
Japanese National Dementia Plan Is Associated with a Small Shift in Location of Death: An Interrupted Time Series Analysis
Abstract
Background:
Japan has one of the highest percentages of persons with dementia and hospital deaths in the world. Hospitals are often not equipped to handle the care complexity required for persons with dementia at the end of life. The National Dementia Orange plan aimed to decrease hospital deaths by expanding time in the community.
Objective:
The aim of this study is to evaluate whether the National Dementia Orange Plan is associated with a decrease in hospitals deaths for persons with dementia.
Methods:
We used quarterly, cross-sectional, national death certificate data consisting of the total Japanese dementia population 65 years and older, spanning a period from 2009 to 2016. The primary outcome was quarterly adjusted relative risk rates (aRRR) of dying in hospital, nursing home, home, or elsewhere. An interrupted time series analysis was performed to study the slope change over time. Analyses were adjusted for sex and seasonality.
Results:
149,638 died with dementia. With the implementation of the Orange Plan, death in nursing home (aRRR 1.08, [1.07–1.08], p < 0.001) and elsewhere (aRRR 1.05, [1.05–1.06], p < 0.001) increased over time compared to hospital death. No changes were found in death at home.
Conclusion:
This study provides evidence that the National Dementia Orange plan was associated with a small increase in death in nursing home and elsewhere. Hospital death remained the primary location of death. End-of-life strategies should be expanded in national dementia policies to increase aging in the community until death.
INTRODUCTION
Japan has the oldest population in the world with nearly 36 million persons of 65 years and older [1]. The proportion of persons over 65 years old is projected to reach 40%of the total population by 2060 [2]. Parallel to the aging of society, the Japanese government projects 7 million persons with dementia by 2025; one of the highest proportions of dementia in the world [3]. Japan also has the highest percentage of hospital deaths in the world [4]. This is not favorable as hospitalization can be harmful for persons with dementia due to the increased risk of delirium, functional decline, inadequate pain control, and mortality [5, 6]. Moreover, as persons with dementia increasingly experience complex symptoms of cognitive and functional impairments, care needs at the end of life can be difficult to address in hospitals [7, 8]. Although there is only limited evidence available on persons’ with dementia own preference for location of death, a small Japanese study showed that death at home or nursing is preferred over hospital death [9].
The Japanese government introduced in 2013 a national dementia plan, the Orange Plan, which aimed to enable persons with dementia to maximize time in the community by developing dementia friendly communities. Important pillars of the Orange Plan included 1) create a widespread, standardized dementia care pathway; 2) improve community-based healthcare services; 3) strengthen family support in communities; 4) accelerate the development of more health care staff providing long-term care; and 5) facilitate end-of-life care in group homes [10]. Koyama et al. [11] found that since 2005 Japanese proportions of hospital death gradually decreased over time for the total population while nursing home deaths increased. Nakanishi et al. [12] showed that after the introduction of the Orange Plan, persons with dementia were still more likely to die in a hospital, compared to nursing home and home. However, the analysis did not include comparisons between pre-reform and post-reform trends, making it difficult to assess if the Orange Plan was associated with changes in location of death.
There is a growing recognition that location of death is an important quality indicator of end-of-life care [13]. Research on location of death is needed to evaluate and create evidenced-based end-of-life dementia policy. In recent years, countries worldwide increasingly adopted end-of-life care strategies in national dementia plans; however, content was varying in terms of comprehensiveness and maturity [14]. Assessing effects of the Japanese Orange Plan could inform on how to address the growing end-of-life care needs for persons with dementia. The aim of this study is to evaluate whether the Orange Plan is associated with a decrease in hospitals deaths for persons with dementia based on population-level data using an interrupted time-series analysis. We hypothesized that the Orange Plan would gradually increase proportions of death in nursing home and at home over time, as establishing the infrastructure for community-based care services was planned over a five-year period [10].
METHODS
Study design
We performed an interrupted time series analysis based on the guidelines of Bernal et al. [15] to evaluate whether the Orange plan reform was associated with changes in location of death for the total Japanese population 65 years and older that died with dementia. In an interrupted time series analysis, outcome data is taken from regularly spaced intervals and is divided by an interruption point, in this case April 1, 2013, the introduction of the Orange Plan. The robust modeling technique analyzes segmented patterns of the pre and post-reform period, which allows for controlling for secular changes that might have occurred when the reform was not implemented [15]. We structured methods and results based on the reporting recommendations for interrupted time series by Jandoc et al. (Supplementary Material) [16].
