies including executive function demonstrated substantial heterogeneity (I2 = 62%). A sensitivity analysis was performed with the main analysis performed with and without each study in investigating executive function; the significance of the results did not change (Supplementary Material, Outcome 1.6 and Outcome 1.6.1). The duration of each aerobic exercise intervention in these studies lasted from 30 to 60 min, with 1–3 sessions/week, ranging from 6 to 26 weeks. There was no significant difference between the aerobic exercise and control groups in immediate memory (p = 0.79), executive function (p = 0.1), working memory (p = 0.49), processing speed (p = 0.93), delayed memory (p = 0.96), attention (p = 0.39), or recognition (p = 0.56). One study observed the maintenance effects of aerobic exercise after treatment termination, reporting that the treatment effects declined during the treatment-free period [52]. There was no difference between the aerobic exercise and control groups in dropout rates (odds ratio [OR], 2.47; 95% CI, 0.94–6.49; seven trials, 251 participants; Supplementary Material, Outcome 1.8). Two studies reported no adverse events in any group during the course of the intervention [48, 50]. One study reported the presence of adverse events, including episodes of shortness of breath that resolved with rest and non-injurious falls [53], with no significant differences between groups (p = 0.54). The other studies did not mention any adverse events.
Table 4
Grouping of cognitive tests and studies over cognitive functions
| Cognitive function | Cognitive tests | Trial |
| Immediate memory | The Verbal Learning and Memory Test Direct recall | Scherder et al. [52] |
| Chinese Version Verbal Learning Test, total free recall | Law et al. [48] | |
| The Rey Auditory Verbal Learning Test | Nagamatsu et al. [53], Yogev-Seligmann et al. [50] | |
| Rey 15-Item Memory Test | Hong et al. [55], Yoon et al. [57] | |
| Working memory | Digit span backward | Lu et al. [58], Combourieu Donnezan et al. [49], Hong et al. [55] |
| Digit span component of the Wechsler memory test | Scherder et al. [52], Yoon et al. [57], Tsai et al. [51], Yogev-Seligmann et al. [50] | |
| Delayed memory | Rey auditory verbal learning test delayed recall trail | Nagamatsu et al. [53], Yogev-Seligmann et al. [50] |
| The Verbal Learning and Memory Test, delayed recall | Scherder et al. [52] | |
| Chinese Version Verbal Learning Test, delayed recall | Law et al. [48] | |
| The list learning delayed recall test | Lam et al. [59] | |
| Processing speed | Reaction time of modified Stroop color-word test | Damirchi et al. [54] |
| Reaction time of spatial memory | Nagamatsu et al. [53] | |
| Trail making test A | Yoon et al. [57], Law et al. [48], Yogev-Seligmann et al. [50] | |
| Trail-making A + B | Scherder et al. [52] | |
| Attention | Trail making test B | Lu et al. [58], Yoon et al. [57], Law et al. [48], Yogev-Seligmann et al. [50] |
| Digit span (forward) | Combourieu Donnezan et al. [49], Damirchi et al. [54], Hong et al. [55] | |
| Executive function | Category verbal fluency | Scherder et al. [52], Lam et al. [59] |
| Verbal fluency, semantic | Hong et al. [55], Yogev-Seligmann et al. [50] | |
| Frontal Assessment Battery | Yoon et al. [57], Lee et al. [56] | |
| Matrix Reasoning test | Combourieu Donnezan et al. [49] | |
| Recognition | Faces/houses recognition | Yogev-Seligmann et al. [50] |
| The Verbal Learning and Memory Test, recognition | Scherder et al. [52] | |
| Rey 15-Item Memory Test, recognition | Hong et al. [55] |
Resistance exercise intervention versus control group
Six studies including 242 participants with MCI relative to resistance exercise intervention and any active or no intervention control groups were pooled for meta-analyses, which contributed data to at least one cognitive domain [51, 53, 55–58]. We performed meta-analyses on five cognitive domains because only one study was involved in the domain of delayed memory [53] and recognition [55] each (Figs. 3 and 4; Supplementary Material, Outcome 2.1 to Outcome 2.4, Outcome 2.7). The results revealed no heterogeneity (I2 = 0%) across studies investigating immediate memory and executive function and low heterogeneity in attention (I2 = 13%); however, studies including working memory (I2 = 32%) and processing speed (I2 = 42%) demonstrated moderate heterogeneity.
Fig. 3
Outcome 2.5 Impact of resistance exercise training on attention. CI, confidence interval; IV, inverse variance; SD standard deviation; Std, standardized.
