
Dementia Care in Times of COVID-19: Experience at Fundació ACE in Barcelona, Spain
Abstract
Background:
Fundació ACE is a non-profit organization providing care based on a holistic model to persons with cognitive disorders and their families for 25 years in Barcelona, Spain. Delivering care to this vulnerable population amidst the COVID-19 pandemic has represented a major challenge to our institution.
Objective:
To share our experience in adapting our model of care to the new situation to ensure continuity of care.
Methods:
We detail the sequence of events and the actions taken within Fundació ACE to swiftly adapt our face-to-face model of care to one based on telemedicine consultations. We characterize individuals under follow-up by the Memory Unit from 2017 to 2019 and compare the number of weekly visits in 2020 performed before and after the lockdown was imposed.
Results:
The total number of individuals being actively followed by Fundació ACE Memory Unit grew from 6,928 in 2017 to 8,147 in 2019. Among those newly diagnosed in 2019, most patients had mild cognitive impairment or mild dementia (42% and 25%, respectively). Weekly visits dropped by 60% following the suspension of face-to-face activity. However, by April 24 we were able to perform 78% of the visits we averaged in the weeks before confinement began.
Discussion:
We have shown that Fundació ACE model of care has been able to successfully adapt to a health and social critical situation as COVID-19 pandemic. Overall, we were able to guarantee the continuity of care while preserving the safety of patients, families, and professionals. We also seized the opportunity to improve our model of care.
INTRODUCTION
Over nearly 25 years, Fundació ACE, a private non-profit organization focused on cognitive disorders and dementia, has been providing care to these individuals based on a holistic approach [1]. This is a patient-centered model, that integrates both the patients and their circumstances, which play a key role in the patient’s health and in the evolution of the disease. While this is true for most ailments, the importance of the patient’s environment in Alzheimer’s disease (AD) is paradigmatic. According to this model, besides the patient there are at least three additional dimensions being considered: 1) the caregiver and families, 2) the patient’s socio-economic conditions, and 3) the team of professionals providing care. Thus, interventions are centered in the patient but also involve these other dimensions. Additionally, this model applies the concept of relational intelligence, based on the relationship between health professionals, patients, and their families, with the objective to obtain a more accurate diagnosis, one that not only takes into account cognition but also social, emotional, and behavioral aspects, and the most appropriate, tailored-made approach to care. From the very beginning, Fundació ACE evolved an organizational structure to meet the needs of patients, families, professionals, and researchers, and to respond to changes in such needs over time [2]. Over this period nearly 30,000 patients have benefited from this holistic and multidisciplinary model of care.
The recent advent of the COVID-19 pandemic has produced profound changes in our lives in an extremely short period of time. Catalonia in general and particularly the metropolitan area of Barcelona (where Fundació ACE is located) is among the hardest hit world regions by the disease with more than 500 officially confirmed COVID-related deaths per million people [3, 4]. The real impact of the outbreak is likely to surpass these estimates, especially among the elderly, as many of them have not received hospital care and have died at home or in long-term care facilities without diagnostic tests being performed [5, 6], especially at the beginning of the outbreak. In fact, if we compare the number of deaths during the outbreak in Spain with the number of deaths expected for this part of the year based on data from previous years [7], we find that the estimated number of excess deaths is 30,864 (close to 20% higher than the official estimates). Furthermore, most of excess deaths occurred among those 65 years and older (n = 29405; 95%). In fact, while observed deaths during the outbreak exceeded in 67% those expected for patients above 74 years of age, this excess was only 17% for those below 65 years. These data confirm that the impact of the pandemic was greatest among the elderly [8]. Furthermore, in order to control the outbreak, authorities in Spain and in most countries around the world adopted preventive measures, such as confinement strategies, that involved suspending academic activities, closure of public spaces, and non-essential businesses, and imposing severe restrictions to non-essential people’s movements. Such measures of social isolation have a great impact on the elderly, and could aggravate the quality of life of the cognitively-impaired patients, resulting in the worsening of their medical condition due to their inability to have medical check-ups [9].
