
Pain and Associated Neuropsychiatric Symptoms in Patients Suffering from Dementia: Challenges at Different Levels and Proposal of a Conceptual Framework
Abstract
Old age is critically associated with multi-morbidity, chronic pain, and high risk for dementia. Recognizing and treating pain is very much dependent on language comprehension and production. Both may be impaired in dementia. Moreover, neuropsychiatric symptoms may interact with pain perception. The main aims of the present article were 1) to identify key areas for future research to elucidate the relation between pain and associated neuropsychiatric symptoms in dementia, and 2) to provide a conceptual framework for ameliorating the clinical process of recognizing, assessing, and managing pain in non-communicating patients with advanced dementia.
INTRODUCTION
The elderly frequently suffer from multi-morbidity. Thus, it is not surprising that 20–50%of elderly (and up to 80%of nursing home residents) report chronic pain [1,2]. As old age also is an important risk factor to develop dementia, chronic pain should also affect patients diagnosed with dementia [1]. Dementia is a degenerative disease characterized, among others, by decreasing cognitive abilities and increasing communication difficulties [3]. In advanced dementia, clinical recognition of patients’ pain may be flawed by difficulties to report pain verbally. Thus, chronic pain is underdiagnosed in advanced dementia (reviewed in [4–6]). However, when unrecognized, patients’ pain may neither be assessed nor treated adequately. This is reflected by accumulating evidence indicating that—compared with matched controls—nursing home residents suffering from dementia are prescribed less, and thus receive less, pain medication [7].