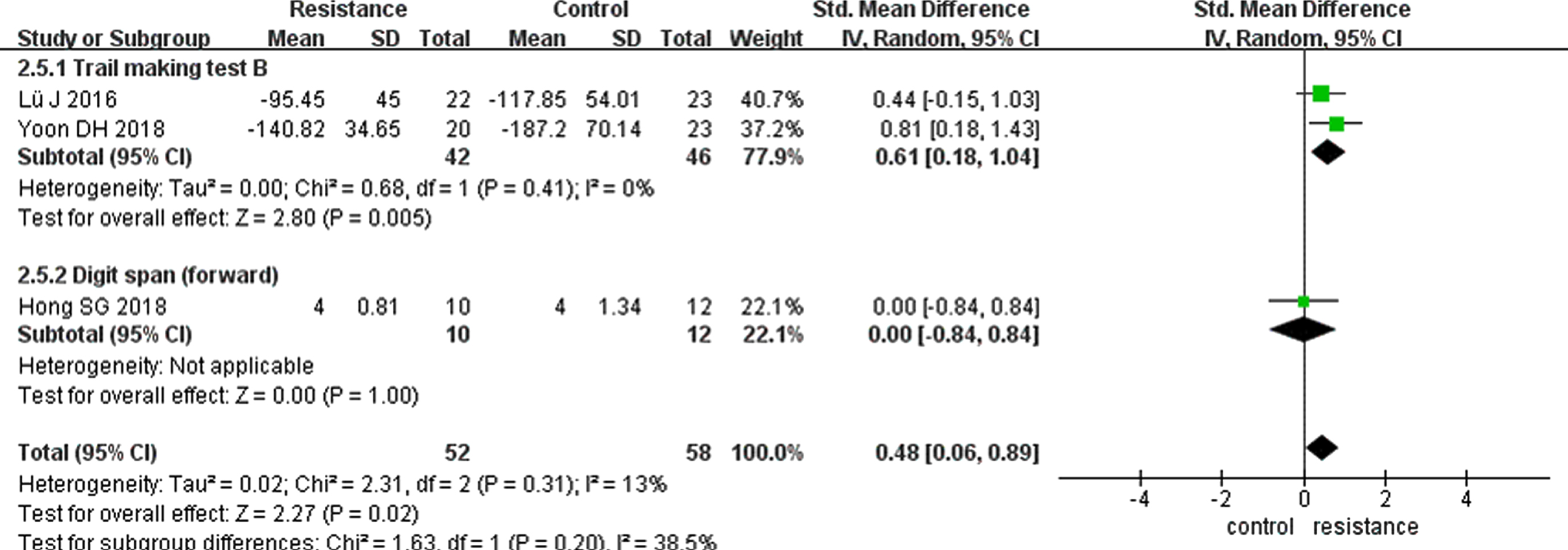
Fig. 4
Outcome 2.6 Impact of resistance exercise training on executive function. CI, confidence interval; IV, inverse variance; SD standard deviation; Std, standardized.
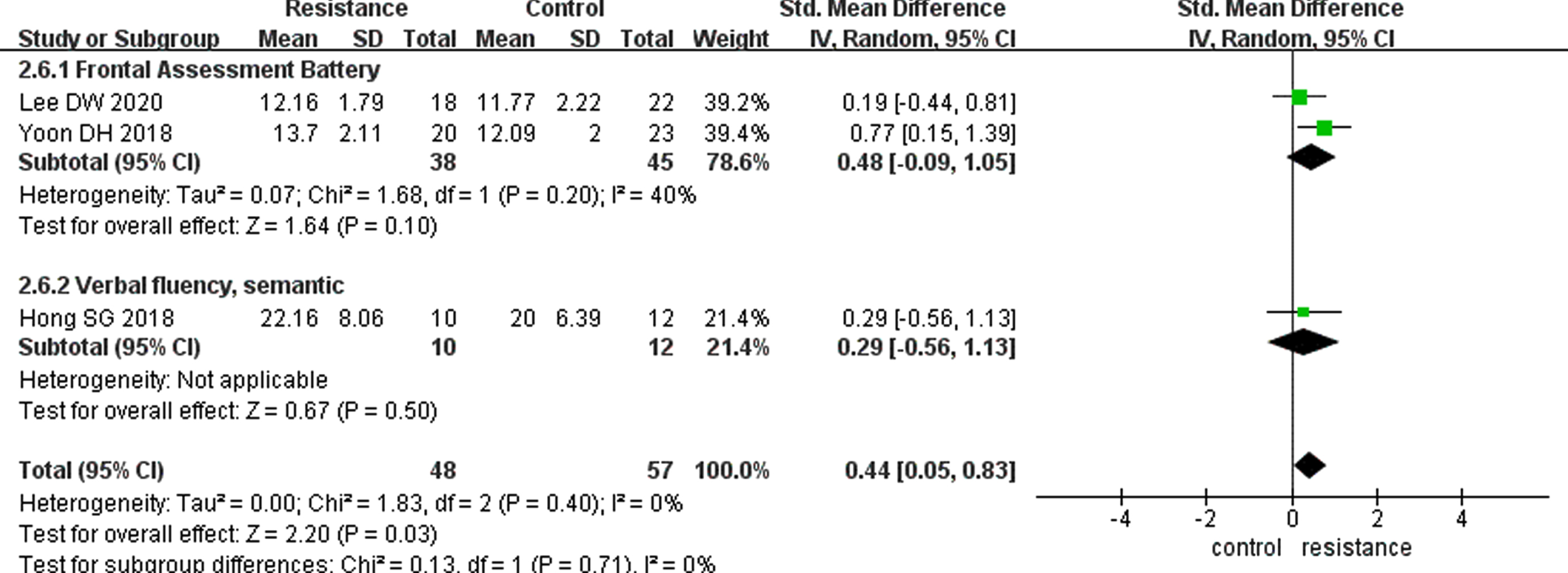
The duration of each resistance exercise intervention in these studies lasted from 40 to 60 minutes, with 2–3 sessions/week, ranging from 8 to 26 weeks. Meta-analysis on pooled data revealed significant improvement differences for the resistance exercise intervention versus control groups on measures of attention (0.48 [0.06–0.89], p < 0.05) and executive function (0.44 [0.05–0.83], p < 0.05), but not on immediate memory (p = 0.79), working memory (p = 0.19), processing speed (p = 0.92), delayed memory (p = 0.82), or recognition (p = 0.77). There was no difference in the dropout rates between the resistance exercise and control groups (OR, 1.21; 95% CI, 0.59–2.50; six trials; Supplementary Material, Outcome 2.8). One study reported the maintenance effects of resistance exercise treatment on participants with MCI [49], and the outcome of the matrix reasoning test (p < 0.01) and digit span forward (p < 0.05) still improved for the 6-month post-test relative to the pre-test. Two studies reported no adverse events in any group during the course of the intervention [56, 58]. One study reported no significant differences of adverse event occurrence between groups (p = 0.54) [53]. The other studies did not mention any adverse events.
Multimodal exercise intervention versus control group
Lam et al. assessed the effect of multimodal exercise intervention on cognitive function in 114 individuals with MCI [59]. These cognitive domains involved outcomes of pre- and post-training measures of delayed recall and executive function (category verbal fluency test). The trial had a fair methodological quality. The author found a significant improvement favoring multimodal exercise intervention over the control group on measures of both the category verbal fluency test and delayed recall after 12 months of intervention (multilevel model, p < 0.001). There was no difference between the multimodal exercise and control groups in the dropout rates. This study reported no adverse events associated with this intervention. No differences in age and educational level were observed between completers and defaulters.
DISCUSSION
Summary of main results
We examined the effects of aerobic, resistance, and multimodal exercise training on cognitive function in adults aged > 60 years with MCI. One multimodal exercise intervention study was presented insufficiently. Meta-analysis results revealed that, compared to the control group, resistance exercise significantly improved performance on measures of attention and executive function. No significant differences were observed in any of the remaining cognitive domains.
