
Sex Difference in the Relation Between Marital Status and Dementia Risk in Two Population-Based Cohorts
Abstract
Background:
The modifying effect of sex on the relation between marital status and dementia has yet to be determined.
Objective:
To examine if sex modifies the association between marital status and incident dementia.
Methods:
Population-based samples from the Mayo Clinic Study of Aging (MCSA, N = 3,471) and the Gothenburg H70 Birth Cohort Study (H70-study, N = 913) were used. A multiplicative interaction term was used to analyze the modifying effect of sex on the relation between marital status (married versus not married) and incident dementia using Cox regression models. Further, risk of dementia by marital status was also evaluated in models separated by sex.
Results:
In the MCSA, there was an interaction between marital status and sex in relation to dementia (p = 0.015). In contrast, in the H70-study, no significant interaction was observed (p = 0.28). Nevertheless, in both studies, not married men had increased risk of dementia compared to married men in models adjusted for age, education, and number of children (H70-study: 1.99; 1.06–3.76, MCSA: 1.43; 1.08–1.89). Associations remained similar after additional adjustment for depression, BMI, hypertension, dyslipidemia, and diabetes mellitus (H70-study: 2.00; 1.05–3.82, MCSA: 1.32; 0.99–1.76). Further, no significant association was observed between marital status and dementia in women (H70-study: 1.24; 0.82–1.89, MCSA: 0.82; 0.64–1.04).
Conclusion:
Sex had a modifying effect on the association between marital status and incident dementia. In analyses separated by sex, not married men had an increased risk of dementia compared to married men, while no significant association was observed between marital status and risk of dementia in women.
INTRODUCTION
With an expected increase in people with dementia, identifying risk factors for dementia has never been more important. Several longitudinal studies report that being married or living with a spouse reduces the risk of cognitive decline [1], all-cause dementia [2–9], and Alzheimer’s disease (AD) [10, 11], but one study did not confirm these findings [12]. Evidence also suggests that marital status effects health differently depending on sex. One study reported a higher risk of hypertension and death in men who had never been married compared to married men, while this was not observed in women [13]. Another study found an increased risk of depression in men compared to women who became widowed [14]. However, few studies have examined the moderating role of sex on the association between marital status and dementia risk [6, 8]. A study from the Health and Retirement Study (HRS) found higher odds of dementia among divorced/separated and widowed men compared to women [6].
We aimed to fill this knowledge gap by studying the modifying effect of sex on the relation between marital status and incident dementia in two population-based samples from Rochester, Minnesota (MN), USA and Gothenburg, Sweden. The analyses were performed separately in each sample to examine if the associations could be replicated.
METHODS
Mayo clinic study of aging, 70+ years old (MCSA 70+ study)
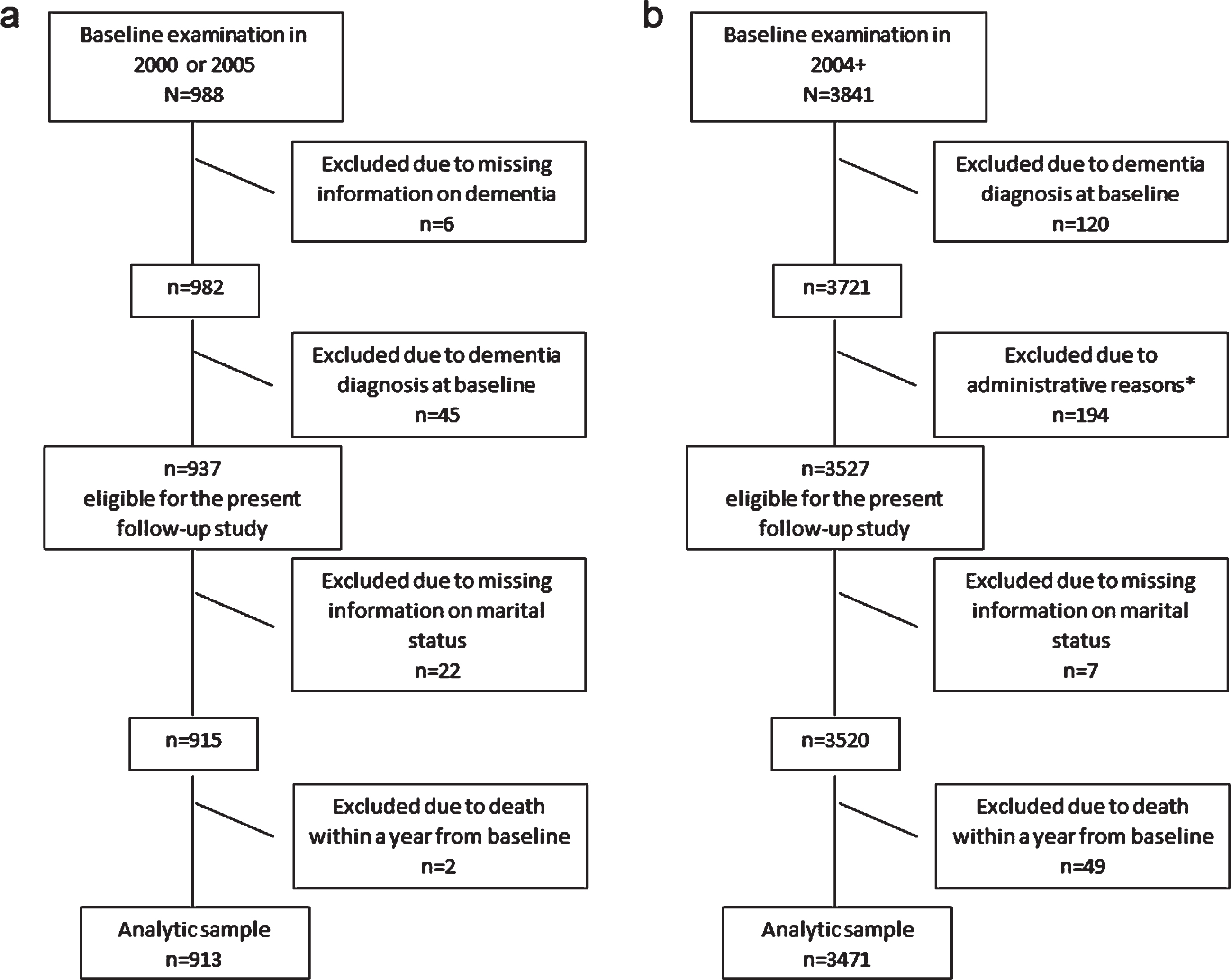
Participants are derived from the Mayo Clinic Study of Aging (MCSA 70+ study), from Rochester, MN, USA, examined in 2004 and re-examined every 15 months using the same clinical protocol for evaluation [15, 16]. In total, 3891 participants aged 70–89 years had a baseline examination, of which 50 participants were living in a convent at baseline and excluded from the current analysis due to the differential social interactions for single women in the convent. After excluding participants with dementia at baseline (n = 120), for administrative reasons (n = 194; excluded due to their initial examination being very close to the completion of the present study and they were therefore not due for a follow-up visit, nor were they reviewed for events in the Rochester Epidemiology Project (REP) medical records-linkage system [15]), with missing information on marital status (n = 7) and death within one year from baseline (n = 49), 3,471 participants were included in the present analyses (Fig. 1).
