
Acute Stroke Care in Dementia: A Cohort Study from the Swedish Dementia and Stroke Registries
Abstract
Background:
Previous studies have shown that patients with dementia receive less testing and treatment for stroke.
Objectives:
Our aim was to investigate hospital management of acute ischemic stroke in patients with and without dementia.
Methods:
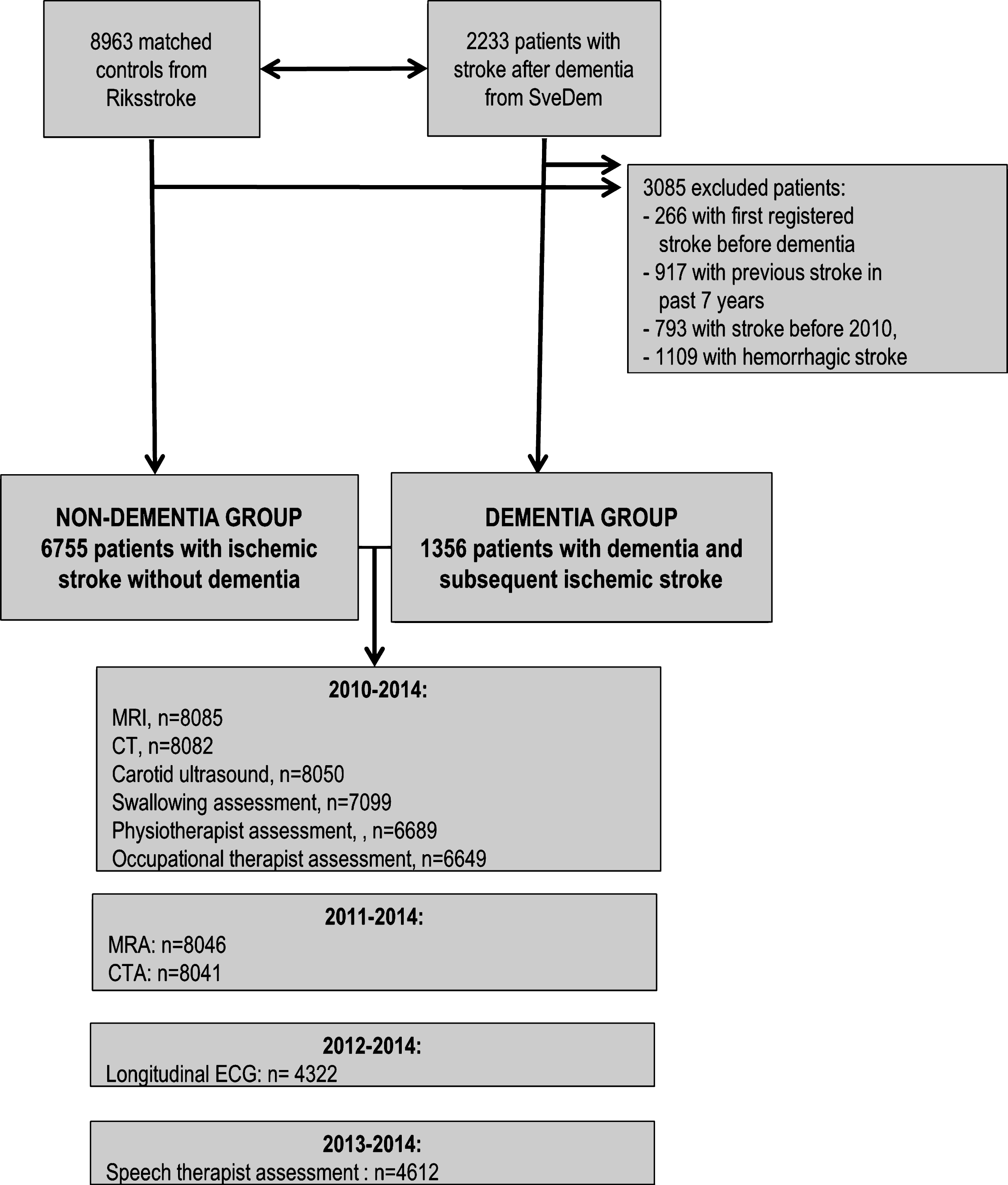
Retrospective analysis of prospectively collected data 2010–2014 from the Swedish national dementia registry (SveDem) and the Swedish national stroke registry (Riksstroke). Patients with dementia who suffered an acute ischemic stroke (AIS) (n = 1,356) were compared with matched non-dementia AIS patients (n = 6,755). Outcomes included length of stay in a stroke unit, total length of hospitalization, and utilization of diagnostic tests and assessments.
Results:
The median age at stroke onset was 83 years. While patients with dementia were equally likely to be directly admitted to a stroke unit as their non-dementia counterparts, their stroke unit and total hospitalization length were shorter (10.5 versus 11.2 days and 11.6 versus 13.5, respectively, p < 0.001). Dementia patients were less likely to receive carotid ultrasound (OR 0.36, 95% CI [0.30–0.42]) or undergo assessments by the interdisciplinary team members (physiotherapists, speech therapists, occupational therapists; p < 0.05 for all adjusted models). However, a similar proportion of patients received CT imaging (97.4% versus 98.6%, p = 0.001) and a swallowing assessment (90.7% versus 91.8%, p = 0.218).
Conclusions:
Patients with dementia who suffer an ischemic stroke have equal access to direct stroke unit care compared to non-dementia patients; however, on average, their stay in a stroke unit and total hospitalization are shorter. Dementia patients are also less likely to receive specific diagnostic tests and assessments by the interdisciplinary stroke team.
