
Telehealth Literacy as a Social Determinant of Health: A Novel Screening Tool to Support Vulnerable Patient Equity
Abstract
Background:
Telehealth has evolved as a solution to COVID-19 isolation precautions and remote care with well-established health, socioeconomic, and practical benefits. However, there are many gaps in the current literature regarding telehealth use among older, low health literate, and resource-limited populations. There are ethical considerations that warrant understanding this digital divide.
Objective:
The objective of this review is to propose the Telehealth Literacy Screening Tool (TLST) for use in older adults and support the future inclusion of telehealth literacy as an important social determinant of health (SDOH).
Methods:
Initially a four-week outreach was performed that targeted older adults and low-health literate patients at the MedVantage Clinic (MVC) within Ochsner Health (OH) to identify common barriers to patient engagement with the OH Epic MyChart telehealth platform. Themes from those barriers directed a meta-synthetic review of the methods and ethical considerations of current, validated technological and telehealth literacy screening tools. Those findings were reported based on the standards of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement.
Results:
Based on the barriers identified during our MVC patient outreach, PRISMA-reported review of telehealth literacy screening research, and evaluation of the MyChart platform and the technological resources required for its use; we developed a multidimensional questionnaire for telehealth literacy screening of older adults.
Conclusion:
The TLST is designed to identify patients in need of additional interventions for successful connection to telehealth services. This is an important step towards addressing the ethical obligation to decrease disparities in telehealth literacy for vulnerable populations and identifying telehealth literacy as a SDOH.
INTRODUCTION
Telehealth is defined as a remote, virtual platform utilizing communicative technology to deliver medical care and health education. eHealth is the use of communication technologies to support health fields, including items such as remote monitoring devices [1]. We define telehealth literacy as a combination of elements of technologic and health literacy that allows for a patient to access, enable, and navigate their telehealth platform. Older adults, individuals living with Alzheimer’s disease and related dementias, patients who have low health literacy, and those with decreased access to services due to living in rural areas are the most vulnerable to having barriers to utilization of eHealth services [2, 3]. Further, older adults also have lower overall health status due to prevalence of chronic issues and propensity to frailty, and rural patients overall die earlier of all leading causes of death [4, 5].
Among older adults, 50 million globally are estimated to have dementia [6]. The Alzheimer’s Disease International (ADI), an umbrella organization for Alzheimer’s disease and dementia associations, reports that the 2017 WHO targets for reducing the burden of dementia remain woefully far from being met [6]. As of May 2021, only 16% of WHO member states have met the criteria in targeting dementia as a public health priority. Furthermore, a lack of consensus within the scientific community on new non-validated practices aimed at improving patients’ well-being pose increasing ethical concerns surrounding responsible application of such non-validated practices in the elderly and cognitively affected and the dissemination of misinformation [7]. These barriers, if handled immediately, would not pose insurmountable societal challenges. However, by continuing to fail in upholding our ethical responsibilities as a society, these challenges will continue to lose their status as a public health priority and further prolong our slow research process, limiting our solutions to these problems [8].
Meanwhile, the COVID-19 pandemic has led to physical distancing requirements that have resulted in the rapid adoption of telehealth and eHealth solutions [2]. Telehealth and eHealth have become essential aspects of healthcare delivery that can reduce the impact of pandemics; therefore, it is important to ensure that these services are scalable to those in most need of medical care and have cognitive and comprehension barriers. In efforts to combat some of these ethical issues, the use of assistive technology such as telehealth has been promoted as a solution to help the elderly, including people with dementia, retain their autonomy and quality of life [9].
Older adults and individuals living with dementia are more likely to have low health and digital literacy, as well as less likely and able to use patient portals or smartphone apps for health-related tasks [2, 4, 7, 10]. In 2018, it was estimated that 38% of all older adults in the United States were not ready for video visits due to reported inexperience with technology or physical disability. Factoring in the assistance of caregivers, 32% of older adults remained unready. Common challenges contributing to this technological inexperience were linked to lack of internet devices or operational knowledge as well as lack of previous experience utilizing these devices [11]. Rural and urban patients of low socioeconomic status have an additional barrier of access to services [3, 12]. To date, there is a scarce understanding of the factors influencing this ‘digital divide,’ nor how to reduce it [13].
