
Characteristics of Changes in Caregiver Burden during Follow-up at a Memory Clinic: A Retrospective Cohort Study
Abstract
Background:
Because dementia is a long-term condition, the appropriate involvement of health-care professionals is considered important. However, little is known about the factors associated with changes in family caregiver burden.
Objective:
To clarify changes in family caregiver burden and associated factors during follow-up at a memory clinic.
Methods:
A retrospective cohort study was conducted, enrolling 495 pairs of patients with dementia or mild cognitive impairment and their family caregivers. A total of 120 pairs completed the second evaluation. The caregiver burden was assessed using the Zarit Burden Interview (ZBI). Data at the initial visit and after an average follow-up of about 2 years were compared and analyzed.
Results:
At initial visit, the patients’ mean age, Mini-Mental State Examination (MMSE) and ZBI scores were 78.6±5.6 years, 23.3±3.5, and 22.6±16.7, respectively. At follow-up, MMSE scores decreased (21.4±4.5, p < 0.001), but ZBI scores remained similar (22.5±13.6). When the difference in ZBI scores between the two time points was defined as ΔZBI, and the related factors were analyzed by multiple regression analysis, ZBI scores at the initial visit, start of psychotropic drug, and decrease of neuropsychiatric symptoms were identified as significant factors (p < 0.001, p = 0.003, p < 0.001, respectively). A significant negative correlation was found between ZBI scores at the initial visit and ΔZBI (r = –0.588, p < 0.001).
Conclusions:
These findings suggest the importance of assessing changes in the burden experienced by family caregivers during the disease follow-up.
INTRODUCTION
Dementia is one of the most common diseases among older adults, and the numbers of people with dementia are increasing with the ongoing aging of society [1, 2]. Dementia not only affects a large number of patients, but also imposes a heavy burden on family caregivers because of the decline in the patient’s ability to live independently and the development of psychiatric symptoms such as delusions and irritability [1, 2].
At present, there is no cure for dementia, so an important goal of interventions in dementia care is to maintain the quality of life of the person with dementia and their family caregivers [3]. Specifically, the primary goals of interventions are to prevent or promote the early remission of psychiatric symptoms in the person with dementia and reduce the caregiving burden on family caregivers [4]. Reducing the burden of caregiving itself can contribute to the prevention or early improvement of psychiatric symptoms, and conversely, the prevention or improvement of psychiatric symptoms can lead to a decreased caregiving burden [5–8]. Several interventions have also been reported to help prevent institutionalization and reduce the social and economic costs associated with dementia [9–11].
Various efforts have been made, and shown to be effective, in reducing the burden of care on family caregivers of people with dementia. However, many interventions have only looked at the effects over a relatively short period of time, such as 6 months [12, 13]. On the other hand, using caregiving burden as an indicator, many longitudinal studies of more than 1 year have shown that the caregiving burden worsens [4, 14–20].
Dementia is a long-term disease that can last for more than a decade, and medical care that follows the long-term progress is thought to play an important role [21–25]. During this period, advice, medication adjustments, and information regarding the use of social resources are provided according to the symptoms of the disease at the time and expected to help reduce the burden of caregiving on family caregivers [21–25]. However, to date, sufficient research is lacking on the effects of longitudinal follow-up at memory clinics on reducing the caregiving burden. In particular, few reports have analyzed changes in the caregiving burden from the early stages of dementia, including in patients with mild cognitive impairment (MCI) [17, 26].
In the current study, we conducted a survey to examine changes over time in clinical indicators, medical interventions, utilization of healthcare resources, and caregiver burden among families whose patients had been regularly visiting an outpatient memory clinic for a minimum of 1 year (with an average duration of approximately 2 years). Our aim was to analyze the characteristics and associated factors of long-term changes in family caregiver burden at a memory clinic, which is one of the important facilities offering involvement of healthcare professionals.
METHODS
Study design and participants
A retrospective cohort study was performed. Participants were pairs consisting of patients with dementia or mild cognitive impairment and their family caregivers who had made their initial visit to the Outpatient Memory Clinic of Fujita Health University Hospital between July 2016 and April 2021. They underwent a comprehensive evaluation and were reevaluated, which included assessing caregiver burden, between June 2019 and April 2022. A total of 495 pairs were enrolled, and 120 completed the second evaluation. The decision to continue treatment at a specialized memory clinic or to request ongoing care from a general practitioner (GP) is made by considering various factors, including the preferences of the patient or family caregiver, the necessity of management in a specialized clinic, and logistical aspects such as transportation for clinic visits. Additionally, interruptions in clinic visits may occur if the patient transitions to a care facility due to the progression of dementia or if family caregivers are unable to accompany the patient due to work or health reasons, despite initially attending the specialized clinic.
The National Institute on Aging and Alzheimer’s Association diagnostic criteria were used for the clinical diagnosis of Alzheimer’s disease (AD) and MCI [27, 28]. Diagnoses of dementia with Lewy bodies (DLB) and vascular dementia (VaD) were made according to the criteria of the fourth consensus report of the DLB Consortium and the National Institute of Neurological Disorders and Stroke, respectively [29, 30]. A diagnosis of mixed-type dementia (MIX) was made when patients were found to have dementia not explained solely by AD, DLB, or VaD. This study was reviewed and approved by the Ethics Committee of Fujita Health University (HM20-585).
Measurements
As part of the overall evaluation, interviews were conducted with the patients to collect data on age, sex, educational history, and residential status. The Mini-Mental State Examination (MMSE) and Geriatric Depression Scale (GDS) were used to assess cognitive function and depressive mood, respectively [31, 32]. For the initial activities of daily living (ADL) assessment, the Dementia Assessment Sheet for Community-based Integrated Care System-21 items (DASC-21: minimum score: 21, maximum score: 84), a 21-item four-point scale combining the observational cognitive function and ADL/instrumental activities of daily living (IADL) assessment, was used [33]. At the time of reassessment, the DASC-8 (minimum score of 8 and maximum score of 32), which was created as an 8-item shortened version of the DASC-21, was used [34]. Higher scores on both the DASC-21 and DASC-8 indicate a higher degree of dementia severity. The 12-item version of the Neuropsychiatric Inventory (NPI-12) was used for the initial assessment of patients’ behavioral and psychological symptoms of dementia (BPSD); however, the NPI score (frequency × severity) at the initial visit was calculated using only 10 items [35, 36]. The Neuropsychiatric Inventory Questionnaire (NPI-Q) was used at reassessment, and a comparison between the initial visit and reassessment was made only using the severity and burden scores on the NPI-12 and NPI-Q [36].