Here, we review clinical manifestations of experienced pain and associated neuropsychiatric symptoms in patients with dementia (Fig. 1A) and delineate the complex interplay between pain, dementia, and associated neuropsychiatric symptoms at different levels of involvement (Fig. 1B). Finally, we propose a conceptual framework for ameliorating diagnostic and treatment approaches related to pain and associated neuropsychiatric symptoms in non-communicating patients with dementia (Fig. 2).
Fig. 1
A) Schematic representation of the clinical manifestations of pain in dementia. B) An integrative perspective of pain in dementia, focusing on potential risk factors and heterogeneity (inner-most rectangle), different levels of involvement (middle rectangle), and manifestations (outer rectangle). Please note that in each patient (and depending on dementia progression, responsiveness to treatment, etc.), all or some of these factors may be intertwined, thus yielding a unique clinical picture that may change over time and with dementia progression.
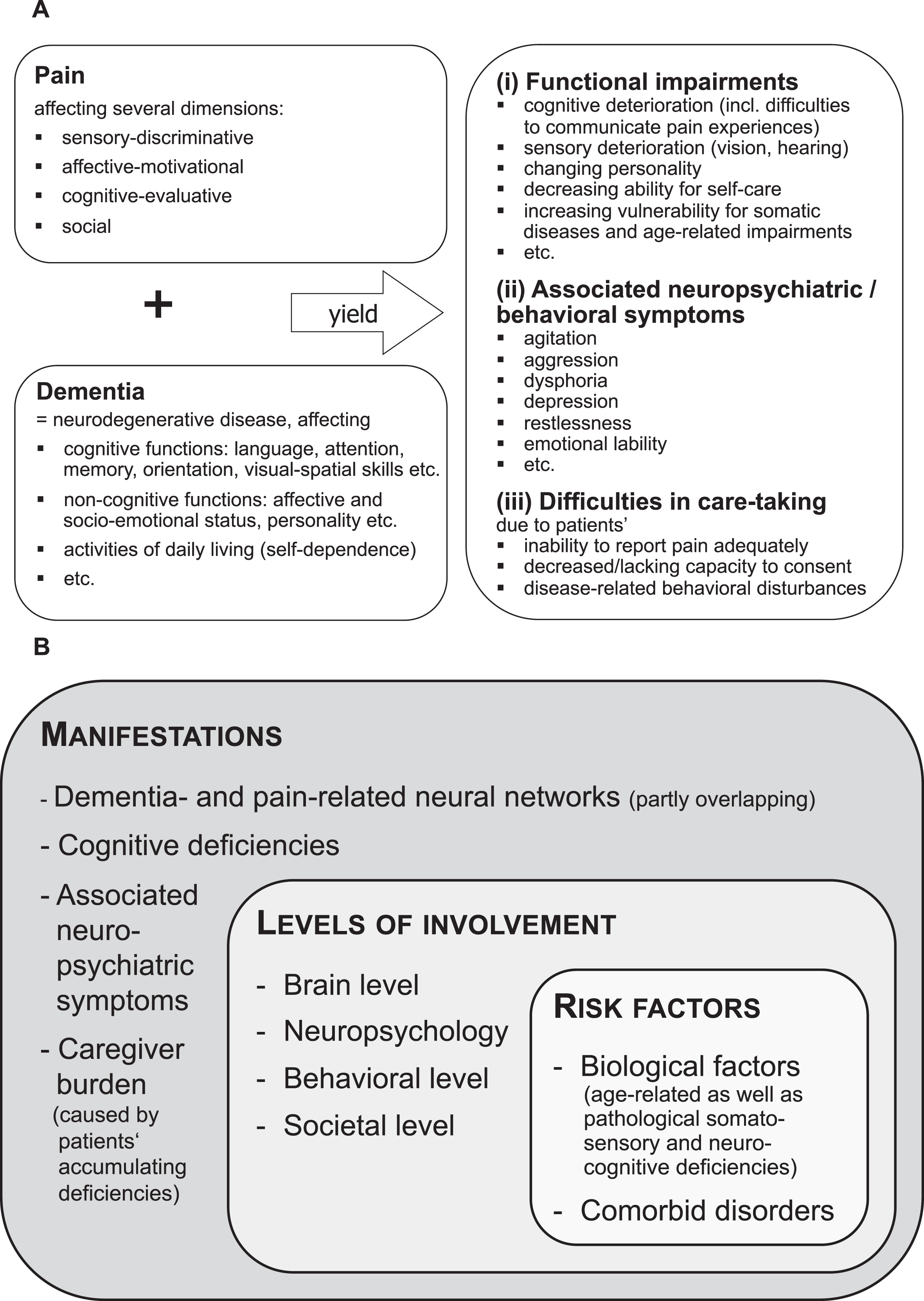
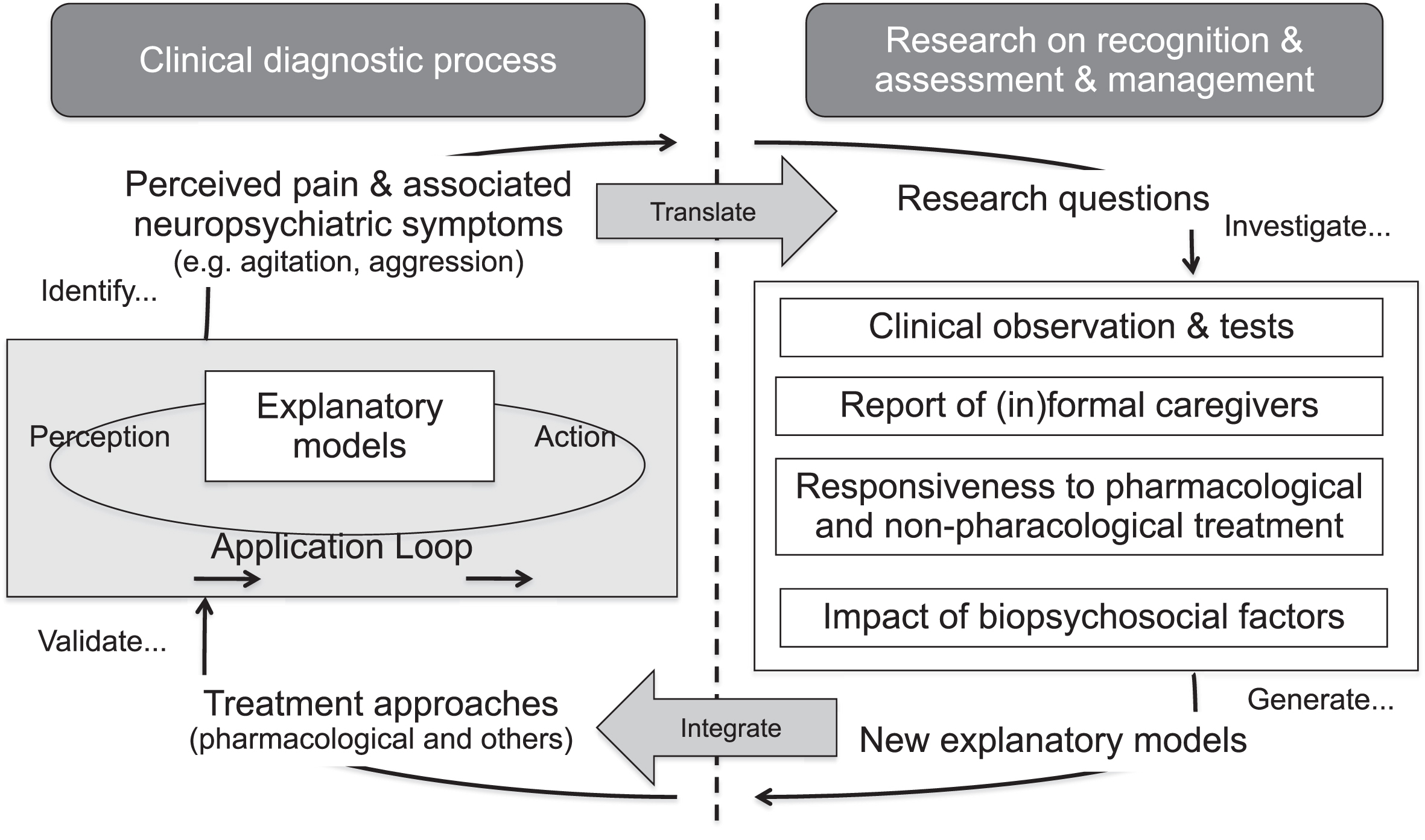
Fig. 2
Conceptual framework for an adaptation loop targeted at ameliorating the clinical process of recognizing, assessing, and managing pain and associated neuropsychiatric symptoms in non-communicating patients with advanced dementia. In our case, relevant