INTRODUCTION
Dementia, stroke, and limb paralysis or weakness are the three conditions which most contribute to disability and dependency worldwide [1–4]. Functional prognosis after stroke in dementia is poor [5–9] and patients with dementia are older, have more severe strokes, and more comorbidities [5, 6, 10, 11]. Pre-stroke dementia is an independent predictor of a poor functional outcome and patients with pre-stroke dementia are often treated less aggressively [5–7, 10, 12].
In the acute phase of stroke, reperfusion treatment, direct admission to a stroke unit, and prompt testing for dysphagia upon arrival to hospital have been shown to improve patient outcomes [13, 14]. In later phases, secondary pharmaceutical prevention treatment, carotid surgery, rehabilitation during and after hospitalization, and providing better psycho-social support have additionally been emphasized in Swedish guidelines [15]. Similar aspects of stroke care have been used as quality indicators in a Canadian study [7].
Hospitals may have their own predefined ‘set’ of investigations, and stroke care and its outcomes might be influenced by various factors, such as patients’ sex, age, physician’s beliefs, or even day of the week [16–18]. Clinical and radiological findings direct further investigations to determine the presumed stroke mechanism, which in turn aids to predict prognosis and optimize further preventive and treatment strategies (e.g., carotid procedure) [19].
Our aim is to evaluate hospital management of acute ischemic stroke (AIS) among Swedish patients with and without pre-existing dementia. We focus on stroke interventions, hospitalization in specialized stroke units, and performance of specific diagnostic tests.
METHODS
Study population, registries, and variables
This study cohort has been previously described in detail [5, 6]. Briefly, a longitudinal observational cohort study was performed, consisting of 1356 patients with pre-existing dementia and first AIS and 6,755 patients with first AIS and no dementia, matched in age (±3 years), sex, year of stroke, and geographic region. Patients with dementia were identified from SveDem, the Swedish national dementia registry [20], while the occurrence of AIS was identified using Riksstroke, the Swedish national registry for acute stroke, presented in detail at the Riksstroke website (http://www.riksstroke.org/eng/). Data on medication and diagnoses other than dementia were obtained from the Swedish Prescribed Drug Registry and National Patient Registry (NPR) respectively. Patients diagnosed 2010–2014 were included.
The Charlson Comorbidity Index (CCI) was calculated using NPR [21]. The Reaction Level Scale (RLS), ranging from 1 to 8, was used to assess the level of consciousness at admission to the hospital and also served as a proxy for stroke severity. Patients with RLS 1 are defined as alert (Glasgow coma scale–GCS 15), RLS 2–3 lethargic (GCS 9–14), and RLS 4–8 unconscious (GCS 3–8) [22]. Diagnostic imaging of the brain, brain vessels, or extracranial vessels consisted of variable combination of the following: 1) computerized tomography (CT); 2) magnetic resonance imaging (MRI); 3) CT angiography (CTA); 4) magnetic resonance angiography (MRA); and/or 5) ultrasound of extracranial vessels (with a focus on carotid ultrasound). The distinction between extra- and intracranial CTA was not available. Management in a stroke unit was defined as an admission to a designated ward with a multidisciplinary stroke care team.
Longitudinal electrocardiogram (ECG) monitoring is performed to discover paroxysmal arrhythmias, most commonly atrial fibrillation (AF), in patients with no previous record of them [23]. Patients with no prior AF were identified according to the NPR. Swallowing was assessed with a water swallowing bedside test. Patients in which testing was unnecessary or impossible due to their condition were excluded from the analysis.
We introduced the variable “total number of all tests” for stroke assessment and management, which is the sum of all tests performed, including CT, MRI, CTA, MRA, carotid ultrasound, longitudinal ECG, and physiotherapist, occupational therapist, speech therapist, and swallowing assessments. All tests were performed during hospitalization, except for longitudinal ECG registration, which was sometimes planned during hospitalization and performed at a later date. Data from years 2010–2014 were used, except for MRA, CTA, longitudinal ECG, and speech therapist assessment, where data was not available for the whole study period (Fig. 1).
Fig.1
Patient selection process. We used data from years 2010–2014. Where data was not available for the whole study period (MRA, CTA, longitudinal ECG, and speech therapist assessment), we used shorter time periods as indicated.
Statistical analysis
Categorical variables are presented as number of cases and percentages, and continuous variables are summarized as mean (±Standard Deviation— SD) or as median (±interquartile range— IQR). For calculating significant differences, Student’s t-test and Mann-Whitney’s U-test are used for continuous and Chi-square for categorical variables, where appropriate.
The length of stay (LOS) in a stroke unit and of the whole hospitalization (total LOS, comprising acute phase and continued hospitalization after acute phase), was analyzed using Cox regressions. These results are presented as hazard ratios (HRs) with 95% CIs. To assess the relationship between dementia status and investigations performed at hospital, multivariate logistic regression analyses were used. Adjusted odds ratios (ORs) with 95% CIs are presented. Model 1 of regression analyses is adjusted for age and sex. Model 2 is additionally adjusted for CCI and nursing home placement prior to stroke, level of consciousness, and treatment in a stroke unit. Covariates were chosen to reflect the burden of comorbidities and living situation before stroke, stroke severity, and type of hospitalization. Model 3 was adjusted for propensity scores, calculated from multiple logistic regression in which dementia status was predicted by age, sex, smoking, number of medication, antiaggregants, antipsychotics, antidepressants, lipid lowering agents, antihypertensives, AF, diabetes, hip fracture, ischemic heart disease, heart failure, renal failure, and liver failure. We conducted post-hoc sensitivity analyses in the dementia subgroup on MMSE and time from dementia diagnosis to stroke event, however, we did not include them as they were not significant in final models (results not presented).