The Zarit Burden Interview (ZBI) was used to measure the burden of family caregivers at both the initial visit and the reassessment, and personal strain (PS) and role strain (RS) were calculated simultaneously [37, 38]. Family caregivers’ age, sex, relationship, and whether they lived with the patient were also investigated. At the initial visit, the patients were also asked about psychotropic and anti-dementia medications and the use of long-term care insurance (LTCI) services [39, 40]. Prescriptions for psychotropic and anti-dementia medications during outpatient follow-up and the initiation of LTCI services were also recorded. No patient was taking antipsychotics at the time of the initial visit, but if antipsychotics were started after the initial visit, the initiation of antipsychotics was also recorded separately from psychotropic medications. Psychotropic medications other than antipsychotics included antidepressants, anxiolytics, sleeping pills, and the Chinese herbal medicine yokukansan [41]. The number of days from the initial visit to the reevaluation and the number of visits during that period were also recorded.
Statistical analysis
Descriptive statistics (e.g., mean, standard deviation [SD], prevalence rates) were used for the participants’ basic characteristics. A paired t-test was used to examine the change in each parameter between the initial visit and reassessment. The difference between the ZBI score at the time of the initial visit and at reevaluation was defined as ΔZBI. We hypothesized three models to analyze ΔZBI and its associated factors. The first model explored the association of patient and family caregiver characteristics at baseline. The second model investigated the association of treatment and care initiation during the follow-up period. The third model examined the concomitant change in cognition and BPSD. To identify factors related to ΔZBI, we conducted multiple regression analyses with ΔZBI as the dependent variable and potentially related factors as independent variables. We aimed to include at least 8 factors, including confounding variables, in each regression model, hence the sample size of 120 was chosen to avoid overfitting of the model [42]. To assess the statistical assumptions for using the linear regression model, we performed residual analysis, calculated the Durbin-Watson ratio, and confirmed the suitability of using the model. Pearson’s correlation analysis was performed for the correlation analysis between the ZBI score at initial visit and ΔZBI. For differences by diagnosis group, statistical analysis was performed using analysis of variance followed by Bonferroni’s post-hoc analysis for quantitative factors. Categorical variables were analyzed using χ2 analysis. SPSS Statistics for Windows (version 27; IBM, Armonk, NY, USA) was used for all statistical analyses, with the level of significance set at 0.05.
RESULTS
In total, the study participants comprised 120 pairs of outpatients (44 with AD, 55 with MCI, 8 with DLB, 10 with MIX, and 3 with other types of dementia) and their family caregivers. At the time of the initial visit, the mean±SD age of the 120 patients (55% female) was 78.6±5.6 years, MMSE score 23.3±3.5, and NPI score 11.2±15.1. The mean±SD age of the family caregivers was 64.3±11.9 years and ZBI score 22.6±16.7. In terms of living arrangements, 119 (99.2%) of the participants were living at home (15 alone and 104 with their families); only one (0.8%) was living in a residential care home. The family caregivers who responded to the questionnaire were most frequently daughters (n = 45), followed by wives (n = 43), husbands (n = 16), sons (n = 12), daughters-in-law (n = 3), and sisters (n = 1). For the further analysis involving relationships, we employed a dichotomous classification: spouse generation (spouses or sisters) and child generation (daughters, sons, or daughters-in-law) to simplify the analysis. As for social services and treatment at the initial visit, 20 patients had already used LTCI services, and 15 and four had previously been prescribed anti-dementia and psychotropic drugs, respectively (Table 1). Out of the 495 pairs initially enrolled, 375 pairs were excluded: 335 were lost to follow-up, and 40 involved different family members who responded to the second evaluation. When comparing the 120 pairs in the final study group to the excluded 375 pairs, we observed some statistical differences. Specifically, the excluded group had slightly higher patient ages (80.1±6.7 versus 78.6±5.6, p = 0.022), slightly lower MMSE scores (21.0±6.9 versus 23.3±3.5, p = 0.005), and higher DASC21 scores (39.7±13.7 versus 34.3±10.2, p < 0.001) compared to the final study group. However, there were no significant differences between the excluded group and the final study group in terms of the age of family caregivers, NPI score, ZBI score, relationship, and living status.
Table 1
Basic characteristics of the patients and family caregivers
| Patient with dementia | ||
| Mean | SD | |
| Age | 78.6 | 5.6 |
| Female (%) | 55.8 | |
| Education | 11.9 | 5.1 |
| MMSE | 23.3 | 3.5 |
| GDS | 4.8 | 3.4 |
| DASC-21 | 34.8 | 9.8 |
| DASC-8 | 12.6 | 3.6 |
| NPI | 11.2 | 15.1 |
| NPI-Q 12 severity | 4.9 | 5.1 |
| NPI-Q burden | 6.0 | 7.5 |
| NPI-Q 12 burden | 6.8 | 8.7 |
| Living arrangement | n | % |
| Alone | 15 | 12.5 |
| Spouse | 53 | 44.2 |
| With children | 51 | 42.5 |
| Senior home | 1 | 0.8 |
| Mean | SD | |
| Follow-up days | 666.3 | 315.6 |
| Intervention | n | % |
| Use of LTCI services (%) | 20 | 16.7 |
| Start of LTCI services (%) | 48 | 40.0 |
| Taking anti-dementia drug (%) | 15 | 12.5 |
| Start of anti-dementia drug (%) | 74 | 61.7 |
| Taking psychotropic drug (%) | 4 | 3.3 |
| Start of psychotropic drug (%) | 24 | 20.0 |
| Start of antipsychotic drug (%) | 7 | 5.8 |
| Family caregiver | ||
| Mean | SD | |
| Age | 64.3 | 11.9 |
| Female (%) | 76.7 | |
| ZBI | 22.6 | 16.7 |
| PS | 13.3 | 9.1 |
| RS | 4.4 | 5.6 |
| Living status | n | % |
| Living with patient | 96 | 80 |
| Living separately | 24 | 20 |
MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale; DASC, Dementia Assessment Sheet in Community-based Integrated Care System; NPI, Neuropsychiatric Inventory; LTCI, long-term care insurance; ZBI, Zarit Burden Interview; PS, personal strain; RS, role strain; SD, standard deviation.