research questions that need to be evaluated empirically are, among others, which pain assessment tools are reliable in dementia, which treatment approaches are effective in terms of pain management, and which are likely to also alleviate pain-related neuropsychiatric symptoms, which factors are apt to impact upon pain perception and responsiveness to treatment, etc.
CLINICAL MANIFESTATIONS OF PAIN AND ASSOCIATED NEUROPSYCHIATRIC SYMPTOMS IN DEMENTIA
There is accumulating evidence that in non-communicating patients with advanced dementia observable neuropsychiatric symptoms (e.g., depression, agitation, restlessness, writhing, vocalizations, etc.) should not only be considered as ‘pure’ psychiatric sequelae of neurodegeneration, but as manifestations of unrecognized pain [2, 5, 6]. Untreated pain in patients with dementia is relevant not only at the individual, but also at the societal level because, beyond increasing treatment efforts [6, 7], chronic pain further increases psychiatric vulnerability of affected patients [2, 6], thus aggravating burden on caregivers and health care services (Fig. 1A). Furthermore, recent evidence indicated that, independent of dementia severity, activities of daily living (ADL) functioning declined with increasing pain scores in nursing home residents with dementia [8]. These findings substantiate a direct association between enhanced burden experienced by caregivers and patients’ (unrecognized) chronic pain that may evoke or exacerbate neuropsychiatric symptoms and may thus yield faster decline of ADL functioning.