Fig. 1
Study flow chart of (a) participants included in the Gothenburg H70 Birth Cohort study (H70-study) and (b) in the Mayo Clinic Study of Aging (MCSA 70+ study). *194 individuals were excluded due to administrative reasons since their first examination was close to the completion of the present study. Thus, they were not due for a follow-up visit, nor reviewed for events in the Rochester Epidemiology Project (REP) medical records-linkage system.
The Institutional Review Boards of the Mayo Clinic and of Olmsted Medical Center approved the study.
Marital status
Information on marital status was obtained by self-report at baseline. Participants were asked if they were married, living together-not married, single-never married, divorced, widowed, or separated. To examine the difference in dementia risk between those who were married/in a marriage-like relationship and those who were not, marital status was dichotomized as “married” (married and cohabitant with a partner) and “not married” (single/divorced/widowed/separated).
Diagnosis of dementia
Diagnosis of dementia was based on Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) criteria [17], using information from an evaluation by a study coordinator or nurse, a physician, and neuropsychometric testing administered by a trained psychometrist [15, 16]. The evaluation by the study coordinator or nurse included assessment of sociodemographic factors, the Clinical Dementia Rating scale (CDR) [18] and the Functional Activities Questionnaire (FAQ) [19]. The evaluation by the physician included the Short Test of Mental Status [20], questions about memory, medical history review, and a neurological evaluation [15, 16]. Neuropsychological testing was performed using nine tests to assess four cognitive domains (memory, executive function, language, and visuospatial skills) [15, 16, 21]. For each visit, all information from the evaluation was reviewed by the nurse or study coordinator, the physician, and the neuropsychologist, and a dementia diagnosis, mild cognitive impairment, or normal cognition was adjudicated by consensus. Evaluators were blinded to information and diagnoses from previous visits.
Assessments of covariates
Age at baseline was defined as age at initial evaluation. Years of education and number of biological children were self-reported. Medical comorbidities (i.e., hypertension, depression, dyslipidemia, and diabetes mellitus) were nurse abstracted from participant medical records using the REP medical records-linkage system [15]. Weight and height were measured at baseline and body mass index (BMI) was defined as kg/m2. Smoking status was defined as ever versus never.
The gothenburg H70 birth cohort studies (H70-study)
Participants are derived from the population-based Gothenburg H70 Birth Cohort Studies (H70-study), examined in 2000–2002, 2005–2007, 2009–2011, and 2015–2016 [22–24].
In total, 988 participants (all born in 1930) had baseline examinations in 2000–2002 (mean age 70.6 years) or 2005–2007 (mean age 75.7 years), of which 982 had information on dementia status. After excluding participants with dementia at baseline (n = 45), missing information on marital status (n = 22), and death within one year from baseline (n = 2), 913 participants were included in the present analyses (Fig. 1).
The Ethics Committee for Medical Research at the University of Gothenburg approved the study.
Marital status
Information on marital status was obtained by self-report at baseline. Participants were asked if they were married, cohabiting with a partner-not married, single-never married, divorced, widowed, or in a relationship but living apart (live-apart). To examine the difference in dementia risk between those who were married/in a marriage-like relationship and those who were not, marital status was dichotomized as “married” (married and cohabitant with a partner) and “not married” (single/divorced/widowed/live-apart).
Diagnosis of dementia
Diagnosis of dementia at each examination was based on DSM-III-R criteria [25], using information from semi-structured neuropsychiatric examinations and close informant interviews performed by experienced psychiatric nurses [26, 27]. Evaluators were blinded to information and diagnoses from previous examinations. Dementia diagnoses for individuals lost to follow-up were obtained from the Swedish Inpatient Registry until 2012 (18.8%) [26]. Age of dementia onset was based on information provided by close informants, the Swedish Inpatient Register, and the neuropsychiatric examinations. If no information could be obtained, age of onset was determined as the mid-point between the last examination free from dementia and the first with dementia diagnosis. Information on deaths during follow-up was obtained from the Swedish Population Registry until December 31, 2016.
Assessments of covariates
Age at baseline was defined as age at examination in 2000–2002 or 2005–2006. Years of education and number of children were obtained by self-report at baseline. Any depression included minor (according to DSM-IV-TR) or major (according to DSM-5) depression, based on information from semi-structured psychiatric examinations at baseline [28–30]. Weight and height were measured at baseline and BMI was defined as kg/m2. Hypertension was defined as systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg or taking antihypertensive medication. Dyslipidemia was defined as having a ratio of total cholesterol and high density lipoprotein ≥5 mmol/l, low density lipoprotein ≥3.5 or taking lipid-lowering drugs. Diabetes mellitus was defined as being on anti-diabetic drugs, diet-treatment for diabetes, or having one venous blood glucose value of ≥11.1 mmol/l. Smoking status was defined as ever versus never.