Study data
We received anonymized and publicly available, repeated cross-sectional, national aggregated data on location of death from vital statistics Japan. The data covered the entire Japanese population 65 years and older at death. We used quarterly data spanning the period January 1, 2009 to December 31, 2016. For the identification of persons with dementia, underlying cause of death was obtained from death certificates based on the International Classification of Diseases, Tenth Revision (codes: F00.0, F00.1, F00.2, F00.9, F01.0, F01.1, F01.2, F01.3, F01.8, F01.9, F02.0, F02.1, F02.2, F02.3, F02.4, F02.8, F03, G30.0, G30.1, G30.8, G30.9).
Primary outcome
The primary outcome variable was location of death based on the death certificate categorized by hospital, nursing home, home, and elsewhere (including rehabilitation centers and unknown). Death certificates did not specify hospice as a separate category. Death in hospice was included in hospital death, as in Japan the vast majority were in-hospital hospice services [17].
Table 1
Unadjusted yearly proportions of location of death (2009–2016) for persons with dementia
| Persons with dementia | |||||||||||||
| Proportion of total population | Female | Nursing Home | Female | Home | Female | Hospital | Female | Elsewhere | Female | ||||
| Years | N | (%) | (%) | (%) | (%) | (%) | (%) | (%) | (%) | (%) | (%) | ||
| 2009 | 10,214 | 1.1 | 65.9 | 19.9 | 81.6 | 12.8 | 69.6 | 57.5 | 58.1 | 9.73 | 75.4 | ||
| 2010 | 12,011 | 1.2 | 66.5 | 21.3 | 81.5 | 12.1 | 67.8 | 54.9 | 58.2 | 11.8 | 77.1 | ||
| 2011 | 14,808 | 1.4 | 66.9 | 22.8 | 80.8 | 11.4 | 69.9 | 54.1 | 58.3 | 11.8 | 76.5 | ||
| 2012 | 17,714 | 1.6 | 67.6 | 23.8 | 80.1 | 11.7 | 68.9 | 52.1 | 58.9 | 12.5 | 77.3 | ||
| 2013a | 20,494 | 1.8 | 67.9 | 25.3 | 80.8 | 11.5 | 69.3 | 51.5 | 59.3 | 11.7 | 76.9 | ||
| 2014a | 22,573 | 2.0 | 67.7 | 26.3 | 79.6 | 10.9 | 67.3 | 50.4 | 59.7 | 12.4 | 75.7 | ||
| 2015a | 24,637 | 2.1 | 67.9 | 27.1 | 79.7 | 10.5 | 68.3 | 49.5 | 59.2 | 12.8 | 76.5 | ||
| 2016a | 27,187 | 2.3 | 67.9 | 28.8 | 79.7 | 10.6 | 68.5 | 48.1 | 59.0 | 12.5 | 74.1 | ||
| Total | 149,638 | ||||||||||||
aIndicates post Orange Plan Reform.
Analysis
We performed a weighted multinomial logistic regression to calculate adjusted relative risk ratios (aRRR) and year-specific mean predicted probabilities of location of death for persons with dementia. The regression analyses were weighted to adjust for population growth over the duration of the study, and sex was included as a covariate. All variables were held at their means when calculating predicted probabilities. Death in hospital was the reference category. The multinomial logistic regression model included an interaction term between a Time variable in year quarters, and a Reform variable coded as 0 pre-reform period and 1 as post-reform period. The interaction can be interpreted as the quarterly change in relative risk of dying at a given location over time since the introduction of the reform compared to the underlying counterfactual (i.e., slope change). We adjusted for sex, and included calendar quarters as a categorical variable in the model to account for seasonality [15]. Stata version 16 was used for all analyses.
RESULTS
Descriptive analysis
Dementia was the registered underlying cause of death for 149,638 individuals during the study period. Before the Orange Plan introduction, the average proportions by location of death were hospital 54.9%, nursing home 21.7%, home 12.1%, and elsewhere 11.3%. Post-implementation, the average proportions by location of death were hospital 50.0%, nursing home 26.7%, home 10.9%, and elsewhere 12.4%. Table one presents yearly unadjusted ratios of location of death. Dementia accounted for between 1.1%and 2.3%of the yearly deaths from the total Japanese population 65 years and older, of which the majority were female.