Clinical manifestations of pain and neuropsychiatric symptoms in dementia are manifold (Fig. 1A) and characterized by considerable inter- and intraindividual heterogeneity regarding etiology, diagnosis, treatment, trajectories, prognosis, societal implications, etc. [4, 7]. Next, we argue that pain needs to be viewed from an integrative perspective to understand the complex relationship between pain and associated neuropsychiatric symptoms in dementia (Fig. 1B) before we discuss potential avenues for future research to elucidate the association between pain and neuropsychiatric symptoms in dementia.
AN INTEGRATIVE PERSPECTIVE OF PAIN
Pain and its manifestations
Understanding of the nature of and the interplay between pain and its behavioral and neurofunctional ramifications is still patchy [4–6]. Importantly, pain is a multi-faceted phenomenon [4, 9]. Recently, four neurofunctional pain networks have been identified: 1) a sensory/discriminative lateral pain pathway (posterior insula, primary and secondary somatosensory cortex), 2) an affective/motivational medial pain pathway (anterior cingulate cortex, dorsolateral prefrontal cortex, anterior insula), 3) a descending modulatory system supporting the cognitive-evaluative dimension of pain (amygdala, hypothalamus, periaqueductal gray), and 4) involvement of the default mode network (hippocampus, cuneus, posterior cingulate cortex) [10]. These pain-related networks work together in sensory recognition, cognitive evaluation, and response (behavior) selection. Furthermore, chronic pain may hasten neurodegeneration in Alzheimer’s disease (AD) through a combination of locus coeruleus dysfunction and neuroinflammation [11].
Importantly, dementia-related brain pathologies partly overlap with cerebral signatures of pain [10–14] and thus, may modulate pain perception itself by affecting one or more aforementioned pain networks. However, the literature is inconsistent as to whether individuals with AD display increased, diminished, or normal pain thresholds (reviewed in [14]). Inconsistent findings across studies are not surprising considering confounds between individual pain thresholds and pain tolerance as well as methodological differences making direct comparisons across studies difficult, if not impossible. Nonetheless, recent findings indicated differential pain thresholds depending on pain severity (i.e., higher thresholds in response to mild, but similar thresholds to moderate pain [10]) and dementia type (i.e., lower thresholds in AD and vascular dementia, but higher thresholds in frontotemporal dementia [15]).
Likewise, dementia severity seems to modulate pain perception (i.e., patients with advanced AD perceiving less pain compared to those with mild AD [6]). Interestingly, higher pain thresholds were accompanied by stronger neural activity in patients with AD [12] and increased functional connectivity in brain regions supporting sensory and affective pain processing ([13], but see [10]). Moreover, pain-related increases of resting-state functional connectivity in dementia might reflect compensatory mechanisms [10, 13]. In particular, anterior cingulate cortex seems to modulate the processing of affective-motivational pain dimensions, whereas dorsolateral prefrontal cortex supports pain-related cognitive evaluation and response selection (reviewed in [10]).
In summary, pain networks partly overlap with dementia-related brain pathologies, thus altering sensory, affective, and cognitive dimensions of patients’ pain experiences. As depicted in Fig. 1B, various dimensions of pain are intertwined and manifest at different levels in patients with dementia, thus forming an intricate network of interactions affecting neurobehavioral and psychosocial aspects of pain.
Diagnosing pain in patients with advanced dementia
Considering the wide range of available pain assessments (differing, among others, regarding conceptual background, presentation/answer format, and psychometric properties), it seems rather challenging to choose the appropriate measure for a specific patient (see [16–19] for comprehensive and critical discussions of pain assessment tools). In early dementia (when patients’ conversation skills are still preserved), subjective reports of perceived pain may be sufficient [20]. In advanced dementia (when patients are unable to report pain), observational tools seem more appropriate to assess pain [4, 7, 20]. However, patients’ self-reports and external observations do not always match [2, 5–7, 14].