All tests were 2-tailed with p value <0.05 considered significant. STATA® version 14 (StataCorp, College Station, TX, USA) and IBM Statistical Package for Social Sciences (IBM SPSS) for Windows, Sciences software version 23 (IBM Corporation, Armonk, NY, USA) were used.
Standard protocol approvals and patient consent
This study was approved by the regional ethical review board in Stockholm, Sweden (dnr 2015/743-31/4) and it complies with the Declaration of Helsinki. Patients and relatives were informed on at the time of registration in SveDem and/or Riksstroke and could decline participation or withdraw their information from the registries at a later date. Data were de-identified before analyses.
RESULTS
Characteristics of patients with and without dementia and acute ischemic stroke are presented in Table 1. In both groups, the median age at stroke onset was 83 years, and there was a similar proportion of women (56.3% in dementia versus 56.8% in non-dementia group, p = 0.747).
Different aspects of hospitalization are presented in Table 2. Thrombolysis was administered to 94 (7.0%) dementia and 639 (9.5%) non-dementia patients (p = 0.003). More than 99.0% of patients from both groups were hospitalized and direct admission to a stroke unit was equal (72.8% versus 72.9%, p = 0.931). However, when all hospitalizations in stroke unit were considered (both direct admission and admission at a later stage), dementia patients were less likely to be placed in a stroke unit (83.6% versus 88.5%, p < 0.001). On average, dementia patients’ LOS in a stroke unit was shorter than their non-dementia counterparts (10.5 versus 11.2, p = 0.016). We observed no significant differences in admission to other hospital wards between the two groups (observation room in the emergency department, intensive care unit, neurosurgery, other departments; p > 0.05 for all). The total LOS was 2 days shorter for dementia patients (11.6 versus 13.5, p < 0.001). LOS was associated with prior nursing home placement; the mean total LOS was 9.7 days in patients coming from a nursing home compared to 13.7 days for those without prior nursing home placement (p < 0.001), while the mean stroke unit LOS was 7.4 days in patients with and 10.2 days for those without prior nursing home placement (p < 0.001) (results not presented in a table). After stratifying for previous stroke unit placement, the difference between dementia and non-dementia patients was present only among those who were nursing home residents before stroke (p < 0.001 for total and stroke unit LOS), but not among non-nursing home residents (p = 0.337 for total LOS and p = 0.448 for stroke unit LOS).
Table 1
Characteristics of patients with and without dementia and acute ischemic stroke
| Dementia Group (n = 1,356) | Non-Dementia Group (n = 6,755) | p | |
| Age at first stroke, median (IQR) | 83 (8) | 83 (9) | 0.077 |
| Female sex | 764 (56.3) | 3838 (56.8) | 0.747 |
| Nursing home placement | 423 (31.5) | 504 (7.5) | < 0.001 |
| ADL-independence | 674 (52.8) | 5785 (87.1) | < 0.001 |
| Smoking | 54 (4.4) | 514 (8.3) | < 0.001 |
| Number of medication, median (IQR) | 6 (4) | 4 (5) | < 0.001 |
| Charlson comorbidity index, median (IQR) | 2 (2) | 1 (3) | < 0.001 |
| The Reaction Level Scale (RLS): | |||
| 1 | 1040 (78.0) | 5674 (84.9) | < 0.001 |
| 2-3 | 241 (18.1) | 771 (11.5) | < 0.001 |
| 4–8 | 52 (3.9) | 238 (3.6) | 0.544 |
| Dementia type: | |||
| Alzheimer’s dementia | 320 (23.6) | ||
| mixed dementia | 308 (22.7) | ||
| vascular dementia | 311 (22.9) | ||
| other dementias | 417 (30.8) |
Results are presented as number of cases (n) and percentage proportion (%), if not stated otherwise. In variables where n (%) are reported, p-values were obtained by chi-square, whereas in variables where median (IQR) are reported, p-values were obtained by Mann-Whitney test. The Reaction Level Scale: proxy for stroke severity measuring level of consciousness, where patients with RLS 1 are defined as alert, RLS 2–3 lethargic, and RLS 4–8 unconscious. ADL: activities of daily living; independence in mobility, dressing and toilet visits. Other dementias: dementia with Lewy bodies, frontotemporal dementia, Parkinson’s disease dementia, unspecified dementias and other dementias. Variables with missing data, n (%): nursing home placement: 42 (0.5), ADL-independence: 192 (2.4), smoking: 712 (8.8), RLS: 95 (1.2).
