
Declining Use of Potentially Inappropriate Medication in People with Dementia from 2000 to 2015: A Repeated Cross-Sectional Nationwide Register-Based Study
Abstract
Background:
Studies have shown declining use of potentially inappropriate medication (PIM), medication where risks associated with use outweigh potential benefits in older people. However, the trend in people with dementia remains unknown.
Objective:
To test the hypothesis that the use of PIM has decreased in people with dementia in line with the declining use in the general older population.
Methods:
Repeated cross-sectional register-based study of the entire Danish population aged ≥65 years (2000: N = 802,106; 2015: N = 1,056,476). PIM was identified using the Danish “Red-yellow-green list”. Changes in the use of PIM were examined by calculating the annual prevalence of filling prescriptions for at least one PIM in older people with and without dementia. Characteristics of the study population were examined annually including comorbidity.
Results:
From 2000 to 2015, the prevalence of PIM use decreased from 54.7%to 43.5%in people with dementia and from 39.5%to 28.8%in people without dementia; the decrease was significant across all age groups and remained so in a sensitivity analysis where antipsychotics were removed. During the same period, comorbidity scores increased in people with and without dementia.
Conclusion:
The declining use of PIM in people with dementia from 2000 to 2015 parallels the trend in the general older population. The use of PIM decreased despite increasing levels of comorbidity and was not solely attributable to the decreasing use of antipsychotics in people with dementia. However, PIM use remained more widespread in people with dementia who may be more vulnerable to the risks associated with PIM.
INTRODUCTION
Potentially inappropriate prescribing, which is a major public health concern in older people, is often defined as treatments where potential risks outweigh benefits [1, 2]. The concept has multiple aspects, including inappropriate drug choice, polypharmacy, drug-drug interactions, drug-disease interactions, or even treatment omissions [3]. Several explicit and implicit quality indicators have been developed to identify inappropriate prescribing. Explicit indicators are criteria-based; most focus mainly or solely on drugs that should be avoided in all older people—often termed potentially inappropriate medication (PIM). The most widely known criteria are the Beers Criteria, first published in 1991 in the United States and since then updated several times [4, 5]. Due to the great variability in available drugs and prescribing practices, many countries have developed their own lists of PIM. In Denmark, the Institute for Rational Pharmacotherapy published its list of PIM in 2011 called the Red-yellow-green list [6].
The use of PIM has been associated with several adverse outcomes including increased risk of falls, fractures, hospitalizations, and mortality [7–9]. Potentially inappropriate prescribing is of particular concern in people with dementia who may be more susceptible to the adverse effects associated with PIM, and in whom widespread polypharmacy, frailty, multimorbidity, and changing goals of care due to the progressive nature of dementia further complicate pharmacological management [10–12]. Additionally, cognitive decline can negatively influence adherence to treatment regimens and the ability to report adverse effects and make people with dementia more susceptible to the adverse effects of specific drugs, e.g., anticholinergics [13]. In a Swedish study, 41%of acute hospitalizations of people with dementia were determined to be drug-related [14]. Nonetheless, PIM is widespread in people with dementia, with a prevalence ranging from 14–64%in a recent review [15]. In our previous study in Denmark, we found that 45%of people with dementia had filled at least one prescription for PIM in 2014 compared to 30%of people without dementia [16].
A review of existing literature revealed that the use of PIM in older people has been decreasing since the mid 1990s in the western world [17–23]. However, the time trend in people with dementia has not been investigated. The aim of this nationwide study was to investigate changes in the use of PIM in older people with dementia from 2000 to 2015. We hypothesized that the use of PIM had decreased in people with dementia in line with the documented decrease in the general older population.
METHODS
Study design
We conducted a repeated-measures cross-sectional study utilizing nationwide Danish registers to examine changes in the use of PIM in people with and without dementia from 2000–2015. The study was approved by the Danish Data Protection Agency (ID no.: 2007-58-0015/30-0667), Statistics Denmark, and the Danish Health and Medicines Authority (ID no.: 6-8011-907/1). According to Danish law, it is not required to obtain ethics committee approval for register-based studies.
Data
All Danish residents are provided a unique personal identification number at birth or upon immigration. This facilitates individual-level linkage of data across nationwide registers including the Danish National Patient Register, the Danish Psychiatric Central Research Register, and the Danish National Prescription Registry [24–27]. The National Patient Register contains information on admission and discharge dates as well as discharge diagnoses from all hospitalizations and invasive procedures since 1978 and hospital-based outpatient clinics and emergency departments since 1995 [24]. The Psychiatric Central Research Register contains data on all psychiatric inpatient admissions since 1969 and outpatient contacts since 1995. The Danish National Prescription Registry contains information on all dispensed prescription medication since 1995; including prescriptions to older people residing in nursing homes. The data on dispensed prescriptions include data on the type of drug according to the Anatomical Therapeutic Chemical (ATC) system as well as strength, amount, and date of dispensing [26].
Study population
The study population was defined annually on January 1st from 2000 to 2015 (index date) and included all residents in Denmark aged ≥65 years. People with dementia were identified as individuals registered with a dementia diagnosis as an in- or outpatient (specific diagnosis codes available in the Supplementary Material) and/or as individuals who had filled at least one prescription for anti-dementia medication (ATC: N06D) before the index date. Anti-dementia drugs are not approved, nor to our knowledge, prescribed for any other indication in Denmark. Individuals were excluded if they had been diagnosed with dementia and/or filled their first prescription for anti-dementia medication before age 60 as previous research has found early diagnoses to be unreliable in the registers [28, 29]. Characteristics of the study population including age, sex, marital status, and comorbidity status were examined to facilitate comparisons between the groups and changes within the study period. Comorbidity status was assessed using the Charlson Comorbidity Index, which was calculated without dementia as one of the items [30].
Potentially inappropriate medication (PIM)
The Danish Red-yellow-green list has three categories: the green category lists drugs where evidence regarding long-term effects is limited; the yellow category lists drugs where the indication and dosage should be reassessed regularly, i.e., to use with care; and lastly, the red category lists drugs that should be avoided in people aged 65 years or above unless under special circumstance [6]. In this study, the red and the yellow categories were examined; however, only the red category, which matches the general definition, was used to define PIM. Most drugs from the red and the yellow categories are included in several other criteria including the Beers Criteria [4]. The red category contains 28 drugs and drug classes (for specific drugs, see Fig. 4). The yellow category contains 10 drugs or drug classes (included drugs available in the Supplementary Material). Both the red and yellow categories are divided into subgroups based on indication: digestive, cardiovascular, urological, analgesics, hypnotics/anxiolytics, antipsychotics, and antidepressants. Two drugs were excluded from our study as recommendations were dependent on dosage information (acetylsalicylic acid and a combination containing dipyridamole and acetylsalicylic acid).
Fig. 3
Proportion of users of potentially inappropriate medication (PIM), defined in this study as drugs from the red category of the red-yellow-green list, filling prescriptions for≥2 different PIM from 2000-2015 in people with (blue) and without (red) dementia.