In 2002, the American Geriatric Society (AGS) set up guidelines for the management of persistent pain in elderly and identified six common pain behaviors that should be assessed in patients with dementia: 1) facial expressions, 2) verbalizations/vocalizations, 3) body movements, 4) changes in interpersonal interactions, 5) changes in activity patterns or routines, 6) mental status changes [21]. Nonetheless, existing observational pain assessments for dementia are quite heterogeneous regarding adherence to the AGS guidelines and were reported to have other methodological shortcomings [16–19].
Recently, the evaluation of facial expressions received increasing scientific interest as a potentially objective pain measure [22], resulting in the electronic Pain Assessment Tool (ePAT) integrating automated facial recognition technology with observational methods of pain-related behaviors [23]. Although the ePAT is reported to have good psychometric properties, it is not in clinical use yet.
To date, the most promising and empirically best validated pain assessment in advanced dementia seems to be the recently developed Pain Assessment in Impaired Cognition (PAIC15) [24]. The PAIC15 resulted from an international cooperation to develop a meta-tool comprising the best items (regarding psychometric properties) of existing observational pain scales for dementia [25] (the Supplementary Material provides a description of the 12 eligible assessment tools). Overall, the PAIC15 includes 15 items on facial expression as well as body movement and vocalization with good psychometric properties [26]. To summarize, the most reliable clinical approach to recognize and assess pain in advanced dementia seems a combination of systematic clinical observations and caregiver reports [21, 24–26].
Heterogeneity, trajectories, and treatment of pain in dementia
Acknowledging the above-mentioned considerable heterogeneity of clinical manifestations of pain and related neuropsychiatric symptoms in patients with dementia, it comes to no surprise that—at an individual level—also the trajectories of chronic pain (and its ramifications) are manifold and only partly explained by treatment effects [5–7]. Though chronic pain was found to correlate with cognitive decline, little is known about the nature and potential mechanisms underlying the repeatedly reported relation between chronic pain and dementia-associated neuropathology [4, 16]. Recent findings suggest that chronic pain, beyond being associated with accelerated memory decline [26] may also trigger a hastened course of dementia-related pathogenesis [11].
There is accumulating evidence that treating pain in patients with AD also reduces associated neuropsychiatric symptoms such as agitation and aggression, among others (reviewed in [6]). Thus, it seems plausible to assume that 1) neuropsychiatric symptoms of patients with chronic pain might be a direct sequela of unrecognized pain, and thus 2) pain relief may have an (indirect) positive effect on pain-related neuropsychiatric symptoms. According to a systematic review of pain treatment in dementia, paracetamol, opioids, and nonsteroidal anti-inflammatory drugs (NSAIDs) are the most frequently prescribed analgesics [7]. However, prescriptions declined recently because NSAID intake was found to increase the risk for gastrointestinal bleeding, renal dysfunction, and cardiovascular events in elderly (especially those with cognitive impairments and vascular dementia). Instead, opioids such as fentanyl and buprenorphine are more frequently prescribed for patients with dementia (despite lacking empirical evidence regarding safety and effectiveness [7, 28]).
Though findings on non-pharmacological psychosocial interventions were mixed [7], listening to music was found to significantly reduce pain scores of affected patients (as rated by informal caregivers [29]). Furthermore, non-pharmacological interventions reported to have beneficial effects on early AD (and AD pathogenesis) include specific diets and nutrient supplements [30–32]. However, systematic evaluations of nutraceuticals were mostly targeted at the neurocognitive rather than the pain dimensions of AD.
To date, there is neither a consensus nor a best-practice approach on how to treat chronic pain and associated neuropsychiatric symptomatology in patients with dementia [6,7]. Instead, clinicians are required to base their therapeutic decisions on a multi-dimensional approach tailored at both patient-specific characteristics and information provided by caregivers [7] (Fig. 1A).