Statistical analysis
All analyses were done using SAS V9.4 and R (version 4.0.0) using survminer (version 0.4.9; Kassambara et al.) and survival (version 3.2–10; Therneau et al.) packages. Sociodemographic and health characteristics are presented as mean, standard deviation (SD), median, minimum (min), maximum (max) and percentages. Differences in sociodemographic and health characteristics by marital status were analyzed using χ2-test for categorical data and Kruskal-Wallis tests for continuous measures. Cox regression models using age as the time scale were used to analyze the effect of marital status on incident dementia, presented as hazard ratios (HR) and 95%confidence interval (CI) in three different models. Model 1 included marital status, baseline age, and sex. Model 2 included marital status, baseline age, sex, years of education, and number of children. Model 3 included depression, BMI, hypertension, dyslipidemia, and diabetes mellitus in addition to covariates included in Model 2. All analyses were conducted in the MCSA 70+ study and the H70-study separately. The proportional hazard assumption was verified using Schoenfeld residuals (Supplementary Figure 1).
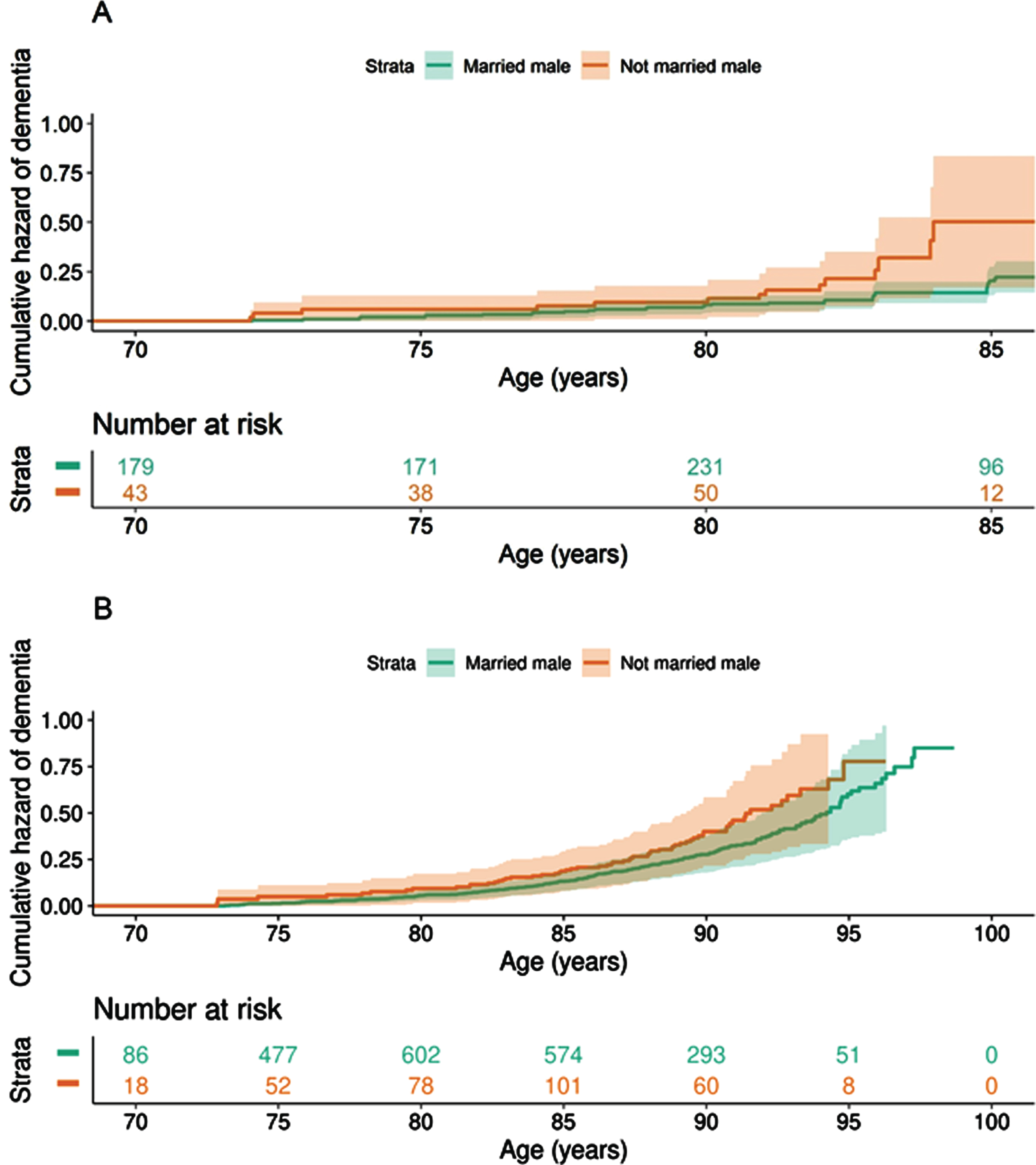
We examined the interaction of sex and marital status in relation to incident dementia using Model 3. Further, to allow potential confounders to differ between sexes, we examined the association between marital status and incident dementia in models separated by sex. In Fig. 2, cumulative hazards of dementia by marital status among men, adjusted for covariates (model 3) set to sample average, are shown.
Fig. 2
Cumulative hazard of dementia by marital status among men, in (a) H70-study and (b) MCSA 70+ study. “Marrieds” include those married and cohabiting with a partner, while “not married” include those single, divorced, widowed, and separated in the MCSA 70+ study and those live-apart in the H70-study). Analyses adjusted for covariates (baseline age, years of education, number of children, any depression, BMI, hypertension, dyslipidemia, and diabetes mellitus) set to sample average.