Interrupted time series analysis
Pre-reform estimates indicated, compared to hospital deaths, a relative increase in death in nursing homes (aRRR 1.08, 95%CI 1.06–1.09, p < 0.001) and elsewhere (aRRR 1.07, 95%CI 1.05–1.10, p < 0.001) (Fig. 1 and Table 2). There was no significant pre-reform change in dying at home. After the implementation of the Orange Plan, an acceleration (increased slope) in nursing home deaths (aRRR 1.08, 95%CI 1.07–1.08, p < 0.001) and death elsewhere (aRRR 1.05, 95%CI 1.05–1.06, p < 0.001) occurred over time. There was no significant slope change for home death. Females compared to males were more likely to die in nursing home (aRRR 2.84, 95%CI 2.76–2.92, p < 0.001), home (aRRR 1.52, 95%CI 1.47–1.58, p < 0.001), and elsewhere (aRRR 2.21, 95%CI 2.13–2.30, p < 0.001) than in hospital.
Fig. 1
Quarterly predicted probabilities of location of death for persons with dementia plotted over time. From multinomial logistic regression, weighted to adjust for population growth over the study period. Grey dashed line is the implementation of the April 2013 National Dementia Orange plan.
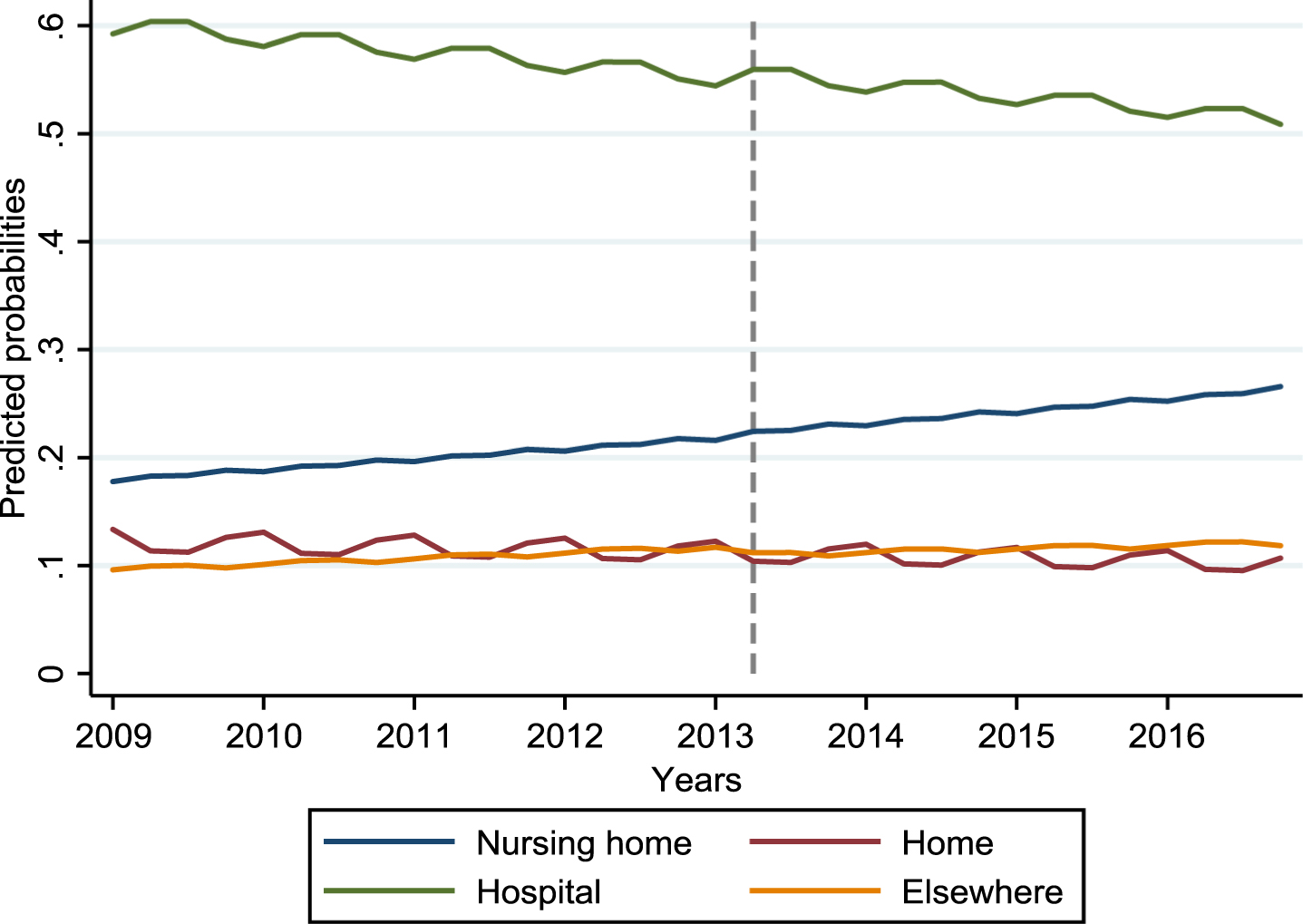
Table 2
Interrupted time series analysis adjusted Relative Risk Ratios of location of death for persons with dementia
| Persons with dementia (N = 149,638) | |||
| Nursing home | Home | Elsewhere | |
| aRRR (95%CI) p | aRRR (95%CI) p | aRRR (95%CI) p | |
| Pre-intervention trend | 1.08 (1.06–1.09) | 1.00 (0.98–1.02) | 1.07 (1.05–1.10) |
| <0.001 | 0.991 | <0.001 | |
| Slope change after | 1.08 (1.07–1.08) | 1.00 (0.99–1.00) | 1.05 (1.05–1.10) |
| Orange Plan | <0.001 | 0.765 | <0.001 |
| Females | 2.84 (2.76–2.92) | 1.52 (1.47–1.58) | 2.21 (2.13–2.30) |
| <0.001 | <0.001 | <0.001 | |
Data are year quarters, adjusted Relative Risk Ratios (aRRR) from multinomial logistic regressions with hospital death set as reference category. Models are weighted for population growth over the study period.
DISCUSSION
Key findings
This study provides evidence that the National Dementia Orange Plan is associated with a small increase in death for persons with dementia in nursing homes and elsewhere compared to hospital. We did not find a significant change over time in home deaths compared to hospital deaths. Hospital remained the primary location of death for persons with dementia.
