
Job Loss After Diagnosis of Early-Onset Dementia: A Matched Cohort Study
Abstract
Early-onset dementia (EOD) affects the employment of patients and family members. To demonstrate how likely employees are to leave their jobs after an EOD diagnosis for themselves or a family member, we conducted a matched cohort study of 143 employees and 77 family members diagnosed with EOD using a claims database. We matched these participants to 5 controls each, and followed them for approximately 600 days. In the employee cohort, patients with EOD were more likely to leave their jobs than were controls (hazard ratio: 2.26). This suggests that healthcare providers should offer employment support to patients just after diagnosis.
INTRODUCTION
Early-onset dementia (EOD), defined as dementia occurring in individuals under 65 years of age, is a rare disease [1]. The incidence of EOD is estimated to be around 13.4 per 100,000 person-years among those aged 30–64 years [2]. Thus, most patients with EOD are still working when their symptoms appear, making it critical for them to understand whether they can continue their job after their diagnosis. While some patients are fortunate to keep working, owing to the workplace adjustments made by employers, others are obliged to leave their jobs because of their impaired performance [3, 4].
Continuing work is an effective method of maintaining self-esteem and alleviating anxiety among patients with EOD, both of which may help improve their quality of life [5–7]. Although some patients who are newly diagnosed with EOD might eventually become unable to work due to the progression of their condition, others may be able to continue their work, provided that they have appropriate workplace support [3, 8].
Prior studies on the employment of patients with EOD are limited because of the rarity of the disease. Most of them were qualitative reports based on interviews with a small number of patients [3, 4, 8]. To the best of our knowledge, there has been no quantitative study demonstrating the time course of job loss among patients with EOD. Quantifying the time to job loss after a diagnosis of EOD— either for themselves or a family member— is important to understand the social and financial burdens of this diagnosis. Therefore, the purpose of this study was to demonstrate how likely it is that employees will leave their jobs after they or a family member is diagnosed with EOD.
MATERIALS AND METHODS
Data source and study cohort
We conducted a matched cohort study of patients with EOD. We used the Japan Medical Data Center database, which comprises inpatient, outpatient, and pharmacy claims for employees and their family members from 79 large occupation-based health societies in Japan [9]. The database contained 1,561,729 employees and 1,534,736 of their family members aged 0–74 years between April 2013 and June 2015, representing approximately 2.4% of the population of Japan [10]. The database contains information on the enrollment period for health insurance; sex; birth date; diagnosis codes based on the International Statistical Classification of Diseases, 10th Revision (ICD-10); drug name; and dispensing date. The database was previously used in several studies on clinical epidemiology [11, 12]. Institutional review board approval was not required for the present study because the database contained data that were completely anonymized of patients’ personal information.
Selection of patients with early-onset dementia
We identified participants aged 40–59 years who were newly diagnosed with EOD within the 26-month study period (April 1, 2013 to June 30, 2015). Newly diagnosed EOD was defined as having an initial definitive diagnosis of dementia (ICD-10 codes F00–03 and G30–G31, with the exception of G319) or being given an initial prescription for anti-dementia drugs (i.e., donepezil, galantamine, memantine, and rivastigmine). The date of the EOD diagnosis served as the index date. To ensure the accuracy of incident cases, we included only participants who were enrolled in the health insurance system at least 365 days prior to the index date and who had not had a definitive diagnosis of dementia or a prescription of anti-dementia drugs within those 365 days. In the cohort of family members with EOD, we included only those whose supporters (e.g., husbands) were aged 40–59 years. We focused only on employees aged <59 years because 17.9% of employees leave their jobs due to the mandatory retirement age in Japan, which is set at 60 years by over 90% of large companies [13, 14].
Control selection
We randomly selected 5 control participants without EOD from the database for each participant with EOD. These control participants were matched to the participants with EOD by sex, age (within 1 year), and month of cohort entry. The index date for control participants was set to be the same as that of their matched participants with EOD.