To examine the effect of competing risk of death, we investigated the effect of marital status on all-cause mortality in a Cox regression model adjusted for baseline age, sex, years of education, number of children, any depression, BMI, hypertension, dyslipidemia and diabetes mellitus. Further, we examined the interaction of sex and marital status in relation to risk of mortality. Finally, to allow potential confounders to differ between sexes, we examined the association between marital status and risk of mortality in models separated by sex.
Participants were censored at the date of a) dementia diagnosis, b) death, or c) end of follow-up (for the MCSA 70+ study: September 12, 2019; for the H70-study: December 31, 2016 for those with last examination year in 2015–2016, and December 31, 2012 for those with last examination year in 2009–2010 and additional information from register data until 2012).
RESULTS
MCSA 70+ study
Of the 3,471 MCSA participants at baseline, 2,316 (66.7%) were married, seven (0.2%) were cohabitant with a partner, 852 (24.6%) were widowed, 189 (5.5%) were divorced, six (0.2%) were separated, and 101 (2.9%) were single-never married. Sample characteristics and differences between those who were married and not married are shown in Table 1. During a mean follow-up of 6.8 years (SD 3.6 years, range 0.04–14.49 years; 23,608.4 person-years), 631 (18.2%) participants developed dementia, with a mean age of dementia onset of 86.5 years (SD 5.5). Compared to those excluded (n = 56; Fig. 1), those included in the analytic sample (n = 3,471) were younger (p < 0.001), had higher median age at death (p < 0.001), lower proportion of diabetes (p < 0.001), and more likely to developed dementia (p = 0.004).
Table 1
Sociodemographic and health characteristics in MCSA 70+ study (≥70 years old) and H70-study by marital status
| Characteristics | MCSA 70+ study | H70-study | ||||||
| Total sample (n = 3,471) | Marrieda (n = 2,323) | Not marriedb (n = 1,148) | p | Total sample (n = 913) | Marrieda (n = 577) | Not marriedc (n = 336) | p | |
| Baseline age, Mean (SD) | 78.6 (5.4) | 77.7 (5.1) | 80.5 (5.6) | <0.001 | 72.7 (2.6) | 72.6 (3.8) | 73.0 (2.7) | 0.03 |
| Sex, women | 48.5 (1,682/3,471) | 35.5 (825/2,323) | 74.7 (857/1,148) | <0.001 | 59.5 (543/913) | 50.1 (289/577) | 75.6 (254/336) | <0.001 |
| Education (y), Mean (SD)d | 13.9 (2.9) | 14.1 (2.9) | 13.4 (2.8) | <0.001 | 10.3 (4.3) | 10.5 (4.3) | 9.8 (4.2) | 0.01 |
| Number of children, Mean (SD)f | 3.2 (2.0) | 3.3 (1.8) | 3.1 (2.4) | <0.001 | 2.1 (1.3) | 2.2 (1.3) | 2.0 (1.4) | 0.03 |
| Smoking status, ever versus never | 49.5 (1,716/3,468) | 51.1 (1,187/2,321) | 46.1 (529/1,147) | 0.001 | 57.4 (479/835) | 55.3 (292/528) | 60.9 (187/307) | 0.1 |
| Depression | 33.9 (1,178/3,470) | 28.9 (670/2,322) | 44.3 (508/1,148) | <0.001 | 16.6 (152/913) | 12.5 (72/577) | 23.8 (80/336) | <0.001 |
| BMI, Mean (SD)e | 28.7 (5.0) | 28.6 (4.7) | 28.7 (5.7) | 0.3 | 26.8 (4.1) | 26.7 (4.0) | 26.9 (4.4) | 0.5 |
| Hypertension | 78.4 (2,720/3,470) | 75.9 (1,762/2,322) | 83.4 (958/1,148) | <0.001 | 82.1 (750/913) | 83.7 (483/577) | 79.5 (267/336) | 0.1 |
| Dyslipidemia | 81.4 (2,826/3,470) | 81.4 (1,891/2,322) | 81.4 (935/1,148) | >0.9 | 61.3 (559/912) | 61.6 (355/576) | 60.7 (204/336) | 0.8 |
| Diabetes | 19.6 (680/3,470) | 18.8 (436/2,322) | 21.3 (244/1,148) | 0.1 | 11.8 (108/913) | 11.4 (66/577) | 12.5 (42/336) | 0.7 |
| Incident dementia cases | 18.2 (631/3,471) | 16.8 (390/2,323) | 21.0 (241/1,148) | <0.001 | 16.3 (149/913) | 14.7 (85/577) | 19.0 (64/336) | 0.1 |
| Age at dementia onset (y), Mean (SD) | 86.5 (5.5) | 85.7 (5.4) | 87.8 (5.4) | <0.001 | 79.5 (3.6) | 79.4 (3.8) | 79.7 (3.3) | 0.6 |
| Censored due to death | 13.2 (459/3,471) | 11.6 (269/2,323) | 16.6 (190/1,148) | <0.001 | 24.5 (224/913) | 23.6 (136/577) | 26.6 (88/336) | 0.4 |
| Age at death (y), Median (min, max) | 87.7 (72.5, 101.9) | 86.8 (72.5, 99.2) | 88.5 (74.0, 101.9) | 0.004 | 80.1 (71.1, 86.1) | 80.1 (71.1, 86.1) | 79.1 (72.0, 86.1) | 0.1 |
%(cases/total), unless otherwise noted. aMarried/cohabitant with a partner; bSingle/Divorced/Widowed/Separated; cSingle/Divorced/Widowed/Live-apart; dH70-study: 21 missing cases; eMCSA 70+ study: 71 missing cases, H70-study: 13 missing cases; fH70-study: 30 missing cases.
