
Sex as a Risk Factor for Developing Cognitive Impairments in National Alzheimer’s Coordinating Center Participants
Abstract
Background:
It is inconclusive on how sex affects the risk of developing mild cognitive impairment (MCI) or dementia.
Objective:
To investigate how sex affects the risk of developing MCI or dementia.
Methods:
A secondary data analysis was performed on data collected from participants enrolled at Alzheimer’s Disease Research Centers funded by National Institute on Aging. There were two inclusion criteria: 1) participants were free of dementia at the baseline visit; 2) every participant must have at least one follow-up visit. A Cox proportional hazards model was used to investigate how sex affects the risk of developing cognitive impairments.
Results:
During a follow-up period of more than 10 years, male participants had a slightly higher incidence than female participants for either MCI or dementia. Not surprisingly, a higher prevalence was observed in male than female participants for either MCI or dementia. However, male participants had a higher mortality rate than their female counterparts.
Conclusion:
The male sex is associated with a higher risk for developing cognitive impairments along the aging process.
INTRODUCTION
Mild cognitive impairment (MCI) and dementia represent the early and advanced stages in the spectrum of cognitive deterioration respectively. Both the incidence of MCI [1] and the prevalence of dementia [2, 3] increased along with the aging process. However, it is inconclusive on how sex interacts with the aging to affect the risk of developing MCI or dementia. As reported, neither prevalence nor incidence of MCI had statistically significant sex differences [3–5]. In addition, no sex difference was observed with either incidence [6] or prevalence of dementia [2, 3]. By contrast, women were observed for having a higher prevalence of MCI than men from two Chinese studies [7, 8]. Interestingly, a higher prevalence of MCI was seen in men than women from a community-based sample [9]. Therefore, our study aimed to investigate how sex interacts with age to affect the risk of developing MCI or dementia using data collected from participants of National Institute on Aging-funded Alzheimer’s Disease Research Centers (ADRCs).
METHODS
Participants
National Alzheimer’s Coordinating Center (NACC) has the data collected from participants of National Institute on Aging-funded ADRCs [10]. Participants are recruited from different sources including references from a relative, friend, or clinician, ADRC solicitation, non-ADRC media appeal, and other community outreach efforts [11]. Demographic information, medical history, neurological examination, and neuropsychological assessment are collected during annual visits [12]. Participants included in the current study met the following three criteria: 1) who were evaluated between 06/09/2005 and 08/14/2016 as part of the Uniform Data Set (UDS); 2) who did not have a diagnosis of dementia at the baseline; 3) who had at least one follow-up visit. In total, there are 8,467 participants, of which 2,868 are males and 5,599 are females. Both demographic information and apolipoprotein (APOE) ɛ4 carrier status were compared between male and female participant groups (Table 1).
Table 1
Demographic and genetic information were compared between male and female participant groups
| Male (n = 2,868) | Female (n = 5,599) | p | |
| Age (y) | 72.84±10.55 | 71.66±10.51 | <0.001 |
| Education (y) | 16.50±3.0 | 15.51±2.82 | <0.001 |
| APOE ɛ4 Carrier | 1,719/719/430 | 3,307/1,427/865 | 0.835 |
| Status (+/-/unknown) | (59.94% /25.07% /14.99%) | (59.06% / 25.49% /15.45%) | |
| Race (White/ | 2573/207/88 | 4,636/782/181 | <0.001 |
| Black/Other) | (89.71% /7.22% /3.07%) | (82.8% /13.97% /3.23%) |
Both age and education are shown in the format of mean±SD. APOE, Apolipoprotein epsilon; SD, standard deviation.
Cognitive diagnosis
As part of the UDS, cognitive assessment data were collected from participants on an approximately annual basis [11]. If a participant missed the annual follow-up visit window, the next assessment would be accepted by the NACC as the subsequent visit. Cognitive diagnoses were made either by a single clinician or a multi-disciplinary consensus team using neuropsychological performance, neurological examination results, and medical history details. Cognitive diagnosis classifications relevant to the current study included normal cognition (NC), MCI, and dementia.