Primary outcome
The primary outcome was participants’ time to leave their job after the index date. For the employee cohort, the job was their own, while for the family member cohort, it was the supporters’ job. Eligible participants were followed up from the index date until June 2016 or the occurrence of a job loss event.
Statistical analyses
Kaplan-Meier survival curves were constructed to calculate the cumulative incidence rates and their 95% confidence intervals (CIs) for job loss at 1 year after the index date according to dementia status. Hazard ratios (HRs) were estimated using stratified Cox proportional hazard models to account for the matched pair design [15]. All statistical analyses were performed with R version 3.3.2. Significance levels were set at 5%.
RESULTS
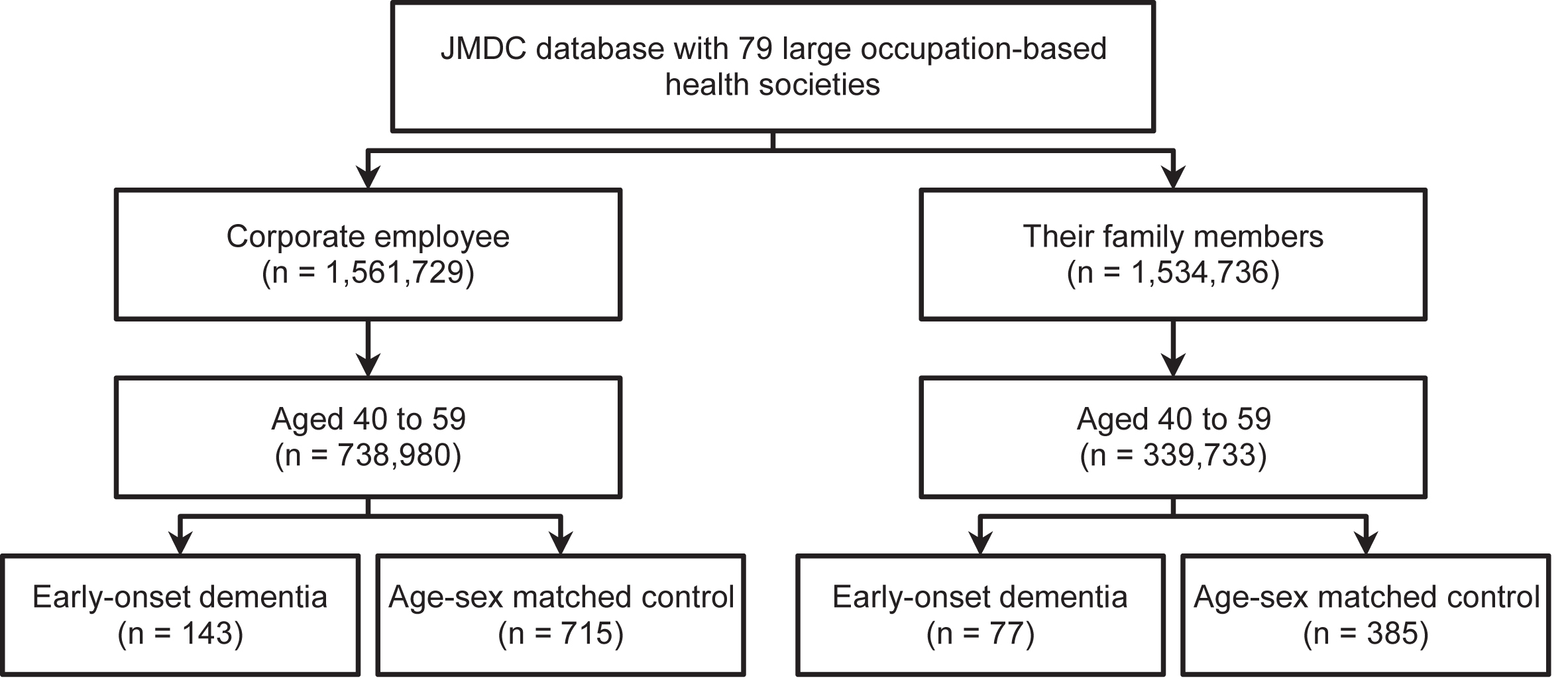
A total of 143 participants with EOD (0.02% of the 738,980 potentially eligible participants) and 715 without EOD were included in the employee cohort. Of the entire employee cohort, 13% were women, with a median age of 53 years (interquartile range 48–57 years). A total of 77 participants with EOD (0.02% of the 339,733 potentially eligible participants) and 385 without EOD were included in the family member cohort; 97% of the individuals in this cohort were women, with a median age of 53 years (interquartile range 50–56 years). A flow diagram of participant selection and the characteristics of participants are shown in Fig. 1 and Supplementary Table 1, respectively.