TENTATIVE RESEARCH CRITERIA UPON WHICH TO TEST AND VALIDATE EXPLANATORY MODELS
As outlined above, the interplay between chronic pain and associated neuropsychiatric symptoms is complex and only poorly understood so far. Recently, it was suggested that at an individual level, the complex interplay of pain, aging and dementia is modulated by predispositions as well as lifelong and current biopsychosocial factors [4]. However, research focusing on the social dimensions of pain in dementia is sparse. Thus, the biopsychosocial model seems a promising framework that awaits further empirical evidence.
In the following, we propose a conceptual framework illustrating how to translate clinical issues to relevant research questions. As depicted in Fig. 2 (right side), relevant research questions need to be addressed empirically to generate new explanatory models (that are apt to increase our understanding of the complex interplay between pain, dementia and associated neuropsychiatric symptoms). Consequently, these new explanatory models might help to develop alternative diagnostic and treatment approaches which in turn need to be validated. Finally (Fig. 2, left side), findings of the latter validation should be fed into a so-called application loop targeted at evaluating and, if needed, modifying previous explanatory models. Ideally, an empirically validated and adapted explanatory model can be used as a clinical guide to reliably identify perceived pain and associated neuropsychiatric symptoms in non-communicating patients with dementia (Fig. 2).
DISCUSSION
Though the recently developed PAIC15 [24] seems a promising tool that overcomes many of the methodological shortcomings of existing pain assessment instruments, it remains open whether it might become widely accepted as a kind of golden diagnostic standard. To date, in absence of a best-practice guide, recognition, assessment, and treatment of chronic pain in non-communicating patients with dementia is still a challenge. Accordingly, chronic pain often remains underdiagnosed in this population. This may foster the development of pain-related neuropsychiatric symptoms such as agitation and aggression, which pose additional burden to patients’ caregivers. In the future, automated pain recognition—based on facial expressions or body postures—may become a valuable diagnostic tool to differentiate pain-related physiological and behavioral responses. Synthesizing latest evidence, we propose a conceptual framework targeted at integrating relevant research into clinical practice (Fig. 2) to ameliorate clinical evaluation and management of chronic pain in non-communicating patients with dementia. Our framework describes an adaptation loop considering clinical issues and research findings to generate new explanatory models of the intricate, and to date poorly understood, interactions of pain, associated neuropsychiatric symptoms and dementia.
ACKNOWLEDGMENTS
The authors did not receive funding for this work.
Authors’ disclosures are available online (https://www.j-alz.com/manuscript-disclosures/21-0263r2).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-210263.
REFERENCES
[1] | Apinis C , Tousignant M , Arcand M , Tousignant-Laflamme Y ((2014) ) Can adding a standardized observational tool to interdisciplinary evaluation enhance the detection of pain in older adults with cognitive impairments? Pain Med 15: , 32–41. |
[2] | Malara A , De Biase GA , Bettarini F , Ceravolo F , Di Cello S , Garo M , Praino F , Settembrini V , Sgró G , Spadea F , Rispoli V ((2016) ) Pain assessment in elderly with behavioral and psychological symptoms of dementia. J Alzheimers Dis 50: , 1217–1225. |