We included 12 studies after screening because of a more qualified inclusion criterion. Most studies involved small sample sizes. There was significant heterogeneity in the methodologies across the studies involved, including sample size, exercise schemes, participant compliance, and study quality. Although the review analyzed the fine-sorted subgroups of cognitive function, there could be variations in the results of each measure. We observed that half of the studies reported significant improvements in composite measures of cognitive function for exercise versus controls, including executive function [49, 52, 57], working memory [55], and processing speed [50, 52, 53, 57]. Despite this, the majority of comparisons yielded no significant differences. Additionally, the results of this meta-analysis could have been affected by the quality of the included trials. Across the included papers, approximately half did not state the methods of randomization or blinding of outcome assessors. For all but one trial, allocation was poorly reported. No trial evaluated contamination bias that could have interfered with the outcomes. Only two trials reported protocols [57, 59]; for most trials, it was not feasible to determine whether there was selective reporting of results.
Some researchers have suggested that improvements in cognitive function could be attributed to improvements in cardiovascular fitness due to exercise [63]. Changes in grip strength and walking speed have been correlated with mental state and fluid cognition [64]. However, most trials involved in this review did not report any objective measures of cardiorespiratory fitness. In addition, studies have reported that short session duration and higher frequency might predict higher effect sizes [65, 66]. However, owing to the inconsistency of exercise modalities in this review, dose-response tests were not performed in this study.
Agreements and disagreements with other studies or reviews
Seven meta-analyses published data based on similar hypotheses yet failed to find comparable results.
Gates et al. assessed the effects of exercise on cognitive function in 14 RCT trials with 1,695 participants [43]. Their eligibility criteria differed from this study in that they included participants with probable MCI, and subjective memory decline who were aged > 65. We both set the criteria for exercise intervention up longer than 4 weeks and prescribed them specifically. However, we only included trials that reported exercise training effectively supervised by centers, physicians, or professionals; those self-reported, at home, or without reported supervision were excluded. The authors concluded that there is limited evidence to prove that any exercise modality improves cognitive function in individuals with MCI.