Such changes occurred abruptly and affected patients and their surrounding environment. Fundació ACE’s model is dynamic by nature and, therefore, able to overcome the challenges that emerge in situations such as this pandemic. In this case, Fundació ACE adapted its protocols according to the events to better accommodate patients in this new scenario to ensure continuity of care.
The aim of this manuscript is to share our experiences in dealing with this major challenge, and with the unexpected disruption of the normality of the health system, caused by the outbreak and its consequences. We also describe the way our model rapidly evolved from being mainly face-to-face-based to embrace telemedicine, and the outcomes of this transition.
METHODS
Fundació ACE
Fundació ACE opened its Memory Clinic in 1996 with the goal of addressing the increasing demand for treatment and education of individuals with dementia and their families. The structure and nature of our organization and the underlying model of care is described to great detail elsewhere [2]. Briefly, Fundació ACE is a non-profit organization that mainly provides services to the public health system of Catalonia, meeting the International Alzheimer’s Plans recommendations [10–12]. Currently the staff comprises 95 professionals organized in different units: a) Memory Unit: A referral center receiving patients from districts of greater Barcelona City, supported by the Catalan Health Service, Department of Health. The Memory Unit includes neurologists, geriatricians, neuropsychologists, social workers, nurses, and clinical and technical staff, providing comprehensive assessment for diagnosis and follow up by this multidisciplinary team under a patient centered holistic model of care (Supplementary Material 1); b) Day care Unit: This unit serves as an alternative to hospitalization or institutionalization, and has a daycare facility for people with late-onset dementia, as well as a day hospital for people with early-onset dementia. Services provided are intended to enhance, preserve, and promote the autonomy of patients in their basic activities of daily living and to reduce caregiver burden, through a personalized comprehensive psychoestimulation program (Integrated Psychostimulantion Program, IPP) [13, 14], interactive multimedia tools (e.g., Smartbrain) [15] and music and choreography therapy [16]. The Unit includes a medical director, an assistant manager, a center coordinator, a hospital coordinator, neurologists, a geriatrician, neuropsychologists, psychologists, social workers, nurses, clinical assistants, occupational and physical therapists; c) Clinical Trials Unit that carries out studies sponsored by the pharmaceutical industry with a team of that includes a neurologist, study and logistics coordinators, research nurses, a pharmacist and a neuropsychologist. Their facilities comprise a nurse station, hospital beds, recovering room, and one positive-pressure room; d) Research Unit: Devoted to in-house research projects and collaborations with other research centers, with special focus on omics, clinical, neuropsychological, and ethical-social research. The team includes bioinformaticians, molecular biologists, geneticists, neurologists, psychologists, a physicist, and laboratory technicians.
Context
From early February 2020 we were in contact with the Department of Labor, Social Affairs and Family, and the Catalan Health Service, Department of Health, and followed their instructions regarding the COVID-19 outbreak. The first confirmed positive case of SARS-CoV-2 infection in Barcelona was reported on February 25 [17]. On March 11, the World Health Organization characterized COVID-19 as a world pandemic [18]. As the outbreak gained momentum in Spain, authorities declared the state of alarm on March 14 [19]. This decree secured the lockdown of non-essential activities and imposed severe restrictions to people’s movements.
Preliminary actions
The highest priority of Fundación ACE was to guarantee the protection, prevention, and safety of both our professionals and the people we care for and to guarantee the continuity of care for people and families with the provision of our services.
During the weeks prior to the state of alarm we took the following actions. First, we established and communicated prevention and protection measures against this disease among our professionals as well as health education measures that targeted our specific population. Second, we developed a contingency plan, and initiated organizational and logistic measures to progressively reduce activity anticipating the evolution of the outbreak. Thus, the Day Care Unit advised families that patients could not attend the center in case of symptoms, and that in the likely event of closure they should reorganize their daily activities for an unknown period of time. Similarly, the Memory Unit reduced its activity by not scheduling new first appointments and by not replacing those that were cancelled. At the same time the Clinical Trial Unit suspended the recruitment of new participants. Third, we provided all facilities within Fundació ACE with the protective equipment and the operating procedures in the event of a suspected case of COVID-19.