NC was defined by 1) Clinical Dementia Rating (CDR)=0 (no dementia) [13]; 2) no deficits in activities of daily living directly attributable to cognitive impairment; and 3) no evidence of objective cognitive impairment. NC was defined as performance falling less than 1.5 standard deviations within the age-adjusted normative mean on neuropsychological tests assessing language, attention, memory, and executive functioning [11].
MCI determinations were based upon Petersen criteria [14] and defined as 1) a CDR ≤0.5 (reflecting mild severity of impairment); 2) relatively spared instrumental activities of daily living; 3) objective cognitive impairment in at least one domain (i.e., performance falling greater than 1.5 standard deviations outside the age-adjusted normative mean in memory, language, attention, or executive functioning) or a significant cognitive decline over time on the neuropsychological evaluation; 4) Mini-Mental State Examination (MMSE)≥23 [15, 16]; 5) report of a cognitive change by the patient or informant or as observed by a clinician; and 6) absence of dementia.
Dementia was defined as meeting criteria for Alzheimer’s disease (AD) [17] or other dementias [18–23] defined as 1) objective cognitive impairment (i.e., performances falling greater than 1.5 standard deviations outside the age-adjusted normative mean) in at least two cognitive systems (i.e., memory, language, attention or executive functioning); and 2) cognitive impairment contributes directly to impaired activities of daily living.
Statistical analysis, tables, and figures
SPSS (version 26.0) was used for all statistical analyses. Descriptive analyses of demographic and clinical variables were compared between male and female participants. Means (and standard deviation) or frequencies were calculated for the demographic variables of age, education, race, and APOE ɛ4 carrier status [24]. Two-sample t-tests were used to compare age and education between the male and female participant groups. Chi-square tests were used to compare the race and APOE ɛ4 carrier status between the male and female participant groups (Table 1).
A Cox proportional hazards model was used to investigate how sex affects the risk of developing cognitive impairments with considering baseline age, level of education, race and APOE ɛ4 carrier status. Then incidence of MCI and its subtypes: amnestic MCI (aMCI) and non-amnestic MCI (naMCI), dementia or mortality was compared between the male and female participant groups during the whole follow-up period of more than 10 years. The prevalence of MCI or dementia was also calculated between the two participant groups and plotted against the annual follow-up visits. Data were presented in the form of mean±standard deviation, and p < 0.05 was considered as significant in all statistical analyses. Figures were created using Microsoft Excel.
Standard protocol approvals, registrations, and patient consents
All contributing ADRCs are required to obtain informed consent from their participants and maintain their own separate IRB review and approval from their institution prior to submitting data to the NACC.
Data availability statement
Data and analytical methods are carefully documented for the performed study. Any data-sharing request can only submit to the NACC for approval purpose.
RESULTS
At the baseline, male and female participants were significantly different pertaining to age, education, and race but not the APOE ɛ4 carrier status (Table 1). The baseline age for male participants was 72.84±10.55, which was slightly older than that of 71.66±10.51 years old for the female participants (p < 0.001). For education, the two sexes had an average of college education although the average of education level (in years) was slightly higher in males than females (p < 0.001). For Race, there was a higher percentage of Whites in the male participant group than the female participant group (p < 0.001). However, the male and female participant groups were comparable according to the APOE ɛ4 carrier status.
From the Cox regression analyses, the haphazard coefficient is around –0.25 for developing MCI. The female group had a lower risk for MCI than the male group with the average relative risk being 0.78 (95% confidence interval: 0.75–0.82; p < 0.001). Similarly, the haphazard coefficient is around –0.21 for developing dementia. The female group had a lower risk for dementia than the male group with the average relative risk being 0.81 (95% confidence interval: 0.71-0.92; p = 0.001).