De Souto Barreto et al. reviewed five papers on long-term exercise (12 months or longer) in older adults with MCI, onset of dementia, or clinically meaningful cognitive decline [67]. Apart from the inclusion criteria, another difference is that they considered the change in MMSE score as a main outcome indicator and analyzed the overall effect of exercise, whereas we discussed the different exercise modalities separately. Their review observed no significant effects of exercise, either individually or in combination, on reducing the risk of cognitive decline.
Zhang et al. published a meta-analytic review of traditional Chinese exercise in older adults with MCI [68]. They found that four Tai Chi studies and one Liuzijue study met the inclusion criteria. We excluded trials on participants with MCI with a definite etiology, whereas this review included medical or neurological disorders, such as AD, dementia, or Parkinson’s disease. The authors concluded that exercise improved the visuospatial function for individuals with MCI.
The meta-analysis presented by Lee et al. has a similar aim (reporting the effects of exercise intervention for older adults with MCI) and exclusion criteria (cross-sectional, protocol, and review studies) [69]. In contrast to this review, our study subdivided cognitive function into detailed items instead of MMSE. In addition, this review finally involved three eligible studies, including five exercise interventions (aerobic or resistance exercise) combined for data analysis, and only one study was classified into a functional category. This review reported that cognitive function was significantly increased in the exercise group.
Biazus-Sehn et al. reviewed the global effects of various exercise modalities on MCI. Their search identified 27 studies that reported data [42]. The difference is that they involved participants with a mean age of ≥60 years who had other diseases, such as insulin resistance. We excluded those who were not purely cognitively impaired but had other diseases, which might disturb the exercise effect and cognitive function. They reported improved global cognitive function, executive function, and delayed recall after the exercise.
Similarly, Zhu et al. reviewed and analyzed aerobic dance in participants with MCI aged > 50 years. This meta-analysis involved five studies with 842 patients [70]. They found that aerobic dance, including Tai Chi, improved global cognitive function and memory executive function in older adults with MCI.
A meta-analysis by Lin et al. assessed the effects of Tai Chi on cognitive performance. Except for exercise intervention, the criteria differed from this review in including younger participants with MCI [71]. This meta-analysis indicated that Tai Chi has positive clinical effects on cognitive function (global cognitive function, memory and learning, executive function) in older adults with MCI.
Implications for practice and research
We found that resistance exercise improved executive function and attention performance in patients aged > 60 years. However, there might be some confounding factors in the outcomes. First, there are more studies and diversified scales involved in aerobic exercise analyses, which might lead to higher heterogeneity, and the large variability in training paradigms and study quality might also influence the outcome. Further investigations into the parameters and populations most associated with the efficacy of physical training for cognitive function are necessary. Cognition is a complex and multi-class function; however, there is insufficient evidence to illustrate the relationship between exercise and brain-processed cognitive function. Certainly, clear differences exist in the effects of exercise on the cognition subgroups. Within the seven disparate intrinsic connectivity networks in the brain, the beneficial effects exerted by aerobic exercise might be mediated by the greatest association with the executive and dorsal attention networks [72]. Exercise activates the hub region of the executive network (e.g., attention, working memory, cognitive control) in the brain [11, 73], and the duration of exercise may be positively correlated with its volume [74]. Exercise-induced brain functional homogeneity variation is likely to improve executive control behavior and predict attention behavior [75]. This evidence may help to explain the results. Thus, to elucidate the exact relationship between exercise and cognitive function in patients with MCI, more large-sample RCTs and animal studies are required in the future. It also raises our wider understanding of how to improve exercise compliance and to use a smaller battery of cognitive scales for the uniformity and comparability of results.
ACKNOWLEDGMENTS
This work was supported by grants from the Capital Health Research and Development of Special (No.2020-1-6011) to HZ. We thank the authors who provided the original article and information during the screening and analysis.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0243r2).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-220243.