As telehealth resources are increasingly integrated into patient care plans, we must recognize the limitations to access and navigation of telemedicine technologies for vulnerable patients. The accelerated need for telehealth and eHealth paradoxically perpetuates inequities in access to care, and a failure to intervene and reduce this digital divide inevitably leads to an expansion in the inequalities of telehealth delivery that cannot be ethically justified. Bridging this gap in telehealth literacy is both an issue of ethics and equity, and vital towards limiting health disparities [14]. As such, an ethical obligation exists to not overlook those who cannot access healthcare because they do not understand how to do so. Quantifying telehealth literacy should be viewed as a major driver of health. However, no tool currently captures telehealth competency and identifies factors that affect engagement.
METHODS
The necessity for a telehealth literacy screening tool surfaced during the peak of the COVID pandemic at OH MVC. The MVC is an innovative primary care clinic modeled to address the health and social needs of medically complex older adults in the New Orleans, Louisiana community. The clinic’s primary aim is to use person-centered and value-based healthcare practices to provide high-quality care to high-risk and older adult populations. The MVC has developed core clinical staff and uses nontraditional clinical services to target healthcare barriers and SDOH identified in this population.
The patient cohort at the MVC is comprised of a diverse, older adult, medically complex, and low-health literate population. They were at a disproportionately high risk of testing positive for COVID-19 based on the Epic COVID-19 risk model earlier on in the pandemic [15, 16]. From March– April 2020 medical students from the University of Queensland Ochsner Clinical School (UQ-OCS) attempted to train MVC patients to perform telehealth visits with the Epic MyChart platform. MyChart is a self-service web portal offered by most Epic healthcare organizations that allows patients to access their medical records and perform telehealth and eHealth services [17]. UQ-OHS students spent on average 5 hours per patient performing one-on-one training and coaching over the phone on telehealth visit navigation. By the end of this intervention period only 58 of the 309 MVC patients, or 18.8%, were able to successfully complete a virtual visit.
The primary barrier to patient engagement during the training period was lack of access to a compatible smart device. At the time of this study, virtual visits within the OH application of the MyChart platform were only compatible with a smart tablet or phone that carried Android 5.0 operating software or higher and Apple iOS 6 or higher with a front-facing camera. There was no option for laptop or computer access under this model. Overall, 27.8% of the patient cohort completed the training, had access to the correct technology that supported the application, and had a stable internet connection.
From these 90 patients, 32.56% encountered aspects of telehealth literacy that impacted success rates. Primarily, they encountered obstacles in accessing, enabling, and navigating the MyChart platform. The MyChart application requires users to log in to their respective health institution, navigate to their appointments, and complete a multi-step pre-check process. A small fraction of patients also had trouble remembering and entering their MyChart login data, and subsequently had difficulty accessing the email associated with their health data to retrieve this information. For those patients who could log on to the platform, the multi-step pre-check process impeded the patient’s progression for over half of participants. Challenging obstacles in pre-check included verifying insurance, entering personal information, signing the telehealth consent form, completing symptom-directed questionnaires, and enabling audio and video prior to the visit.
A notable influence on telehealth navigation and overall use is reliance on social support. Due to isolation precautions during the peak of the COVID-19 pandemic, we found that many older adult patients no longer had family members physically present with them to navigate the encounter that they had relied on in the past.
Overall, the clinical team concluded that successful telehealth connections were impacted by biopsychosocial features of the patient, including access to technology; literacy surrounding that technology; and literacy using eHealth process. These identified barriers guided the focus of our meta-synthetic review of current publications on telehealth and eHealth that we reported based on the standards of the PRISMA Statement (Fig. 1).
Fig. 1
PRISMA flow diagram.