The small increase in nursing home deaths may be related to several policies of the Orange Plan. For example, a goal of the Orange Plan to facilitate end-of-life care in small group nursing homes might have enabled more persons with dementia to reside in nursing homes until death. Previous to the Orange Plan, end-of-life care in group homes was uncommon as a national survey showed that in 2004 only 5.4%of Japanese group homes provided a form of end-of-life care [9]. Yet, Hirakawa et al. [18] found that 76.4%of the managing directors from group homes deemed it was possible under the conditions: that staff had the appropriate training, no need of medical interventions, and understanding of users and family. By accelerating the development of more health care staff providing long-term care, and facilitating end-of-life care, capacity in nursing homes to provide end-of-life care might have been expanded.
However, the Orange Plan might have been suboptimal in extending time in nursing homes until death. Japan has several types of nursing home facilities that provide care for the dementia population such as small group homes, special nursing homes, care medical facilities, and fee-based homes for older persons. All facilities have a different aim and provision of social and health care services, which complicates care coordination. Nakanishi et al. [19] found that medical deterioration is an important factor that drives care transitions in Japan, frequently resulting in hospitalization. This is disadvantageous for persons with dementia who experience increased symptom burden over time. Furthermore, specific end-of-life policies for persons with dementia such as advance care planning are lacking in Japanese nursing homes, which also increases the risk of rushed decisions in acute situations, resulting in hospitalization in the end of life [20]. Although the Orange Plan aimed to create a widespread standardized dementia care pathway, increased attention to continuity of care in long-term care may enable an increase in the number of persons with dementia dying in nursing homes [21].
Proportions of death elsewhere marginally increased over time after the Orange Plan implementation, and gradually surpassed proportions of home death in the post-reform period. Death elsewhere mainly included death in geriatric intermediate care facilities. The increase in death elsewhere could be a consequence of geriatric intermediate care facilitates serving as nursing homes for people with complex care needs who are discharged from hospital, yet, cannot find nursing home placement due to long waiting lists [22]. Persons with dementia rarely return home from geriatric intermediate care facilities [23]. Residents that were using care services at home before geriatric intermediate care facility admission were more likely to be discharged home, suggesting the need for appropriate home-based care services [24].