The mean±SD duration from the initial visit to the follow-up evaluation was 666.3±315.6 days, and the mean number of clinic visits was 9.7±4.2. Regarding caregiver burden, the mean±SD ZBI score was 22.6±16.7 at the initial visit and 22.5±13.6 at the follow-up evaluation; this difference was not significant. In addition, no significant difference was found for PS and RS in the ZBI score (Table 2). The mean±SD MMSE and DASC-8 scores at the initial visit and follow-up evaluation were 23.3±3.5 and 21.4±4.5, and 12.6±3.6 and 16.6±4.4, respectively, showing significant deterioration (both p < 0.001). No significant difference in GDS scores was found between the initial visit and follow-up evaluation. Regarding the severity and burden scores for the NPI-12, no significant difference in severity was found, but a significant decrease in burden was seen, from 6.8±8.7 to 3.8±5.4 (p < 0.001).
Table 2
Differences in parameters between the initial and follow-up evaluations
| Initial | Follow-up | ||||
| Mean | SD | Mean | SD | p | |
| ZBI | 22.6 | 16.7 | 22.5 | 13.6 | 0.949 |
| PS | 13.3 | 9.1 | 13.4 | 8.2 | 0.800 |
| RS | 4.4 | 5.6 | 4.5 | 4.3 | 0.804 |
| MMSE | 23.3 | 3.5 | 21.4 | 4.5 | <0.001 |
| GDS | 4.8 | 3.4 | 4.5 | 3.2 | 0.187 |
| DASC-8 | 12.6 | 3.6 | 16.6 | 4.4 | <0.001 |
| NPI-Q 12 severity | 4.9 | 5.1 | 4.2 | 4.5 | 0.059 |
| NPI-Q 12 burden | 6.8 | 8.7 | 3.8 | 5.4 | <0.001 |
ZBI, Zarit Burden Interview; PS, personal strain; RS, role strain; MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale; DASC, Dementia Assessment Sheet in Community-based Integrated Care System; NPI, Neuropsychiatric Inventory; SD, standard deviation.
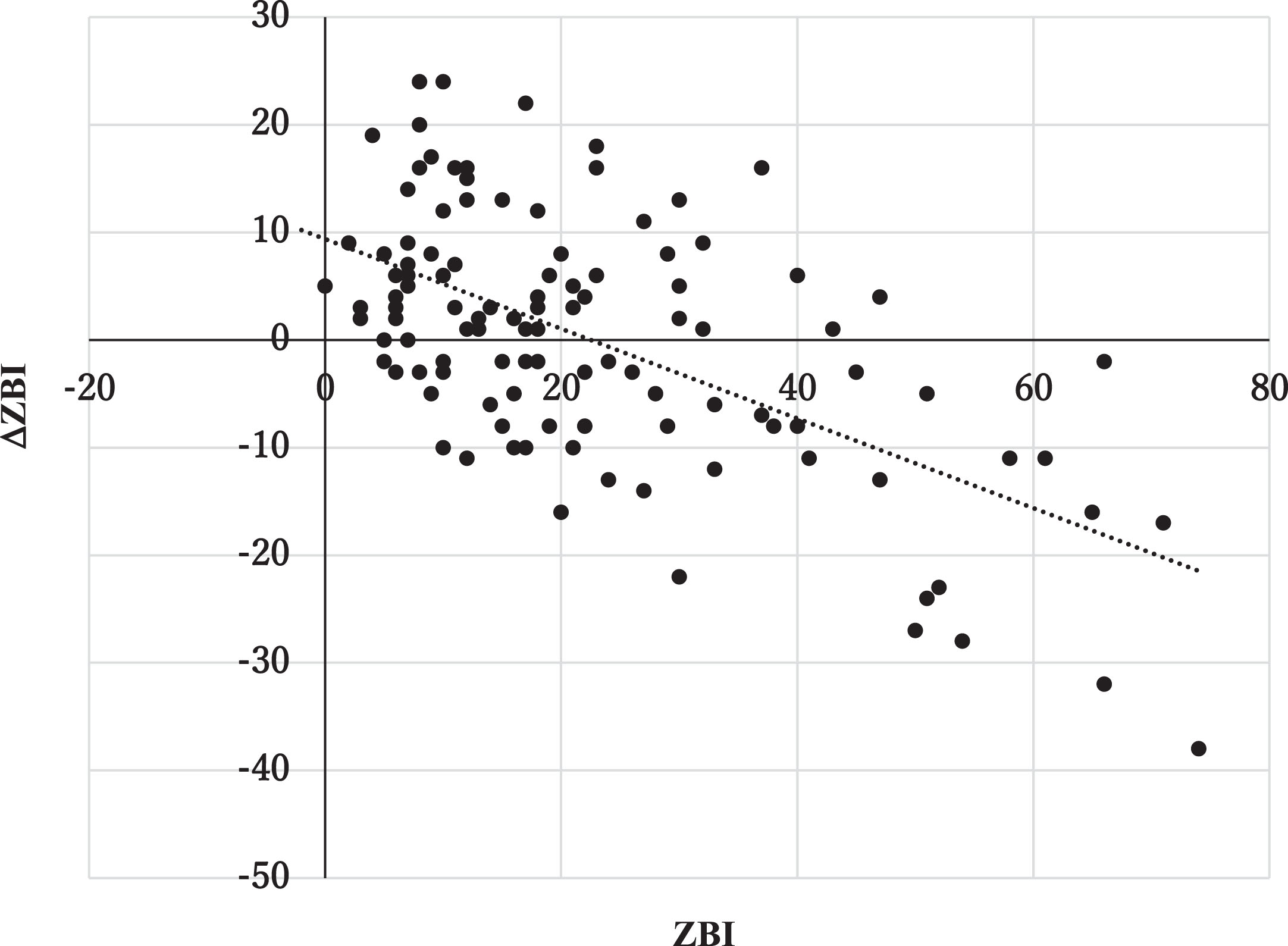
As shown in Table 2, no significant difference was found when comparing the mean ZBI scores between the initial visit and follow-up evaluation. Then we analyzed associate factors with ΔZBI. To analyze these factors, we employed three separate models. The first model explored the association of patient and family caregiver characteristics at baseline. The second model investigated the association of treatment and care initiation during the follow-up period. The third model examined the concomitant change in cognition and BPSD. In these analyses, we adjusted for the age and gender of patients, the age of caregivers, relationship, and living status. Additionally, in the third model, we also adjusted for the duration from the initial visit to the follow-up evaluation. In the second model, the initiation of psychotropic drugs and antipsychotic drugs was combined to prevent overfitting of the model. The results of these analyses indicated that ZBI scores at the initial visit, the initiation of psychotropic drugs, and ΔNS were significantly associated with ΔZBI (Table 3). Pearson’s correlation analysis revealed that the relationship between ZBI score at the initial visit and ΔZBI was significant (r=–0.588, p < 0.001), demonstrating that if the ZBI score was high at the initial visit, it improved significantly over the course of follow-up (Fig. 1). Due to the substantial variation in the intervals between the two evaluations, we conducted two additional assessments. Firstly, we performed multivariate analysis by adding the interval between evaluations as an explanatory factor, the interval was not extracted as a significant factor (for the analysis of association between ΔZBI and baseline characteristics, β= 0.002, t = 0.02, p = 0.984; for the analysis of association between ΔZBI and treatment and care, β= –0.004, t = –0.048, p = 0.962). It did not affect other results either. Secondly, the analysis was narrowed down to subjects with intervals within three years. However, the results in Table 3 were almost equivalent (n = 101, interval between evaluations 554.4±191.7 days).