Actions after lockdown
On March 16, 2020, following the instructions of the Government of Catalonia, we proceeded to close the Day Care Unit and to stop face-to-face activity of the Memory Unit. At this point, the essence of our model of care, and our commitment to patients, families, and staff led us to perform a record-time transition from a face-to-face to a telemedicine model by implementing our contingency plan.
The objectives of this plan were: a) Safety: preserve safety of people, including professionals, people we care for, and indirectly also all society, b) Continuity of care: guarantee the continuity of care with the will to serve people, covering the needs of our patients and their families adapting our holistic care model process to the new reality, c) Ethical responsibility: once the previous two goals are fulfilled, we should attempt to go further and add positive value to what we already did before, living up to our ethical responsibility with the community.
Management positions and administrative staff at Fundació ACE (i.e., communication, administration, general services, information systems), continued office-based activity until Friday, March 20, 2020, to roll out the contingency plan. The most immediate action was to ensure that Fundació ACE professionals could safely and effectively deliver care while home-based. This included procurement of software and hardware, as well as establishing a health monitoring protocol for all staff. Work meetings to coordinate activities were programmed.
In order to guarantee the continuity of care to patients and their families several milestones were met within days. We habilitated secure remote access to medical records through a virtual private network (VPN). We migrated from a face-to-face model of care to one mainly based on telemedicine, in an adaptive and individualized manner so no one was left behind. Thus, depending on available resources on the patients’ side, we began doing consultations using videoconference platforms such as WhatsApp, Skype, Teams, or Facetime. If videoconference was not possible, we could alternatively have these consultations over the phone. We adapted the neurological, neuropsychological, and social assessment protocols to be performed by videoconference (Supplementary Material 2), and evaluated how professionals at Fundació ACE viewed this rapid transition to telemedicine by using a recently validated questionnaire [20]. We aimed to maintain scheduled activities as far as possible and developed new support and health education materials for this crisis time. We monitored the health status of all 190 patients from the Day Care Unit through daily phone contacts using an ad-hoc health checklist. We opened a registry with all patients from the Day Care and the Memory Units (ascertained during visits) with a positive SARS-CoV-2 test result or with compatible COVID-19 symptoms but not tested. Following the plan, the Clinical Trials Unit suspended temporarily all treatments. We analyzed individually the situation of each trial with sponsors to find optimal ways of handling the new scenario that guaranteed the safety of patients without compromising the validity of the results of these trials by adapting protocols to this exceptional circumstance aligned with regulatory agencies. In this respect, we performed weekly calls to all 133 active clinical trial participants to monitor their health and established a specific circuit to manage trial adverse events and suspected COVID-19 situations. To comply with confinement regulations, courier service was used to deliver study medication when required. Simultaneously, all academic clinical sessions, continuing education, as well as all intramural administrative or clinical activities were migrated to online platforms.
In order to guarantee its sustainability, the plan also sought ways to minimize the financial impact of the inevitable reduction in activity and income. This included a temporary suspension in Day Care Unit jobs related to services that cannot be provided online, and the activation of a flexible working schedule system.
The plan also established the importance of visibility and communication of all these changes. To this end, we posted regular press releases in the web of Fundació ACE [21] and social networks and maintained close communication with families of Day Care Unit users. The distribution of support and health education material was also prioritized as well promoting the position of Alzheimer’s Europe in defense of the rights of people with dementia, endangered in this crisis times [22].
Statistical methods
We describe the number of patients being followed up in Fundació ACE Memory Unit in the three years prior to the pandemic (i.e., since 2017). We report separately the number of new and follow-up patients by year and type of diagnosis.
We compared the number of weekly visits (by type) performed in 2020 starting the first full week of January (January 6-10) through week 16 (April 20-24). Note that from the declaration of the state of alarm (effective from week 11, which corresponds to March 16-20) all consultations were virtual using available tools. To weigh the consequences of the outbreak on the activity of the Memory Unit, we estimated the average number of visits by type before the state of alarm declaration (weeks 1-10) and compared these estimates with the observed number of weekly visits afterwards (weeks 11-16). Furthermore, we provide details on scheduled visits on week 16 to describe reported causes for not doing these virtual consultations and the tools used among those performed.