In the total sample, no significant association was found between marital status and incident dementia (Table 2). There was an interaction between sex and marital status in relation to incident dementia (p = 0.015, Model 3). In analyses separated by sex, not married men had an increased risk of dementia compared to married men (Model 2 HR: 1.43; 95%CI 1.08–1.89, Table 2). The association was slightly attenuated after additional adjusting for depression, BMI, hypertension, dyslipidemia, and diabetes mellitus (Model 3 HR: 1.32; 95%CI 0.99–1.76, Table 2). No significant association was observed between marital status and incident dementia among women (Table 2). Further, the results did not change after excluding those in living in nursing homes and assisted living (n = 31; results not shown).
Table 2
Association between marital status and incident dementia in the H70-study and in MCSA 70+ study, stratified by sex
| Model 1a | Model 2b | Model 3c | |
| H70 study - Total sample | |||
| Events/total | 149/913 | 142/871 | 142/864 |
| Not married | 1.47 (1.05–2.08) | 1.44 (1.01–2.04) | 1.42 (0.99–2.02) |
| Men | |||
| Events/total | 54/370 | 52/354 | 52/351 |
| Not married | 2.13 (1.18–3.85) | 1.99 (1.06–3.76) | 2.00 (1.05–3.82) |
| Women | |||
| Events/total | 95/543 | 90/517 | 90/513 |
| Not married | 1.26 (0.84–1.89) | 1.27 (0.84–1.92) | 1.24 (0.82–1.89) |
| MCSA 70+ study - Total sample | |||
| Events/total | 631/3,471 | 622/3,433 | 611/3,360 |
| Not married | 1.06 (0.88–1.28) | 1.05 (0.87–1.27) | 1.00 (0.83–1.21) |
| Men | |||
| Events/total | 325/1,789 | 319/1,767 | 314/1,734 |
| Not married | 1.48 (1.13–1.93) | 1.43 (1.08–1.89) | 1.32 (0.99–1.76) |
| Women | |||
| Events/total | 306/1,682) | 303/1,666 | 297/1,626 |
| Not married | 0.83 (0.65–1.05) | 0.83 (0.65–1.06) | 0.82 (0.64–1.04) |
Cox regression models using “married” as the reference group and age as the time scale, presented as Hazard ratios and 95%Confidence intervals. aModel 1 include marital status, baseline age and sex. bModel 2 include marital status, baseline age, sex, years of education, and number of children. cModel 3 include marital status, baseline age, sex, years of education, number of children, any depression, BMI, hypertension, dyslipidemia, and diabetes mellitus.
In total, 459 participants were censored due to death (41.8%women) with a median age at death of 87.7 years (range, 72.5–101.9 years). Those who were not married had an increased risk of all-cause mortality compared to those who were married in a model adjusted for baseline age, sex, years of education, number of children, any depression, BMI, hypertension, dyslipidemia, and diabetes mellitus (HR 1.41; 95%CI 1.12–1.77). No significant interaction was found between marital status and sex in relation to mortality (p = 0.31). However, in models separated by sex, not married men had increased risk of death compared to married men (HR 1.56; 95%CI 1.16–2.11), while no significant association was observed in women (HR 1.25; 95%CI 0.91–1.72).
The H70-study
Of the 913 H70-study participants at baseline, 533 (58.4%) were married, 44 (4.8%) were cohabitant with a partner, 34 (3.7%) were in a relationship but live-apart, 163 (17.9%) were widowed, 112 (12.3%) were divorced, and 27 (3%) were single-never married. Compared to MCSA 70+ study, the H70-study had a lower proportion of marrieds (χ2-test; p < 0.0001) and widowed (p < 0.0001) and a higher proportion of those cohabiting with a partner (p < 0.0001) and divorced (p < 0.0001), while there was no difference in the proportion of those single-never married (p = 0.9). Sample characteristics and differences between those who were married and not married are shown in Table 1. During a mean follow-up of 10.4 years (SD 4.0 years, range 1–16 years; 9,470 person-years), 149 (16.3%) participants developed dementia, with a mean age of dementia onset of 79.5 years (SD 3.6 years). Compared to those excluded (n = 24; Fig. 1), those included in the analytic sample (n = 913) had higher median age at death (p < 0.001), higher mean time of education (p < 0.001), lower mean BMI (p < 0.001), and were less often former/current smokers (p = 0.03).
In the total sample, participants who were not married had an increased risk of dementia compared to those who were married (Table 2). No significant interaction was found between marital status and sex for risk of incident dementia (p = 0.28, Model 3). However, in models separated by sex, not married men had an increased risk of dementia compared to men who were married (Model 2 HR: 1.99; 95%CI 1.06–3.76, Table 2). The association remained similar after additional adjustment for depression, BMI, hypertension, dyslipidemia, and diabetes mellitus (Model 3 HR: 2.00; 95%CI 1.05–3.82, Table 2). There was no significant association between marital status and incident dementia among women (Table 2). Further, the results did not change after excluding those living in nursing homes and assisted living (n = 9; results not shown).
In total, 224 participants were censored due to death (46.0 %women) with a median age at death of 80.1 years (range, 71.1–86.1 years). Those not married had an increased risk of all-cause mortality compared to those who were married in a model adjusted for baseline age, sex, years of education, number of children, any depression, BMI, hypertension, dyslipidemia, and diabetes mellitus (HR 1.46; 95%CI 1.08–1.96). No significant interaction was found between marital status and sex for risk of mortality (p = 0.66). However, in models separated by sex, not married men had an increased risk of mortality compared to married men (HR 1.58; 95%CI 1.03–2.43), while no significant association was observed in women (HR 1.37; 95%CI 0.91–2.06).
DISCUSSION
In this collaborative project that includes two population-based samples from Rochester, Minnesota, USA and Gothenburg, Sweden, we examined the modifying effect of sex on the association between marital status and risk of dementia. In the H70 study, participants who were not married had an increased risk of dementia compared to those who were, but there was no association in the MCSA 70+ study. Instead, in the MCSA 70+ study, sex modified the relationship between marital status and risk of dementia. Analyses separated by sex showed that not married men had an increased risk of dementia compared to married men, while no significant association was observed between marital status and incident dementia in women. However, for the MCSA 70+ study, the association between marital status and risk of dementia among men remained only borderline significant in the fully adjusted model, probably due to loss of statistical power since the estimates were in agreement. In the H70-study, the interaction between marital status and sex in relation to incident dementia was not significant. Nevertheless, analyses separated by sex similarly showed that men who were not married, compared to married men, had an increased risk of dementia, while no significant association was observed in women.