The Danish red-yellow-green list was first published in 2011 and since updated in 2016, the original 2011 edition was used in this study. The most significant changes in the 2016 edition were that all antipsychotics, all benzodiazepines and similar drugs (z-drugs), and all antidepressants were considered red, some of which were not included in the 2011 edition or considered yellow [31].
Statistics
To examine changes in the use of PIM from 2000 to 2015 in people with and without dementia, we calculated the following measures annually: 1) The percentage of PIM users, defined as people filling at least one prescription for a PIM within a given calendar year, 2) the percentage of new PIM users in a given year, defined as filling a prescription for a subgroup of the red category for which the individual had not filled a prescription in the previous calendar year. New use was determined by subgroup and not by specific drugs as this allowed substitution within groups without this being registered as the initiation of a new treatment, 3) the percentage of PIM users filling prescriptions for multiple different PIM, defined as filling prescriptions for ≥2 different PIM within a given calendar year, and 4) utilization patterns per subgroup of the red and yellow categories, done by calculating the percentage who filled prescriptions for drugs from each subgroup of the red and yellow categories within a given calendar year.
The use of antipsychotics in the management of behavioral symptoms associated with dementia has decreased following national and international warnings on adverse events including increased mortality associated with such use [32–35]. In Denmark, the use of antipsychotics in people with dementia decreased from 31%to 20%from 2000 to 2012 [36]. The red category of the Red-yellow-green list includes eight antipsychotics. Therefore, a sensitivity analysis was conducted excluding antipsychotics from the analyses to discern whether a potential decline in the use of PIM was driven solely by the established decline in the use of antipsychotic medication.
Logistic regression was used to compare the annual prevalence of filling one or more prescriptions for PIM in 2015, 2010, 2005, and 2000 (reference year). To obtain the independent observations necessary for the analyses, the population was divided into 5-year age groups (age 65–69, 70–74, 75–79, 80–84, 85–89, 90–94, and 95–99), so that an individual would not be represented at more than one time point in the same group. Logistic regression was done separately for people with and without dementia. First, a crude logistic regression was conducted with the calendar year as the independent variable. Second, sex was included in a multivariable logistic regression as potential confounders. Third, as a sensitivity analysis, the Charlson Comorbidity Index was added to the multivariable analysis. Odds ratios (OR) were presented with 95%confidence intervals (CI). A p-value of < 0.5 was considered statistically significant. The data analysis was performed using SAS statistical software, version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Characteristics of the study population
On January 1, 2000, we identified 19,062 people≥65 years with dementia (2.4%) and 781,056 without dementia (97.6%). In 2015, this had increased to 36,031 (3.4%) individuals with dementia and 1,018,015 individuals without dementia (96.6%). Table 1 lists the characteristics of the study population in 2000 and 2015. In both years, people with dementia were older, more likely to be female, and had higher comorbidity scores. From 2000 to 2015, the age distribution in the two groups remained largely the same over time, while the comorbidity scores increased in people with and without dementia.
Table 1
Characteristics of the study population in 2000 and 2015 stratified by dementia status
| 2000 | 2015 | |||
| Dementia | No dementia | Dementia | No dementia | |
| N = 19,062 | N = 781,056 | N = 36,031 | N = 1,018,015 | |
| (100 %) | (100%) | (100%) | (100%) | |
| Sex (female) | 12,865 (67.5) | 452,944 (58.0) | 22,789 (63.3) | 551,093 (54.1) |
| Married1 | 5,832 (30.6) | 382,946 (49.8) | 12,726 (35.3) | 583,822 (57.7) |
| Age groups | ||||
| 65–69 | 1,070 (5.6) | 221,119 (28.3) | 2,031 (5.6) | 351,056 (34.5) |
| 70–74 | 2,266 (11.9) | 195,146 (25.0) | 4,167 (11.6) | 269,962 (26.5) |
| 75–79 | 4,236 (22.2) | 165,670 (21.2) | 6,468 (18.0) | 180,439 (17.7) |
| 80–84 | 4,661 (24.5) | 107,665 (13.8) | 8,589 (23.8) | 113,720 (11.2) |
| 85–89 | 4,491 (23.6) | 63,072 (8.1) | 8,723 (24.2) | 66,100 (6.5) |
| 90–94 | 1,930 (10.1) | 23,108 (3.0) | 4,878 (13.5) | 28,827 (2.8) |
| 95–99 | 388 (2.0) | 4,809 (0.6) | 1,064 (3.0) | 6,991 (0.7) |
| CCI score2 | ||||
| 0 | 8,632 (45.3) | 484,636 (62.1) | 11,931 (33.1) | 512,375 (50.3) |
| 1 | 4,929 (25.9) | 137,353 (17.6) | 8,451 (23.5) | 183,425 (18.0) |
| 2 | 2,875 (15.1) | 94,073 (12.0) | 6,415 (17.8) | 159,420 (15.7) |
| ≥3 | 2,626 (13.8) | 64,994 (8.3) | 9,234 (25.6) | 162,795 (16.0) |
CCI, Charlson Comorbidity Index. 1data missing on civil status: 11,767 in 2000 and 6,245 in 2015. 2Calculated without dementia as one of the items. Numbers are given as n (%) and median (25–75%interquartile range), as appropriate.