Table 3
Association between ΔZBI and parameters
| β | t | p | |
| Baseline characteristics | |||
| MMSE | –0.054 | –0.689 | 0.492 |
| ZBI | –0.531 | –5.667 | <0.001 |
| NPI | –0.184 | –1.911 | 0.059 |
| Treatment and Care | |||
| Start of anti-dementia drug | 0.03 | 0.318 | 0.751 |
| Start of psychotropic drug | –0.284 | –3.065 | 0.003 |
| Start of LTCI services | 0.012 | 0.12 | 0.904 |
| Change during follow-up | |||
| ΔMMSE | –0.143 | –1.533 | 0.128 |
| ΔNPI-Q 12 severity | 0.406 | 4.698 | <0.001 |
| Interval between 2 evaluations | –0.118 | –1.326 | 0.188 |
MMSE, Mini-Mental State Examination; ZBI, Zarit Burden Interview; NPI, Neuropsychiatric Inventory; LTCI, long-term care insurance. For these analyses, we adjusted for the age and gender of patients, the age of caregivers, relationship, and living status. In the third model, we also adjusted for the duration from the initial visit to the follow-up evaluation. Additionally, we combined the initiation of psychotropic drugs and antipsychotic drugs as the initiation of psychotropic drugs to prevent overfitting of the model in this analysis.
Fig. 1
Relationship between Zarit Burden Interview (ZBI) scores at initial visit and ΔZBI. The horizontal and vertical axes show ZBI scores at initial visit and ΔZBI (the difference in ZBI scores between initial visit and follow-up evaluation), respectively.
Finally, details were examined by diagnostic group (Table 4). In this analysis, cases belonging to other dementia were omitted from the analysis because these only involved three patients. MMSE and DASC scores were significantly higher in the MCI group, and NPI scores were higher in the DLB group, but not significantly different. ZBI scores significantly differed among the four groups, with higher values in the DLB than in the AD group. Although not significantly high in the MIX group, ZBI was high in the DLB and MIX group, so the factors related to ΔZBI were analyzed only in the MCI and AD groups (n = 99). As with the analyses for all participants, the multiple regression analysis using ΔZBI as a dependent valuable revealed an association only with ZBI scores at the initial visit (β= –0.57, p < 0.001).
Table 4
Differences in caregiver burden and other parameters among underlying diseases
| Total (n = 117) | MCI (n = 55) | AD (n = 44) | DLB (n = 8) | MIX (n = 10) | p | Post-hoc | ||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Age | 78.5 | 5.7 | 78.8 | 5.7 | 78.3 | 5.9 | 79.6 | 5.9 | 77.6 | 4.3 | 0.865 | |
| Female (n, %) | 67 (57.3) | 26 (47.3) | 29 (65.9) | 6 (75.0) | 6 (60.0) | 0.200 | ||||||
| Education | 12.0 | 5.1 | 12.9 | 6.8 | 10.8 | 2.9 | 11.6 | 2.5 | 12.3 | 2.7 | 0.255 | |
| Follow-up (days) | 671.4 | 317.2 | 676.0 | 329.7 | 634.7 | 281.6 | 652.1 | 302.0 | 822.6 | 403.2 | 0.411 | |
| Number of visits | 9.7 | 4.2 | 9.4 | 4.4 | 9.5 | 3.4 | 11.3 | 4.8 | 11.1 | 5.6 | 0.464 | |
| Age, caregiver | 64.0 | 11.9 | 66.1 | 11.6 | 63.6 | 12.7 | 60.3 | 9.3 | 58.5 | 10.3 | 0.219 | |
| Caregiver, female (n, %) | 89 (76.1) | 44 (80.0) | 31 (75.0) | 5 (62.5) | 9 (90.0) | 0.376 | ||||||
| Relationship, spouse (n, %) | 60 (51.3) | 26 (47.3) | 21 (47.7) | 7 (87.5) | 6 (60.0) | 0.166 | ||||||
| Living with patient (n, %) | 93 (79.5) | 45 (81.8) | 35 (79.5) | 5 (62.5) | 8 (80.0) | 0.659 | ||||||
| MMSE | 23.3 | 3.4 | 25.7 | 2.3 | 20.9 | 2.9 | 21.8 | 3.5 | 21.9 | 1.7 | <0.001 | 1 > 2,3,4 |
| GDS | 4.8 | 3.4 | 4.1 | 3.1 | 5.4 | 3.4 | 4.9 | 4.8 | 5.2 | 4.2 | 0.290 | |
| DASC-21 | 34.9 | 9.9 | 32.2 | 7.5 | 37.7 | 11.3 | 38.6 | 13.9 | 33.3 | 7.1 | 0.037 | 2 > 1 |
| NPI | 11.5 | 15.2 | 9.4 | 11.3 | 10.8 | 14.2 | 24.9 | 31.4 | 14.4 | 16.8 | 0.053 | |
| ZBI | 22.9 | 16.8 | 21.9 | 17.5 | 20.2 | 12.5 | 38.1 | 20.8 | 27.8 | 21.0 | 0.030 | 3 > 2 |
| PS | 13.5 | 9.1 | 13.2 | 9.7 | 11.9 | 6.4 | 21.4 | 11.5 | 16.1 | 11.6 | 0.040 | 3 > 2 |
| RS | 4.5 | 5.6 | 4.0 | 5.4 | 3.8 | 4.8 | 10.3 | 7.4 | 5.7 | 6.3 | 0.016 | 3 > 1,2 |
MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale; DASC, Dementia Assessment Sheet in Community-based Integrated Care System; NPI, Neuropsychiatric Inventory; ZBI, Zarit Burden Interview; PS, personal strain; RS, role strain; MCI, mild cognitive impairment; AD, Alzheimer’s disease; DLB, Dementia with Lewy Bodies; MIX, mixed-type dementia; SD, standard deviation.