Our finding in the H70-study that those not married had an increased risk of dementia compared to those who were married is in line with previous studies [4, 8, 9, 11, 31]. In contrast, the MCSA 70+ study, in line with the PAQUID-study [12], did not find an association between marital status and incident dementia. Reasons for discrepant results between the H70-study and the MCSA 70+ study could be due to differences in the proportion of types of marital status (the MCSA 70+ study had a higher proportion of married and widowed, but a lower proportion of divorced and those cohabiting with a partner, than the H70-study). Other reasons for divergent results could be differences in the welfare systems (e.g., health care, social security and pension system are to a higher degree regulated by the government in Sweden than in USA) and income levels (higher median household income in USA than in Sweden) between USA and Sweden [32–34]. Our finding of a moderating effect of sex on the association between marital status and dementia risk in the MSCA 70+ study is in line with results from the Health and Retirement Study (HRS) [6]. Similarly, the Singapore Longitudinal Aging Study reported increased odds ratio of cognitive impairment in single and widowed men compared to married men, but no association was observed among women [1]. In the H70-study, lack of significant interaction between sex and marital status in relation to incident dementia was likely due to low statistical power since stratified analyses by sex showed similar results as the MCSA 70+ study.
A possible explanation for our finding that individuals who were married had reduced risk of dementia compared to those not married may be due to the effect of marital status on the cognitive reserve. Individuals who are married may have greater exposure to cognitive stimulation, thus resulting in an increased cognitive reserve and a higher resilience against dementia pathology [35]. Indeed, in the Rush Memory and Aging Project, individuals who were not demented and reported larger social networks, performed better on tests of cognitive function even though they were found to have similar levels of dementia pathology as participants with smaller networks [36]. Further, our finding of a moderating effect of sex on the association between marital status and incident dementia may be explained by sex differences in the experience of loneliness. Not married men may experience loneliness to a higher degree than not married women; evidence show that married men rely more exclusively on their partner for social support, while married women have larger social networks of friends and relatives to rely on [6, 37–39]. Loneliness is proposed to activate stress responses with downstream effects on cognitive health, mediated by sleep disturbance, dysregulation of the immune system, increased oxidative stress and decreased levels of brain-derived neurotrophic factors [40–43]. Another explanation for our findings could be the additional effect of marital status on other health outcomes. A meta-analysis of 7,881,040 individuals reported that unmarried individuals were at greater risk of all-cause, cancer, cardiovascular disease, and coronary heart disease mortalities and that this association was stronger among men [44]. Similarly, previous studies have reported an increased risk of hypertension and death among men who had never been married compared to women [13], and an increased risk of depression in men who become widowed compared to women [14]. In line with this, we found that not married men had an increased risk of all-cause mortality compared to married men, while no significant association was observed in women.
Strengths of this study include the two large population-based samples from different countries. In addition, dementia diagnosis was based on information from neuropsychiatric examinations and hospital registry. Limitations should also be addressed. First, not all participants had information on marital status and covariates. Those included in the analytic samples were younger, had higher median age at death, higher mean time of education, and fewer cardiovascular risk factors, compared to those excluded. Thus, our samples could be healthier than the general population. Second, although we had information on marital status and number of children, we did not have information on other social factors that could have affected the studied associations, such as quality and duration of the marital status, the living situation for those not in a relationship, social networks, and marital trajectories. Third, there were some differences in the classification of marital status between the MCSA 70+ study and the H70-study, which could have affected the results. Regarding the “not married” group, information on those separated was available in the MCSA 70+ study (not available in the H70-study), while information on those live-apart was available in the H70-study (not available in the MCSA 70+ study). Due to the heterogeneity of those live-apart, and as the aim of the study was to examine difference in dementia risk between those who were married/in a marriage-like relationship and those who were not, those live-apart were included in the “not married” group. Fourth, cumulative attrition is a problem in follow-up studies. However, this was alleviated by the use of registry data in the H70-study and the REP medical records-linkage system in the MCSA 70+ study to detect dementia in those lost to follow-up. As aforementioned, 194 individuals were excluded due to having their first evaluation very close to completion of the present study and were therefore not due for a follow-up visit nor were they reviewed for dementia status in the REP medical records-linkage system. However, considering the reason for exclusion, we do not believe that the exclusion of these individuals has affected the studied associations. Fifth, in follow-up studies, competing risk of death may affect the results. We found that those not married had an increased risk of death compared to marrieds. Although we did not find a statistically significant interaction between sex and marital status in relation to mortality, the risk of death for not married men was elevated compared to not married women. Sixth, the two population-based samples comprise Caucasian participants living in Rochester (MN), USA and Gothenburg, Sweden, limiting the possibility of generalizing the results to other populations.
In conclusion, in two population-based samples from Rochester (MN), USA and Gothenburg, Sweden, not married men had increased risk of dementia compared to married men, while no association was observed in women. Results from this study provide additional information on sex differences in risk factors for dementia.