Next, the incidence of MCI, dementia or mortality was compared between the male and female participant groups (Table 2). The males had a slightly higher incidence of MCI or dementia. For either amnestic or non-amnestic subtypes of MCI, a higher incidence was observed in the male than the female participant group (Table 2). Not surprisingly, the mortality rate was also higher in the male participant group. In order to ascertain if a younger death age in the males was the reason for their slightly higher mortality than females, the death age was compared between the male and female participant groups. Surprisingly, the death age was comparable between the two sexes. Death age for male participants was 89.12±6.77, which is not significantly different from that for female participants of 89.06±8.3 (p = 0.99).
Table 2
The incidence of MCI, dementia or mortality was compared between male and female participant groups
| Male (N = 2,868) | Female (N = 5,599) | Risk Ratio (95% confidence interval) | |
| MCI | 185.19/1000 person-years | 157.48/1000 person-years | 1.18 (1.18–1.25) |
| aMCI | 210.13/1000 person-years | 189.22/1000 person-years | 1.11 (1.03–1.34) |
| naMCI | 107.32/1000 person-years | 94.61/1000 person-years | 1.13 (1.05–1.34) |
| Dementia | 30.52/1000 person-years | 26.06/1000 person-years | 1.17 (1.09–1.29) |
| Mortality | 177.77/1000 person-years | 140.54/1000 person-years | 1.26 (1.04–1.41) |
MCI, mild cognitive impairment; aMCI, amnestic MCI; naMCI, non-amnestic MCI.
Last, the prevalence of either MCI or dementia was compared between the two sex groups (Figs. 1 and 2). For MCI, the male participant group always had a higher prevalence than the female participant group for the whole follow-up duration. The prevalence had a steadily up-going phase for the first 5 years, which was followed by a plateau phase of about 3 years and down-going phase after that. Interestingly, the prevalence for the male participant group went down around the eighth year of follow-up and then the two sexes had comparable prevalence.