Table 2
Aspects of hospitalization in acute ischemic stroke in patients with and without dementia
| Number of patients | Dementia Group (n = 1356) | Non-Dementia Group (n = 6755) | p | |
| Thrombolysis | 8074 | 94 (7.0) | 639 (9.5) | 0.003 |
| Patient hospitalized | 8111 | 1344 (99.1) | 6731 (99.6) | 0.007 |
| Inhospital stroke | 8101 | 47 (3.5) | 318 (4.7) | 0.046 |
| Admitted first to another hospital | 7335 | 25 (2.1) | 253 (4.1) | 0.001 |
| Admitting hospital department | ||||
| Stroke unit | 8055 | 975 (72.8) | 4898 (72.9) | 0.931 |
| Intensive care unit | 47 (3.5) | 307 (4.6) | 0.084 | |
| Neurosurgery | 1 (0.1) | 5 (0.1) | 0.998 | |
| Observation room in the emergency department | 78 (5.8) | 356 (5.3) | 0.438 | |
| Other departments | 238 (17.8) | 1150 (17.1) | 0.565 | |
| Stroke unit admittance (direct or later) | 7850 | 1093 (83.6) | 5793 (88.5) | <0.001 |
| Continued hospitalization after acute phase | 8111 | 187 (13.8) | 1205 (17.8) | <0.001 |
| Discharged home | 7135 | 413 (35.0) | 3653 (61.6) | <0.001 |
| Length of stay (LOS): | ||||
| Total, mean±SD | 8087 | 11.6±10.9 | 13.5±13.7 | <0.001 |
| In a nursing home prior to stroke | 927a | 7.9±8.5 | 11.1±9.5 | <0.001 |
| (n = 423) | (n = 504) | |||
| Not in a nursing home prior to stroke | 7142a | 13.7±14.0 | 13.3±11.5 | 0.337 |
| (n = 921) | (n = 6221) | |||
| bIn acute care, mean±SD | 8087 | 9.5±8.8 | 10.3±10.7 | 0.001 |
| In a stroke unit, any stay, mean±SD | 6886 | 10.5±9.4 | 11.2±11.5 | 0.016 |
| In a nursing home prior to stroke | 727c | 7.8±6.9 | 9.9±9.1 | <0.001 |
| (n = 331) | (n = 396) | |||
| Not in a nursing home prior to stroke | 6144c | 11.6±10.1 | 11.3±11.7 | 0.448 |
| (n = 760) | (n = 5384) | |||
| In continued care, mean±SD | 1365 | 15.8±11.5 | 18.2±13.7 | 0.009 |
Results are presented for years 2010–2014 as number of cases (n) and percentage proportion (%), if not stated otherwise. In variables where n (%) are reported, p-values were obtained by chi-square, whereas in variables where mean and SD are reported, p-values were obtained by Student t-test. Discharged home: results are presented for survivors of hospitalization (n = 7135). Days of hospitalization in stroke unit: including patients who were subsequently transferred. Variables with missing data, n (%): thrombolysis: 37 (0.5); inhospital stroke: 10 (0.1); admitted first to another hospital: 776 (9.6); admitting hospital department: 56; (0.7); later stroke unit admittance: 261 (3.2); days of hospitalization in stroke unit: 349 (4.3); days of hospitalization, acute and altogether: 24 (0.3); discharge home: 23 (0.3); anursing home placement in total LOS: 42 (0.5), cnursing home placement in LOS in a stroke unit: 15 (0.2). bIncluding stroke unit care.
Investigations and assessments are presented in Table 3. Almost all patients received CT imaging (97.4% versus 98.6%, p = 0.001). The greatest difference between dementia and non-dementia patients was observed in the utilization of MRI, CTA, and carotid ultrasound, with smaller proportion of dementia patients receiving these investigations. Patients with dementia were also less likely to be assessed by the interdisciplinary stroke-oriented team, including physiotherapist, occupational therapist, or a speech therapist (all p≤0.001). The proportion of missing data was too high for analyses of variables on implementation of rehabilitation measures, so these data are not presented. Prior to stroke, 453 (33.4%) dementia and 1,874 (27.7%) non-dementia patients had AF (p < 0.001, results not presented in a table). Longitudinal ECG was less often completed in dementia patients during hospitalization (39.6% versus 57.6%, p < 0.001), however, when we included planned investigations after the hospitalization course, patients with dementia had more referrals and completed ECG investigations compared to non-dementia patients (97.6% versus 94.7%, p = 0.001). Overall, dementia patients received a median of 4 (IQR 2) hospital tests while non-dementia patients received a median of 5 (IQR 2). There were no differences in the frequency of swallowing assessment (90.7% versus 91.8%, p = 0.218) between the two groups.
Table 3
Investigations and assessments in hospital management of acute ischemic stroke in patients with and without dementia
| Years included | Number of patients | Dementia Group (n = 1356) | Non-Dementia Group (n = 6755) | p | |
| CT | 2010–2014 | 8082 | 1312 (97.4) | 6644 (98.6) | 0.001 |
| MRI | 2010–2014 | 8085 | 54 (4.0) | 743 (11.1) | <0.001 |
| CTA | 2011–2014 | 8041 | 107 (8.9) | 1009 (16.6) | <0.001 |
| MRA | 2011–2014 | 8046 | 6 (0.5) | 104 (1.7) | 0.002 |
| Carotid ultrasound | 2010–2014 | 8050 | 238 (17.7) | 2856 (42.6) | <0.001 |
| Longitudinal ECG – completed during hospitalization | 2012–2014 | 4322 | 268 (39.6) | 2098 (57.6) | <0.001 |
| Longitudinal ECG – completed or planned during hospitalization | 2012–2014 | 4322 | 661 (97.6) | 3453 (94.7) | 0.001 |
| Swallowing assessment | 2010–2014 | 7099 | 1060 (90.7) | 5442 (91.8) | 0.218 |
| Physiotherapist assessment | 2010–2014 | 6689 | 902 (82.8) | 4963 (88.6) | <0.001 |
| Occupational therapist assessment | 2010–2014 | 6649 | 842 (78.1) | 4763 (85.5) | <0.001 |
| Speech therapist assessment | 2013-2014 | 4612 | 223 (30.1) | 1430 (38.1) | <0.001 |
| Total number of tests, median (IQR) | 2010–2014 | 8092 | 4 (2) | 5 (2) | <0.001 |
Results are presented as number of cases (n) and percentage proportion (%), if not stated otherwise. In variables where n (%) are reported, p-values were obtained by chi-square, whereas in variables where median (IQR) are reported, p-values were obtained by Mann-Whitney test. The years for which the variables are available are reported. Total number of tests is a sum of tests reported above (CT, MRI, CTA, MRA, carotid ultrasound, and longitudinal ECG investigations, swallowing, physiotherapist, occupational therapist, and speech therapist assessments). Swallowing assessment: patients in which testing was not possible or unnecessary were excluded from the analysis. Longitudinal ECG is reported for patients with previously unknown atrial fibrillation. Variables with missing data, n (%): CT: 29 (0.4); MRI: 53 (0.7); CTA: 70 (1.0); MRA: 65 (0.9); carotid ultrasound: 61 (0.8); longitudinal ECG: 108 (1.7); swallowing assessment: 433 (5.3); physiotherapist assessment: 1422 (17.5); occupational therapist assessment: 1462 (18.0); speech therapist assessment: 114 (2.5); total number of tests: 19 (0.2).