Fig.1
Flow diagram of included participants.
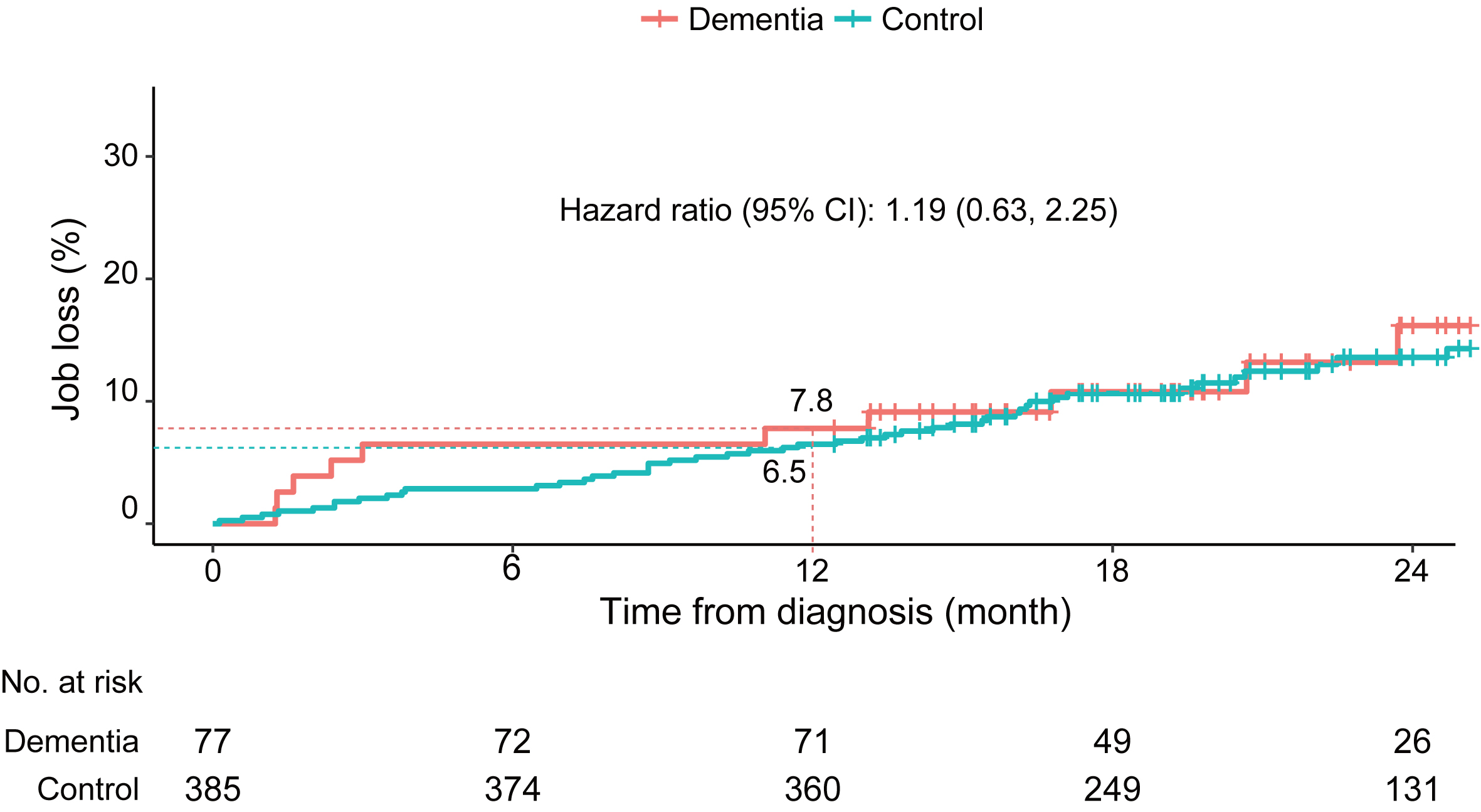
The median follow-up time without a job loss event was 625 days for employees (interquartile range: 477–807 days) and 612 days for family members (interquartile range: 492–774 days). In the employee cohort, the 1-year job loss rate was two times higher (HR: 2.26, 95% CI: 1.47–3.47) for participants with EOD (rate: 14.0%, 95% CI: 8.1% –19.5%) than for participants without EOD (rate: 7.3%, 95% CI: 5.3% –9.2%) (Fig. 2). In the family member cohort, the 1-year job loss rate for their supporters was similar (HR: 1.19, 95% CI: 0.63–2.25) between family members with (rate: 7.8%, 95% CI: 1.6% –13.9%) and without EOD (rate: 6.5%, 95% CI: 4.0% –8.9%) (Fig. 3).
Fig.2
Cumulative incidence of job loss in the employee cohort.
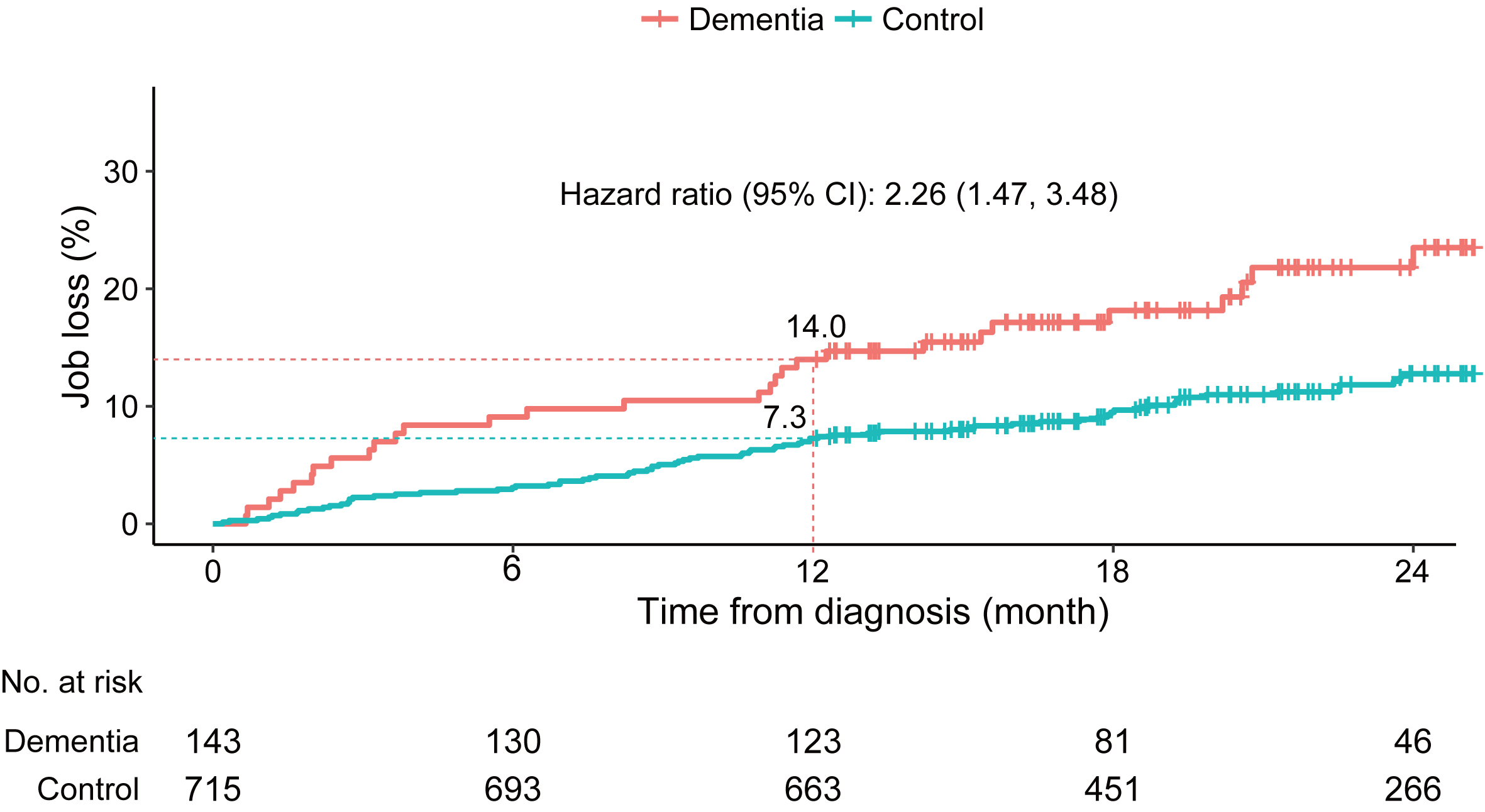
Fig.3
Cumulative incidence of job loss (of supporters) in the family member cohort.
DISCUSSION
This is the first quantitative study to demonstrate the incidence of job loss among patients with EOD. We found that 14% of patients with EOD left their jobs within one year after their diagnosis, which was twice the rate of those without EOD. This finding is similar to the