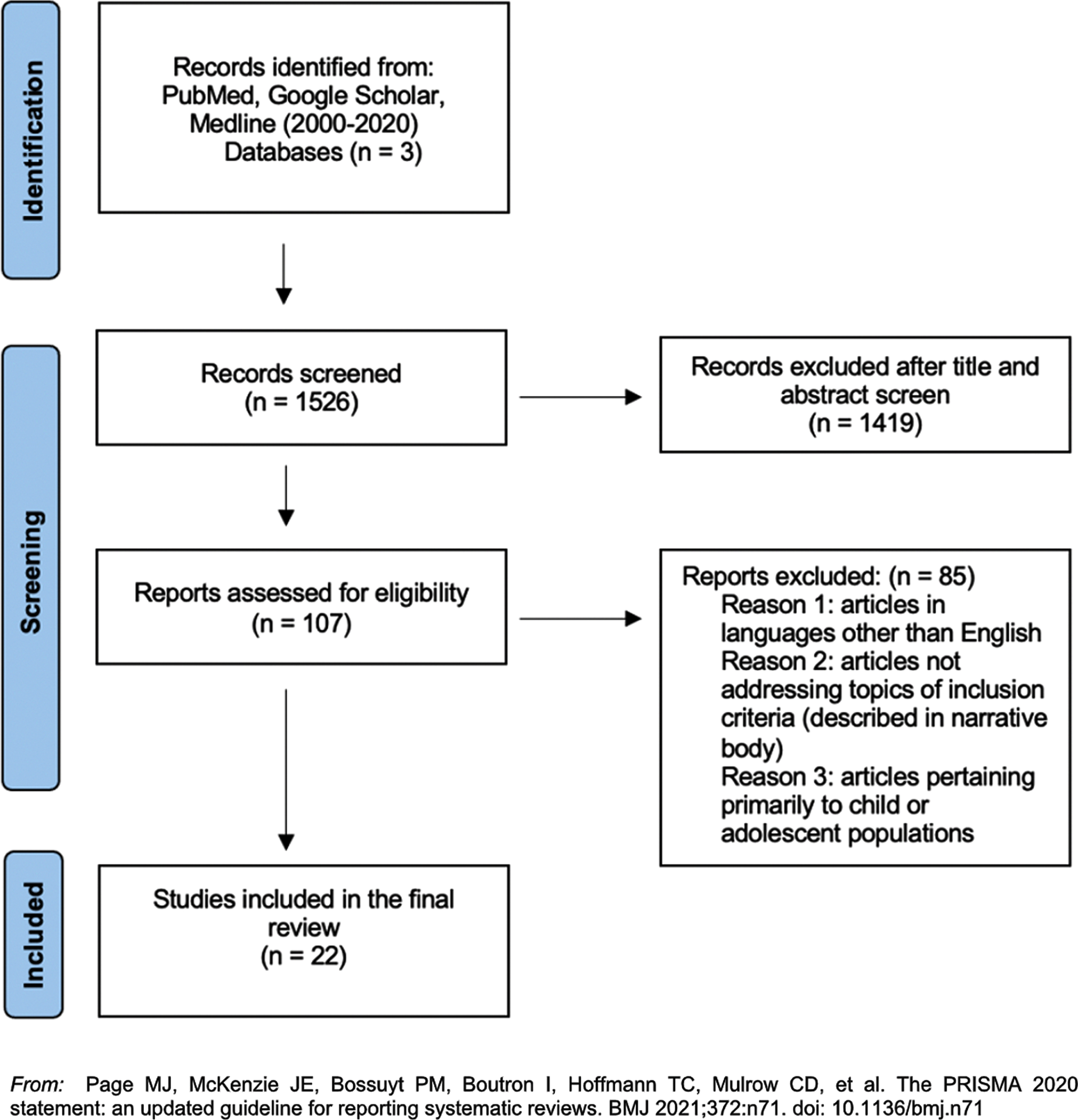
The meta-synthetic review was performed using PubMed, Google Scholar, and Medline, with a combination of search terms related to telehealth, telemedicine, and eHealth literacy, competency, or fluency in older ‘geriatric’ populations. Our initial search resulted in 1,526 articles, of which 1,419 were excluded as they did not pertain to target population, were not in English, or did not meet inclusion criteria. The remaining 107 met inclusion criteria based on title and abstract of discussing screening tools of previously stated search terms for the target population. These were all manually reviewed in full, and 85 articles were further excluded based on inclusion criteria, and the final 22 articles were included in the meta-synthetic review. After the exclusion of many tools based on our search and exclusion parameters the following ‘toolkits’ were selected because of their focus on multidomain literacies of interest: READHY, eHEALS, eHLF, eHLA, and eHLQ [12, 16– 19]. We identified key components of each tool that addressed the telehealth navigation trouble points identified in our outreach, while being mindful of selecting components that would be practical for use with older adult and low literatepopulations.