Prevalence of PIM
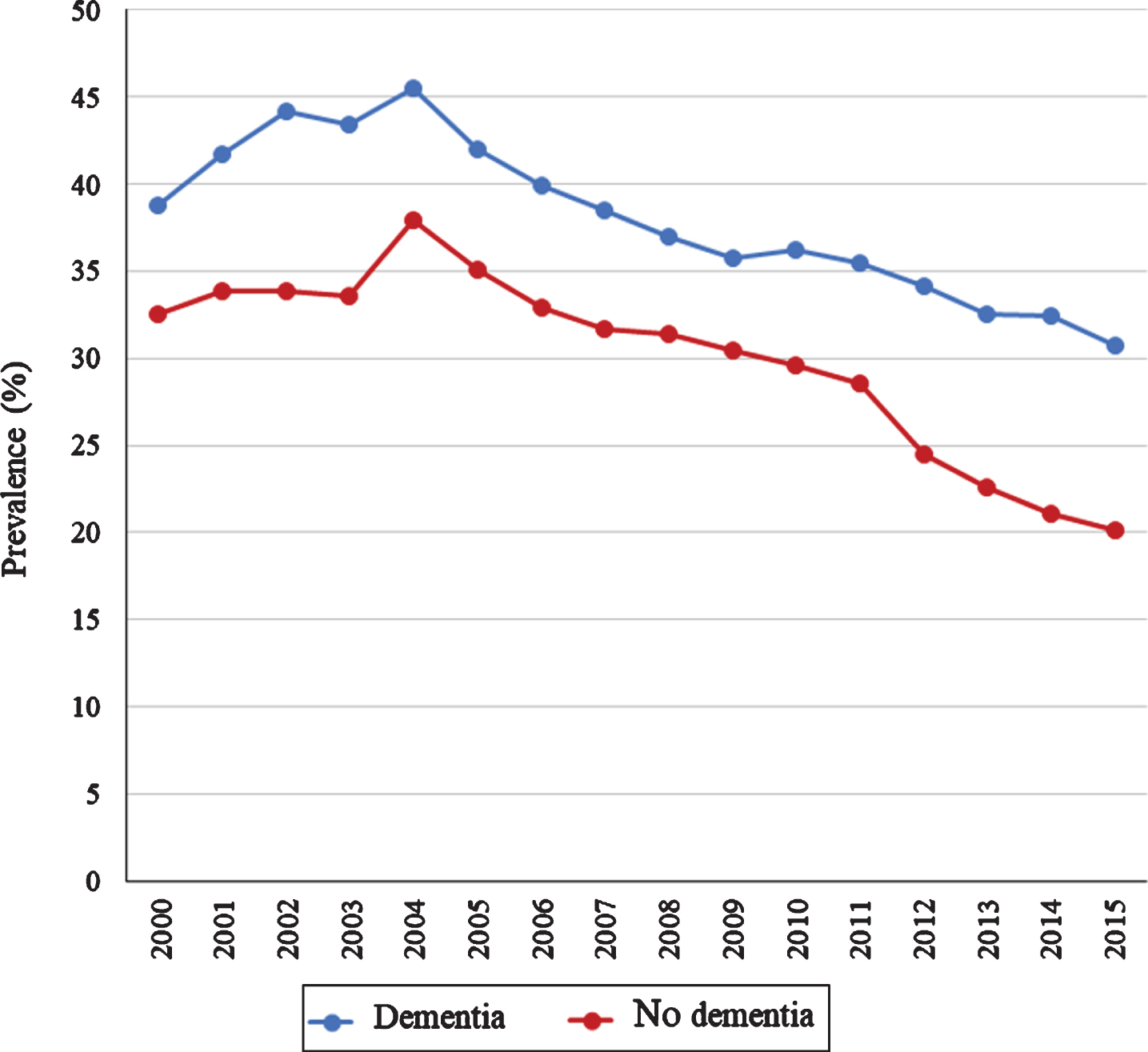
Figure 1 shows the annual proportion of people with and without dementia filling at least one prescription for one or more drugs from the red category of the Red-yellow-green list which was used to identify PIM. As seen in Fig. 1, the use of PIM was continuously more widespread in people with dementia from 2000 to 2015. In people with dementia, the prevalence decreased from 54.7%to 43.5%from 2000 to 2015, whereas it decreased from 39.5%to 28.8%in people without dementia. Figure 2 shows the results of the logistic regression comparing 2000 to 2015 in 5-year age groups stratified by dementia status and adjusted for sex. The use of PIM was significantly less likely in 2015 compared to 2000 in all age groups in both people with and without dementia. The most marked decrease was found in people aged 85–89 where the likelihood of PIM use in 2015 was almost half of what it had been in 2000 (adjusted ORs: dementia, 0.60 (0.55–0.64); no dementia: 0.52 (0.51–0.53)) (detailed results available in the Supplementary Material). In a sensitivity analysis, the Charlson Comorbidity Index was added to the multivariable logistic regression to adjust for changes in comorbidity levels, this made the decreasing trend slightly more marked across all age groups (detailed results available in the Supplementary Material). In a second sensitivity analysis excluding all antipsychotics, the decrease remained significant across all age groups in people with dementia (detailed results available in the Supplementary Material).
Fig. 1
Prevalence of potentially inappropriate medication (PIM), defined as the red category of the red-yellow-green list, in older people with dementia (blue line) and without dementia (red line) from 2000 to 2015. And the prevalence of new use of PIM in people with dementia (dashed transparent blue line) and without dementia (dashed transparent red line) from 2000 to 2015.
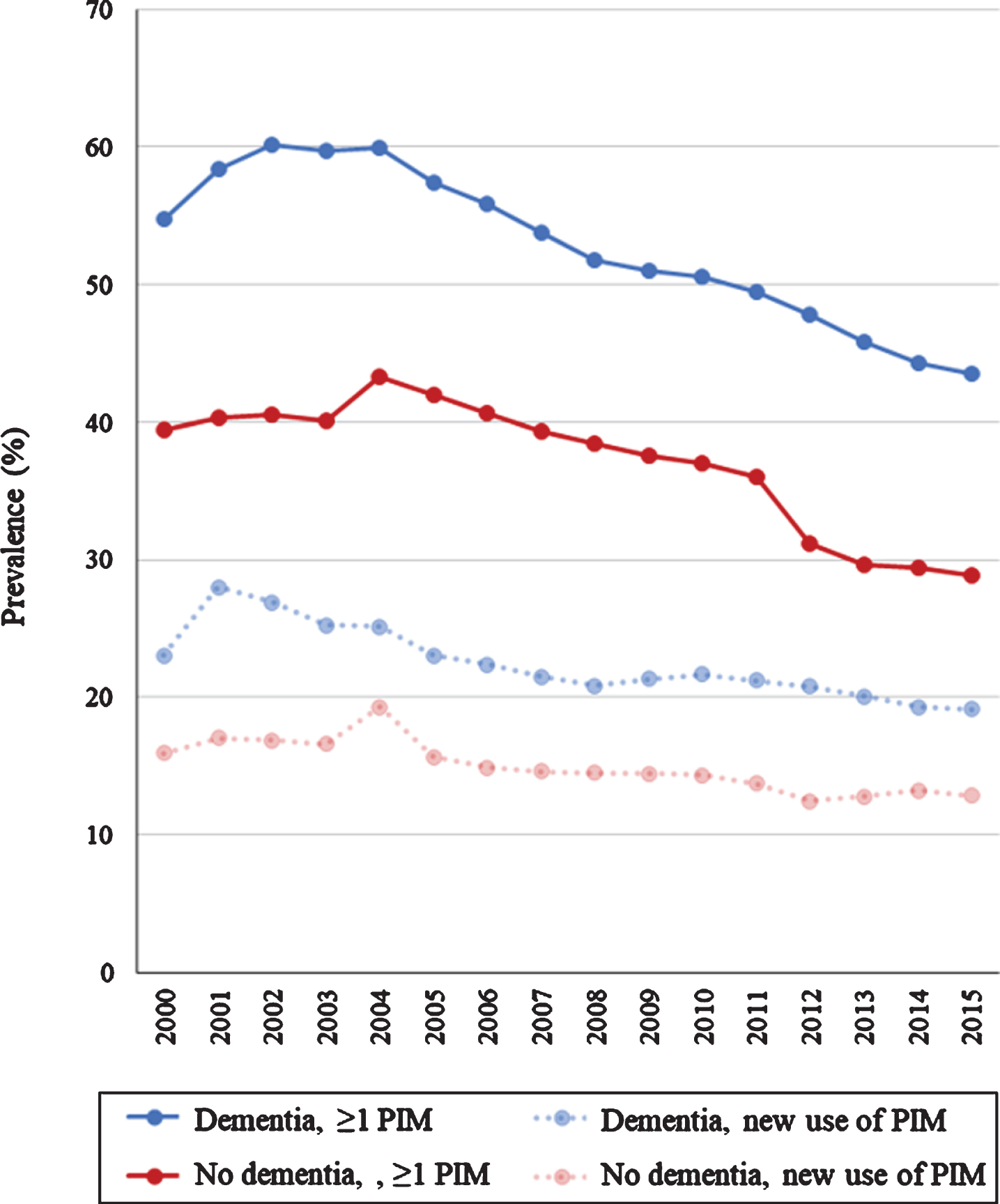
Fig. 2
Likelihood of potentially inappropriate medication (PIM), defined as drugs from the red category of the red-yellow-green list, use in 2015 versus 2000 in people with dementia (blue) and without (red) dementia. Panel A shows the results of logistic regression analyses comparing 2015 versus 2000 and Panel B shows the result of the sensitivity analysis where antipsychotics from the red category were excluded from the analysis in 5-year age groups displaying adjusted odds ratios (ORs) and 95%confidence intervals (CIs). Adjustments were made for sex.