This study found no changes over time in proportions of dying at home. An increase in home deaths may be difficult to achieve due to the complex demanding care needs of persons with dementia in the end of life. This is consistent with the findings of Sato et al. [25] who researched the 2006 Japanese incentivization program that aimed to decrease hospitals death, and found that the shift from hospitals towards different locations of death was more prominent for nursing home residents than for older adults living in at home. In addition, Penders et al. [26] showed that nursing homes seem to be more successful than home-based care in avoiding hospitalizations at the end of life. Although home-based end-of-life care services in Japan are expected to provide care for a variation of diseases, it is primarily offered to cancer patients, which leave the demanding end-of-life care needs of community-dwelling persons with dementia unaddressed [27].
The decreasing trend in hospital death over the total study period can be mainly attributed to the increase in nursing home death. We expect that this shift in location of death also might be the result of previous health policy reforms, as since 2000 Japan has implemented a series of long-term care reforms. The most substantial reforms occurred in 2005 with the Long-Term Care Insurance Act and in 2006 the Health Care Reform Act. Both reforms were characterized by integrated measures across health and social care for all older adults at the community level, which also included changes in end-of-life policies [28, 29]. Koyama et al. [11] who studied location of death of persons with dementia in Japan over the period 1999–2016 found that the peak of hospital deaths was in 2005 and declined consistently after, while nursing home deaths steadily increased. Further research evaluating previous policy reforms on location of death could contribute to evidenced-based end-of-life policies.
Despite the decrease in hospital death, the proportion of Japanese persons with dementia dying in a hospital (48.1%) remained considerably high compared to rates of other developed countries like the Netherlands (11.6%), USA (13.2%) New Zealand (14.3%), and England (31.7%) [30, 31]. These countries appear to have adapted their health system in a way that enabled nursing home death for persons with dementia (Netherlands 69.7%, USA 62.6%, New Zealand 76.6%, England 61.7%) [30, 31]. Nakanishi [10] compared the Japanese national dementia strategy to those of other countries and found that coordination of dementia care in Japan is fragmented, compared to England were the local government personnel coordinates health- and social-care services, while in the Netherlands care is coordinated by a dementia case manager. Furthermore, unlike other countries, Japanese families are rarely involved in decision-making process for the arrangement of care services, strategies for family advocacy are lacking, and there are limited family caregiver support options such as respite care. Also, Japan has no explicit legislation on advance directives and advance care planning, which are generally well established in the Netherlands, USA, New Zealand, and England [10].
In the perspective of geographical location, South Korea has a higher proportion of hospital death (73%) for persons with dementia compared to Japan (48.1%) [30]. Like Japan, in South Korea traditionally older adults were cared for by family members at home; however, in recent years there is a high reliance on hospital care at the end of life. Despite the implementation of a long-term care insurance in 2008, that aimed to increase access to nursing homes and home care services, over time trends show that hospital and nursing home deaths increased while home deaths decreased. Suggesting increasing home deaths asks for substantial investments in home-based care services [32].
Strengths of this study include being the first study evaluating effects of national dementia Orange Plan on location of death, using longitudinal population-level data, comparing pre- and post-reform trends. However, several limitations remain. We depended on the death certificate data to identify persons with dementia making these results a conservative underestimate, as the Japanese prevalence of Alzheimer’s and related dementia aged 65 years and older is estimated to be 11.3%[3]. Furthermore, information on changes in location shortly before death is not included in death certificate data. Lastly, there may be other sociodemographic and health factors that are associated to location of death; however, those data were not available. Fortunately, the use of interrupted time series analysis is as stated by Bernal et al. [15] “is usually robust against typical confounding variables like population age distribution or socioeconomic status because they change slowly over time and are normally accounted for when modelling the underlying long-term trend”.