results of prior studies investigating the increased risk of job loss associated with health problems (i.e., cancer and stroke) [16–19]. For example, a previous cohort study showed that patients who had been diagnosed with colorectal cancer (stage II and III) had a 1.7- to 1.9-fold higher risk of job loss at 2 years after diagnosis than did those without such a diagnosis [18].
The higher job loss rate among patients with EOD might be attributed to both inevitable and preventable factors [3, 4, 20]. Past studies have shown that some patients are dismissed due to their impaired performance, whereas others impulsively left their jobs because of the shock caused by the diagnosis [3, 4]. Patients with EOD who cannot continue working because of their advancing symptoms might seek a substitute activity to help improve their quality of life [5, 21]. On the other hand, a prior study showed that more than half of patients with EOD were still in the mild stage of dementia shortly after their diagnosis, which means that some patients retain the ability to work, provided that their employers accommodate them [3, 8, 22]. These patients should be encouraged to continue their jobs as long as possible to ensure that they continue receiving a job-related income and to maintain their self-esteem [3, 8]. Healthcare providers might make an effort to help patients with EOD continue working or to alleviate the harm caused by their unemployment, such as by advising them on requests for workplace adjustments or providing useful information on substitute activities following their initial diagnosis [5, 6, 21].
To the best of our knowledge, this is the first study to evaluate the comparative risk of job loss due to family members’ health problems. Unlike the results concerning job loss among employees following their own diagnosis, employees whose family members had EOD had a similar risk of job loss as employees whose family members did not have EOD. These findings are not consistent with those of prior studies [23–25]. One questionnaire survey showed that only 18% of supporters who were employed full time at the time of an EOD diagnosis retained the same employment status at the time of survey (i.e., around 4 years after diagnosis) [20]. One potential explanation for this inconsistency is that our follow-up time was too short to capture the resignations that might occur after supporters’ caregiver burden increased.