The use of drugs from the yellow category was also studied: Use of drugs from the yellow category was also continuously more widespread in people with dementia compared to people without dementia. In people with dementia, the prevalence of filling at least one prescription for drugs from the yellow category, drugs to use with caution, decreased from 56.2%in 2000 to 43.7%in 2015. In people without dementia, the prevalence decreased from 29.8%to 25.4%.
New use of PIM
Figure 1 also shows the percentage of new users of PIM from 2000–2015. In people with dementia from 2000 to 2015, the percentage of new users of PIM decreased from 23.0 to 19.1%, whereas it decreased from 15.9%to 12.8%in people without dementia.
Use of multiple PIM
Most users of PIM, irrespective of dementia status, only filled prescriptions for one potentially inappropriate drug. Figure 3 shows the proportion of users who filled prescriptions for multiple PIM, which peaked in 2004 (dementia: 45.5%; no dementia: 34.1%). Overall, the proportion of PIM users who filled prescriptions for multiple different PIM decreased from 38.7%to 30.7%in people with dementia and from 32.5%to 20.2%in people without dementia from 2000 to 2015.
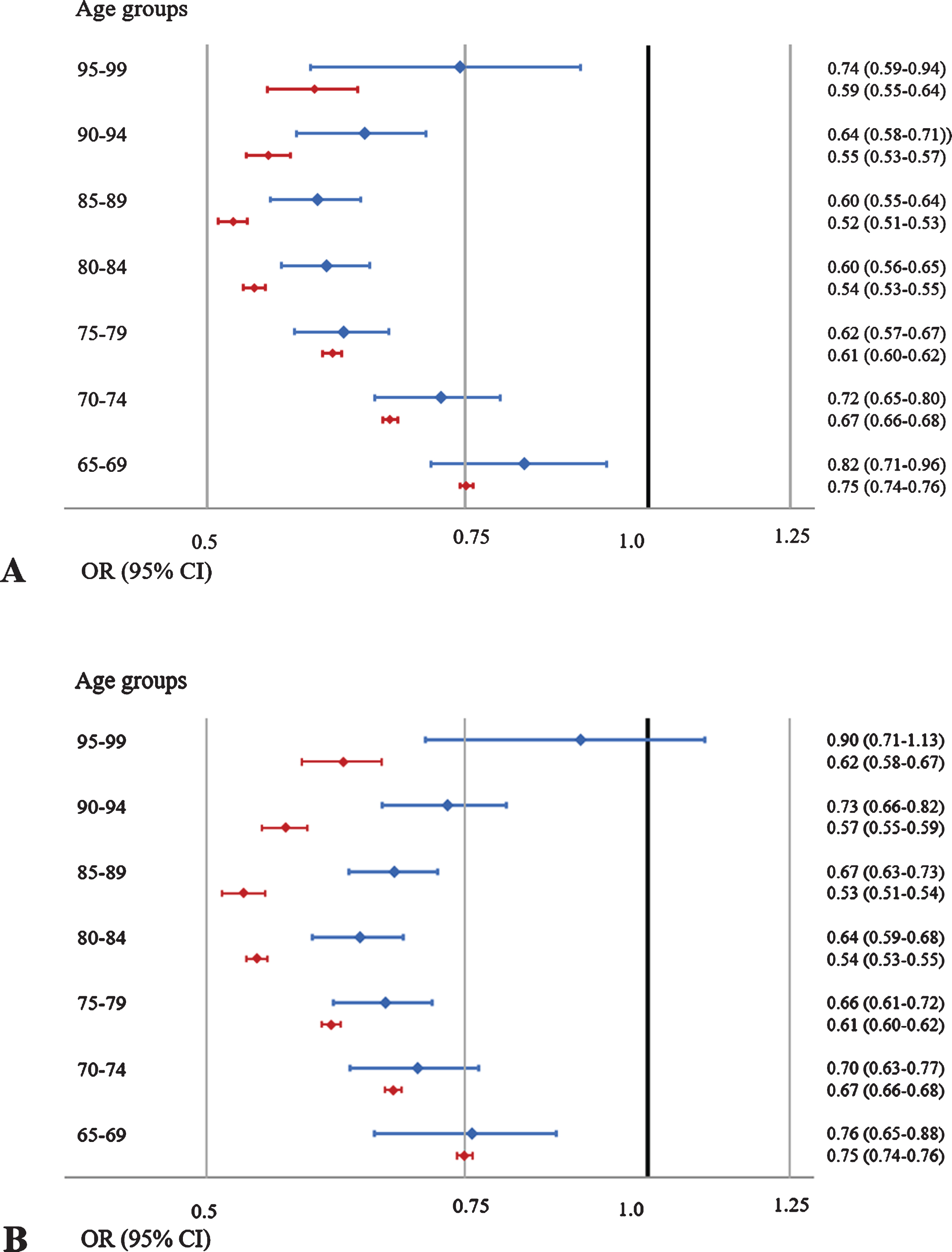
Subgroups of PIM
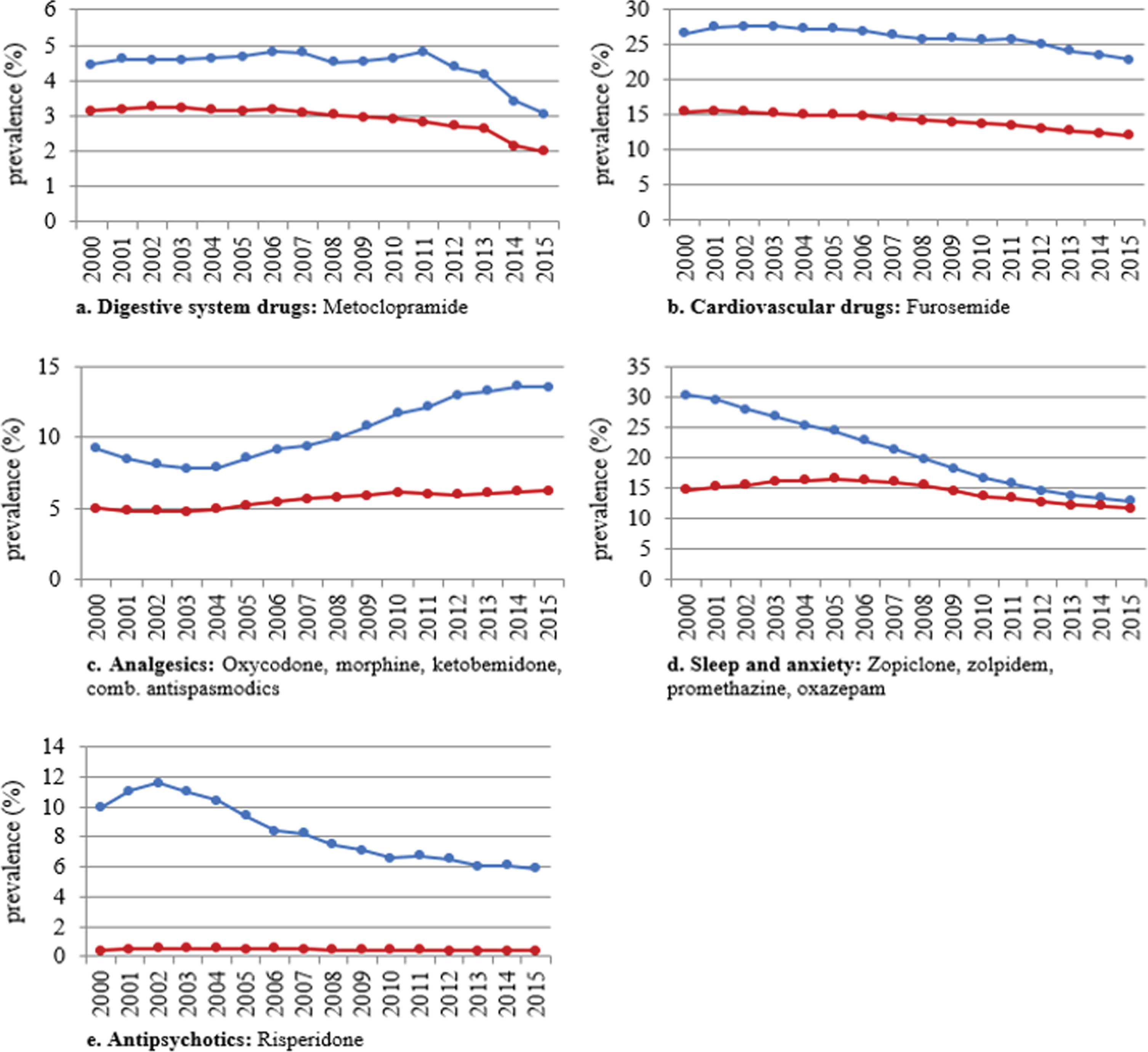