DISCUSSION
We conducted a retrospective cohort study of clinical parameters including family caregiver burden before and after an average follow-up of about 2 years in an outpatient memory clinic. The results showed that although cognitive function and ADL declined during the course of the study, caregiver burden did not. The results of the survey on the initiation of social care services and the use of anti-dementia and psychotropic drugs showed that 40.0%, 61.7%, and 20.0% of the patients started to use them, respectively, during the follow-up period. An examination of the course of caregiving burden using multiple regression analysis indicated that a higher ZBI score at the initial visit, the initiation of psychotropic drugs, and a decrease in neuropsychiatric symptoms were associated with an improvement in the ZBI score by the time of follow-up. The psychological support and advice given to family caregivers by a specialist during outpatient visits were not included in the analysis because these were difficult to quantify as variables; however, they may have been involved in the effect of improving the caregiving burden. These results suggest that the caregiver burden improves during visits to an outpatient memory clinic, at least in groups with a heavy caregiving burden.
At present, no anti-dementia drugs are effective enough against dementia to halt its progression. Cognitive function tests such as the MMSE and ADL and IADL assessments are usually used as indicators to evaluate the situations of dementia patients and family caregivers over a long disease course. It is important for professionals to provide appropriate advice and referrals to community resources according to the results of these assessments, but it is difficult to improve these indicators through interventions. On the other hand, many studies have reported that interventions for caregiver burden lead to improvements, at least in the short term [12, 13].
However, previous longitudinal studies have often reported increases in the caregiver burden over time [4, 14–20, 43, 44]. Moreover, reports on what interventions were carried out during this period have been limited. In the present study, during an approximate 2-year period, the patients were seen on average once every 2 months at an outpatient memory clinic and referred to community resources and prescribed psychotropic medications as needed. These interventions may have been effective, as no increase in ZBI scores on average was seen for any patients. In addition, the follow-up at the outpatient memory clinic was thought to have reduced the sense of burden of care for those with a high ZBI score at the beginning of the intervention. On the other hand, those with a low ZBI score at the time of the initial visit showed a gradual increase in the ZBI score. However, even in these cases, if the patients had not been followed up at the outpatient memory clinic, their ZBI scores may have worsened further. Therefore, comparative studies between outpatient memory clinics and other outpatient settings are needed in the future.
A previous longitudinal survey of caregiver burden reported that multiple groups were involved in the transition of caregiver burden [44]. In that study, only patients with AD were included and followed up over a 3-year period. Compared with the present study, the MMSE scores were lower at the initial visit because only AD was included. The trajectories of caregiver burden were differentiated into three groups, showing that the group with a high psychiatric symptom score and low daily life function at the initial visit showed a reduction in caregiver burden over the course of the study, whereas the caregiver burden tended to increase among spouses and children living with the patient [44]. The present study was similar in that the caregiver burden decreased during outpatient visits when the family caregiver had a high caregiver burden at the initial visit. However, BPSD, daily functioning, and living arrangements at the initial consultation were not found to be significantly associated with ΔZBI. The results of the present study also indicate the importance of focusing on caregiver burden at the initial visit and the changes that occur during the course of the disease, even in patients in the early stages of dementia, including those with MCI.
From the point of view of possible interventions during follow-up at an outpatient memory clinic, referrals are made to social resources that the person with dementia can use to maintain their ADL, and advice is given on how to continue social participation, depending on their condition. For family members of persons with dementia, outpatient clinics promote understanding of the disease, provide psychological support and advice on how to cope with persons with dementia, and introduce local resources that family members of persons with dementia can use for peer support [23, 45]. The regular advice given by dementia specialists varies widely depending on the situations of the patient and family caregivers. However, it is difficult to quantify each of these as an explanatory factor and verify them statistically. Family caregivers of persons with dementia often report that they expect information to be provided at medical institutions, and a practice system that meets their needs is thus likely to be important [23]. It has also been noted that referrals from medical institutions to organizations that provide peer support are inadequate [23, 46]. In the present survey, only the introduction of LTCI services as a care intervention was analyzed as an explanatory factor. In the future, it will be important to analyze the provision of information on community resources that provide peer support, such as dementia cafés and family caregiver support groups, as an explanatory factor. In addition, it would be meaningful to consider participation in dementia cafés and peer support groups for family caregivers as an integrated program along with outpatient memory clinics, and to evaluate such combination programs in terms of the caregiver burden.
If long-term and multifaceted interventions through outpatient care are considered effective, it is also necessary to examine what kind of outpatient care is effective. Although there have been reports that there is no difference between follow-up at memory clinics and follow-up by GPs, it is difficult to draw general conclusions because it is assumed that there are differences in the training of doctors in each country or region [21, 47, 48]. In addition, some medical institutions and community resources provide multidisciplinary support involving nurses, social workers, occupational therapists, and psychologists [22, 49]. A detailed comparison of each medical care system remains an issue for future research.
Differences based on diagnostic groups were investigated in the present study. MCI was included in the survey, as it affected 45.8% of the participants. Cognitive function and ADL were significantly better in the MCI than in the AD group, and psychiatric symptoms were better in the MCI than in the AD group, although this difference was not significant. Nevertheless, the caregiver burden among family caregivers of patients with MCI was similar and even higher than that in AD, although this difference was not significant. Until now, there have been limited reports on the caregiver burden of family caregivers of patients with MCI, but there have been reports that neuropsychiatric symptoms are clearly recognized in MCI [50–53]. Therefore, we believe that it is important to investigate the longitudinal course of caregiver burden from the MCI stage.