The literature review results directed our design of a novel telehealth literacy screening tool. The format of our tool is modeled after the eHLA, which is a multifaceted eHealth literacy assessment toolkit with two sections for self-reported technology familiarity and confidence surrounding both health and digital literacy [19]. With this format, we aim to capture three categories of information: biopsychosocial background including access to technology, technological literacy screening, and eHealth literacy screening.
We created biopsychosocial background questions based on multiple studies which found that advanced age, access to technology and internet, cognitive barriers, and audiovisual impairments were predictors of need for eHealth assistance [18, 20, 21]. For these reasons, evaluation of technology access, cognitive skills and physical abilities were central aspects in our tool design. Key intrinsic factors that we aim to capture with our tool include perceived self-efficacy and readiness (i.e., knowledge, skills, trust, and motivation), because these impact a patient’s willingness to overcome barriers with eHealth use [21– 23]. Finally, we incorporated social support as a factor in telehealth integration and use [19, 22, 24– 26]. These concepts are captured in the biopsychosocial background section of our survey.
The technological literacy portion of our survey assesses the skills needed for digital navigation of the home screen, such as exiting and opening applications, altering device settings, scrolling up and down, and inputting and deleting text. We focus on comfortability with navigating applications specifically while interacting with crucial text, buttons, and icons [22, 24]. The functional and communicative literacies described by Paige et al. were considered when developing the operative skills questions that evaluate for the ability to identify, navigate and operantly respond to information [16, 27]. Although other investigators have explored length of time of use of a smart phone or tablet as a predictor of needing assistance, our survey focuses on the multidimensional nature of comfort with digital interactions and does not include questions about length of time of use [16, 21]. Instead, we assess for frequency of technology usage [12].
The goal of the eHealth section is to gauge an individual’s baseline ability and engagement with the current OH telehealth services. We assess for functional literacy and comfortability with the MyChart application and accessing the email connected to their MyChart account while on a smart device. The eHealth-inspired questions are based on the critical and translational literacies as conceptualized by Paige et al., such as the ability to discern and apply telehealth-relevant information [27].
RESULTS
With input from a targeted intervention to increase telehealth use among complex, older adult patients at OH as well as an in-depth review of validated technological and health literacy screening tool models; we developed the Telehealth Literacy Screening Tool (TLST). The goal of the TLST is to better understand the unique barriers that older, low telehealth literate and resource-challenged populations face in telehealth utilization.
The TLST is organized into three parts: biopsychosocial background including access to technology, technological literacy screening, and eHealth literacy screening (Supplementary Material). The biopsychosocial section consists of eight questions, many of which can be completed by chart review. The final two sections are each composed of four questions that are asked of the patient, each with quantifiable answers. The technological literacy screening section assesses for access to technology, and the eHealth literacy screening section evaluates knowledge and comfortability of usage of the technology and Epic MyChart. Our answer options mirror the eHLA 1- 2 grading scale for simplicity, with an added 0 for null answers [19]. “No”, “Never” or “Unsure” was 0; “Sometimes” and “Yes” was 1; and “Frequently” was 2.
The TLST can be performed over the phone or in-person as determined by patient comfort. Given that the target audience for the TLST is older adults and complex patients, having “a real person” as the interview operator, even if over the phone, is the ideal method of survey delivery [18].
DISCUSSION
Further research is needed to determine validity and reliability of this screening tool and determine cutoff points predicting how TLST scores among patients predict various degrees of success within the given telehealth system. Stratifying patients based on clinical predictability of successful telehealth use with the TLST is currently underway at the MVC, while the Innovation Ochsner (iO) Department is exploring utilization of aspects of the tool within the OH Epic platform. This work will support validation of the TLST thereby overcoming the challenge with current technological screening tools, which assume a dichotomy of high and low telehealth literacy with arbitrarily set cutoff points [27].