REFERENCES
[1] | Fazio S , Pace D , Maslow K , Zimmerman S , Kallmyer B ((2018) ) Alzheimer’s Association dementia care practice recommendations. Gerontologist 58: , S1–S9. |
[2] | Petersen RC ((2004) ) Mild cognitive impairment as a diagnostic entity. J Intern Med 256: , 183–194. |
[3] | Petersen RC , Caracciolo B , Brayne C , Gauthier S , Jelic V , Fratiglioni L ((2014) ) Mild cognitive impairment: A concept in evolution. J Intern Med 275: , 214–228. |
[4] | Albert MS , DeKosky ST , Dickson D , Dubois B , Feldman HH , Fox NC , Gamst A , Holtzman DM , Jagust WJ , Petersen RC , Snyder PJ , Carrillo MC , Thies B , Phelps CH ((2011) ) The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7: , 270–279. |
[5] | Liss JL , Seleri Assuncao S , Cummings J , Atri A , Geldmacher DS , Candela SF , Devanand DP , Fillit HM , Susman J , Mintzer J , Bittner T , Brunton SA , Kerwin DR , Jackson WC , Small GW , Grossberg GT , Clevenger CK , Cotter V , Stefanacci R , Wise-Brown A , Sabbagh MN ((2021) ) Practical recommendations for timely, accurate diagnosis of symptomatic Alzheimer’s disease (MCI and dementia) in primary care: A review and synthesis. J Intern Med 290: , 310–334. |
[6] | Petersen RC , Lopez O , Armstrong MJ , Getchius TSD , Ganguli M , Gloss D , Gronseth GS , Marson D , Pringsheim T , Day GS , Sager M , Stevens J , Rae-Grant A ((2018) ) Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 90: , 126–135. |
[7] | Karssemeijer EGA , Aaronson JA , Bossers WJ , Smits T , Olde Rikkert MGM , Kessels RPC ((2017) ) Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res Rev 40: , 75–83. |
[8] | Gavelin HM , Dong C , Minkov R , Bahar-Fuchs A , Ellis KA , Lautenschlager NT , Mellow ML , Wade AT , Smith AE , Finke C , Krohn S , Lampit A ((2021) ) Combined physical and cognitive training for older adults with and without cognitive impairment: A systematic review and network meta-analysis of randomized controlled trials. Ageing Res Rev 66: , 101232. |
[9] | Meng Q , Yin H , Wang S , Shang B , Meng X , Yan M , Li G , Chu J , Chen L ((2021) ) The effect of combined cognitive intervention and physical exercise on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Aging Clin Exp Res 34: , 261–276. |
[10] | Ryan SM , Kelly ÁM ((2016) ) Exercise as a pro-cognitive, pro-neurogenic and anti-inflammatory intervention in transgenic mouse models of Alzheimer’s disease. Ageing Res Rev 27: , 77–92. |
[11] | Lu X , Moeini M , Li B , de Montgolfier O , Lu Y , Bélanger S , Thorin É , Lesage F ((2020) ) Voluntary exercise increases brain tissue oxygenation and spatially homogenizes oxygen delivery in a mouse model of Alzheimer’s disease. Neurobiol Aging 88: , 11–23. |
[12] | Choi DH , Kwon KC , Hwang DJ , Koo JH , Um HS , Song HS , Kim JS , Jang Y , Cho JY ((2021) ) Treadmill exercise alleviates brain iron dyshomeostasis accelerating neuronal amyloid-β production, neuronal cell death, and cognitive impairment in transgenic mice model of Alzheimer’s disease. Mol Neurobiol 58: , 3208–3223. |
[13] | Liu Y , Chu JMT , Yan T , Zhang Y , Chen Y , Chang RCC , Wong GTC ((2020) ) Short-term resistance exercise inhibits neuroinflammation and attenuates neuropathological changes in 3xTg Alzheimer’s disease mice. J Neuroinflammation 17: , 4. |
[14] | Nakanishi K , Sakakima H , Norimatsu K , Otsuka S , Takada S , Tani A , Kikuchi K ((2021) ) Effect of low-intensity motor balance and coordination exercise on cognitive functions, hippocampal Aβ deposition, neuronal loss, neuroinflammation, and oxidative stress in a mouse model of Alzheimer’s disease. Exp Neurol 337: , 113590. |
[15] | Kim TW , Park SS , Park JY , Park HS ((2020) ) Infusion of plasma from exercised mice ameliorates cognitive dysfunction by increasing hippocampal neuroplasticity and mitochondrial functions in 3xTg-AD mice. Int J Mol Sci 21: , 3291. |
[16] | García-Mesa Y , Colie S , Corpas R , Cristòfol R , Comellas F , Nebreda AR , Giménez-Llort L , Sanfeliu C ((2016) ) Oxidative stress is a central target for physical exercise neuroprotection against pathological brain aging. J Gerontol A Biol Sci Med Sci 71: , 40–49. |
[17] | Pang R , Wang X , Pei F , Zhang W , Shen J , Gao X , Chang C ((2019) ) Regular exercise enhances cognitive function and intracephalic GLUT expression in Alzheimer’s disease model mice. J Alzheimers Dis 72: , 83–96. |
[18] | Binda KH , Lillethorup TP , Real CC , Bærentzen SL , Nielsen MN , Orlowski D , Brooks DJ , Chacur M , Landau AM ((2021) ) Exercise protects synaptic density in a rat model of Parkinson’s disease. Exp Neurol 342: , 113741. |