DLB was also included in this survey, albeit in small numbers, and ZBI scores were high among family caregivers of patients with DLB. There have been reports that family caregivers of patients with DLB have a strong perception of caregiver burden, and thus it is necessary to give due consideration to this [54]. However, in the present analysis, the correlation between ΔZBI and ZBI scores at the initial visit was strong, even if the analysis was limited to MCI and AD groups.
The present study has several limitations. First, it was conducted at a single outpatient memory clinic; further studies should be conducted at multiple facilities in the future. Second, it is difficult to perform long-term post-diagnosis follow-up of all patients at specialized memory clinics. This is because, in cases where patients have few psychiatric symptoms or where family caregivers are expected to be able to manage the disease on their own, they are often referred to local GPs. In the future, it will be desirable to examine the difference between continuing medical care at a specialized memory clinic and requesting continued treatment by a GP. Third, in this study, assessments of caregiving burden were conducted only twice: at the initial consultation and during the study evaluation. We plan to explore this further by increasing the number of evaluation points in future studies. This will help us determine at which point, within the average two-year evaluation intervals, the caregiving burden tends to decrease.
Conclusion
The results of the present study suggest that continuous dementia care may reduce the burden perceived by caregivers and potentially prevent deterioration, especially in pairs of patients and family caregivers experiencing a high caregiver burden. It is important to monitor the caregiver’s sense of burden while providing post-diagnosis support for patients with dementia. Regular monitoring and analysis of the caregiver burden in addition to assessments of cognitive and daily functions could be expected to provide better post-diagnosis support.
CREDIT AUTHOR STATEMENT
Hajime Takechi (Conceptualization; Formal analysis; Funding acquisition; Investigation; Writing –original draft); Hiroshi Yoshino (Investigation; Supervision; Writing –review & editing); Megumi Suzuki (Data curation; Supervision; Writing –review & editing); Akiko Maeda (Data curation; Writing –review & editing); Shota Suzumura (Data curation; Writing –review & editing); Eiko Kamiya (Data curation; Writing –review & editing).
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This work was supported by JSPS KAKENHI Grant No. JP22K02079 to Hajime Takechi. The sponsor had no role in the design, methods, data, collection, analysis, or preparation of the manuscript.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available because of privacy or ethical restrictions.
REFERENCES
[1] | GBD2019 Dementia Forecasting Collaborators ((2022) ) Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 7: , e105–e125. |
[2] | GBD 2016 Dementia Collaborators ((2019) ) Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 18: , 88–106. |
[3] | Livingston G , Sommerlad A , Orgeta V , Costafreda SG , Huntley J , Ames D , Ballard C , Banerjee S , Burns A , Cohen-Mansfield J , Cooper C , Fox N , Gitlin LN , Howard R , Kales HC , Larson EB , Ritchie K , Rockwood K , Sampson EL , Samus Q , Schneider LS , Selbæk G , Teri L , Mukadam N ((2017) ) Dementia prevention, intervention, and care. Lancet 390: , 2673–2734. |
[4] | Reed C , Belger M , Scott Andrews J , Tockhorn-Heidenreich A , Jones RW , Wimo A , Dodel R , Haro JM ((2020) ) Factors associated with long-term impact on informal caregivers during Alzheimer’s disease dementia progression: 36-month results from GERAS. Int Psychogeriatr 32: , å-277. |
[5] | Cooke DD , McNally L , Mulligan KT , Harrison MJ , Newman SP ((2001) ) Psychosocial interventions for caregivers of people with dementia: A systematic review. Aging Ment Health 5: , 120–135. |
[6] | Sörensen S , Duberstein P , Gill D , Pinquart M ((2006) ) Dementia care: Mental health effects, intervention strategies, and clinical implications. Lancet Neurol 5: , 961–973. |
[7] | Lyketsos CG , Sheppard JM , Steinberg M , Tschanz JA , Norton MC , Steffens DC , Breitner JC ((2001) ) Neuropsychiatric disturbance in Alzheimer’s disease clusters into three groups: The Cache County study. Int J Geriatr Psychiatry 16: , 1043–1053. |
[8] | Livingston G , Kelly L , Lewis-Holmes E , Baio G , Morris S , Patel N , Omar RZ , Katona C , Cooper C ((2014) ) Non-pharmacological interventions for agitation in dementia: Systematic review of randomised controlled trials. Br J Psychiatry 205: , 436–442. |
[9] | Mittelman MS , Haley WE , Clay OJ , Roth DL ((2006) ) Improving caregiver well-being delays nursing home placement of patients with Alzheimer disease. Neurology 67: , 1592–1599. |
[10] | Eska K , Graessel E , Donath C , Schwarzkopf L , Lauterberg J , Holle R ((2013) ) Predictors of institutionalization of dementia patients in mild and moderate stages: A 4-year prospective analysis. Dement Geriatr Cogn Dis Extra 3: , 426–445. |
[11] | Donnelly NA , Hickey A , Burns A , Murphy P , Doyle F ((2015) ) Systematic review and meta-analysis of the impact of carer stress on subsequent institutionalisation of community-dwelling older people. PLoS One 10: , e0128213. |