The predominant focus of our tool is to better understand the barriers to telehealth use; however, it was developed in relation to the MyChart platform. While the TLST may be applied to wider audiences and health systems utilizing the MyChart telehealth platform following validation, it would need to be modified if it were to be scaled beyond hospital systems that utilize Epic.
Potential impacts of the TLST include increasing awareness and depth of understanding of the unique barriers that older adults, individuals living with Alzheimer’s disease and related dementias, and vulnerable populations face in telehealth utilization. The results from a system-wide application of TLST could also be used to address context-specific issues faced during telehealth interactions and offer an opportunity to develop accommodations for patients accordingly.
Lastly, we aim to increase recognition of telehealth literacy and access to technology as an evolving SDOH. This carries an ethical obligation to address telehealth literacy to avoid structural violence against vulnerable populations in the new age of virtual medicine. To support improved health equity and uniform use of eHealth systems, we must also look beyond intermediary initiatives and develop equitable strategies across policy, practice, research, and implementation. Exploring methods of data collection on telehealth literacy is the start of this process.
Utilization of the TLST will generate new evidence surrounding telehealth literacy to direct the development of adaptations and accommodations for vulnerable populations, expand engagement of stakeholders, and contribute to the body of knowledge supporting telehealth literacy as an SDOH.
ACKNOWLEDGMENTS
We thank Emily Rosensweig, PhD and Elizabeth Mulcahy, NP, for their input on survey development, the University of Queensland Ochsner Clinical School medical students who collected data in the MVC, and Paige Pielet for manuscript revision.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/ADR-210024.
REFERENCES
[1] | Triana AJ , Gusdorf RE , Shah KP , Horst SN ((2020) ) Technology literacy as a barrier to telehealth during COVID-19. Telemed J E Health 26: , 1118–1119. |
[2] | Perez-Stable EJ , El-Toukhy S ((2018) ) Communicating with diverse patients: How patient and clinician factors affect disparities. Patient Educ Couns 101: , 2186–2194. |
[3] | Price-Haywood EG , Harden-Barrios J , Ulep R , Luo Q ((2017) ) eHealth literacy: Patient engagement in identifying strategies to encourage use of patient portals among older adults. Popul Health Manag 20: , 486–494. |
[4] | Lam K , Lu AD , Shi Y , Covinsky KE ((2020) ) Assessing telemedicine unreadiness among older adults in the United States during the COVID-19 pandemic. JAMA Intern Med 180: , 1389–1391. |
[5] | Parker S , Prince A , Thomas L , Song H , Milosevic D , Harris MF , Group IS ((2018) ) Electronic, mobile and telehealth tools for vulnerable patients with chronic disease: A systematic review and realist synthesis. BMJ Open 8: , e019192. |
[6] | The Lancet N ((2021) ) Amid competing priorities, dementia must not be forgotten. Lancet Neurol 20: , 685. |
[7] | Daly T , Mastroleo I , Gorski D , Epelbaum S ((2020) ) The ethics of innovation for Alzheimer’s disease: The risk of overstating evidence for metabolic enhancement protocols. Theor Med Bioeth 41: , 223–237. |
[8] | Davis DS ((2017) ) Ethical issues in Alzheimer’s disease research involving human subjects. J Med Ethics 43: , 852–856. |
[9] | Zwijsen SA , Niemeijer AR , Hertogh CM ((2011) ) Ethics of using assistive technology in the care for community-dwelling elderly people: An overview of the literature. Aging Ment Health 15: , 419–427. |
[10] | Lind L , Karlsson D ((2014) ) Telehealth for “the digital illiterate”–elderly heart failure patients experiences. Stud Health Technol Inform 205: , 353–357. |