Fig.1
A higher prevalence of mild cognitive impairment (MCI) was seen in male than female participants.
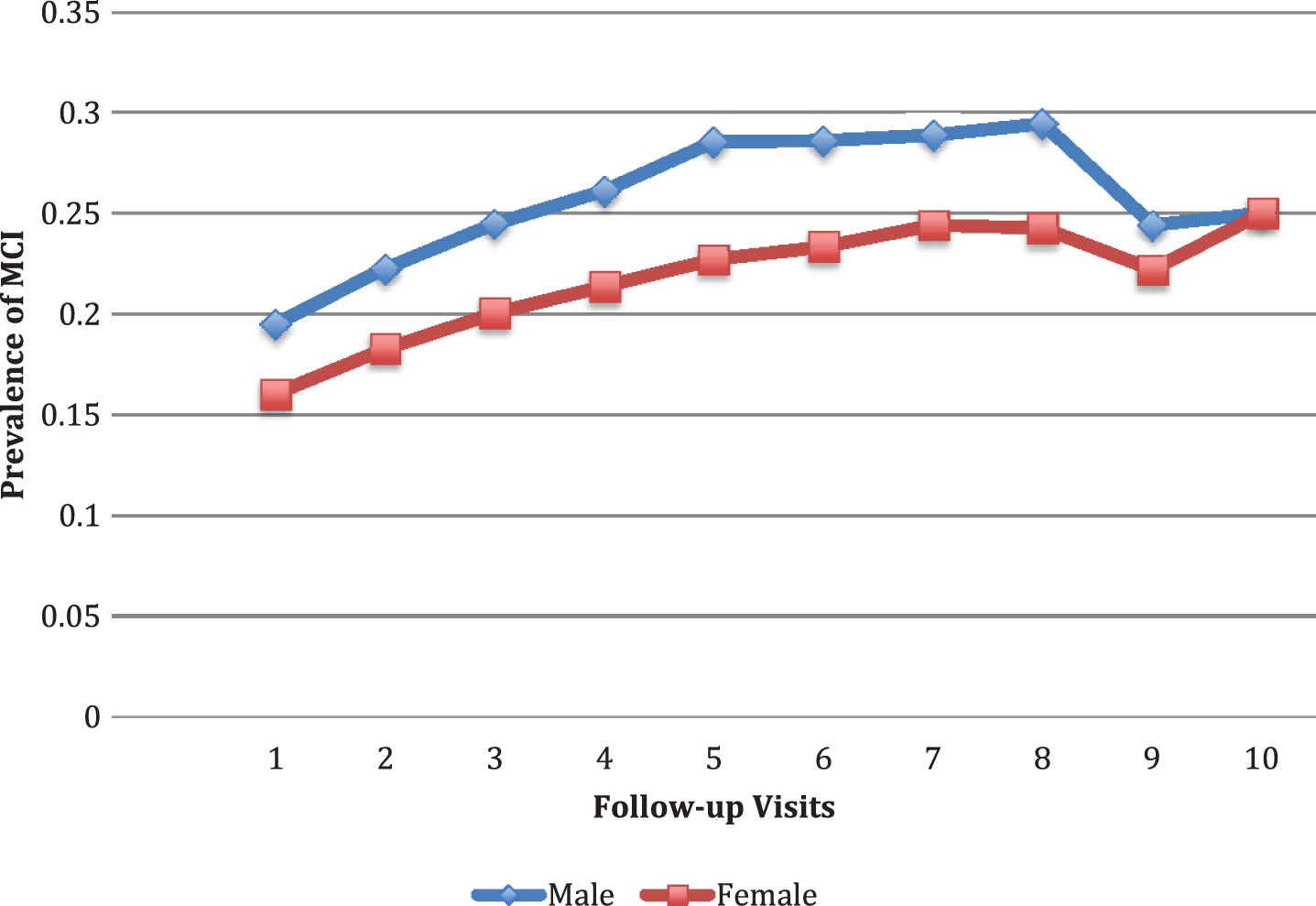
Fig.2
A higher prevalence of dementia was seen in male than female participants.
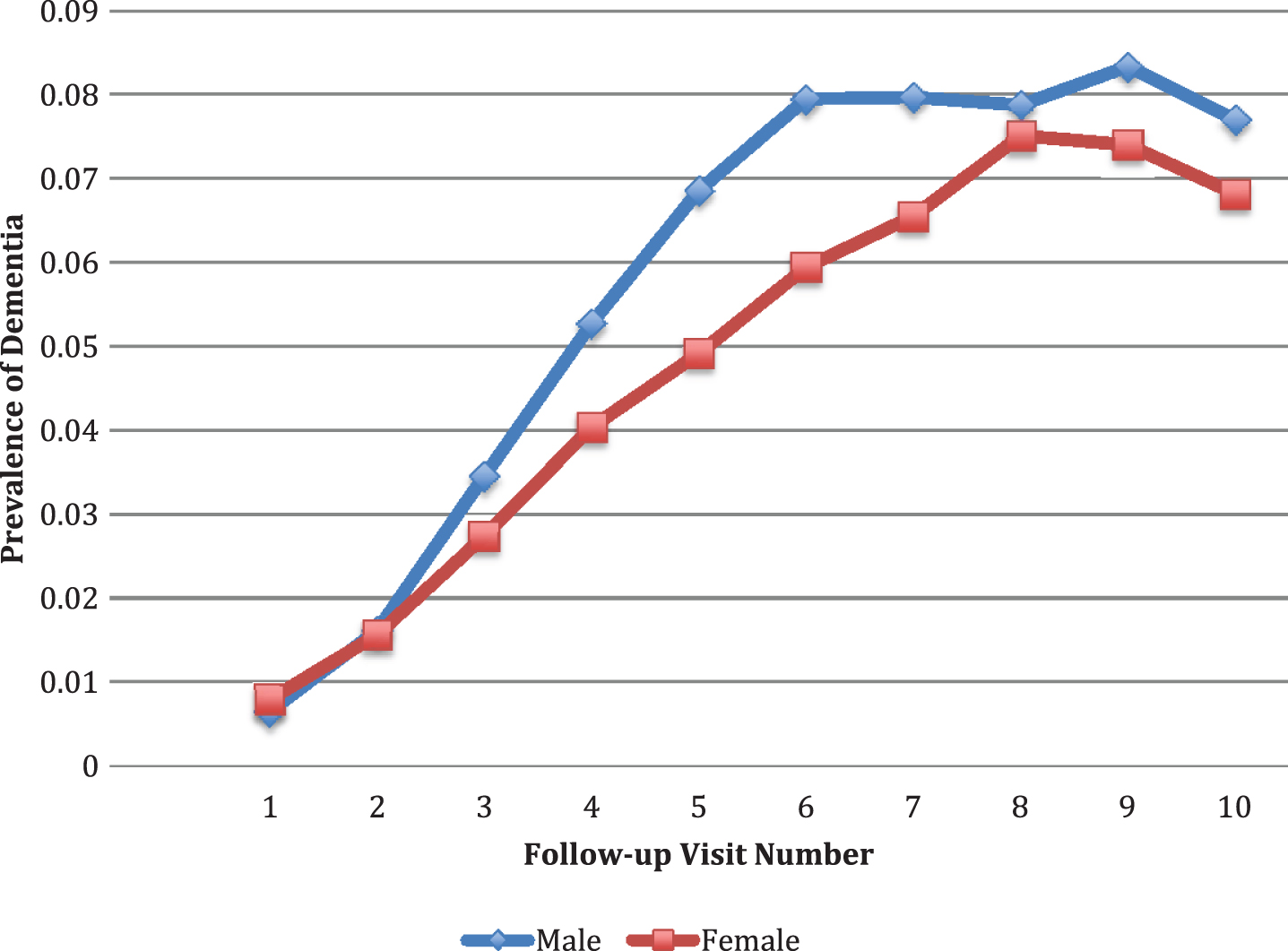
For dementia, the male participant group had a higher prevalence than the female participant group for the whole follow-up duration. Although the prevalence was getting close to each other between the two sex groups around the eighth follow-up year, the prevalence of dementia in male participant group was always higher than the female participant group as a pattern.
DISCUSSION
Both incidence and prevalence of MCI were higher in the male than the female participant group (Table 2 and Fig. 1). The overall prevalence of MCI in our study was consistent with what has been reported in a previous study [8]. Regarding to the aMCI, our findings are consistent with previous reports that men had a higher prevalence than women [25, 26]. However, women were reported for having a higher prevalence of naMCI than men [4].
The prevalence of dementia in our study is comparable to those from a Korean study with an elderly population [27]. It is worthy to note that our study sample does represent a population instead of a convenience sample. By contrast, a higher prevalence of dementia had been reported by another recent study, in which the participants were adults aged 70 and above [28]. The baseline age is different from those participants in our study, which might explain the discrepancy on the dementia prevalence, as aging by itself is a significant risk factor for dementia [2, 3]. As shown from our data, if the death age were comparable between the sexes, males would have a higher incidence or prevalence of either MCI or dementia than females.
Although female sex was reported as a risk factor for AD in some studies [6, 29], our specific dataset did not have information for us to differentiate AD and other types of dementia. Therefore, it is beyond the scope of the current study to compare incidence or prevalence of AD between the two sexes.
The current study has a number of strengths. The large NACC sample size offered power to detect even modest effects of sex on incidence or prevalence of MCI or dementia. Additionally, the diagnostic criteria for NC, MCI, and dementia are standard across participating sites, which made it possible for obtaining a decent sample from the NACC UDS. At last, the longitudinal follow-up represents an important methodological strength, allowing us to better delineate how sex interacts with age to affect the incidence as well as prevalence of MCI or dementia. Despite these strengths, there are some limitations for the current study. Participants comprising the NACC dataset represent a convenience sample, including clinical-referrals and community-based volunteers who are predominantly White and well educated. The prevalence was calculated using number of affected individuals MCI or dementia divided by the total number of observed participants, which did catch the effects of follow-up losses. In addition, there are more female participants than male participants, which might reflect the difference on the willingness to participate in study or how do they approach healthcare between the two sexes. Thus, forming comparison groups based on sex could bring selection biases to the observed outcomes. Collectively, these factors limit the generalizability of our findings.