Nakanishi et al. [12] showed that the absolute number of Japanese dementia deaths in hospital, nursing home, and intermediate geriatric care facilities increased consistently over the period 1996 to 2016, mainly due to the steep increase in the total dementia deaths over time. Even though the National Dementia Orange Plan aimed to invest in the care capacity of long-term care facilities, and stimulated end-of-life care in community settings, it might have been insufficient to cope with the care demand of the rising number of persons with dementia. The Orange Plan was characterized by policies enabling persons with dementia to maximize their time in the community. However, the reform included few end-of-life strategies. Results of this study show that the Orange Plan had a modest effect on location of death in persons with dementia, as proportions of hospital death slightly decreased, moving towards death in nursing home and elsewhere, while proportions of home death remained relatively unchanged. This may imply that end-of-life strategies in national dementia policy must be expanded to extend time in the community until death. Policy makers should consider addressing coordination of care between home, social and health care services, as end-of-life care for persons with dementia requires an integrated approach with continuity of care across settings. Establishing strong home-based end-of-life services integrated in dementia care might help family caregivers to extend the time at home of their loved ones. In addition, including family in the decision-making process of arranging care, providing advocacy services, and family support such as respite care seem important to increase aging in the community. Furthermore, nursing homes should institute strategies such as advance care planning to minimize hospitalizations at the end of life. Further work is required to create a better understanding of persons with dementia, care provider, and system related factors for successful community-based end-of-life care.
ACKNOWLEDGMENTS
This study is funded by the Netherlands Organization for Health Research and Development (NWO-ZonMw Veni, 091.619.060).
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-0521r1).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-210521.
REFERENCES
[1] | Japan Vital Statistics, Population Estimates by Age (Five-Year Groups) and Sex, https://www.e-stat.go.jp/en/stat-search/file-download?statInfId=000032054870&fileKind=4, Accessed December 20, 2020. |
[2] | Worldbank, Population ages 65 and above, Japan, https://data.worldbank.org/indicator/SP.POP.65UP.TO.ZS?locations=JP, Accessed 20 December, 2020. |
[3] | Dodge H , Buracchio T , Fisher G , Kiyohara Y , Meguro K , Tanizaki Y , Kaye J ((2012) ) Trends in the prevalence of dementia in Japan. Int J Alzheimers Dis 2012: , 956354. |
[4] | Broad JB , Gott M , Kim H , Boyd M , Chen H , Connolly MJ ((2013) ) Where do people die? An international comparison of the percentage of deaths occurring in hospital and residential aged care settings in 45 populations, using published and available statistics. Int J Public Health 58: , 257–267. |
[5] | Rao A , Suliman A , Vuik S , Aylin P , Darzi A ((2016) ) Outcomes of dementia: Systematic review and meta-analysis of hospital administrative database studies. Arch Gerontol Geriatr 66: , 198–204. |
[6] | Nakanishi M , Nakashima T , Shindo Y , Niimura J , Nishida A ((2016) ) Japanese care location and medical procedures for people with dementia in the last month of life. J Alzheimers Dis 51: , 747–755. |
[7] | Birch D , Draper J ((2008) ) A critical literature review exploring the challenges of delivering effective palliative care to older people with dementia. J Clin Nurs 17: , 1144–1163. |
[8] | Sampson EL ((2010) ) Palliative care for people with dementia. Br Med Bull 96: , 159–174. |
[9] | Nakanishi M , Honda T ((2009) ) Processes of decision making and end-of-life care for patients with dementia in group homes in Japan. Arch Gerontol Geriatr 48: , 296–299. |
[10] | Nakanishi M , Nakashima T ((2014) ) Features of the Japanese national dementia strategy in comparison with international dementia policies: How should a national dementia policy interact with the public health- and social-care systems? Alzheimers Dement 10: , 468–476 e463. |
[11] | Koyama T , Sasaki M , Hagiya H , Zamami Y , Funahashi T , Ohshima A , Tatebe Y , Mikami N , Shinomiya K , Kitamura Y , Sendo T , Hinotsu S , Kano MR ((2019) ) Place of death trends among patients with dementia in Japan: A population-based observational study. Sci Rep 9: , 20235. |