RESULTS
The number of patients being actively followed in the Memory Unit at Fundació ACE has been steadily increasing ever since it was first established almost 25 years ago [2]. In the last three years, the total number of patients evaluated grew from 6,928 in 2017, to 7,415 in 2018, and 8,147 in 2019 with average yearly increases close to 9%. In the same period, the number of new patients, who receive a first full clinical evaluation, grew from 1,708 in 2017 to 1,998 in 2019 (average yearly increase of 8.5%). Overall, the number of consultations (including visits with social workers, neuropsychologist, and neurologist/geriatrician) grew from 29,273 in 2017 to 30,719 in 2019 that correspond to roughly 4 visits per patient each year. As shown in Table 1, among all patients on active follow-up with a final diagnosis during 2019, 61% (n = 4,494) of them had dementia, 32% (n = 2,357) had cognitive impairment without dementia (i.e., mild cognitive impairment), and 7% (n = 531) had no signs of cognitive impairment (mainly subjective memory complaints). As expected, the proportion of patients with mild cognitive impairment was quite higher among new patients. Thus, in 2019 a total of 862 new patients (42%) were diagnosed with mild cognitive impairment, compared to 907 diagnosed with dementia (45%). Notably, among those with dementia, most of them (n = 517; 57%) were at an early stage of the disease (i.e., very mild, or mild dementia; CDR≤1).
Table 1
New and follow-up patients seen in Fundació ACE during 2019 by diagnosis
| New patients | Follow-up patients | Total | ||||
| Diagnosis | N | % | N | % | N | % |
| No cognitive impairment | 262 | 13% | 269 | 5% | 531 | 7% |
| Mild cognitive impairment | 862 | 42% | 1495 | 28% | 2357 | 32% |
| Dementia | 907 | 45% | 3587 | 67% | 4494 | 61% |
| Alzheimer’s disease | 700 | 77% | 2658 | 74% | 3358 | 75% |
| Lewy bodies and Parkinson’s disease | 63 | 7% | 224 | 6% | 287 | 6% |
| Frontotemporal lobar dementia | 20 | 2% | 107 | 3% | 127 | 3% |
| Cerebral vascular disease | 95 | 10% | 481 | 13% | 576 | 13% |
| Dementia due to other entities | 29 | 3% | 117 | 3% | 146 | 3% |
| All | 2031 | 5351 | 7382 | |||
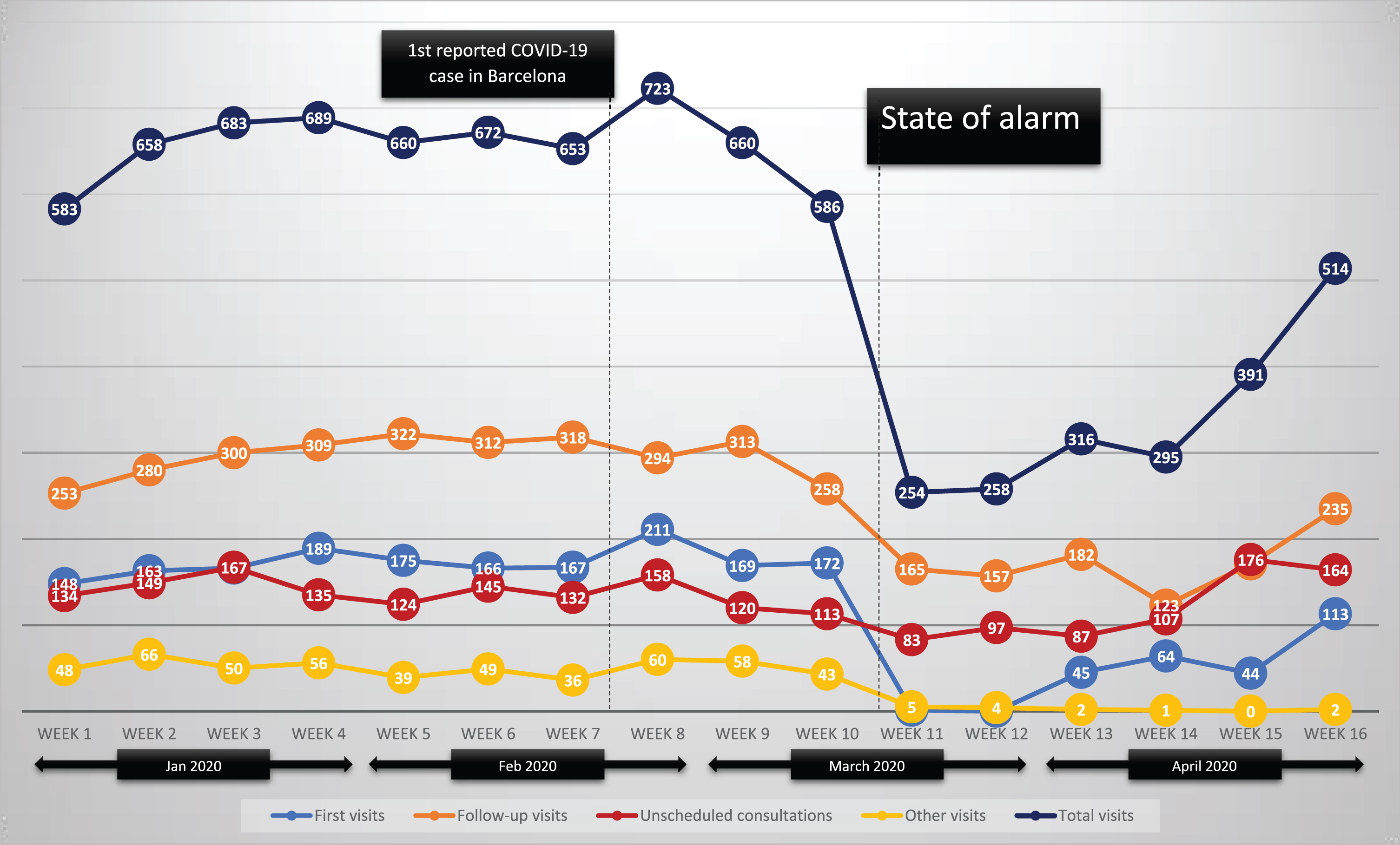