Our study has several important limitations. First, our study population was limited to the employees and family members of 79 large occupation-based health societies. As a result, the cumulative incidence of job loss was likely underestimated because large companies might be more able to afford to support employees with health problems than small companies might. Therefore, our findings may not be representative of the broader population of patients with EOD. To improve the generalizability of our findings, it is important for future studies to include all types of workers including civil servants, employees, and self-employed workers. Second, we were unable to identify the reasons for the job loss. Namely, we might have included individuals who had retired voluntarily (as under an early retirement plan) or involuntarily (e.g., due to business closure, layoffs, or health problems). As a result, the cumulative incidence of job loss due to a diagnosis of EOD may be overestimated. Third, we could only adjust for a limited number of risk factors, including sex, age, and month of cohort entry, because of data limitations; it is unlikely that all potential risk factors for job loss were controlled in the present study. Future studies should consider additional covariates including types and severity of dementia, education, and job category [3, 8, 16, 18]. Fourth, we were unable to identify the impact of job loss after the EOD diagnosis. As a result, we could not identify whether employees who leave their job after EOD diagnosis retain self-esteem or quality of life. The impact related to job loss might be a more critical outcome for employees and their family members.
In conclusion, our study showed that patients with EOD are more likely than are people without EOD to leave their jobs shortly after receiving their diagnosis. To help patients with EOD continue working or find a substitute activity, healthcare providers should advise and support patients and their families on employment just after the initial diagnosis.
ACKNOWLEDGMENTS
This study was supported by grants from the Japan Agency for Medical Research and Development (No. 16dk0207024h0001). The sponsors of this study had no role in the design and conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication. The authors are grateful to Ms. Makiko Kaneko for her preparation of the dataset from the Japan Medical Data Center (JMDC) database. We also would like to express our appreciation to Editage for providing editorial assistance.
Authors’ disclosures available online (http://j-alz.com/manuscript-disclosures/17-0478r1).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: http://dx.doi.org/10.3233/JAD-170478.
REFERENCES
[1] | Ikejima C , Yasuno F , Mizukami K , Sasaki M , Tanimukai S , Asada T ((2009) ) Prevalence and causes of early-onset dementia in Japan. Stroke 40: , 2709–2714. |
[2] | Garre-Olmo J , Genís Batlle D , del Mar Fernández M , Marquez Daniel F , de Eugenio Huélamo R , Casadevall T , TurbauRecio J , Turon Estrada A , López-Pousa S , Registry of Dementiaof Girona Study Group ((2010) ) Incidence and subtypes of early-onsetdementia in a geographically defined general population. Neurology 75: , 1249–1255. |
[3] | Evans D ((2016) ) An exploration of the impact of younger-onset dementia on employment. Dementia (London), doi: 10.1177/1471301216668661 |
[4] | Chaplin R , Davidson I ((2016) ) What are the experiences of people with dementia in employment? Dementia 15: , 147–161. |
[5] | Roach P , Drummond N ((2014) ) ′It’s nice to have something to do’:Early-onset dementia and maintaining purposeful activity. JPsychiatr Ment Health Nurs 21: , 889–895. |
[6] | Robertson J , Evans D ((2015) ) Evaluation of a workplace engagement project for people with younger onset dementia. J Clin Nurs 24: , 2331–2339. |