Cox hazard regressions and logistic regression models are presented in Table 4. After adjusting for 4 possible confounders (level of comorbidity and living situation before stroke, stroke severity, and stroke unit hospitalization), patients with dementia had higher HR of faster discharge (1.11, 95% CI [1.04–1.18]), lower odds of receiving carotid ultrasound (OR 0.36, 95% CI [0.30–0.42]) and speech therapist assessment (0.70 [0.58–0.84]). On the other hand, patients with dementia were almost twice as likely to receive longitudinal ECG (1.89 [1.09–3.30]). In model 3 (propensity scores), similar trends were observed, with the exception of physiotherapist and occupational therapist assessments, where the difference between dementia and non-dementia patients was no longer present.
Table 4
Performance of investigations after stroke in patients with dementia
| Model 1 | Model 2 | Model 3 | |
| COX HAZARD REGRESSION FOR TIME TO DISCHARGE | |||
| Total days of hospitalization | 1.16 (1.09–1.23)*** | 1.11 (1.04–1.18)*** | 1.15 (1.08–1.22)*** |
| Days of hospitalization in a stroke unit | 1.06 (0.98–1.13) | 1.025 (0.95–1.10) | 1.06 (0.99–1.13) |
| LOGISTIC REGRESSION FOR RECEIVING TESTS | |||
| Hospitalization in a stroke unit | 1.0 (0.88–1.14) | 1.0 (0.91–1.21) | 1.06 (0.93–1.22) |
| Carotid ultrasound | 0.28 (0.24–0.33)*** | 0.36 (0.30–0.42)*** | 0.34 (0.29–0.39)*** |
| Longitudinal ECG | 2.22 (1.33–3.73)* | 1.89 (1.09–3.30)* | 2.02 (1.23–3.31)** |
| Speech therapist assessment | 0.70 (0.59–0.83)* | 0.70 (0.58–0.84)*** | 0.69 (0.58–0.83)*** |
| Physiotherapist assessment | 0.63 (0.53–0.75)*** | 0.80 (0.65–0.98)* | 0.94 (0.79–1.11) |
| Occupational therapist assessment | 0.61 (0.52–0.72)*** | 0.82 (0.68–0.99)* | 0.86 (0.73–1.02) |
For total days of hospitalization and days of hospitalization in a stroke unit, results are presented as hazards ratios (HRs) with 95% CI. For all other variables, results are presented as odds ratio (ORs) with 95% CI. Longitudinal ECG is reported for patients with previously unknown atrial fibrillation, either completed or planned during hospitalization. In binary logistic regression models, model 1 is adjusted for age and sex, model 2 is adjusted for age, sex, level of consciousness, treatment in stroke unit, nursing home placement prior to stroke, and Charlson comorbidity index (CCI) before stroke, and model 3 is adjusted for propensity scores of dementia. *p < 0.05, **p < 0.01, ***p≤0.001.
DISCUSSION
The principal findings of this study are: 1) patients with dementia have equal direct access to stroke unit care, however, on average, their stay there is shorter, 2) patients with dementia have 2 days shorter hospitalization length, and 3) dementia patients receive fewer diagnostic tests and assessments by the interdisciplinary stroke team.
The American [23], European [24], and Swedish national [25] guidelines for stroke management state that acute stroke patients should be treated in a dedicated stroke unit. Management in stroke units should be a priority since it carries the greatest population benefit (lives saved from death or dependency), surpassing the benefits of intravenous thrombolysis [14]. In Sweden, stroke unit management has been one of the top priorities, and by 2011, 85% of acute stroke patients under 75 years were treated in a stroke unit [26], which is similar to our study cohort (84% of dementia and 89% of non-dementia patients) with a median age of 83 years. This proportion is higher than in a 2003–2008 Canadian study where 52% of dementia and 55% of non-dementia patients were hospitalized in a dedicated stroke unit [7]. The difference might be due to the Canadian study being older, differences in stroke unit definition and access and/or differences in stroke care organization between Canada and Sweden.
Both dementia and non-dementia patients had equal direct access to a stroke unit but dementia patients’ length of stay (LOS) in a stroke unit was shorter. Moreover, the total LOS was 2 days shorter in the dementia group, which is in a disagreement with previous studies reporting no difference [27] or a longer LOS in stroke patients with dementia [7]. Dementia patients are less likely to be discharged to geriatric rehabilitation programs [5] and they might also be excluded from subacute inhospital rehabilitation, which could partly explain longer LOS in non-dementia patients. Another explanation could be that non-dementia patients might have longer hospital LOS waiting for a nursing home bed, or for home adaptations and home help to be in place. Prior to stroke, more dementia patients had either been nursing home residents and dependent in everyday activities, and some might have already been receiving help, which could have facilitated their transfer back to their previous residence. Indeed, LOS was shorter in prior nursing home residents. However, the interesting finding is that the difference between dementia and non-dementia patients was apparent only among prior nursing home residents and not those who were living at home. It is possible that non-dementia nursing home residents might have been less functionally impaired, making them better candidates for rehabilitation which could consequently explain longer LOS compared to dementia patients.