[19] | Borjesson M , Onerup A , Lundqvist S , Dahlof B ((2016) ) Physical activity and exercise lower blood pressure in individuals with hypertension: Narrative review of 27 RCTs. Br J Sports Med 50: , 356–361. |
[20] | O’Malley PG , Arnold MJ , Kelley C , Spacek L , Buelt A , Natarajan S , Donahue MP , Vagichev E , Ballard-Hernandez J , Logan A , Thomas L , Ritter J , Neubauer BE , Downs JR ((2020) ) Management of dyslipidemia for cardiovascular disease risk reduction: Synopsis of the 2020 updated U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guideline. Ann Intern Med 173: , 822–829. |
[21] | Balducci S , Sacchetti M , Haxhi J , Orlando G , D’Errico V , Fallucca S , Menini S , Pugliese G ((2014) ) Physical exercise as therapy for type 2 diabetes mellitus. Diabetes Metab Res Rev 30: , 13–23. |
[22] | Yarizadeh H , Eftekhar R , Anjom-Shoae J , Speakman JR , Djafarian K ((2021) ) The effect of aerobic and resistance training and combined exercise modalities on subcutaneous abdominal fat: A systematic review and meta-analysis of randomized clinical trials. Adv Nutr 12: , 179–196. |
[23] | Aengevaeren VL , Mosterd A , Sharma S , Prakken NHJ , Möhlenkamp S , Thompson PD , Velthuis BK , Eijsvogels TMH ((2020) ) Exercise and coronary atherosclerosis: Observations, explanations, relevance, clinical management. Circulation 141: , 1338–1350. |
[24] | Grabs V , Peres T , Zelger O , Haller B , Pressler A , Braun S , Halle M , Scherr J ((2015) ) Decreased prevalence of cardiac arrhythmias during and after vigorous and prolonged exercise in healthy male marathon runners. Am Heart J 170: , 149–155. |
[25] | Kalaria RN , Maestre GE , Arizaga R , Friedland RP , Galasko D , Hall K , Luchsinger JA , Ogunniyi A , Perry EK , Potocnik F , Prince M , Stewart R , Wimo A , Zhang ZX , Antuono P ; World Federation of Neurology Dementia Research Group ((2008) ) Alzheimer’s disease and vascular dementia in developing countries: Prevalence, management, risk factors. Lancet Neurol 7: , 812–826. |
[26] | Niewada M , Michel P ((2016) ) Lifestyle modification for stroke prevention: Facts and fiction. Curr Opin Neurol 29: , 9–13. |
[27] | Kelly ME , Loughrey D , Lawlor BA , Robertson IH , Walsh C , Brennan S ((2014) ) The impact of exercise on the cognitive functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res Rev 16: , 12–31. |
[28] | Chen FT , Etnier JL , Chan KH , Chiu PK , Hung TM , Chang YK ((2020) ) Effects of exercise training interventions on executive function in older adults: A systematic review and meta-analysis. Sports Med 50: , 1451–1467. |
[29] | Northey JM , Cherbuin N , Pumpa KL , Smee DJ , Rattray B ((2018) ) Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br J Sports Med 52: , 154–160. |
[30] | Marinus N , Hansen D , Feys P , Meesen R , Timmermans A , Spildooren J ((2019) ) The impact of different types of exercise training on peripheral blood brain-derived neurotrophic factor concentrations in older adults: A meta-analysis. Sports Med 49: , 1529–1546. |
[31] | Wang R , Holsinger RMD ((2018) ) Exercise-induced brain-derived neurotrophic factor expression: Therapeutic implications for Alzheimer’s dementia. Ageing Res Rev 48: , 109–121. |
[32] | Rogge AK , Roder B , Zech A , Hotting K ((2018) ) Exercise-induced neuroplasticity: Balance training increases cortical thickness in visual and vestibular cortical regions. Neuroimage 179: , 471–479. |
[33] | Colcombe SJ , Erickson KI , Scalf PE , Kim JS , Prakash R , McAuley E , Elavsky S , Marquez DX , Hu L , Kramer AF ((2006) ) Aerobic exercise training increases brain volume in aging humans. J Gerontol A Biol Sci Med Sci 61: , 1166–1170. |
[34] | Frodl T , Strehl K , Carballedo A , Tozzi L , Doyle M , Amico F , Gormley J , Lavelle G , O’Keane V ((2020) ) Aerobic exercise increases hippocampal subfield volumes in younger adults and prevents volume decline in the elderly. Brain Imaging Behav 14: , 1577–1587. |
[35] | Erickson KI , Voss MW , Prakash RS , Basak C , Szabo A , Chaddock L , Kim JS , Heo S , Alves H , White SM , Wojcicki TR , Mailey E , Vieira VJ , Martin SA , Pence BD , Woods JA , McAuley E , Kramer AF ((2011) ) Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A 108: , 3017–3022. |
[36] | Thomas AG , Dennis A , Rawlings NB , Stagg CJ , Matthews L , Morris M , Kolind SH , Foxley S , Jenkinson M , Nichols TE , Dawes H , Bandettini PA , Johansen-Berg H ((2016) ) Multi-modal characterization of rapid anterior hippocampal volume increase associated with aerobic exercise. Neuroimage 131: , 162–170. |