Every week the Memory Unit at Fundació ACE performs between 600 and 700 patient appointments. During the weeks before mandatory confinement measures were established, the number of weekly visits ranged from 583 to 723 (Fig. 1). Almost half of them were scheduled follow-up visits of patients and families. First visits and on-demand consultations accounted for one quarter of all visits each. A small number of remaining visits correspond mainly to ongoing observational research projects. After the state of alarm was declared, there was a sudden drop in the total number of visits. Then, these appointments were no longer face-to-face but became telemedicine consultations. The distribution by type of visit changed following the suspension of first visits during the initial weeks of the confinement. Thus, follow-up visits accounted for almost two-thirds of all visits, while on-demand unscheduled visits accounted for the remaining one-third. In absolute terms, visits dropped from an average of 657 weekly visits in the first ten weeks of 2020, to 254 visits in the first week after the state of alarm was declared (i.e., a drop of 60%). This drop was of 44% for follow-up visits and of 40% for on demand consultations. By week 13, we had already resumed first visits in the new telemedicine format, and that week we managed to complete 45 of them, that represent 26% of the number of first visit we did on an average week before the outbreak (mean = 173). By week 16, we were already doing a 65% of the average number of first visits. The evolution of on demand consultations shows that after the initial decrease, these visits increased gradually and by week 15, we reached 176 visits, 28% more visits of this type than we recorded on an average week before the outbreak (mean = 138). Overall, by week 16 the total number of visits (n = 514; 78%) was quickly converging with the expected number of visits before the outbreak (mean = 657).
Fig.1
Weekly visits during 2020 by type.
According to additional information collected on scheduled visits for week 16 (see Table 2), we were able to perform 350 out of the 475 scheduled visits (74%). Of note only 26 scheduled visits were cancelled due to lack of patients’ telecommunications devices (5%). Among scheduled visits that were conducted, videoconferencing was used in 71%, compared to 29% over a regular telephone call. The most frequent teleconference application used was Whatsapp (86%), followed by Skype (12%), and Facetime (2%).
