
Incorporating a Usual Care Comparator into a Study of Meditation and Music Listening for Older Adults with Subjective Cognitive Decline: A Randomized Feasibility Trial
Abstract
Background:
Recent studies suggest meditation and music listening (ML) may improve cognitive and psychosocial outcomes in adults with subjective cognitive decline (SCD). However, lack of a usual care group has limited conclusions.
Objective:
To assess the: 1) feasibility of incorporating an enhanced usual care (EUC) comparator in a trial of Kirtan Kriya meditation (KK) and ML for adults experiencing SCD; and 2) preliminary effects of active treatment (KK/ML) versus an EUC program.
Methods:
Forty participants with SCD were randomized 1:1:2 to a 12-week KK, ML, or EUC program. KK and ML participants were asked to practice 12 minutes/day; EUC participants were given a comprehensive educational packet regarding healthy aging and strategies for improving/maintaining brain health and asked to record any activities or strategies used. Feasibility was assessed using measures of retention, adherence, treatment expectancies, and participant satisfaction, as well as information from exit questionnaires and daily practice/activity logs. Cognitive functioning, stress, mood, sleep-quality, and health-related quality of life (QOL) were measured pre- and post-intervention using well-validated instruments.
Results:
Thirty-two participants (80%) completed the 3-month study, with retention highest in the EUC group (p < 0.05). Active treatment participants averaged 6.0±0.4 practice sessions/week, and EUC participants, 7.5±0.6 brain health activities/week. Treatment expectancies were similar across groups. EUC participants indicated high satisfaction with the program and study. Despite limited study power, the active treatment group showed significantly greater gains in subjective memory functioning (ps≤0.025) and nonsignificant improvements in cognitive performance (TMT-B), perceived stress, QOL, and mood (ps≤0.08) compared to the EUC group.
Conclusion:
Findings of this pilot feasibility trial suggest incorporation of an EUC program is feasible, and that participation in a simple 12-week relaxation program may be helpful for adults with SCD versus engagement in an EUC program.
INTRODUCTION
Despite decades of research, there is still no cure for Alzheimer’s disease (AD), and effective therapies for preventing or slowing cognitive decline in at-risk populations, including those with subjective cognitive decline (SCD), remain elusive. Characterized by neuropathological changes linked to AD, SCD may lead to accelerated cognitive decline, mild cognitive impairment (MCI), and incident AD, and may represent a critical window for therapeutic intervention [1–3]. Chronic stress, mood disturbances, and sleep deficits are also elevated in those with SCD, and are, in turn, significant, independent predictors of accelerated cognitive decline, neurodegenerative changes, and AD [1, 2]. Therapies that target cognitive function as well as sleep impairment and psychological distress may thus hold particular promise for slowing and possibly preventing cognitive decline in those with SCD.
There is growing evidence that both meditation and simple music listening may be beneficial for strengthening memory and cognitive function, reducing stress, anxiety, and depression, and enhancing well-being and quality of life (QOL) in those at risk for cognitive decline and AD [2, 4–9]. However, trials investigating the potential utility of these practices for improving cognitive performance and related psychosocial outcomes in those with preclinical memory loss are few, and apart from our recently completed study, randomized controlled trials (RCTs) remain sparse. In our previous trial of 60 elders with SCD, those randomized to a 12-week beginner meditation (Kirtan Kriya) or simple music listening (ML) program demonstrated significant improvement in multiple domains of memory and cognitive function, as well as in mood and sleep quality [1, 2], with gains in perceived stress, mood, psychological well-being, and QOL particularly pronounced in the KK group. Observed gains were sustained or strengthened at 6 months, with both groups showing significant improvements in most outcomes and effect sizes ranging from moderate to large. Findings also indicated that both programs were well-accepted and feasible for adults with early memory loss [10].