[37] | Horowitz AM , Fan X , Bieri G , Smith LK , Sanchez-Diaz CI , Schroer AB , Gontier G , Casaletto KB , Kramer JH , Williams KE , Villeda SA ((2020) ) Blood factors transfer beneficial effects of exercise on neurogenesis and cognition to the aged brain. Science 369: , 167–173. |
[38] | Wayne PM , Walsh JN , Taylor-Piliae RE , Wells RE , Papp KV , Donovan NJ , Yeh GY ((2014) ) Effect of tai chi on cognitive performance in older adults: Systematic review and meta-analysis. J Am Geriatr Soc 62: , 25–39. |
[39] | Wu C , Yi Q , Zheng X , Cui S , Chen B , Lu L , Tang C ((2019) ) Effects of mind-body exercises on cognitive function in older adults: A meta-analysis. J Am Geriatri Soc 67: , 749–758. |
[40] | Bhattacharyya KK , Andel R , Small BJ ((2021) ) Effects of yoga-related mind-body therapies on cognitive function in older adults: A systematic review with meta-analysis. Arch Gerontol Geriatr 93: , 104319. |
[41] | Zhou XL , Wang LN , Wang J , Zhou L , Shen XH ((2020) ) Effects of exercise interventions for specific cognitive domains in old adults with mild cognitive impairment: A meta-analysis and subgroup analysis of randomized controlled trials. Medicine 99: , e20105. |
[42] | Biazus-Sehn LF , Schuch FB , Firth J , Stigger FdS ((2020) ) Effects of physical exercise on cognitive function of older adults with mild cognitive impairment: A systematic review and meta-analysis. Arch Gerontol Geriatr 89: , 104048. |
[43] | Gates N , Fiatarone Singh MA , Sachdev PS , Valenzuela M ((2013) ) The effect of exercise training on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Am J Geriatr Psychiatry 21: , 1086–1097. |
[44] | Sofi F , Valecchi D , Bacci D , Abbate R , Gensini GF , Casini A , Macchi C ((2011) ) Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J Intern Med 269: , 107–117. |
[45] | Higgins J , Green SR (2011) Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions. Chichester, England. |
[46] | Higgins JP , Green S (2008) Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration. |
[47] | Cumpston M , Li T , Page MJ , Chandler J , Welch VA , Higgins JP , Thomas J ((2019) ) Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev 10: , ED000142. |
[48] | Law LLF , Mok VCT , Yau MMK ((2019) ) Effects of functional tasks exercise on cognitive functions of older adults with mild cognitive impairment: A randomized controlled pilot trial. Alzheimers Res Ther 11: , 98. |
[49] | Combourieu Donnezan L , Perrot A , Belleville S , Bloch F , Kemoun G ((2018) ) Effects of simultaneous aerobic and cognitive training on executive functions, cardiovascular fitness and functional abilities in older adults with mild cognitive impairment. Ment Health Phys Act 15: , 78–87. |
[50] | Yogev-Seligmann G , Eisenstein T , Ash E , Giladi N , Sharon H , Nachman S , Bregman N , Kodesh E , Hendler T , Lerner Y ((2021) ) Neurocognitive plasticity is associated with cardiorespiratory fitness following physical exercise in older adults with amnestic mild cognitive impairment. J Alzheimers Dis 81: , 91–112. |
[51] | Tsai CL , Pai MC , Ukropec J , Ukropcová B ((2019) ) Distinctive effects of aerobic and resistance exercise modes on neurocognitive and biochemical changes in individuals with mild cognitive impairment. Curr Alzheimer Res 16: , 316–332. |
[52] | Scherder EJ , Van Paasschen J , Deijen JB , Van Der Knokke S , Orlebeke JF , Burgers I , Devriese PP , Swaab DF , Sergeant JA ((2005) ) Physical activity and executive functions in the elderly with mild cognitive impairment. Aging Ment Health 9: , 272–280. |
[53] | Nagamatsu LS , Chan A , Davis JC , Beattie BL , Graf P , Voss MW , Sharma D , Liu-Ambrose T ((2013) ) Physical activity improves verbal and spatial memory in older adults with probable mild cognitive impairment: A 6-month randomized controlled trial. J Aging Res 2013: , 861893. |
[54] | Damirchi A , Hosseini F , Babaei P ((2018) ) Mental training enhances cognitive function and BDNF more than either physical or combined training in elderly women with MCI: A small-scale study. Am J Alzheimers Dis Other Demen 33: , 20–29. |
[55] | Hong SG , Kim JH , Jun TW ((2018) ) Effects of 12-week resistance exercise on electroencephalogram patterns and cognitive function in the elderly with mild cognitive impairment: A randomized controlled trial. Clin J Sport Med 28: , 500–508. |
[56] | Lee DW , Yoon DH , Lee JY , Panday SB , Park J , Song W ((2020) ) Effects of high-speed power training on neuromuscular and gait functions in frail elderly with mild cognitive impairment despite blunted executive functions: A randomized controlled trial. J Frailty Aging 9: , 179–184. |
[57] | Yoon DH , Lee JY , Song W ((2018) ) Effects of resistance exercise training on cognitive function and physical performance in cognitive frailty: A randomized controlled trial. J Nutr Health Aging 22: , 944–951. |