Figure 4 shows the annual proportion of people with and without dementia filling prescriptions for the various subgroups of the red category and Fig. 5 shows the annual proportion of people with and without dementia filling prescriptions for the various subgroups of the yellow category. The largest decrease in people with and without dementia was in the use of drugs for “hypnotics and anxiolytics”: red category (dementia: from 10.3%in 2000 to 5.1%in 2015); no dementia (11.2%to 2.1%) and yellow category (dementia: 30.3%to 12.8%; no dementia: 14.7%to 11.7%). Use of drugs from the various yellow subcategories also decreased from 2000–2015; however, an important exception was the analgesics category (including oxycodone, ketobemidone in combination with antispasmodics, and morphine) which increased from 9.2%to 13.5%in people with dementia and 5.0%to 6.2%in people without dementia. The use of morphine specifically increased from 5.2%to 10.1%in people with dementia and from 2.5%to 4.1%in people without dementia.
Fig. 4
Annual prevalence of potentially inappropriate medications (PIM), defined as the red category of the red-yellow-green list, use from 2000 to 2015 in people with (blue) and without dementia (red) per subgroup of the red category.
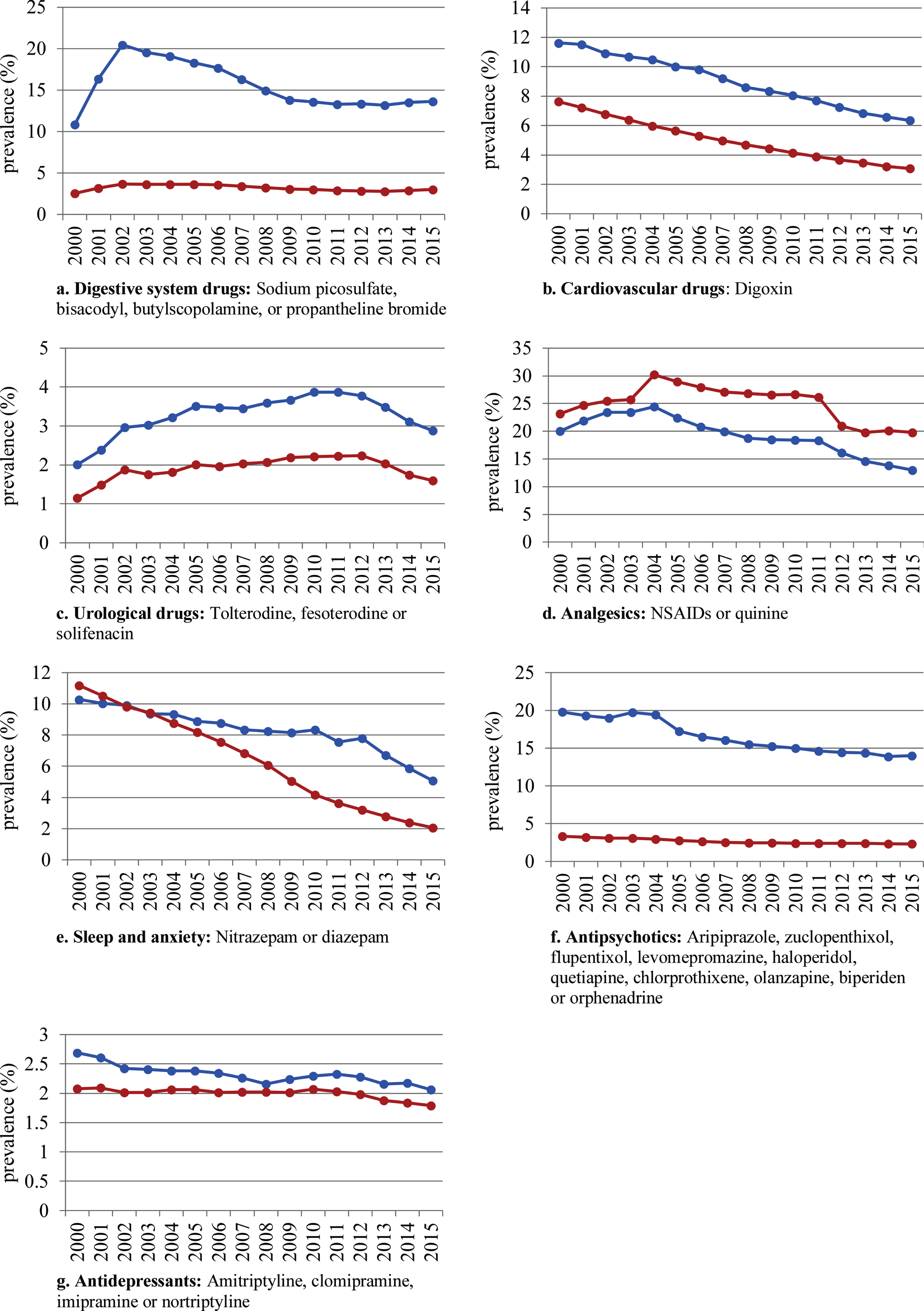
Fig. 5
Annual prevalence of drugs from the yellow category of the red-yellow-green list use from 2000 to 2015 in people with (blue) and without dementia (red) per subgroup of the yellow category.