To summarize, male sex itself is a risk factor for developing cognitive impairments of either MCI or dementia. It was reported sex specific degenerations occurred along with aging in certain subcortical brain structures including basal ganglia, thalamus, hippocampus, and amygdala [30]. For example, hippocampus degeneration was only observed in males, whereas disproportionate degeneration in the basal ganglia and thalamus was specific for females [30]. The different sex-specific degenerations of subcortical brain structures explains not only why sex plays a role in the different incidence and prevalence of MCI or dementia but also those differences in the subtypes of MCI or dementia. Nonetheless, many other factors are known to be involved in the cognitive impairment development including education [3, 29], APOE ɛ4 carrier status, and race, which in turn are closely related to either incidence or prevalence of MCI or dementia. For example, rates of aMCI increased significantly with age in men and in Blacks [26]. In addition, the prevalence of dementia increased in subjects with a low level of education [3]. Therefore, it is important to consider all these factors when studying the role of sex in the process of cognitive deteriorations.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
ACKNOWLEDGMENTS
The NACC database is funded by NIA/NIH Grant U01 AG016976. NACC data are contributed by the NIA-funded ADCs: P30 AG019610 (PI Eric Reiman, MD), P30 AG013846 (PI Neil Kowall, MD), P50 AG008702 (PI Scott Small, MD), P50 AG025688 (PI Allan Levey, MD, PhD), P50 AG047266 (PI Todd Golde, MD, PhD), P30 AG010133 (PI Andrew Saykin, PsyD), P50 AG005146 (PI Marilyn Albert, PhD), P50 AG005134 (PI Bradley Hyman, MD, PhD), P50 AG016574 (PI Ronald Petersen, MD, PhD), P50 AG005138 (PI Mary Sano, PhD), P30 AG008051 (PI Thomas Wisniewski, MD), P30 AG013854 (PI M. Marsel Mesulam, MD), P30 AG008017 (PI Jeffrey Kaye, MD), P30 AG010161 (PI David Bennett, MD), P50 AG047366 (PI Victor Henderson, MD, MS), P30 AG010129 (PI Charles DeCarli, MD), P50 AG016573 (PI Frank LaFerla, PhD), P50 AG005131 (PI James Brewer, MD, PhD), P50 AG023501 (PI Bruce Miller, MD), P30 AG035982 (PI Russell Swerdlow, MD), P30 AG028383 (PI Linda Van Eldik, PhD), P30 AG053760 (PI Henry Paulson, MD, PhD), P30 AG010124 (PI John Trojanowski, MD, PhD), P50 AG005133 (PI Oscar Lopez, MD), P50 AG005142 (PI Helena Chui, MD), P30 AG012300 (PI Roger Rosenberg, MD), P30 AG049638 (PI Suzanne Craft, PhD), P50 AG005136 (PI Thomas Grabowski, MD), P50 AG033514 (PI Sanjay Asthana, MD, FRCP), P50 AG005681 (PI John Morris, MD), P50 AG047270 (PI Stephen Strittmatter, MD, PhD).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/ADR-200275.