[12] | Olazaran J , Reisberg B , Clare L , Cruz I , Pena-Casanova J , Del Ser T , Woods B , Beck C , Auer S , Lai C , Spector A , Fazio S , Bond J , Kivipelto M , Brodaty H , Rojo JM , Collins H , Teri L , Mittelman M , Orrell M , Feldman HH , Muniz R ((2010) ) Nonpharmacological therapies in Alzheimer’s disease: A systematic review of efficacy. Dement Geriatr Cogn Disord 30: , 161–178. |
[13] | Brodaty H , Green A , Koschera A ((2003) ) Meta-analysis of psychosocial interventions for caregivers of people with dementia. J Am Geriatr Soc 51: , 657–664. |
[14] | Dauphinot V , Ravier A , Novais T , Delphin-Combe F , Mouchoux C , Krolak-Salmon P ((2016) ) Risk factors of caregiver burden evolution, for patients with subjective cognitive decline or neurocognitive disorders: A longitudinal analysis. J Am Med Dir Assoc 17: , 1037–1043. |
[15] | Connors MH , Seeher K , Teixeira-Pinto A , Woodward M , Ames D , Brodaty H ((2020) ) Dementia and caregiver burden: A three-year longitudinal study. Int J Geriatr Psychiatry 35: , 250–258. |
[16] | Ransmayr G , Hermann P , Sallinger K , Benke T , Seiler S , Dal-Bianco P , Marksteiner J , Defrancesco M , Sanin G , Struhal W , Guger M , Vosko M , Hagenauer K , Lehner R , Futschik A , Schmidt R ((2018) ) Caregiving and caregiver burden in dementia home care: Results from the prospective dementia registry (PRODEM) of the Austrian Alzheimer Society. J Alzheimers Dis 63: , 103–114. |
[17] | Park MH , Smith SC , Hendriks AAJ , Black N ((2019) ) Caregiver burden and quality of life 2 years after attendance at a memory clinic. Int J Geriatr Psychiatry 34: , 647–656. |
[18] | Kawaharada R , Sugimoto T , Matsuda N , Tsuboi Y , Sakurai T , Ono R ((2019) ) Impact of loss of independence in basic activities of daily living on caregiver burden in patients with Alzheimer’s disease: A retrospective cohort study. Geriatr Gerontol Int 19: , 1243–1247. |
[19] | Svendsboe EJ , Testad I , Terum T , Jörg A , Corbett A , Aarsland D , Rongve A ((2018) ) Patterns of carer distress over time in mild dementia. Int J Geriatr Psychiatry 33: , 987–993. |
[20] | van den Kieboom R , Snaphaan L , Mark R , Bongers I ((2020) ) The trajectory of caregiver burden and risk factors in dementia progression: A systematic review. J Alzheimers Dis 77: , 1107–1115. |
[21] | Draskovic I , Vernooij-Dassen M , Verhey F , Scheltens P , Rikkert MO ((2008) ) Development of quality indicators for memory clinics. Int J Geriatr Psychiatry 23: , 119–128. |
[22] | Steiner GZ , Ee C , Dubois S , MacMillan F , George ES , McBride KA , Karamacoska D , McDonald K , Harley A , Abramov G , Andrews-Marney ER , Cave AE , Hohenberg MI ((2020) ) “We need a one-stop-shop”: Co-creating the model of care for a multidisciplinary memory clinic with community members, GPs, aged care workers, service providers, and policy-makers. BMC Geriatr 20: , 49. |
[23] | Takechi H , Hara N , Eguchi K , Inomata S , Okura Y , Shibuya M , Yoshino H , Ogawa N , Suzuki M ((2023) ) Dynamics of interaction among professionals, informal supporters, and family caregivers of people with dementia along the dementia care pathway: A nationwide survey in Japan. Int J Environ Res Public Health 20: , 5044. |
[24] | National Institute for Health and Care Excellence (2018) Dementia: Assessment, management and support for people living with dementia and their carers. NICEGuideline 2018, National Institute for Health and Care Excellence (NICE), London. |
[25] | Alzheimer’s Disease International, World Alzheimer Report 2015: The Global Impact of Dementia, https://www.alz.co.uk/research/world-report-2015, |
[26] | Connors MH , Seeher K , Teixeira-Pinto A , Woodward M , Ames D , Brodaty H ((2019) ) Mild cognitive impairment and caregiver burden: A 3-year-longitudinal study. Am J Geriatr Psychiatry 27: , 1206–1215. |
[27] | McKhann GM , Knopman DS , Chertkow H , Hyman BT , Jack CR Jr. , Kawas CH , Klunk WE , Koroshetz WJ , Manly JJ , Mayeux R , Mohs RC , Morris JC , Rossor MN , Scheltens P , Carrillo MC , Thies B , Weintraub S , Phelps CH ((2011) ) The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7: , 263–269. |
[28] | Albert MS , DeKosky ST , Dickson D , Dubois B , Feldman HH , Fox NC , Gamst A , Holtzman DM , Jagust WJ , Petersen RC , Snyder PJ , Carrillo MC , Thies B , Phelps CH ((2011) ) The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7: , 270–279. |
[29] | Román GC , Tatemichi TK , Erkinjuntti T , Cummings JL , Masdeu JC , Garcia JH , Amaducci L , Orgogozo JM , Brun A , Hofman A , et al. ((1993) ) Vascular dementia: Diagnostic criteria for research studies. Reportof the NINDS-AIREN International Workshop.. Neurology 43: , 250–260. |
[30] | McKeith IG , Boeve BF , Dickson DW , Halliday G , Taylor JP , Weintraub D , Aarsland D , Galvin J , Attems J , Ballard CG , Bayston A , Beach TG , Blanc F , Bohnen N , Bonanni L , Bras J , Brundin P , Burn D , Chen-Plotkin A , Duda JE , El-Agnaf O , Feldman H , Ferman TJ , Ffytche D , Fujishiro H , Galasko D , Goldman JG , Gomperts SN , Graff-Radford NR , Honig LS , Iranzo A , Kantarci K , Kaufer D , Kukull W , Lee VMY , Leverenz JB , Lewis S , Lippa C , Lunde A , Masellis M , Masliah E , McLean P , Mollenhauer B , Montine TJ , Moreno E , Mori E , Murray M , O’Brien JT , Orimo S , Postuma RB , Ramaswamy S , Ross OA , Salmon DP , Singleton A , Taylor A , Thomas A , Tiraboschi P , Toledo JB , Trojanowski JQ , Tsuang D , Walker Z , Yamada M , Kosaka K ((2017) ) Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology 89: , 88–100. |
[31] | Folstein MF , Folstein SE , McHugh PR ((1975) ) “Mini-mental state”. Apractical method for grading the cognitive state of patients for theclinician. J Psychiatr Res 12: , 189–198. |