DISCUSSION
To our knowledge, this is the first study to examine the time trend of PIM use in people with dementia. First, in line with our hypothesis, we found a decrease in the use of PIM in people with dementia that paralleled the documented decrease in the general older population. Second, this decrease was not attributable to the declining use of antipsychotics alone. Third, the decreasing use of PIM from 2000 to 2015 was observed despite increasing comorbidity scores in older people both with and without dementia. Last, throughout the study period, the use of PIM was more widespread in people with dementia compared to people without dementia.
To the best of our knowledge, this was the first time-trend study of the use of PIM specifically in people with dementia. However, several studies have examined the time trend of PIM as measured by various explicit criteria in the general older population: differences in national settings, study periods, selection of the study population, and, in particular, differences between the various explicit quality indicators used, impede direct comparisons. Nevertheless, in line with our findings, most reported a decrease [18–20, 22, 37–40], while three reported either a slight increase [41] or a stable prevalence [42, 43]. Two out of these three used subsets of the STOPP-criteria, indicating that the observed decrease may not apply to all measures of potentially inappropriate medication. In our study, the use of PIM decreased from 55%to 44%in people with dementia and from 39%to 29%in older people without dementia from 2000 to 2015. Using the Beers criteria to define PIM, other studies have found comparable declines: in Australia, PIM use declined from 45%in 1993 to 40%in 2005 [40]; a US study reported a decline from 46%to 41%from 2006 to 2012 [20]. While we found no studies examining the time trend in PIM use specifically in people with dementia, a study investigated the Swedish drug-specific recommendations in geriatric care units where approximately 70%of the residents were cognitively impaired [21]. They found a decrease from 44%to 26%from 2007 to 2013 which, though more marked, is in line with our findings [21].
In our study, there was a small increase in the use of PIM in the initial years of study. A possible explanation could be that some of the drugs included in the red category of the red-yellow-green list were newly introduced to the market at the beginning of the study period, e.g., quetiapine (N05AH04). However, the initial increasing use of quetiapine was accompanied by a simultaneous decrease in other drugs from the same drug class indicating substitution rather than novel use.
One possible explanation for the declining use of PIM could be the growing attention to potential risks associated with the use of PIM in older people. As evident from the steady rate of publications of criteria for PIM, guidelines on pharmacotherapy, and warnings from, for instance, the FDA, efforts to improve the quality and safety of prescribing for the older population have intensified [4, 44, 45]. Our study indicates that these efforts have also influenced the quality of prescribing for people with dementia. As is evident by our results, the decreasing trend identified in this study preceded the publication and, subsequently, indicates an underlying trend which the publication of the list itself was a result of [6].
The use of antipsychotics in people with dementia has been associated with increased mortality risk, and several guidelines regarding this issue have been published [46–48]. Thus, in recent years, the use of antipsychotics in the treatment of behavioral symptoms associated with dementia has decreased [36]. Consequently, another explanation for the declining use of PIM in older people with dementia could be the decrease in the use of antipsychotics. However, in this study, we found that the decline in the use of PIM in people with dementia could not be attributed to the decrease in the use of antipsychotics alone.
Another possible explanation for the decreasing use of PIM could be a change in the demographics of the population and thus a lower prevalence of risk factors for PIM. Age is a risk factor for PIM [49], but the mean age remained largely unchanged throughout the study period. Polypharmacy also increases the risk of PIM [49, 50]; but in a previous study, we found an increase in polypharmacy from 2000 to 2011, and thereafter, a relatively stable prevalence until 2014 [51]. Additionally, increasing levels of comorbidity heighten the risk of PIM use [52], but despite an increase in comorbidity within the study period, the use of PIM decreased. Furthermore, in a sensitivity analysis, we adjusted for the comorbidity levels, which made the decreasing trend slightly more marked. Thus, changes in demographics do not explain the decrease in the use of PIM. Consequently, the use of PIM decreased despite increasing polypharmacy and comorbidity, indicating greater awareness of PIM and greater caution when prescribing to older people and people with dementia. While the decline in the use of PIM demonstrated in this study is a positive find, the study also identified potential implications to the safety of patient: First, the use of PIM was continuously more widespread in people with dementia who could be more susceptible to the adverse effects associated with the use of PIM. Secondly, while the use of drugs from most subgroups of the Red-yellow-green list decreased in the study period, the use of analgesics from the yellow category increased in people with dementia. This increase was mainly driven by the increasing use of morphine which was also observed in a recent study in the same population. In this study, a disproportionate increase in the use of opioids was observed in people with dementia. The authors speculated that a possible explanation could be that opioids have replaced antipsychotics in the treatment of behavioral and psychological symptoms associated with dementia [53].
The greatest strength of the study is the use of complete nationwide data which makes it possible to identify individuals with dementia and follow them in the registers and examine real-life prescription patterns without risk of selection bias. However, this study also has some limitations: First, while the study was based on complete information on all filled prescriptions, we cannot ascertain whether the medication was actually consumed. Furthermore, information on over-the-counter sales, as well as treatment duration, and dosage, is not available in the registers. In Denmark, low-dose ibuprofen, which is in the red category, is available over the counter in limited quantities which could lead to an underestimation of use. Secondly, while the validity of a dementia diagnosis in the Danish registers has previously proven to be high it is well known that dementia is underdiagnosed [29]. In 2015, we identified 36,031 people aged 65 years or above who had been registered with a dementia diagnosis in the Danish registers. However, based on the extrapolation from European population-based studies, Alzheimer Europe estimates that approximately 87,000 aged 60 or above in Denmark are living with dementia [54]. Consequently, the reference group without dementia contains an unknown number of individuals with undiagnosed or untreated dementia, which could have led to an underestimation of differences between people with and without dementia. Thirdly, using the Danish Red-yellow-green list rather than an internationally well-known indicator could limit generalizability. However, the majority of drugs in the red category is also included in other well-known explicit indicators. Furthermore, due to differences in prescribing practices, guidelines, and available medication, we believe the national Danish list is better suited to this setting.
This nationwide study found a decrease in the use of PIM from 2000 to 2015 in people with dementia comparable to the decrease found in the general older population. The decrease in the use of PIM in people with dementia was not attributable to the decreasing use of antipsychotics alone. Furthermore, the decrease was observed despite increasing levels of comorbidity in the same period. This indicates that efforts to improve prescribing practices in the older population also had an effect in people with dementia. However, the use of PIM remained continually more widespread in people with dementia compared to people without dementia which could have implications for patient safety and thus emphasizes the need for continued efforts to improve drug therapy especially in people with dementia.