REFERENCES
[1] | Ganguli M , Fu B , Snitz BE , Hughes TF , Chang CC ((2013) ) Mild cognitive impairment: incidence and vascular risk factors in a population-based cohort. Neurology 80: , 2112–2120. |
[2] | Fratiglioni L , Grut M , Forsell Y , Viitanen M , Grafström M , Holmén K , Ericsson K , Bäckman L , Ahlbom A , Winblad B ((1991) ) Prevalence of Alzheimer’s disease and other dementias in an elderly urban population: relationship with age, sex, and education. Neurology 41: , 1886–1892. |
[3] | Prencipe M , Casini AR , Ferretti C , Lattanzio MT , Fiorelli M , Culasso F ((1996) ) Prevalence of dementia in an elderly rural population: effects of age, sex, and education. J Neurol Neurosurg Psychiatry 60: , 628–633. |
[4] | Au B , Dale-McGrath S , Tierney MC ((2017) ) Sex differences in the prevalence and incidence of mild cognitive impairment: A meta-analysis. Ageing Res Rev 35: , 176–199. |
[5] | Overton M , Pihlsgård M , Elmståhl S ((2019) ) Prevalence and incidence of mild cognitive impairment across subtypes, age, and sex. Dement Geriatr Cogn Disord 47: , 219–232. |
[6] | Gao S , Hendrie HC , Hall KS , Hui S ((1998) ) The relationships between age, sex, and the incidence of dementia and Alzheimer disease: a meta-analysis. Arch Gen Psychiatry 55: , 809–815. |
[7] | Ma F , Wu T , Zhao J , Ji L , Song A , Zhang M , Huang G ((2016) ) Prevalence of mild cognitive impairment and its subtypes among Chinese older adults: role of vascular risk factors. Dement Geriatr Cogn Disord 41: , 261–272. |
[8] | Zhang Y , Guan Y , Shi Z , Yue W , Liu S , Liu S , Lu H , Zhao L , Zhang Y , Su W , Ji Y ((2019) ) Sex differences in the prevalence of and risk factors for cognitive impairment no dementia among the elderly in a rural area of Northern China: a population-based cross-sectional study. Neuroepidemiology 52: , 25–31. |
[9] | Petersen RC , Roberts RO , Knopman DS , Geda YE , Cha RH , Pankratz VS , Boeve BF , Tangalos EG , Ivnik RJ , Rocca WA ((2010) ) Prevalence of mild cognitive impairment is higher in men. The Mayo Clinic Study of Aging. Neurology 75: , 889–897. |
[10] | Morris JC , Weintraub S , Chui HC , Cummings J , Decarli C , Ferris S , Foster NL , Galasko D , Graff-Radford NR , Peskind E , Beekly DL , Ramos EM , Kukull WA ((2006) ) The Uniform Data Set (UDS): Clinical and cognitive variables and descriptive data from Alzheimer Disease Centers. Alzheimer Dis Assoc Disord 20: , 210–216. |
[11] | Weintraub S , Salmon D , Mercaldo N , Ferris S , Graff-Radford NR , Chui HC , Cummings J , Decarli C , Foster NL , Galasko D , Peskind E , Beekly DL , Kukull WA , Morris JC ((2009) ) The Alzheimer’s Disease Centers’ Uniform Data Set (UDS): the neuropsychologic test battery. Alzheimer Dis Assoc Disord 23: , 91–101. |
[12] | Beekly DL , Ramos EM , Lee WW , Deitrich WD , Jacka ME , Wu J , Hubbard JL , Koepsell TD , Morris JC , Kukull WA ((2007) ) The National Alzheimer’s Coordinating Center (NACC) database: the Uniform Data Set. Alzheimer Dis Assoc Disord 21: , 249–258. |
[13] | Morris JC ((1993) ) The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology 43: , 2412–2414. |
[14] | Petersen RC ((2004) ) Mild cognitive impairment as a diagnostic entity. J Intern Med 256: , 183–194. |
[15] | Folstein MF , Folstein SE , McHugh PR ((1975) ) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: , 189–198. |
[16] | Mitchell AJ ((2009) ) A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J Psychiatr Res 43: , 411–431. |