Even severely cognitively impaired patients have been shown to benefit from post-stroke rehabilitation programs [28, 29]. In our study, after adjusting for possible confounders, patients with dementia had 20–30% lower odds of receiving speech therapist, physiotherapist, and occupational therapist assessments. This differs from previous reports, where dementia patients were more likely to receive physiotherapy (91% versus 87%) [7]. Even though cognitively normal post-stroke patients achieve better functional outcomes, absolute motor gains appear to be independent of cognition [29]. Longer or specialized rehabilitation programs might be required for dementia patients, and these could reduce long-term health-care costs, caregiver burden, and nursing home placements [29].
Carotid evaluation aids in determining the mechanism of stroke and allows identification of candidates for a carotid procedure. In patients with focal neurological symptoms corresponding to the internal carotid artery territory, carotid ultrasound is recommended to detect carotid stenosis, unless CTA or MRA have already been performed in the acute phase [30]. Fewer such investigations were performed in dementia patients. The difference in utilization of carotid ultrasound between dementia and non-dementia patients persisted even after adjusting for age and level of consciousness (independent predictors in another Riksstroke study [31]), and sex, treatment in stroke unit, nursing home placement prior to stroke, and comorbidities. Even though more dementia patients had AF (33.4% versus 27.7%, p < 0.001), this should not preclude these patients from carotid imaging [31]. Possible explanations could be presence of dementia, stroke and/or dementia severity, or shorter hospitalization length (although, the relationship could also be reversed; because fewer investigations are performed, patients with dementia are discharged sooner). Whatever the reason, if a patient is not a candidate for a carotid procedure, the investigation might be excessive.
An important goal in secondary stroke prevention is the detection and treatment of AF. Longitudinal ECG is performed only in one third of non-AF patients after stroke [32], and less often in patients with dementia [7]. Encouragingly, in our study, a great majority of patients with no previous AF received or were referred for longitudinal ECG monitoring. Surprisingly, dementia patients had around 2-fold increased odds of being referred to this investigation even after adjusting for possible confounders; however, the absolute percentage difference in performance was 3% and a statistically significant difference between the groups might not mean a clinically relevant difference. One possible explanation could be that the healthier non-dementia cohort would be less likely to have an AF diagnosis in hospital or specialist care (which the NPR registers) and more likely to have a primary care AF diagnosis (which does not appear in the NPR). Physicians caring for stroke patients do have access to these primary care diagnoses, and they could have been aware of a previous primary care AF diagnosis that we cannot detect in our study. Thus, these differences in investigations for AF might be due to a bias in our study.
Dysphagia, detected in 25–67% of strokes, influences the discharge destination [33] and increases the incidence of aspiration pneumonia 3-fold [34]. Swallowing assessment is recommended before the patient begins with oral intake of fluids, food, or oral medication after AIS. Initial screening of swallowing, using, e.g., a water swallow test, is safe, can be performed before a more detailed assessment by a speech therapist, and is a key step in early identification of patients at high risk for aspiration [23]. It is reassuring that we did not find any differences between dementia and non-dementia groups in evaluation for swallowing difficulties. In AIS, dysphagia is more common in patients with dementia [8], and although many AIS patients spontaneously regain swallowing function within the first month post-stroke, recovery in dementia might be worse because of limited neuroplasticity reserve [33].
This study has several limitations. First, frail old people with dementia and other chronic disorders, residing in a nursing home, may not be referred to a hospital in case of AIS. Thus, they are probably underrepresented in this study, as Riksstroke does not cover out-of-hospital stroke events. Nevertheless, in Sweden, only a small percent of acute stroke patients are treated outside of hospitals [26]. Second, while Riksstroke’s coverage is excellent (>90%) [35], SveDem’s coverage (which entails diagnostics in memory clinics and primary care facilities across Sweden) was estimated to be 36% in 2012 [36], which is based on the number of registered patients in relation to the estimated incidence of dementia in Sweden. It is uncertain to which extent our sample represents the whole Swedish dementia population. Variables from Riksstroke have a high inter-rater reliability as Riksstroke validation process demonstrated >15% disagreement in only 4 out of 81 variables (day of stroke onset, delay from onset to arrival in hospital, swallowing assessment, and CTA or MRA) [37]. The proportion of missing surpassed 30% in the variables on implementation of rehabilitation, so we excluded these from analyses and used physiotherapist, speech therapist, and occupational therapist assessments instead. Strengths of this study are the large dementia and stroke population obtained from national quality registries and the high quality and detail of procedures registered in Riksstroke.
It is encouraging that we found no or small differences in most aspects of stroke care (CT, swallowing assessment, longitudinal ECG). For other aspects of stroke care, such as assessments by the interdisciplinary stroke team, there is still room for improvement in patients with dementia, as they received fewer investigations and rehabilitation assessments overall. The lower use of carotid ultrasound or imaging is harder to evaluate since it does not make sense to test if the patient is not a candidate for vascular or stent procedure. Since it is impossible to ascertain dementia severity at the time of stroke, we adjusted for MMSE and time from dementia diagnosis to stroke event in our post-hoc sub-group analyses in dementia patients, however, these variables were non-significant. Stroke severity in combination with preexistent dementia can predefine the care/management decisions and this could, at least partly, explain the differences. However, some types of care may not be appropriate for patients with dementia or for certain dementia subtypes, as they might carry different disease-specific effects or risks [11]. Until dementia-specific risks are characterized, patients should not be excluded from post-stroke investigations and rehabilitation solely because of dementia diagnosis. A careful consideration of each individual’s previous functioning and type and severity of stroke is critical for prognostication and for deciding level and type of care and testing.