However, while these studies suggest these simple practices may have promise for improving cognitive and psychosocial outcomes in older adults with SCD [1, 2, 10, 11], the lack of a usual care group in our prior studies is a major limitation, precluding the assessment of potential practice effects and time trends, as well as the feasibility of implementing an RCT in adults with SCD that includes a usual care arm. To gather critical preliminary data on these issues in order to inform the planning of a larger RCT, we conducted a pilot 3-month feasibility RCT that incorporated an enhanced usual care arm. The primary objective of this pilot feasibility trial was to evaluate the feasibility and acceptability of incorporating a 12-week enhanced usual care (EUC) arm in a trial of meditation and music listening for SCD. Our secondary aim was to assess, in older adults with SCD, the preliminary effects of a simple 12-week KK and ML program as implemented in our prior trials vs. a newly developed 12-week EUC program. Methods and participant selection procedures mirrored those of our previous trial [10] in order to facilitate comparisons.
METHODS
Study participants
Study participants were independently living adults with SCD, defined as meeting 7 SCD criteria consistent with those outlined in recent expert reviews [12–15] and incorporating several key SCD-plus criteria, features thought to aid in the capture of those with perceived memory loss who are at risk for poor cognitive outcomes [14, 16]. These 7 criteria, along with other inclusion and exclusion criteria, are given in Table 1. Criteria for SCD included expressed concern or worry about memory problems, shown in prospective studies to substantially strengthen the association of SCD to incident MCI and AD [17–23], and to be associated with elevated beta-amyloid deposition [24, 25]. Additional study inclusion criteria included age at least 50 years, English-speaking, and willing and able to complete paper-and-pencil questionnaires and comply with the protocol. The trial was approved by the West Virginia University Institutional Review Board (IRB #1708731747).
Table 1
Major Eligibility Criteria
| Major Inclusion Criteria | Major Exclusion Criteria |
| Adults at least 50 years old with subjective cognitive decline (SCD), defined as meeting the following criteria: | Practiced meditation or other relaxation technique within the past year |
| 1) Presence of subjective cognitive deficits for at least 6 months; | Diagnosis of dementia or mild cognitive impairment |
| 2) Onset of SCD within the past 5 years | Recently (within the last 6 weeks) changed dosage of psychotropic medication (e.g., tricyclics, serotonin reuptake inhibitors, monoamine oxidase inhibitors, anti-panic or anti-anxiety agents) |
| 3) Frequency of memory problems at least once/week; | History of psychotic or schizophrenic episodes, major neurologic diagnosis (Parkinson’s, stroke, brain injury, epilepsy) or other condition that might impair cognition or confound assessments (e.g., cardiovascular event within the past 6 months (myocardial infarction, unstable angina, hospitalization for congestive heart failure, bypass surgery or angioplasty (coronary or carotid), transient ischemic attack) |
| 4) Able to give an example in which memory/cognitive problems occur in everyday life; | History of chemotherapy treatment within the past 10 years |
| 5) Belief that one’s cognitive capacities have declined in comparison with 5 or 10 years previously/adults of same age | |
| 6) Absence of overt cognitive deficits | |
| 7) Expressed concerns/worries regarding memory problems | |
| English speaking | Recent (within the last 3 months) serious physical trauma or diagnosis of serious chronic health condition requiring medical treatment and monitoring (e.g., uncontrolled hypertension, serious endocrine or pulmonary disorder, renal disease, active cancer treatment) |
| Willing and able to complete the intervention and all assessments | |
| For those concerned about their ability to fully understand consent or complete questionnaires, study buddy willing to attend baseline visit and other assessments if needed | |
| Willing to avoid new treatments other than the assigned intervention | Participant in another intervention study within the past 30 days |
Recruitment, screening, and enrollment
Participants were recruited from the community via flyers and brochures posted in community bulletin boards, medical clinics, office buildings, churches, senior centers, and other locations; advertisements in listservs, intranet, and other media venues; and presentations at local senior centers. Following a telephone pre-screen (N = 74), 44 potential participants were scheduled for an initial visit, of whom 40 completed the consent process and were enrolled in the study.