[17] | McKhann G , Drachman D , Folstein M , Katzman R , Price D , Stadlan EM ((1984) ) Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 34: , 939–944. |
[18] | McKeith IG , Galasko D , Kosaka K , Perry EK , Dickson DW , Hansen LA , Salmon DP , Lowe J , Mirra SS , Byrne EJ , Lennox G , Quinn NP , Edwardson JA , Ince PG , Bergeron C , Burns A , Miller BL , Lovestone S , Collerton D , Jansen EN , Ballard C , de Vos RA , Wilcock GK , Jellinger KA , Perry RH ((1996) ) Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 47: , 1113–1124. |
[19] | Román GC , Tatemichi TK , Erkinjuntti T , Cummings JL , Masdeu JC , Garcia JH , Amaducci L , Orgogozo JM , Burn A , Hofman A ((1993) ) Vascular dementia: diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology 43: , 250–260. |
[20] | Neary D , Snowden JS , Gustafson L , Passant U , Stuss D , Black S , Freedman M , Kertesz A , Robert PH , Albert M , Boone K , Miller BL , Cummings J , Benson DF ((1998) ) Frontotemporal lobar degeneration: A consensus on clinical diagnostic criteria. Neurology 51: , 1546–1554. |
[21] | Litvan I , Agid Y , Calne D , Campbell G , Dubois B , Duvoisin RC , Goetz CG , Golbe LI , Grafman J , Growdon JH , Hallett M , Jankovic J , Quinn NP , Tolosa E , Zee DS ((1996) ) Clinical research criteria for the diagnosis of progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome): report of the NINDS-SPSP international workshop. Neurology 47: , 1–9. |
[22] | Litvan I , Bhatia KP , Burn DJ , Goetz CG , Lang AE , McKeith I , Quinn N , Sethi KD , Shults C , Wenning GK ((2003) ) Movement Disorders Society Scientific Issues Committee report: SIC Task Force appraisal of clinical diagnostic criteria for Parkinsonian disorders. Mov Disord 18: , 467–486. |
[23] | Mesulam MM ((2001) ) Primary progressive aphasia. Ann Neurol 49: , 425–432. |
[24] | Irie F , Fitzpatrick AL , Lopez OL , Kuller LH , Pelia R , Newman AB , Launer LJ ((2008) ) Enhanced risk for Alzheimer disease in persons with type 2 diabetes and APOE epsilon4: the Cardiovascular Health Study Cognition Study. Arch Neurol 65: , 89–93. |
[25] | Elmståhl S , Widerström E ((2014) ) Orthostatic intolerance predicts mild cognitive impairment: incidence of mild cognitive impairment and dementia from the Swedish general population cohort Good Aging in Skåne. Clin Interv Aging 9: , 1993–2002. |
[26] | Katz MJ , Lipton RB , Hall CB , Zimmerman ME , Sanders AE , Verghese J , Dickson DW , Derby CA ((2012) ) Age-specific and sex-specific prevalence and incidence of mild cognitive impairment, dementia, and Alzheimer dementia in blacks and whites: a report from the Einstein Aging Study. Alzheimer Dis Assoc Disord 26: , 335–343. |
[27] | Kim YH , Kim NH , Jung MH , Kim HJ ((2017) ) Sex differences in metabolic risk indicator of dementia in an elderly urban Korean population: A community-based cross-sectional study. Geriatr Gerontol Int 17: , 2136–2142. |
[28] | Zhu YY , Chen Y , Crimmins EM , Zissimopoulos JM ((2020) ) Sex, race, and age differences in prevalence of dementia in Medicare claims and survey data. J Gerontol B Psychol Sci Soc Sci, doi: 10.1093/geronb/gbaa083. |
[29] | Lin RT , Lai CL , Tai CT , Liu CK , Yen YY , Howng SL ((1998) ) Prevalence and subtypes of dementia in southern Taiwan: impact of age, sex, education, and urbanization. J Neurol Sci 160: , 67–75. |
[30] | Li W , van Tol MJ , Li M , Miao W , Jiao Y , Heinze HJ , Bogerts B , He H , Walter M ((2014) ) Regional specificity of sex effects on subcortical volumes across the lifespan in healthy aging. Hum Brain Mapp 35: , 238–247. |