ACKNOWLEDGMENTS
All researchers were independent of the funding source and declare no support for any organization for the submitted work. The Danish Dementia Research Centre is supported by grants from the Danish Ministry of Health (file no. 2007-12143-112/59506, file no. 1604063, and file no. 0901110/34501). CG was funded by an independent research grant of the Alfred Benzon Foundation, Denmark.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-0627r2).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-200627.
REFERENCES
[1] | Fialová D , Laffon B , Marinković V , Tasić L , Doro P , Sóos GO , Mota J , Dogan S , Brkić J , Teixeira JP , Valdiglesias V , Costa S ((2019) ) Medication use in older patients and age-blind approach: Narrative literature review (insufficient evidence on the efficacy and safety of drugs in older age, frequent use of PIMs and polypharmacy, and underuse of highly beneficial nonpharmacological strat. Eur J Clin Pharmacol 75: , 451–466. |
[2] | Mangin D , Bahat G , Golomb BA , Mallery LH , Moorhouse P , Onder G , Petrovic M , Garfinkel D ((2018) ) International Group for Reducing Inappropriate Medication Use & Polypharmacy (IGRIMUP): Position statement and 10 recommendations for action. Drugs Aging 35: , 575–587. |
[3] | Spinewine A , Schmader KE , Barber N , Hughes C , Lapane KL , Swine C , Hanlon JT ((2007) ) Appropriate prescribing in elderly people: How well can it be measured and optimised? Lancet 370: , 173–184. |
[4] | American Geriatrics Society 2015 Beers Criteria Update Expert Panel ((2015) ) American Geriatrics Society 2015 Updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 63: , 2227–2246. |
[5] | American Geriatrics Society Beers Criteria® Update Expert Panel ((2019) ) American Geriatrics Society 2019 Updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc 67: , 674–694. |
[6] | Danish Institute for Rational Pharmacotherapy (2011) Rød-gul-grøn listen (red-yellow-green list). |
[7] | Pérez T , Moriarty F , Wallace E , McDowell R , Redmond P , Fahey T ((2018) ) Prevalence of potentially inappropriate prescribing in older people in primary care and its association with hospital admission: Longitudinal study. BMJ 363: , k4524. |
[8] | Hyttinen V , Taipale H , Tolppanen A-M , Tanskanen A , Tiihonen J , Hartikainen S , Valtonen H ((2017) ) Incident use of a potentially inappropriate medication and hip fracture in community-dwelling older persons with Alzheimer’s disease. Ann Pharmacother 51: , 725–734. |
[9] | Hyttinen V , Jyrkkä J , Saastamoinen LK , Vartiainen AK , Valtonen H ((2019) ) The association of potentially inappropriate medication use on health outcomes and hospital costs in community-dwelling older persons: A longitudinal 12-year study. Eur J Heal Econ 20: , 233–243. |
[10] | Veronese N , Stubbs B , Noale M , Solmi M , Pilotto A , Vaona A , Demurtas J , Mueller C , Huntley J , Crepaldi G , Maggi S ((2017) ) Polypharmacy is associated with higher frailty risk in older people: An 8-year longitudinal cohort study. J Am Med Dir Assoc 18: , 624–628. |
[11] | Clague F , Mercer SW , McLean G , Reynish E , Guthrie B ((2017) ) Comorbidity and polypharmacy in people with dementia: Insights from a large, population-based cross-sectional analysis of primary care data. Age Ageing 46: , 33–39. |
[12] | Kojima G , Liljas A , Iliffe S , Walters K ((2017) ) Prevalence of frailty in mild to moderate Alzheimer’s disease: A systematic review and meta-analysis. Curr Alzheimer Res 14: , 1256–1263. |
[13] | Hayes TL , Larimer N , Adami A , Kaye JA ((2009) ) Medication adherence in healthy elders: Small cognitive changes make a big difference. J Aging Health 21: , 567–580. |
[14] | Gustafsson M , Sjolander M , Pfister B , Jonsson J , Schneede J , Lovheim H ((2016) ) Drug-related hospital admissions among old people with dementia. Eur J Clin Pharmacol 72: , 1143–1153. |
[15] | Delgado J , Bowman K , Clare L ((2020) ) Potentially inappropriate prescribing in dementia: A state-of-the-art review since 2007. BMJ Open 10: , e029172. |
[16] | Kristensen RU , Nørgaard A , Jensen-Dahm C , Gasse C , Wimberley T , Waldemar G ((2018) ) Polypharmacy and potentially inappropriate medication in people with dementia: A nationwide study. J Alzheimers Dis 63: , 383–394. |
[17] | Pugh MJV , Hanlon JT , Wang C-P , Semla T , Burk M , Amuan ME , Lowery A , Good CB , Berlowitz DR ((2011) ) Trends in use of high-risk medications for older veterans: 2004 to 2006. J Am Geriatr Soc 59: , 1891–1898. |
[18] | Zimmermann T , Kaduszkiewicz H , van den Bussche H , Schon G , Brettschneider C , Konig H-H , Wiese B , Bickel H , Mosch E , Luppa M , Riedel-Heller S , Werle J , Weyerer S , Fuchs A , Pentzek M , Hanisch B , Maier W , Scherer M , Jessen F ((2013) ) [Potentially inappropriate medication in elderly primary care patients: A retrospective, longitudinal analysis]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 56: , 941–949. |
[19] | Hovstadius B , Petersson G , Hellstrom L , Ericson L ((2014) ) Trends in inappropriate drug therapy prescription in the elderly in Sweden from 2006 to 2013: Assessment using national indicators. Drugs Aging 31: , 379–386. |
[20] | Davidoff AJ , Miller GE , Sarpong EM , Yang E , Brandt N , Fick DM ((2015) ) Prevalence of potentially inappropriate medication use in older adults using the 2012 Beers criteria. J Am Geriatr Soc 63: , 486–500. |
[21] | Gustafsson M , Sandman PO , Karlsson S , Isaksson U , Schneede J , Sjolander M , Lovheim H ((2015) ) Reduction in the use of potentially inappropriate drugs among old people living in geriatric care units between 2007 and 2013. Eur J Clin Pharmacol 71: , 507–515. |
[22] | Jirón M , Pate V , Hanson LC , Lund JL , Jonsson Funk M , Stürmer T ((2016) ) Trends in prevalence and determinants of potentially inappropriate prescribing in the United States: 2007 to 2012. J Am Geriatr Soc 64: , 788–797. |
[23] | Thorell K , Midlöv P , Fastbom J , Halling A ((2020) ) Use of potentially inappropriate medication and polypharmacy in older adults: A repeated cross-sectional study. BMC Geriatr 20: , 73. |
[24] | Lynge E , Sandegaard JL , Rebolj M ((2011) ) The Danish National Patient Register. Scand J Public Health 39: , 30–33. |
[25] | Mors O , Perto GP , Mortensen PB ((2011) ) The Danish Psychiatric Central Research Register. Scand J Public Health 39: , 54–57. |