Table 2
Details of scheduled visits from week 16 (April 20-24)
| N | % | |
| Not performed | 125 | 26% |
| Family decides to wait for face to face visit | 58 | 46% |
| Professional team cancels because of social and clinical conditions | 20 | 16% |
| Lack of telecommunication devices | 26 | 21% |
| Exitus | 16 | 13% |
| Other | 5 | 4% |
| Performed | 350 | 74% |
| Videoconference | 249 | 71% |
| 214 | 86% | |
| Skype | 29 | 12% |
| Facetime | 5 | 2% |
| Google DUO | 1 | 0% |
| Telephone call | 101 | 29% |
| Total scheduled visits | 475 |
We sent a short, validated questionnaire to 20 neurologists, neuropsychologists, and social workers from Fundació ACE to evaluate their experience with telemedicine during this crisis. We obtained responses from 16 of them and found that 81% of them considered the quality of telemedicine consultations to be either good or excellent. Furthermore 75% viewed telemedicine visits as equal or better than face-to-face consultations.
By the time this manuscript was drafted, the number of patients from the Day Care Unit with a positive SARS-CoV-2 test result or COVID-19 compatible symptoms was 7 out of 190 (3 of them deceased). Among patients from the Memory Unit, we have recorded 77 with a positive SARS-CoV-2 test result or probable case (34 of them deceased).
DISCUSSION
We have shown that Fundació ACE model of care has been able to successfully adapt to a health and social critical situation as COVID-19 pandemic. The current scenario has proven to be stressful for our institution, due to the uncertainty and the ever-changing conditions on a day-to-day basis. However, our institution’s resilience, not resistance, was able to effectively respond to these challenges.
We have met the objectives, transitioning in a matter of days from a traditional face-to-face approach to a telemedicine-based approach in which care is provided by a network of fully coordinated multidisciplinary team of professionals. Other organizations facing the same challenge during this pandemic have also relied on telemedicine to provide continuous care with positive results [23–25]. In our case, there are several critical factors that contributed to this success. Firstly, the commitment to a holistic model of care which involves not only the patients but also their families and their social context, as well as the emotional well-being of professionals involved. Secondly, we have an outstanding team of professionals that was able to understand the importance of their full implication in this crisis time. And thirdly, we designed a detailed contingency plan that guided our actions throughout this process. Overall, we have been able to preserve people’s safety, to guarantee continuity of care during these difficult times, and to improve in many ways our model of care.
Our results show that after an initial dip, activity in the Memory Unit was able to reach 78% of regular activity within six weeks (by April 24) showing a trend to reach an acceptable normality.
At the time of publication of this paper, the outbreak has now been successfully controlled in Spain and, as result, confinement measures have started to be gradually lifted. Notably, restrictions on mobility have been relaxed and individuals may now leave their homes. However, the pace of this four-staged deconfinement process is not homogeneous. In the metropolitan areas of Barcelona and Madrid, the most densely populated in Spain and the hardest hit, the pace is being slower than in other regions. Thus, we expect to be able resume face-to-face visits in the Memory Unit sometime in June as the best-case scenario. Furthermore, it is unlikely that we will return to normality afterwards since some type of social distancing rules will remain as long as no effective treatment against COVID-19 is available. Meanwhile, the Memory Unit at Fundació ACE continues its path towards normal activity mainly via telemedicine consultations.
One of the goals of our ambitious contingency plan was not only to simply provide the same type of care adapted to the new tools, but also to seize the opportunity to further improve this care. Along those lines, we should highlight the increase of the number of consultations without an appointment. The latter clearly relates to the critical situation and the increased need of patients and families to be assisted during the lockdown, but also to the extended availability provided generously by the team of professionals at Fundació ACE during this period.
Moreover, most patients and their families provided positive feedback about being able to attend scheduled visits while they were confined. Once we have successfully incorporated telemedicine to our model of care, it becomes a real option of care. This will allow patients and caregivers to choose between face-to-face (once it becomes available) or telemedicine on their convenience. In our holistic model, this translates into inclusive care. This can be especially useful to achieve continuity of care when there are temporary changes in the patient’s residence, which is not unusual during the summer season or when several family members share caregiving duties.