[58] | Lu J , Sun M , Liang L , Feng Y , Pan X , Liu Y ((2016) ) Effects of momentum-based dumbbell training on cognitive function in older adults with mild cognitive impairment: A pilot randomized controlled trial. Clin Interv Aging 11: , 9–16. |
[59] | Lam LC , Chan WC , Leung T , Fung AW , Leung EM ((2015) ) Would older adults with mild cognitive impairment adhere to and benefit from a structured lifestyle activity intervention to enhance cognition? A cluster randomized controlled trial. PLoS One 10: , e0118173. |
[60] | Kasai JY , Busse AL , Magaldi RM , Soci MA , Rosa Pde M , Curiati JA , Jacob Filho W ((2010) ) Effects of Tai Chi Chuan on cognition of elderly women with mild cognitive impairment. Einstein (Sao Paulo) 8: , 40–45. |
[61] | Sungkarat S , Boripuntakul S , Chattipakorn N , Watcharasaksilp K , Lord SR ((2017) ) Effects of Tai Chi on cognition and fall risk in older adults with mild cognitive impairment: A randomized controlled trial. J Am Geriatr Soc 65: , 721–727. |
[62] | Lam LC , Chau RC , Wong BM , Fung AW , Tam CW , Leung GT , Kwok TC , Leung TY , Ng SP , Chan WM ((2012) ) A 1-year randomized controlled trial comparing mind body exercise (Tai Chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 13: , 568.e15–568.e20. |
[63] | Angevaren M , Aufdemkampe G , Verhaar HJJ , Aleman A , Vanhees L (2008) Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst Rev, CD005381. |
[64] | Clouston SA , Brewster P , Kuh D , Richards M , Cooper R , Hardy R , Rubin MS , Hofer SM ((2013) ) The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol Rev 35: , 33–50. |
[65] | Chen ML , Wotiz SB , Banks SM , Connors SA , Shi Y ((2021) ) Dose-response association of Tai Chi and cognition among community-dwelling older adults: A systematic review and meta-analysis. Int J Environ Res Public Health 18: , 3179. |
[66] | Sanders LMJ , Hortobágyi T , la Bastide-van Gemert S , van der Zee EA , van Heuvelen MJG ((2019) ) Dose-response relationship between exercise and cognitive function in older adults with and without cognitive impairment: A systematic review and meta-analysis. PloS One 14: , e0210036. |
[67] | de Souto Barreto P , Demougeot L , Vellas B , Rolland Y ((2018) ) Exercise training for preventing dementia, mild cognitive impairment, and clinically meaningful cognitive decline: A systematic review and meta-analysis. J Gerontol A Biol Sci Med Sci 73: , 1504–1511. |
[68] | Zhang Q , Hu J , Wei L , Cao R , Ma R , Song H , Jin Y ((2019) ) Effects of traditional Chinese exercise on cognitive and psychological outcomes in older adults with mild cognitive impairment: A systematic review and meta-analysis. Medicine 98: , e14581. |
[69] | Lee J ((2020) ) Effects of aerobic and resistance exercise interventions on cognitive and physiologic adaptations for older adults with mild cognitive impairment: A systematic review and meta-analysis of randomized control trials. Int J Environ Res Public Health 17: , 9216. |
[70] | Zhou HX , Chen X , Shen YQ , Li L , Chen NX , Zhu ZC , Castellanos FX , Yan CG ((2020) ) Rumination and the default mode network: Meta-analysis of brain imaging studies and implications for depression. Neuroimage 206: , 116287. |
[71] | Lin R , Cui S , Yang J , Yang H , Feng Z , Wahner-Roedler DL , Zhou X , Salinas M , Mallory MJ , Do A , Bublitz SE , Chon TY , Tang C , Bauer BA , Xu M ((2021) ) Effects of Tai Chi on patients with mild cognitive impairment: A systematic review and meta-analysis of randomized controlled trials. BioMed Res Int 2021: , 5530149. |
[72] | Talukdar T , Nikolaidis A , Zwilling CE , Paul EJ , Hillman CH , Cohen NJ , Kramer AF , Barbey AK ((2018) ) Aerobic fitness explains individual differences in the functional brain connectome of healthy young adults. Cereb Cortex 28: , 3600–3609. |
[73] | Kujach S , Byun K , Hyodo K , Suwabe K , Fukuie T , Laskowski R , Dan I , Soya H ((2018) ) A transferable high-intensity intermittent exercise improves executive performance in association with dorsolateral prefrontal activation in young adults. Neuroimage 169: , 117–125. |
[74] | Northey JM , Rattray B , Pumpa KL , Pryor DJ , Fraser MA , Shaw ME , Anstey KJ , Cherbuin N ((2020) ) Objectively measured physical activity is associated with dorsolateral prefrontal cortex volume in older adults. Neuroimage 221: , 117150. |
[75] | Wei GX , Dong HM , Yang Z , Luo J , Zuo XN ((2014) ) Tai Chi Chuan optimizes the functional organization of the intrinsic human brain architecture in older adults. Front Aging Neurosci 6: , 74. |