[7] | Werner P , Stein-Shvachman I , Korczyn AD ((2009) ) Early onset dementia: Clinical and social aspects. Int Psychogeriatrics 21: , 631. |
[8] | Ohman A , Nygard L , Borell L ((2001) ) The vocational situation in cases of memory deficits or younger-onset dementia. Scand J Caring Sci 15: , 34–43. |
[9] | Kimura S , Sato T , Ikeda S , Noda M , Nakayama T ((2010) ) Development of a database of health insurance claims: Standardization of disease classifications and anonymous record linkage. J Epidemiol 20: , 413–419. |
[10] | Statistics Bureau ((2014) ) Population estimates: Table 1. Populationby age (single year), sex and sex ratio (in Japanese), http://www.e-stat.go.jp/SG1/estat/Xlsdl.do?sinfid=000029025950. Last updated 2015, accessed on May 27, 2017. |
[11] | Fukuda H , Mizobe M ((2017) ) Impact of nonadherence on complication risks and healthcare costs in patients newly-diagnosed with diabetes. Diabetes Res Clin Pract 123: , 55–62. |
[12] | Okumura Y , Shimizu S , Matsumoto T ((2016) ) Prevalence, prescribed quantities, and trajectory of multiple prescriber episodes for benzodiazepines: A 2-year cohort study. Drug Alcohol Depend 158: , 118–125. |
[13] | Ministry of Health, Labour and Welfare ((2016) ) General Survey onWorking Conditions (in Japanese),http://www.mhlw.go.jp/toukei/itiran/roudou/jikan/syurou/16/dl/gaiyou02.pdf. Last updated 2016, accessed on May 27, 2017. |
[14] | Ministry of Health, Labour and Welfare ((2015) ) Survey on EmploymentConditions of Elderly Persons (in Japanese), http://www.mhlw.go.jp/stf/houdou/0000101253.html. Last updated 2016, accessed on May 30, 2017. |
[15] | Kleinbaum DG , Klein M ((2012) ) Survival analysis: A self-learning text, Springer, New York. |
[16] | Maaijwee NAMM , Rutten-Jacobs LCA , Arntz RM , Schaapsmeerders P , Schoonderwaldt HC , van Dijk EJ , de Leeuw F-E ((2014) ) Long-term increased risk of unemployment after young stroke: A long-term follow-up study. Neurology 83: , 1132–1138. |
[17] | Rottenberg Y , Jacobs JM , Ratzon NZ , Grinshpun A , Cohen M , Uziely B , de Boer AGEM ((2017) ) Unemployment risk 2 years and 4 years following gastric cancer diagnosis: A population-based study. J Cancer Surviv 11: , 119–125. |
[18] | Rottenberg Y , Ratzon NZ , Cohen M , Hubert A , Uziely B , de Boer AGEM ((2016) ) Unemployment risk at 2 and 4 years following colorectal cancer diagnosis: A population based study. Eur J Cancer 69: , 70–76. |
[19] | Taskila-Åbrandt T , Pukkala E , Martikainen R , Karjalainen A , Hietanen P ((2005) ) Employment status of Finnish cancer patients in 1997. Psychooncology 14: , 221–226. |
[20] | Alzheimer’s association ((2006) ) Early onset dementia: A nationalchallenge, a future crisis, http://www.alz.org/national/documents/report_earlyonset_full.pdf. Accessed on May 27, 2017. |
[21] | Richardson A , Pedley G , Pelone F , Akhtar F , Chang J , Muleya W , Greenwood N ((2016) ) Psychosocial interventions for people with young onset dementia and their carers: A systematic review. Int Psychogeriatrics 28: , 1441–1454. |
[22] | Van Vliet D , de Vugt ME , Bakker C , Pijnenburg YAL , Vernooij-Dassen MJFJ , Koopmans RTCM , Verhey FRJ ((2013) ) Time to diagnosis in young-onset dementia as compared with late-onset dementia. Psychol Med 43: , 423–432. |
[23] | Luscombe G , Brodaty H , Freeth S ((1998) ) Younger people with dementia: Diagnostic issues, effects on carers and use of services. Int J Geriatr Psychiatry 13: , 323–330. |
[24] | Delany N , Rosenvinge H ((1995) ) Presenile dementia: Sufferers, carers and services. Int J Geriatr Psychiatry 10: , 597–601. |
[25] | Van Vliet D , de Vugt ME , Bakker C , Koopmans RTCM , Verhey FRJ ((2010) ) Impact of early onset dementia on caregivers: A review. Int J Geriatr Psychiatry 25: , 1091–1100. |