[11] | Huhta AM , Hirvonen N , Huotari ML ((2018) ) Health literacy in web-based health information environments: Systematic review of concepts, definitions, and operationalization for measurement. J Med Internet Res 20: , e10273. |
[12] | Kayser L , Karnoe A , Furstrand D , Batterham R , Christensen KB , Elsworth G , Osborne RH ((2018) ) A multidimensional tool based on the eHealth literacy framework: Development and initial validity testing of the eHealth Literacy Questionnaire (eHLQ). J Med Internet Res 20: , e36. |
[13] | van Houwelingen CT , Ettema RG , Antonietti MG , Kort HS ((2018) ) Understanding older people’s readiness for receiving telehealth: Mixed-method study. J Med Internet Res 20: , e123. |
[14] | Antonio MG , Petrovskaya O , Lau F ((2019) ) Is research on patient portals attuned to health equity? A scoping review. J Am Med Inform Assoc 26: , 871–883. |
[15] | Miller DP Jr. , Weaver KE , Case LD , Babcock D , Lawler D , Denizard-Thompson N , Pignone MP , Spangler JG ((2017) ) Usability of a novel mobile health iPad app by vulnerable populations. JMIR Mhealth Uhealth 5: , e43. |
[16] | Stellefson M , Paige SR , Tennant B , Alber JM , Chaney BH , Chaney D , Grossman S ((2017) ) Reliability and validity of the telephone-based eHealth literacy scale among older adults: Cross-sectional survey. J Med Internet Res 19: , e362. |
[17] | Garvelink MM , Agbadje TT , Freitas A , Bergeron L , Petitjean T , Dugas M , Blair L , Archambault P , Roy N , Jones A , Legare F ((2020) ) Improving a web-based tool to support older adults to stay independent at home: Qualitative study. JMIR Mhealth Uhealth 8: , e16979. |
[18] | Kayser L , Rossen S , Karnoe A , Elsworth G , Vibe-Petersen J , Christensen JF , Ried-Larsen M , Osborne RH ((2019) ) Development of the multidimensional Readiness and Enablement Index for Health Technology (READHY) tool to measure individuals’ health technology readiness: Initial testing in a cancer rehabilitation setting. J Med Internet Res 21: , e10377. |
[19] | Wildenbos GA , Jaspers MWM , Schijven MP , Dusseljee-Peute LW ((2019) ) Mobile health for older adult patients: Using an aging barriers framework to classify usability problems. Int J Med Inform 124: , 68–77. |
[20] | Banbury A , Nancarrow S , Dart J , Gray L , Parkinson L ((2018) ) Telehealth interventions delivering home-based support group videoconferencing: Systematic review. J Med Internet Res 20: , e25. |
[21] | Winbush GB , McDougle L , Labranche L , Khan S , Tolliver S ((2013) ) Health empowerment technologies (HET): Building a web-based tool to empower older African American patient-doctor relationships. J Health Care Poor Underserved 24: , 106–117. |
[22] | Levin-Zamir D , Bertschi I ((2018) ) Media health literacy, eHealth literacy, and the role of the social environment in context. Int J Environ Res Public Health 15: . |
[23] | Paige SR , Stellefson M , Krieger JL , Anderson-Lewis C , Cheong J , Stopka C ((2018) ) Proposing a transactional model of ehealth literacy: Concept analysis. J Med Internet Res 20: , e10175. |
[24] | Hyde LL , Boyes AW , Mackenzie LJ , Leigh L , Oldmeadow C , Riveros C , Sanson-Fisher R ((2019) ) Electronic health literacy among magnetic resonance imaging and computed tomography medical imaging outpatients: Cluster analysis. J Med Internet Res 21: , e13423. |
[25] | Paige SR , Stellefson M , Krieger JL , Miller MD , Cheong J , Anderson-Lewis C ((2019) ) Transactional eHealth literacy: Developing and testing a multi-dimensional instrument. J Health Commun 24: , 737–748. |
[26] | Roque NA , Boot WR ((2018) ) A new tool for assessing mobile device proficiency in older adults: The Mobile Device Proficiency Questionnaire. J Appl Gerontol 37: , 131–156. |
[27] | Roberts ET , Mehrotra A ((2020) ) Assessment of disparities in digital access among medicare beneficiaries and implications for telemedicine. JAMA Intern Med 180: , 1386–1389. |