[32] | Yesavage JA , Brink TL , Rose TL , Lum O , Huang V , Adey M , Leirer VO ((1982) ) Development and validation of a geriatric depression screening scale: A preliminary report. J Psychiatr Res 17: , 37–49. |
[33] | Awata S , Sugiyama M , Ito K , Ura C , Miyamae F , Sakuma N , Niikawa H , Okamura T , Inagaki H , Ijuin M ((2016) ) Development of the dementia assessment sheet for community-based integrated care system. Geriatr Gerontol Int 16: (Suppl 1):123–131. |
[34] | Toyoshima K , Araki A , Tamura Y , Iritani O , Ogawa S , Kozaki K , Ebihara S , Hanyu H , Arai H , Kuzuya M , Iijima K , Sakurai T , Suzuki T , Toba K , Arai H , Akishita M , Rakugi H , Yokote K , Ito H , Awata S ((2018) ) Development of the Dementia Assessment Sheet for Community-based Integrated Care System 8-items, a short version of the Dementia Assessment Sheet for Community-based Integrated Care System 21-items, for the assessment of cognitive and daily functions. Geriatr Gerontol Int 18: , 1458–1462. |
[35] | Kaufer DI , Cummings JL , Christine D , Bray T , Castellon S , Masterman D , MacMillan A , Ketchel P , DeKosky ST ((1998) ) Assessing the impact of neuropsychiatric symptoms in Alzheimer’s disease: The Neuropsychiatric Inventory Caregiver Distress Scale. J Am Geriatr Soc 46: , 210–215. |
[36] | Kaufer DI , Cummings JL , Ketchel P , Smith V , MacMillan A , Shelley T , Lopez OL , DeKosky ST ((2000) ) Validation of the NPI-Q, a brief clinical form of the Neuropsychiatric Inventory. J Neuropsychiatry Clin Neurosci 12: , 233–239. |
[37] | Whitlatch CJ , Zarit SH , von Eye A ((1991) ) Efficacy of interventions with caregivers: A reanalysis. Gerontologist 31: , 9–14. |
[38] | Zarit SH , Reever KE , Bach-Peterson J ((1980) ) Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 20: , 649–655. |
[39] | Takechi H , Sugihara Y , Kokuryu A , Nishida M , Yamada H , Arai H , Hamakawa Y ((2012) ) Both conventional indices of cognitive function and frailty predict levels of care required in a long-term care insurance program for memory clinic patients in Japan. Geriatr Gerontol Int 12: , 630–636. |
[40] | Tsutsui T , Muramatsu N ((2007) ) Japan’s universal long-term care system reform of 2005: Containing costs and realizing a vision. J Am Geriatr Soc 55: , 1458–1463. |
[41] | Matsunaga S , Kishi T , Iwata N ((2016) ) Yokukansan in the treatment of behavioral and psychological symptoms of dementia: An updated meta-analysis of randomized controlled trials. J Alzheimers Dis 54: , 635–643. |
[42] | Harrell FE Jr Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis. Springer, New York. |
[43] | Raccichini A , Spazzafumo L , Castellani S , Civerchia P , Pelliccioni G , Scarpino O ((2015) ) Living with mild to moderate Alzheimer patients increases the caregiver’s burden at 6 months. Am J Alzheimers Dis Other Demen 30: , 463–467. |
[44] | Conde-Sala JL , Turro-Garriga O , Calvo-Perxas L , Vilalta-Franch J , Lopez-Pousa S , Garre-Olmo J ((2014) ) Three-year trajectories of caregiver burden in Alzheimer’s disease. J Alzheimers Dis 42: , 623–633. |
[45] | Jennings LA , Reuben DB , Evertson LC , Serrano KS , Ercoli L , Grill J , Chodosh J , Tan Z , Wenger NS ((2015) ) Unmet needs of caregivers of individuals referred to a dementia care program. J Am Geriatr Soc 63: , 282–289. |
[46] | Riffin C , Wolff JL , Pillemer KA ((2021) ) Assessing and addressing family caregivers’ needs and risks in primary care. J Am Geriatr Soci 69: , 432–440. |
[47] | Hum S , Cohen C , Persaud M , Lee J , Drummond N , Dalziel W , Pimlott N ((2014) ) Role expectations in dementia care among family physicians and specialists. Can Geriatr J 17: , 95–102. |
[48] | Meeuwsen EJ , Melis RJ , Van Der Aa GC , Golüke-Willemse GA , De Leest J , Van Raak FH , Schölzel-Dorenbos CJ , Verheijen DC , Verhey FR , Visser MC , Wolfs CA , Adang EM , Olde Rikkert MG ((2012) ) Effectiveness of dementia follow-up care by memory clinics or general practitioners: Randomised controlled trial. BMJ 344: , e3086. |
[49] | Lee L , Hillier LM , Stolee P , Heckman G , Gagnon M , McAiney CA , Harvey D ((2010) ) Enhancing dementia care: A primary care-based memory clinic. J Am Geriatr Soc 58: , 2197–2204. |
[50] | O’Caoimh R , Calnan M , Dhar A , Molloy DW ((2021) ) Prevalence and predictors of caregiver burden in a memory clinic population. J Alzheimers Dis Rep 5: , 739–747. |
[51] | Tsunoda K , Yamashita T , Osakada Y , Sasaki R , Tadokoro K , Matsumoto N , Nomura E , Morihara R , Nakano Y , Takahashi Y , Hatanaka N , Shang J , Sato K , Takemoto M , Hishikawa N , Ohta Y , Abe K ((2020) ) Early emergence of neuropsychiatric symptoms in cognitively normal subjects and mild cognitive impairment. J Alzheimers Dis 73: , 209–215. |
[52] | Nunes PV , Schwarzer MC , Leite REP , Ferretti-Rebustini REL , Pasqualucci CA , Nitrini R , Rodriguez RD , Nascimento CF , Oliveira KC , Grinberg LT , Jacob-Filho W , Lafer B , Suemoto CK ((2019) ) Neuropsychiatric inventory in community-dwelling older adults with mild cognitive impairment and dementia. J Alzheimers Dis 68: , 669–678. |
[53] | Köhler CA , Magalhaes TF , Oliveira JM , Alves GS , Knochel C , Oertel-Knöchel V , Pantel J , Carvalho AF ((2016) ) Neuropsychiatric disturbances in mild cognitive impairment (MCI): A systematic review of population-based studies. Curr Alzheimer Res 13: , 1066–1082. |
[54] | Kanemoto H , Sato S , Satake Y , Koizumi F , Taomoto D , Kanda A , Wada T , Yoshiyama K , Ikeda M ((2021) ) Impact of behavioral and psychological symptoms on caregiver burden in patients with dementia with Lewy bodies. Front Psychiatry 12: , 753864. |