[26] | Kildemoes HW , Sorensen HT , Hallas J ((2011) ) The Danish National Prescription Registry. Scand J Public Health 39: , 38–41. |
[27] | Pedersen CB ((2011) ) The Danish Civil Registration System. Scand J Public Health 39: , 22–25. |
[28] | Salem LC , Andersen BB , Nielsen TR , Stokholm J , Jorgensen MB , Rasmussen MH , Waldemar G ((2012) ) Overdiagnosis of dementia in young patients - a nationwide register-based study. Dement Geriatr Cogn Disord 34: , 292–299. |
[29] | Phung TK , Andersen BB , Hogh P , Kessing LV , Mortensen PB , Waldemar G ((2007) ) Validity of dementia diagnoses in the Danish hospital registers. Dement Geriatr Cogn Disord 24: , 220–228. |
[30] | Charlson ME , Pompei P , Ales KL , MacKenzie CR ((1987) ) A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis 40: , 373–383. |
[31] | Danish Institute for Rational Pharmacotherapy (2016) Rød-gul-grøn listen (red-yellow-green list) 2nd edition. |
[32] | Wang PS , Schneeweiss S , Avorn J , Fischer MA , Mogun H , Solomon DH , Brookhart MA ((2005) ) Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med 353: , 2335–2341. |
[33] | Danish Health and Medicines authority (2004) Indskærper landets læger at udvise stor forsigtighed ved behandling med atypiske antipsykotika til ældre patienter med demens [Danish]. |
[34] | FDA (2008) Information for Healthcare Professionals: Conventional Antipsychotics. |
[35] | Banerjee S (2009) The use of antipsychotic medication for people with dementia: Time for action. Department of Health. |
[36] | Norgaard A , Jensen-Dahm C , Gasse C , Hansen HV ((2015) ) Time trends in antipsychotic drug use in patients with dementia: A nationwide study. J Alzheimers Dis 49: , 211–220. |
[37] | Stuart B , Kamal-Bahl S , Briesacher B , Lee E , Doshi J , Zuckerman IH , Verovsky I , Beers MH , Erwin G , Friedley N ((2003) ) Trends in the prescription of inappropriate drugs for the elderly between 1995 and 1999. Am J Geriatr Pharmacother 1: , 61–74. |
[38] | Carey IM , De Wilde S , Harris T , Victor C , Richards N , Hilton SR , Cook DG ((2008) ) What factors predict potentially inappropriate primary care prescribing in older people? Analysis of UK primary care patient record database. Drugs Aging 25: , 693–706. |
[39] | Bongue B , Naudin F , Laroche M-L , Galteau M-M , Guy C , Gueguen R , Convers J-P , Colvez A , Maarouf N ((2009) ) Trends of the potentially inappropriate medication consumption over 10 years in older adults in the East of France. Pharmacoepidemiol Drug Saf 18: , 1125–1133. |
[40] | Price SD , Holman CDJ , Sanfilippo FM , Emery JD ((2014) ) Are older Western Australians exposed to potentially inappropriate medications according to the Beers Criteria? A 13-year prevalence study. Australas J Ageing 33: , E39–48. |
[41] | Moriarty F , Hardy C , Bennett K , Smith SM , Fahey T ((2015) ) Trends and interaction of polypharmacy and potentially inappropriate prescribing in primary care over 15 years in Ireland: A repeated cross-sectional study. BMJ Open 5: , e008656. |
[42] | Ble A , Masoli JAH , Barry HE , Winder RE , Tavakoly B , Henley WE , Kuchel GA , Valderas JM , Melzer D , Richards SH ((2015) ) Any versus long-term prescribing of high risk medications in older people using 2012 Beers Criteria: Results from three cross-sectional samples of primary care records for 2003/4, 2007/8 and 2011/12. BMC Geriatr 15: , 146. |
[43] | Bruin-Huisman L , Abu-Hanna A , van Weert HCPM , Beers E ((2017) ) Potentially inappropriate prescribing to older patients in primary care in the Netherlands: A retrospective longitudinal study. Age Ageing 46: , 614–619. |
[44] | FDA U.S. Food and Drug Administration (2015) FDA Drug Safety Communication: FDA strengthens warning that non-aspirin nonsteroidal anti-inflammatory drugs (NSAIDs) can cause heart attacks or strokes. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-strengthens-warning-non-aspirin-nonsteroidal-anti-inflammatory |
[45] | O’Mahony D , O’Sullivan D , Byrne S , O’Connor MN , Ryan C , Gallagher P ((2015) ) STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 44: , 213–218. |
[46] | Alzheimer’s Association (2013) Managing behavioral and psychological symptoms of dementia (BPSD). |
[47] | National Institute for Health and Care Excellence (2018) Dementia: Assessment, management and support for people living with dementia and their carers. Grants Regist 2019, 540. |
[48] | Sundhedsstyrelsen (2019) National klinisk retningslinje for forebyggelse og behandling af adfærdsmæssige og psykiske symptomer hos personer med demens. |
[49] | Johnell K , Fastbom J , Rosen M , Leimanis A ((2007) ) Inappropriate drug use in the elderly: A nationwide register-based study. Ann Pharmacother 41: , 1243–1248. |
[50] | Tommelein E , Mehuys E , Petrovic M , Somers A , Colin P , Boussery K ((2015) ) Potentially inappropriate prescribing in community-dwelling older people across Europe: A systematic literature review. Eur J Clin Pharmacol 71: , 1415–1427. |
[51] | Kristensen RU , Nørgaard A , Jensen-Dahm C , Gasse C , Wimberley T , Waldemar G ((2019) ) Changes in the prevalence of polypharmacy in people with and without dementia from 2000 to 2014: A nationwide study. J Alzheimers Dis 67: , 949–960. |
[52] | Renom-Guiteras A , Thürmann PA , Miralles R , Klaaßen-Mielke R , Thiem U , Stephan A , Bleijlevens MHC , Jolley D , Leino-Kilpi H , Hallberg IR , Saks K , Soto-Martin M , Zabalegui A , Meyer G , Sauerland D , Wuebker A , Bremer P , Hamersb JPH , Afram B , Beerens HC , Verbeek H , Zwakhalen SMG , Ruwaard D , Ambergen T , Emilsson UM , Karlsson S , Bokberg C , Lethin C , Challis D , Sutcliffe C , Tucker S , Bowns I , Roe B , Burns A , Koskenniemi J , Suhonen R , Viitanen M , Arve S , Stolt M , Hupli M , Tiit EM , Leibur J , Raamat K , Armolik A , Toivari TTM , Navarro M , Cabrera E , Risco E , Alvira C , Farré M , Miguel S , Soto M , Milhet A , Sourdet S , Gillette S , Vellas B ((2018) ) Potentially inappropriate medication among people with dementia in eight European countries. Age Ageing 47: , 68–74. |
[53] | Jensen-Dahm C , Christensen AN , Gasse C , Waldemar G ((2020) ) The use of opioids and antipsychotics in elderly with dementia-have opioids replaced antipsychotics in treating behavioral symptoms in dementia? J Alzheimers Dis 73: , 259–267. |
[54] | Alzheimer Europe (2020) Dementia in Europe Yearbook 2019. |