ACKNOWLEDGMENTS
The Mayo Clinic Study of Ageing was financed by grants from the National Institutes of Health (NIH) (grant numbers U01 AG006786, U54 AG044170, RF1 AG055151); the GHR Foundation; the Mayo Foundation for Medical Education and Research; and the Rochester Epidemiology Project (grant number R01 AG034676). The H70-study was financed by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement (grant numbers ALF 716681, ALFGBG-81392, ALF GBG-771071); Stena Foundation; Swedish Research Council (grant numbers 11267, 2005-8460, 2007-7462, 2012-5041, 2015-02830, 2019-01096, 2013-8717, NEAR 2017-00639, 2019-02075); Swedish Research Council for Health, Working Life and Welfare (grant numbers 2004-0145, 2006-0596, 2008-1111, 2010-0870, 2013-1202, 2018-00471, 2001-2646, 2003-0234, 2004-0150, 2006-0020, 2008-1229, 2012-1138, AGECAP 2013-2300, 2013-2496); Konung Gustaf V:s och Drottning Victorias Frimurarestiftelse; Hjärnfonden (grant numbers FO2014-0207, FO2016-0214, FO2018-0214, FO2019-0163); Alzheimerfonden (grant numbers AF-842471, AF-737641, AF-939825, AF-554461, AF-647651, AF-743701, AF-844671, AF-930868); Eivind och Elsa K:son Sylvans stiftelse; The Alzheimer’s Association Zenith Award (grant number ZEN-01-3151); The Alzheimer’s Association Stephanie B. Overstreet Scholars (grant number IIRG-00-2159); The Bank of Sweden Tercentenary Foundation; Stiftelsen Söderström-Königska Sjukhemmet; Stiftelsen för Gamla Tjänarinnor; Handlanden Hjalmar Svenssons Forskningsfond (grant number HJSV2020027); Stiftelsen Demensfonden; and Stiftelsen Wilhelm och Martina Lundgrens vetenskapsfond. The funding sources had no role in the study design, subject recruitment, data collection, analysis, data interpretation, manuscript preparation or the decision to submit this paper for publication.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-0246r2).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-210246.
REFERENCES
[1] | Feng L , Ng XT , Yap P , Li J , Lee TS , Håkansson K , Kua EH , Ng TP ((2014) ) Marital status and cognitive impairment among community-dwelling Chinese older adults: The role of gender and social engagement. Dement Geriatr Cogn Dis Extra 4: , 375–384. |
[2] | Arai A , Katsumata Y , Konno K , Tamashiro H ((2004) ) Sociodemographic factors associated with incidence of dementia among senior citizens of a small town in Japan. Care Manag J 5: , 159–165. |
[3] | Fan LY , Sun Y , Lee HJ , Yang SC , Chen TF , Lin KN , Lin CC , Wang PN , Tang LY , Chiu MJ ((2015) ) Marital status, lifestyle and dementia: A nationwide survey in Taiwan. PLoS One 10: , e0139154. |
[4] | Fratiglioni L , Wang HX , Ericsson K , Maytan M , Winblad B ((2000) ) Influence of social network on occurrence of dementia: A community-based longitudinal study. Lancet 355: , 1315–1319. |
[5] | Liu H , Zhang Y , Burgard SA , Needham BL ((2019) ) Marital status and cognitive impairment in the United States: Evidence from the National Health and Aging Trends Study. Ann Epidemiol 38: , 28–34.e22. |
[6] | Liu H , Zhang Z , Choi SW , Langa KM ((2020) ) Marital status and dementia: Evidence from the health and retirement study. J Gerontol B Psychol Sci Soc Sci 75: , 1783–1795. |
[7] | Saito T , Murata C , Saito M , Takeda T , Kondo K ((2018) ) Influence of social relationship domains and their combinations on incident dementia: A prospective cohort study. J Epidemiol Community Health 72: , 7–12. |
[8] | Sundström A , Westerlund O , Kotyrlo E ((2016) ) Marital status and risk of dementia: A nationwide population-based prospective study from Sweden.. BMJ Open 6: , 008565. |
[9] | Sundström A , Westerlund O , Mousavi-Nasab H , Adolfsson R , Nilsson LG ((2014) ) The relationship between marital and parental status and the risk of dementia. Int Psychogeriatr 26: , 749–757. |
[10] | Bae JB , Kim YJ , Han JW , Kim TH , Park JH , Lee SB , Lee JJ , Jeong HG , Kim JL , Jhoo JH , Yoon JC , Kim KW ((2015) ) Incidence of and risk factors for Alzheimer’s disease and mild cognitive impairment in Korean elderly. Dement Geriatr Cogn Disord 39: , 105–115. |
[11] | Håkansson K , Rovio S , Helkala EL , Vilska AR , Winblad B , Soininen H , Nissinen A , Mohammed AH , Kivipelto M ((2009) ) Association between mid-life marital status and cognitive function in later life: Population based cohort study. BMJ 339: , b2462. |
[12] | Amieva H , Stoykova R , Matharan F , Helmer C , Antonucci TC , Dartigues JF ((2010) ) What aspects of social network are protective for dementia? Not the quantity but the quality of social interactions is protective up to 15 years later. Psychosom Med 72: , 905–911. |
[13] | Ramezankhani A , Azizi F , Hadaegh F ((2019) ) Associations of marital status with diabetes, hypertension, cardiovascular disease and all-cause mortality: A long term follow-up study. PLoS One 14: , e0215593. |
[14] | Lee GR , DeMaris A , Bavin S , Sullivan R ((2001) ) Gender differences in the depressive effect of widowhood in later life. J Gerontol B Psychol Sci Soc Sci 56: , S56–61. |
[15] | Roberts RO , Geda YE , Knopman DS , Cha RH , Pankratz VS , Boeve BF , Ivnik RJ , Tangalos EG , Petersen RC , Rocca WA ((2008) ) The Mayo Clinic Study of Aging: Design and sampling, participation, baseline measures and sample characteristics. Neuroepidemiology 30: , 58–69. |
[16] | Petersen RC , Roberts RO , Knopman DS , Geda YE , Cha RH , Pankratz VS , Boeve BF , Tangalos EG , Ivnik RJ , Rocca WA ((2010) ) Prevalence of mild cognitive impairment is higher in men The Mayo Clinic Study of Aging. Neurology 75: , 889–897. |