[3] | American Psychiatric Association ((2013) ) Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. American Psychiatric Association, Arlington, VA. |
[4] | Gagliese L , Gauthier LR , Narain N , Freedman T ((2018) ) Pain, aging and dementia: Towards a biopsychosocial model. Prog Neuropsychopharmacol Biol Psychiatry 87: (Pt B), 207–213. |
[5] | Husebo BS , Achterberg W , Flo E ((2016) ) Identifying and managing pain in people with Alzheimer’s disease and other types of dementia: A systematic review. CNS Drugs 30: , 481–497. |
[6] | Pergolizzi JV , Raffa RB , Paladini A , Varrasi G , LeQuang JA ((2019) ) Treating pain in patients with dementia and the possible concomitant relief of symptoms of agitation. Pain Manag 9: , 569–582. |
[7] | Bullock L , Bedson J , Jordan JL , Bartlam B , Chew-Graham CA , Campbell P ((2019) ) Pain assessment and pain treatment for community-dwelling people with dementia: A systematic review and narrative synthesis. Int J Geriatr Psychiatry 34: , 807–831. |
[8] | van Dalen-Kok AH , Pieper MJC , deWaal MWM , van der Steen JT , Scherder EJA , Achterberg WP ((2020) ) The impact of pain on the course of ADL functioning in patients with dementia. Age Ageing 50: , 906–913. |
[9] | Melzack R , Casey K ((1986) ) Sensory, motivational and central control determinants of pain. In The Skin Senses, Kenshado D, Thomas CC, eds. Thomas, Springfield, IL, 423–443. |
[10] | Monroe TB , Beach PA , Bruehl SP , Dietrich MS , Rogers PB , Gore JC , Atalla SW , Cowan RL ((2017) ) The impact of Alzheimer’s disease on resting state functional connectivity of brain regions modulating pain: A cross sectional study. J Alzheimers Dis 57: , 71–83. |
[11] | Cao S , Fisher DW , Yu T , Dong H ((2019) ) The link between chronic pain and Alzheimer’s disease. J Neuroinflammation 16: , 204. |
[12] | Cole LJ , Farrell MJ , Duff EP , Barber JB , Egan GF , Gibson SJ ((2006) ) Pain sensitivity and fMRI pain-related brain activity in Alzheimer’s disease. Brain 129: , 2957–2965. |
[13] | Cole LJ , Gavrilescu M , Johnston LA , Gibson SJ , Farrell MJ , Egan GF ((2011) ) The impact of Alzheimer’s disease on the functional connectivity between brain regions underlying pain perception. Eur J Pain 15: , 568. |
[14] | Monroe TB , Gore JC , Min Chen L , Mion LC , Cowan RL ((2012) ) Pain in people with Alzheimer disease: Potential applications for psychophysical and neurophysiological research. J Geriatr Psychiatry Neurol 25: , 240–255. |
[15] | Bathgate D , Snowden JS , Varma A , Blackshaw A , Neary D ((2001) ) Behaviour in frontotemporal dementia, Alzheimer’s disease and vascular dementia.. Acta Neurol Scand 103: , 367–378. |
[16] | Corbett A , Husebo B , Malcangio M , Staniland A , Cohen-Mansfield J , Aarsland D , Ballard C ((2012) ) Assessment and treatment of pain in people with dementia. Nat Rev Neurol 8: , 264–274. |
[17] | Lichtner V , Dowding D , Esterhuizen P , Closs SJ , Long AF , Corbett A , Briggs M ((2014) ) Pain assessment for people with dementia: A systematic review of systematic reviews of pain assessment tools. BMC Geriatr 14: , 138. |
[18] | Zwakhalen S , Hamers J , Huijer Abu-Saad H , Berger M ((2006) ) Pain in elderly people with severe dementia: A systematic review of behavioral pain assessment tools. BMC Geriatrics 6: , 3. |
[19] | Zwakhalen S , Docking RE , Gnass I , Sirsch E , Stewart C , Allcock N , Schofield P ((2018) ) Pain in older adults with dementia. A survey across Europe on current practices, use of assessment tools, guidelines and policies. Schmerz 32: , 364–373. |