Inequalities in access to healthcare are common even within universal public health systems in Europe. This is a key determinant of worse health outcomes observed in rural versus urban areas [26]. If only face-to-face visits are available, the location of Fundació ACE in a large city like Barcelona hinders access to our model of care for patients living in rural areas from Barcelona and neighboring provinces within the Catalan Health Service system. The possibility of attending just a first on-site appointment, in which the lengthy initial evaluation is best carried out, and then doing regular follow-up visits though videoconference leads to quality care of dementia in rural or distant areas that currently have difficulties accessing such services. Thus, the “mise en scène” of telemedicine might be the single most positive consequence of COVID-19 pandemic.
However, we have also found that some patients and families are reluctant to telemedicine, and some other simply do not have the telecommunication devices needed to perform to virtual consultations. The latter does not represent an issue when these services are offered as an alternative to face-to-face visits. Nonetheless, during the pandemic, videoconferencing is the only option and that leads us to be extremely flexible in the use of tools, and to employ telephone calls when teleconferencing is not possible.
Throughout the outbreak we have also migrated our weekly continuous education sessions to online platforms. Therefore, we have been able to grant access to these sessions to professionals outside Fundació ACE. This experience has proved to be rewarding for the participating professionals and, at the same time, facilitated the exchange of various experiences and points of view, adding value to the session content. These sessions are held in Spanish or English, which paves the way to participation of colleagues from all around the globe.
Our growth mindset approach leads us to take this as an opportunity to learn from all the struggles that the COVID-19 pandemic has brought. Thus, this should not only help us be more diligent and prepared for dealing with future pandemics. We should also seize the opportunity to test our institutional resilience and innovation capacity, towards improving the way we do things. We have adapted our holistic model of caring patients and families with cognitive problems in Fundació ACE to the new circumstances efficiently and effectively. We can conclude that this experience has strengthened our model of care, helped us make improvements, and overcome our initial reluctance to leave comfort zones. We firmly believe that sharing our experience will benefit patients who suffer dementia and their families, as well as guide health policymakers and stakeholders on their strategic planning and decision making.
ACKNOWLEDGMENTS
No funding was received for this work. Other collaborators from Fundació ACE administrative department include, Idoia Ruiz, Marta Lozano, Salvador Almagro, Ma Jesús Allué, Verónica Ferrer, Charo Romero, Mercè Roca, Esther Pelejà, Ma José Castillón, Cristina Arso, and Purificación Conde.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-0547r1).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-200547.
REFERENCES
[1] | Grups de treball del consell Asesor en Psicogeriatría ((1998) ) Els trastorns cognitius i de la conducta en l’atenció sociosanitària. Pla de Salut. Quadern 10., Barcelona. |
[2] | Boada M , Tárraga L , Hernández I , Valero S , Alegret M , Ruiz A , Lopez OL , Becker JT ((2014) ) Design of a comprehensive Alzheimer’s disease clinic and research center in Spain to meet critical patient and family needs. Alzheimers Dement 10: , 409–415. |
[3] | Ministerio de Sanidad, Actualizacion 100 COVID-19, https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/Actualizacion_100_COVID-19.pdf. |
[4] | Agència de Qualitat i Avaluació Sanitàries de Catalunya (AQuAS). Generalitat de Catalunya, Dades actualitzades SARS-CoV-2, http://aquas.gencat.cat/ca/actualitat/ultimes-dades-coronavirus/. |
[5] | Grey S, Macaskill A, In shielding hospitals from COVID-19, Britain left the weakest exposed, https://www.reuters.com/investigates/special-report/health-coronavirus-britain-elderly/. |