[17] | American Psychiatric Association ((1994) ) Diagnostic and Statistical Manual of Mental Disorders, American Psychiatric Association, Washington, DC. |
[18] | Morris JC ((1993) ) The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 43: , 2412–2414. |
[19] | Pfeffer RI , Kurosaki TT , Harrah CH Jr. , Chance JM , Filos S ((1982) ) Measurement of functional activities in older adults in the community. J Gerontol 37: , 323–329. |
[20] | Kokmen E , Smith GE , Petersen RC , Tangalos E , Ivnik RC ((1991) ) The short test of mental status. Correlations with standardized psychometric testing. Arch Neurol 48: , 725–728. |
[21] | Ivnik RJ , Malec JF , Smith GE , TAngalos EG , Petersen RC , Kokmen E , Kurland LT ((1992) ) Mayo’s Older Americans Normative Studies: WAIS-R norms for ages 56 to 97. Clin Neuropsychol 6 (suppl 001): , 1–30. |
[22] | Rydén L , Zettergren A , Seidu NM , Guo X , Kern S , Blennow K , Zetterberg H , Sacuiu S , Skoog I ((2019) ) Atrial fibrillation increases the risk of dementia amongst older adults even in the absence of stroke. J Intern Med 286: , 101–110. |
[23] | Sacuiu S , Gustafson D , Sjögren M , Guo X , Ostling S , Johansson B , Skoog I ((2010) ) Secular changes in cognitive predictors of dementia and mortality in 70-year-olds. Neurology 75: , 779–785. |
[24] | Karlsson P , Thorvaldsson V , Skoog I , Gudmundsson P , Johansson B ((2015) ) Birth cohort differences in fluid cognition in old age: Comparisons of trends in levels and change trajectories over 30 years in three population-based samples. Psychol Aging 30: , 83–94. |
[25] | American Psychiatric Association ((1987) ) Diagnostic and Statistical Manual of Mental Health Disorders (3rd ed. revised). American Psychiatric Association, Washington, DC. |
[26] | Guo X , Waern M , Sjogren K , Lissner L , Bengtsson C , Bjorkelund C , Ostling S , Gustafson D , Skoog I ((2007) ) Midlife respiratory function and Incidence of Alzheimer’s disease: A 29-year longitudinal study in women. Neurobiol Aging 28: , 343–350. |
[27] | Skoog I , Nilsson L , Palmertz B , Andreasson LA , Svanborg A ((1993) ) A population-based study of dementia in 85-year-olds. N Engl J Med 328: , 153–158. |
[28] | Rydberg Sterner T , Gudmundsson P , Sigström R , Ahlner F , Seidu N , Zettergren A , Kern S , Östling S , Waern M , Skoog I ((2019) ) Depression and neuroticism decrease among women but not among men between 1976 and 2016 in Swedish septuagenarians. Acta Psychiatr Scand 139: , 381–394. |
[29] | American Psychiatric Association ((2011) ) Diagnostic and statistical manual of mental disorders (4th ed.). American Psychiatric Association, Washington, DC. |
[30] | American Psychiatric Association ((2013) ) Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association, Washington, DC. |
[31] | Helmer C , Damon D , Letenneur L , Fabrigoule C , Barberger-Gateau P , Lafont S , Fuhrer R , Antonucci T , Commenges D , Orgogozo JM , Dartigues JF ((1999) ) Marital status and risk of Alzheimer’s disease: A French population-based cohort study. Neurology 53: , 1953–1958. |
[32] | Galloway BW (2017) Swedish SocialWelfare and its Application to American Welfare Systems. |
[33] | DATA USA, Rochester, MN, https://datausa.io/profile/geo/rochester-mn/#housing, Accessed 2021-04-21. |
[34] | Statistics Sweden, Median household income by region, household, age and year http://www.statistikdatabasen.scb.se/pxweb/sv/ssd/START__HE__HE0110__HE0110G/Tab4bDispInkN/table/tableViewLayout1/, Accessed 2021-04-21. |
[35] | Borenstein AR , Mortimer JA ((2016) ), Alzheimer’s disease: Life course perspectives on risk reduction. Academic Press. |
[36] | Bennett DA , Schneider JA , Tang Y , Arnold SE , Wilson RS ((2006) ) The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: A longitudinal cohort study. Lancet Neurol 5: , 406–412. |
[37] | Williams K , Umberson D ((2004) ) Marital status, marital transitions, and health: A gendered life course perspective. J Health Soc Behav 45: , 81–98. |
[38] | Hemström Ö ((1996) ) Is marriage dissolution linked to differences in mortality risks for men and women? J Marriage Fam 58: , 366–378. |
[39] | Gove WR ((1973) ) Sex, marital status, and mortality. Am J Sociol 79: , 45–67. |
[40] | Hsiao YH , Chang CH , Gean PW ((2018) ) Impact of social relationships on Alzheimer’s memory impairment: Mechanistic studies. J Biomed Sci 25: , 3. |
[41] | Lara E , Martín-María N , De la Torre-Luque A , Koyanagi A , Vancampfort D , Izquierdo A , Miret M ((2019) ) Does loneliness contribute to mild cognitive impairment and dementia? A systematic review and meta-analysis of longitudinal studies. Ageing Res Rev 52: , 7–16. |
[42] | McHugh JE , Lawlor BA ((2013) ) Perceived stress mediates the relationship between emotional loneliness and sleep quality over time in older adults. Br J Health Psychol 18: , 546–555. |
[43] | Murínová J , Hlaváčová N , Chmelová M , Riečanský I ((2017) ) The evidence for altered BDNF expression in the brain of rats reared or housed in social isolation: A systematic review. Front Behav Neurosci 11: , 101. |
[44] | Wang Y , Jiao Y , Nie J , O’Neil A , Huang W , Zhang L , Han J , Liu H , Zhu Y , Yu C , Woodward M ((2020) ) Sex differences in the association between marital status and the risk of cardiovascular, cancer, and all-cause mortality: A systematic review and meta-analysis of 7,881,040 individuals. Glob Health Res Policy 5: , 4. |