ACKNOWLEDGMENTS
The authors thank all participants, their caregivers, reporting units, coordinators, and steering commitees in SveDem and Riksstroke. This project was conducted with support from the Swedish Order of Saint John/Johanniterorden, the Swedish Stroke Association, Stiftelsen Dementia, the Swedish Brain Foundation, the Swedish Research Council and the Swedish Associations of Local Authorities and Regions, and FORTE Swedish Research Council for Health, Working Life and Welfare (2017-01646). Zupanic was funded by Stiftelsen Dementia Foundation. Religa and Eriksdotter were supported by the Swedish Research Council grants (2012-2291 and 2016-02317 respectively). Garcia-Ptacek holds a postdoctoral fellowship from the Swedish Society for Medical Research and is funded by the Swedish Order of Saint John/Johanniterorden.
Authors’ disclosures avaiable online (https://www.j-alz.com/manuscript-disclosures/18-0653r1).
References
[1] | Prince M , Wimo A , Guerchet M , Ali G , Wu Y , Prina M ((2015) ) World Alzheimer Report 2015. The global impact of dementia. An analysis of prevalence, incidence, cost & trends; Alzheimer’s Disease International: London. [online] Available at: https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf. Accessed on Jul 25 2017. |
[2] | Abajobir AA , Abate KH , Abbafati C , Abbas KM , Abd-Allah F , Abdulkader RS , Abdulle AM , Abebo TA , Abera SF , Aboyans V ((2017) ) Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 390: , 1260–1344. |
[3] | Wimo A , Jönsson L , Bond J , Prince M , Winblad B , Alzheimer’s Disease International ((2013) ) The worldwide economic impact of dementia 2010. Alzheimers Dement 9: , 1–11. e13. |
[4] | Winblad B , Amouyel P , Andrieu S , Ballard C , Brayne C , Brodaty H , Cedazo-Minguez A , Dubois B , Edvardsson D , Feldman H ((2016) ) Defeating Alzheimer’s disease and other dementias: A priority for European science and society. Lancet Neurol 15: , 455. |
[5] | Garcia-Ptacek S , Escamez BC , Zupanic E , Religa D , von Koch L , Johnell K , von Euler M , Kåreholt I , Eriksdotter M ((2017) ) Prestroke mobility and dementia as predictors of stroke outcomes in patients over 65 years of age: A cohort study from the Swedish Dementia and Stroke Registries. J Am Med Dir Assoc 19: , 154–161. |
[6] | Zupanic E , von Euler M , Kåreholt I , Escamez BC , Fastbom J , Norrving B , Religa D , Kramberger MG , Winblad B , Johnell K ((2017) ) Thrombolysis in acute ischemic stroke in patients with dementia A Swedish registry study. Neurology 89: , 1860–1868. |
[7] | Saposnik G , Cote R , Rochon PA , Mamdani M , Liu Y , Raptis S , Kapral MK , Black SE ((2011) ) Care and outcomes in patients with ischemic stroke with and without preexisting dementia. Neurology 77: , 1664–1673. |
[8] | Saposnik G , Kapral MK , Cote R , Rochon PA , Wang J , Raptis S , Mamdani M , Black SE ((2012) ) Is pre-existing dementia an independent predictor of outcome after stroke? A propensity score-matched analysis. J Neurol 259: , 2366–2375. |
[9] | Gensicke H , Strbian D , Zinkstok SM , Scheitz JF , Bill O , Hametner C , Moulin S , Zini A , Kagi G , Pezzini A , Padjen V , Bejot Y , Corbiere S , Zonneveld TP , Seiffge DJ , Roos YB , Traenka C , Putaala J , Peters N , Bonati LH , Curtze S , Erdur H , Sibolt G , Koch P , Vandelli L , Ringleb P , Leys D , Cordonnier C , Michel P , Nolte CH , Lyrer PA , Tatlisumak T , Nederkoorn PJ , Engelter ST ((2016) ) Intravenous thrombolysis in patients dependent on the daily help of others before stroke. Stroke 47: , 450–456. |
[10] | Wakisaka Y , Matsuo R , Hata J , Kuroda J , Kitazono T , Kamouchi M , Ago T ((2017) ) Adverse influence of pre-stroke dementia on short-term functional outcomes in patients with acute ischemic stroke: The Fukuoka Stroke Registry. Cerebrovasc Dis 43: , 82–89. |
[11] | Subic A , Cermakova P , Norrving B , Winblad B , von Euler M , Kramberger MG , Eriksdotter M , Garcia-Ptacek S ((2017) ) Management of acute ischaemic stroke in patients with dementia. J Intern Med 281: , 348–364. |
[12] | Subic A CP, Religa D, Han S, von Euler M, Kåreholt I, Johnell K, Fastbom J, Bognandi L, Winblad B, Kramberger MG, Eriksdotter M, Garcia-Ptacek S ((2018) ) Treatment of atrial fibrillation in patients with dementia: A cohort study from the Swedish Dementia Registry. J Alzheimers Dis 61: , 1119–1128. |
[13] | Palli C , Fandler S , Doppelhofer K , Niederkorn K , Enzinger C , Vetta C , Trampusch E , Schmidt R , Fazekas F , Gattringer T ((2017) ) Early dysphagia screening by trained nurses reduces pneumonia rate in stroke patients: A clinical intervention study. Stroke 48: , 2583–2585. |
[14] | Gilligan AK , Thrift AG , Sturm JW , Dewey HM , Macdonell RA , Donnan GA ((2005) ) Stroke units, tissue plasminogen activator, aspirin and neuroprotection: Which stroke intervention could provide the greatest community benefit? Cerebrovasc Dis 20: , 239–244. |