[20] | Lukas A , Schuler M , Fischer TW , Gibson SJ , Savvas SM , Nikolaus T , Denkinger M ((2012) ) Pain and dementia: A diagnostic challenge. Z Gerontol Geriatr 45: , 45–49. |
[21] | American Geriatrics Society (AGS) Panel on Persistent Pain in Older Persons ((2002) ) The management of persistent pain in older persons. J Am Geriatr Soc 50: , S205–S224. |
[22] | Kunz M , Meixner D , Lautenbacher S ((2019) ) Facial muscle movements encoding pain –a systematic review. Pain 160: , 535–549. |
[23] | Atee M , Hoti K , Parsons R , Hughes JD ((2017) ) Pain assessment in dementia: Evaluation of a point-to-care technological solution. J Alzheimers Dis 60: , 137–150. |
[24] | Kunz M , de Waal MWM , Achterberg WP , Gimenez-Llort L , Lobbezoo F , Sampson EL , van Dalen-Kok AH , Defrin R , Invitto S , Konstantinovic L , Oosterman J , Petrini L , van der Stehen JT , Strand L-I , de Tommaso M , Zwakhalen S , Husebo B , Lauterbach S ((2020) ) The Pain Assessment in Impaired Cognition scale (PAIC15): A multidisciplinary and international approach to develop and test a meta-tool for pain assessment in impaired cognition, especially dementia. Eur J Pain 24: , 192–208. |
[25] | Corbett A , Achterberg W , Husebo B , Lobbezzo F , de Vet H , Kunz M , Strand L , Constantinou M , Tudose C , Kappesser J , de Waal M , Lautenbacher S , on behalf of the EUCOST action td 1005 Pain Assessment in Patients with Impaired Cognition, especially Dementia Collaborators: http://www.cost-td1005.net/ ((2014) ) An international road map to improve pain assessment in people with impaired cognition: The development of the Pain Assessment in Impaired Cognition (PAIC) meta-tool. BMC Neurol 14: , 229. |
[26] | deWaal MWM , van Dalen-Kok AH , de Vet HC , Gimenez-Llort L , Konstantinovic L , de Tommaso M , Fischer T , Lukas A , Kunz M , Lautenbacher S , Lobbezoo F , McGuire B , van der Stehen J , Achterberg WP ((2020) ) Observational pain assessment in older persons with dementia in four countries: Observer agreement of items and factor structure of the Pain Assessment in Impaired Cognition. Eur J Pain 24: , 279–296. |
[27] | Whitlock EL , Diaz-Ramirez GL , Glymour MM , Boscardin JW , Covinsky KE , Smith AK ((2017) ) Association between persistent pain and memory decline and dementia in a longitudinal cohort of elders. JAMA Int Med 177: , 1146–1153. |
[28] | Jensen-Dahm C , Christensen AN , Gasse C , Waldemar G ((2020) ) The use of opioids and antipsychotics in elderly with dementia –Have opioids replaced antipsychotics in treating behavioral symptoms in dementia? J Alzheimers Dis 73: , 259–267. |
[29] | Park H ((2010) ) Effect of music on pain for home-dwelling persons with dementia. Pain Manag Nurs 11: , 141–147. |
[30] | Cummings J , Passmore P , McGuinness B , Mok V , Chen C , Engelborghs S , Woodward M , Manzano S , Garcia-Ribas G , Cappa S , Bertolucci P , Chi L-W ((2019) ) Souvenaid in the management of mild cognitive impairment: An expert consensus opinion. Alzheimers Res Ther 11: , 73. |
[31] | Livingston G , Sommerlad A , Orgeta V , Costfreda SG , Huntley J , Ames D , Ballard C , Banerjee S , Burns A , Cohen-Mansfield J , Cooper C , Fox N , Gitlin LN , Howard R , Kales HC , Larson EB , Ritchie K , Rockwood K , Sampson EI , Samus Q , Schneider LS , Selbaek G , Teri L , Mukadam N ((2017) ) Dementia prevention, intervention, and care. Lancet 390: , 2673–2734. |
[32] | Veurink G , Perry G , Singh SK ((2020) ) Role of antioxidants and a nutrient rich diet in Alzheimer’s disease. Open Biol 10: , 200084. |