[12] | Nakanishi M , Yamasaki S , Nishida A ((2018) ) In-hospital dementia-related deaths following implementation of the national dementia plan: Observational study of national death certificates from 1996 to 2016. BMJ Open 8: , e023172. |
[13] | Paddy M ((2011) ) Influence of location on a good death. Nurs Stand 26: , 33–36. |
[14] | Nakanishi M , van der Steen JT ((2020) ) National dementia plans to address escalating global palliative care needs. Palliat Med 34: , 966–967. |
[15] | Bernal JL , Cummins S , Gasparrini A ((2017) ) Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int J Epidemiol 46: , 348–355. |
[16] | Jandoc R , Burden AM , Mamdani M , Lévesque LE , Cadarette SM ((2015) ) Interrupted time series analysis in drug utilization research is increasing: Systematic review and recommendations. J Clin Epidemiol 68: , 950–956. |
[17] | Lee CY , Komatsu H , Zhang W , Chao YF , Kim KK , Kim GS , Cho YH , Ko JS ((2010) ) Comparison of the hospice systems in the United States, Japan and taiwan. Asian Nurs Res (Korean Soc Nurs Sci) 4: , 163–173. |
[18] | Hirakawa Y , Masuda Y , Uemura K , Kuzuya M , Kimata T , Iguchi A ((2006) ) End-of-life care at group homes for patients with dementia in Japan. Findings from an analysis of policy-related differences. Arch Gerontol Geriatr 42: , 233–245. |
[19] | Nakanishi M , Hattori K , Nakashima T , Sawamura K ((2014) ) Health care and personal care needs among residents in nursing homes, group homes, and congregate housing in Japan: Why does transition occur, and where can the frail elderly establish a permanent residence? J Am Med Dir Assoc 15: , 76 e71–76. |
[20] | Ikegami N , Ikezaki S ((2012) ) Japan’s policy of promoting end-of-life care in nursing homes: Impact on facility and resident characteristics associated with the site of death. Health Policy 105: , 303–311. |
[21] | Gozalo P , Teno JM , Mitchell SL , Skinner J , Bynum J , Tyler D , Mor V ((2011) ) End-of-life transitions among nursing home residents with cognitive issues. N Engl J Med 365: , 1212–1221. |
[22] | Ministry of Health Labor and Welfare, Number of persons on waiting list for nursing home placement, by long-term care insurance care level, type of current place, https://www.mhlw.go.jp/file/04-Houdouhappyou-12304250-Roukenkyoku-Koureishashienka/0000041929.pdf, Accessed January 5 2020. |
[23] | Nakanishi M , Shindo Y , Niimura J ((2016) ) Discharge destination of dementia patients who undergo intermediate care at a facility. J Am Med Dir Assoc 17: , 92 e91–97. |
[24] | Morita K , Ono S , Ishimaru M , Matsui H , Naruse T , Yasunaga H ((2018) ) Factors affecting discharge to home of geriatric intermediate care facility residents in Japan. J Am Geriatr Soc 66: , 728–734. |
[25] | Sato M , Tamiya N , Jin X , Watanabe T , Takahashi H , Noguchi H ((2021) ) Impact of a Japanese incentivization program to increase end-of-life care outside of hospitals. J Am Med Dir Assoc 22: , 329–333. |
[26] | Penders YW , Albers G , Deliens L , Vander Stichele R , Van den Block L , Euro I ((2015) ) Awareness of dementia by family carers of nursing home residents dying with dementia: A post-death study. Palliat Med 29: , 38–47. |
[27] | Nakanishi M , Niimura J , Nishida A ((2017) ) Factors associated with end-of-life by home-visit nursing-care providers in Japan. Geriatr Gerontol Int 17: , 991–998. |
[28] | WHO (2018) Asia Pacific Observatory on Health Systems and Policy, Health Systems in Transition 155-164. |
[29] | Tsutsui T ((2014) ) Implementation process and challenges for the community-based integrated care system in Japan. Int J Integr Care 14: , e002. |
[30] | Reyniers T , Deliens L , Pasman HR , Morin L , Addington-Hall J , Frova L , Cardenas-Turanzas M , Onwuteaka-Philipsen B , Naylor W , Ruiz-Ramos M , Wilson DM , Loucka M , Csikos A , Rhee YJ , Teno J , Cohen J , Houttekier D ((2015) ) International variation in place of death of older people who died from dementia in 14 European and non-European countries. J Am Med Dir Assoc 16: , 165–171. |
[31] | Joling KJ , Janssen O , Francke AL , Verheij RA , Lissenberg-Witte BI , Visser PJ , van Hout HPJ ((2020) ) Time from diagnosis to institutionalization and death in people with dementia. Alzheimers Dement 16: , 662–671. |
[32] | Lee JK , Jang SN ((2018) ) Place of death and associated gender difference in Korea 2006–2014: Evidence from exit interviews of the Korean Longitudinal Study of Ageing. Arch Gerontol Geriatr 78: , 196–202. |