[15] | ((2013) ) Quality and efficiency of stroke care in Sweden: National performance assessment 2011, Socialstyrelsen, Stockholm. [online], Available at: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/18980/2013-3-4.pdf. Accessed on July 25, 2017. |
[16] | Smith MA , Lisabeth LD , Brown DL , Morgenstern LB ((2005) ) Gender comparisons of diagnostic evaluation for ischemic stroke patients. Neurology 65: , 855–858. |
[17] | Rudd AG , Hoffman A , Down C , Pearson M , Lowe D ((2007) ) Access to stroke care in England, Wales and Northern Ireland: The effect of age, gender and weekend admission. Age Ageing 36: , 247–255. |
[18] | Pradhan AA , Levine MA ((2002) ) Warfarin use in atrial fibrillation: A random sample survey of family physician beliefs and preferences. Can J Clin Pharmacol 9: , 199–202. |
[19] | Mehndiratta P , Chapman Smith S , Worrall BB ((2015) ) Etiologic stroke subtypes: Updated definition and efficient workup strategies. Curr Treat Options Cardiovasc Med 17: , 357. |
[20] | Garcia-Ptacek S , Farahmand B , Kareholt I , Religa D , Cuadrado ML , Eriksdotter M ((2014) ) Mortality risk after dementia diagnosis by dementia type and underlying factors: A cohort of 15,209 patients based on the Swedish Dementia Registry. J Alzheimers Dis 41: , 467–477. |
[21] | Charlson ME , Pompei P , Ales KL , MacKenzie CR ((1987) ) A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis 40: , 373–383. |
[22] | Starmark JE , Stalhammar D , Holmgren E ((1988) ) The Reaction Level Scale (RLS85). Manual and guidelines. Acta Neurochir (Wien) 91: , 12–20. |
[23] | Jauch EC , Saver JL , Adams HP , Bruno A , Demaerschalk BM , Khatri P , McMullan PW , Qureshi AI , Rosenfield K , Scott PA ((2013) ) Guidelines for the early management of patients with acute ischemic stroke. Stroke 44: , 870–947. |
[24] | Committee ESOE, Committee EW ((2008) ) Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis 25: , 457–507. |
[25] | ((2009) ) Socialstyrelsen. National Guidelines for Stroke Care (Nationella riktlinjer för strokesjukvård) [online in Swedish], Stockholm. Available at: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/17790/2009-11-4.pdf. Accessed on January 10, 2017. |
[26] | Glader EL , Edlund H , Sukhova M , Asplund K , Norrving B , Eriksson M ((2013) ) Reduced inequality in access to stroke unit care over time: A 15-year follow-up of socioeconomic disparities in Sweden. Cerebrovasc Dis 36: , 407–411. |
[27] | Alshekhlee A , Li CC , Chuang SY , Vora N , Edgell RC , Kitchener JM , Kale SP , Feen E , Piriyawat P , Callison RC , Cruz-Flores S ((2011) ) Does dementia increase risk of thrombolysis? A case-control study. Neurology 76: , 1575–1580. |
[28] | Rabadi MH , Rabadi FM , Edelstein L , Peterson M ((2008) ) Cognitively impaired stroke patients do benefit from admission to an acute rehabilitation unit. Arch Phys Med Rehabil 89: , 441–448. |
[29] | Heruti RJ , Lusky A , Dankner R , Ring H , Dolgopiat M , Barell V , Levenkrohn S , Adunsky A ((2002) ) Rehabilitation outcome of elderly patients after a first stroke: Effect of cognitive status at admission on the functional outcome. Arch Phys Med Rehabil 83: , 742–749. |
[30] | Brot T , Halperin J , Abbara S ((2011) ) Guideline on the management of patients with extracranial carotid and vertebral artery disease. J Am Coil Cardiol 57: , 1002–1044. |
[31] | Buchwald F , Norrving B , Petersson J ((2018) ) Is carotid imaging underused in patients with transient ischemic attack or ischemic stroke? A Swedish Stroke Register (Riksstroke) study. Acta Neurol Scand 137: , 462–468. |
[32] | Edwards JD , Kapral MK , Fang J , Saposnik G , Gladstone DJ ((2016) ) Underutilization of ambulatory ECG monitoring after stroke and transient ischemic attack: Missed opportunities for atrial fibrillation detection. Stroke 47: , 1982–1989. |
[33] | Altman KW , Richards A , Goldberg L , Frucht S , McCabe DJ ((2013) ) Dysphagia in stroke, neurodegenerative disease, and advanced dementia. Otolaryngol Clin North Am 46: , 1137–1149. |
[34] | Martino R , Foley N , Bhogal S , Diamant N , Speechley M , Teasell R ((2005) ) Dysphagia after stroke: Incidence, diagnosis, and pulmonary complications. Stroke 36: , 2756–2763. |
[35] | Asplund K , Sukhova M , Wester P , Stegmayr B ((2015) ) Diagnostic procedures, treatments, and outcomes in stroke patients admitted to different types of hospitals. Stroke 46: , 806–812. |
[36] | Religa D , Fereshtehnejad S-M , Cermakova P , Edlund A-K , Garcia-Ptacek S , Granqvist N , Hallbäck A , Kåwe K , Farahmand B , Kilander L ((2015) ) SveDem, the Swedish Dementia Registry–A tool for improving the quality of diagnostics, treatment and care of dementia patients in clinical practice. PLoS One 10: , e0116538. |
[37] | Evaluations of variables in Riksstroke, the Swedish Stroke Register. Short version in English [online]. Available at: http://www.riksstroke.org/wp-content/uploads/2015/06/Evaluations-of-variables-in-Riksstroke-rev-15-08-03.pdf. Accessed 2017 Jul 25th. |