[6] | The Guardian, The Guardian view on the care home crisis: Culpable neglect (Editorial), https://www.theguardian.com/commentisfree/2020/apr/14/the-guardian-view-on-the-care-home-crisis-culpable-neglect. |
[7] | Instituto de Salud Carlos III, Vigilancia de los excesos de mortalidad por todas las causas. MoMo. Situacion a 4 de mayo, https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/MoMo/Documents/informesMoMo2020/MoMo_Situaciona4demayo_CNE.pdf. |
[8] | United Nations ((2020) ), Policy Brief: The Impact of COVID-19 on older persons. New York. |
[9] | Armitage R , Nellums LB ((2020) ) COVID-19 and the consequences of isolating the elderly. Lancet Public Health 5: , e256. |
[10] | Prince M , Comas-Herrera A , Knapp M , Guerchet M , Karagiannidou M ((2016) ) World Alzheimer Report 2016. Improving healthcare for people living with dementia: Coverage, quality and costs now and in the future. Alzheimer’s Disease International, London. |
[11] | Alzheimer’s Disease International ((2019) ) World Alzheimer Report 2019. Attitudes to dementia. Alzheimer’s Disease International, London. |
[12] | World Health Organization ((2017) ) Global action plan on the public health response to dementia, 2017–2025. Geneva. |
[13] | Tárraga Mestre L ((1998) ) Terapias blandas: Programa de Psicoestimulación Integral. Alternativa terapéutica para las personas con enfermedad de Alzheimer. Rev Neurol 27: , 51. |
[14] | Ibarria M , Alegret M , Valero S , Morera A , Guitart M , Cañabate P , Moreno M , Lara S , Diego S , Hernández J , Tantinyá N , Vera M , Hernández I , Becker JT , Ruíz A , Boada M , Tárraga L ((2016) ) Beneficial effects of an integrated psychostimulation program in patients with Alzheimer’s disease. J Alzheimers Dis 50: , 559–566. |
[15] | Tárraga L , Boada M , Modinos G , Espinosa A , Diego S , Morera A , Guitart M , Balcells J , López OL , Becker JT ((2006) ) A randomised pilot study to assess the efficacy of an interactive, multimedia tool of cognitive stimulation in Alzheimer’s disease. J Neurol Neurosurg Psychiatry 77: , 1116–1121. |
[16] | Bisbe M , Fuente-Vidal A , López E , Moreno M , Naya M , De Benetti C , Milà R , Bruna O , Boada M , Alegret M ((2020) ) Comparative cognitive effects of choreographed exercise and multimodal physical therapy in older adults with amnestic mild cognitive impairment: Randomized clinical trial. J Alzheimers Dis 73: , 769–783. |
[17] | La Vanguardia, Catalunya: Confirmado el primer caso de coronavirus, https://www.lavanguardia.com/vida/20200225/473782485232/coronavirus-primer-caso-cataluna.html. |
[18] | World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report – 51, https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10. |
[19] | Boleting Oficial del Estado, BOE.es - Documento BOE-A-2020-3692, https://www.boe.es/diario_boe/txt.php?id=BOE-A-2020-3692. |
[20] | Vidal-Alaball J , Mateo GF , Domingo JLG , Gomez XM , Valmaña GS , Ruiz-Comellas A , Seguí FL , Cuyàs FG ((2020) ) Validation of a short questionnaire to assess healthcare professionals’ perceptions of asynchronous telemedicine services: The Catalan version of the health optimum telemedicine acceptance questionnaire. Int J Environ Res Public Health 17: , 2202. |
[21] | Fundació ACE, COVID-19 | Fundació ACE, making Alzheimer’s history | Fundació ACE, https://www.fundacioace.com/en/covid-19.html. |
[22] | Alzheimer Europe, Triage decisions during COVID-19 pandemic - Our opinion on... - Policy - Alzheimer Europe, https://www.alzheimer-europe.org/Policy/Our-opinion-on/Triage-decisions-during-COVID-19-pandemic. |
[23] | Ousset PJ , Vellas B ((2020) ) Impact of the Covid-19 outbreak on the clinical and research activities of memory clinics: An Alzheimer’s disease center facing the Covid-19 crisis. J Prev Alzheimers Dis 7: , 197–198. |
[24] | Matías-Guiu J , Porta-Etessam J , Lopez-Valdes E , Garcia-Morales I , Guerrero-Solá A , Matias-Guiu JA ((2020) ) Management of neurological care during the COVID-19 pandemic. Neurologia 35: , 233–237. |
[25] | Hollander JE , Carr BG ((2020) ) Virtually perfect? Telemedicine for Covid-19. N Engl J Med 382: , 1679–1681. |
[26] | Baird AG , Wright N ((2006) ) Poor access to care: Rural health deprivation? Br J Gen Pract 56: , 567–568. |