Randomization and treatment allocation
Eligible participants were randomized to a 12-week KK meditation program, a 12-week ML pro-gram or an enhanced usual care (EUC) group in a 1:1:2 ratio using a randomly varying block randomization method to ensure equal distribution between groups [26]. The study statistician, who had no contact with participants, prepared the randomization schedule and assignment packets, enclosing each treatment assignment and information in sequentially numbered, sealed opaque envelope. Following baseline assessment (see below), the consenting team member, who had no advance knowledge of the allocation schedule, gave the next sequentially numbered, sealed envelope to the participant.
Interventions
Immediately following the baseline assessment, participants opened their numbered envelopes to reveal their treatment assignment, and met with the trainer for 30–45 min of in-person program instruction. All training was delivered by a health educator familiar with all study programs, experienced in teaching a range of mind-body skills, and specifically trained in KK instruction. The trainer also followed up with each participant by phone within the first week of the intervention, and at least monthly thereafter to address any concerns and provide additional instruction or clarification as needed. Upon study completion, each participant was provided modest compensation and offered instruction materials for the groups to which s/he was not assigned.
Active interventions (KK and ML)
As in our previous RCT and detailed in our recently published papers [1, 2, 10, 11], participants assigned to KK or ML received in-person instruction in either the KK or the ML program, a program CD and an illustrated instructional brochure, along with a portable CD player for home use. The onsite trainer reviewed the instructions for the assigned program, introduced the various tracks on the CD, and familiarized participants in the operation of the CD player and the practice log sheet; each participant then used the CD to perform their first meditation/ML session and recorded it on their log sheet. The trainer provided any guidance required for the participant to become proficient. Participants were instructed to engage in their assigned practice while seated comfortably with eyes closed, for 12 min daily for 12 weeks (84 practice sessions total) and to record every practice session daily on the home practice log, along with any comments.
Kirtan Kriya meditation program. KK is a beginner meditation practice that has been shown to engage several areas of the brain, but is simple to learn and practice [27]. Specifically, KK includes a repeated Kirtan or song (singing repetition of the ‘Sa-Ta-Na-Ma’ mantra), a mudra or physical/motor component (touching each fingertip to the thumb in sequence with the chant), and a visualization component (imagining a beam of light or energy moving through the top of the head and out between the eyebrows in an ‘L’). The KK intervention, including instructional materials, was based on the one successfully implemented in our previous trial [10]. The program CD included an introduction to the KK practice along with detailed instructions, and five meditation tracks from which participants could choose (guided meditation with male voice, guided by female voice, and timing cues only (the latter two options available with and without background ocean sounds). Once seated comfortably, eyes closed, participants were instructed to take a moment to still themselves before beginning the 12 min practice. Following completion of the 12 min practice, participants were instructed to continue sitting quietly for a few moments (or more) before slowly opening their eyes.
Music listening program. As in our prior study [10], participants randomized to the ML group were instructed to sit comfortably in a quiet place with eyes closed, take a minute to settle, then listen to a 12 min selection on the music CD provided; after completing each session, participants were instructed to take another moment or more if needed to quietly come out of the practice, then record each practice session on a home practice log. The music CD included a selection of 6 relaxing 12 min instrumental classical music compositions by 6 different composers (Pachelbel, Bach, Mozart, Vivaldi, Debussy, and Beethoven). Participants were asked to sample each composer once but were otherwise free to choose which musical selection(s) to listen to for their daily practice.
Enhanced usual care
Participants assigned to EUC received a comprehensive, illustrated 60-page educational booklet regarding healthy aging and dementia, including materials from the Alzheimer’s Association, Administration for Community Living, National Institute on Aging (NIA)/National Institutes of Health (NIH), and Centers for Disease Control (CDC). Topics included general information on changes associated with aging, as well as on memory loss and dementia; risk factors for Alzheimer’s disease and related dementias (ADRD), highlighting modifiable factors such as mental and physical health conditions, poor sleep, and specific lifestyle factors; strategies for healthy aging, and specifically for improving and maintaining brain health; importance of medication management; and resources for additional information, support, and volunteer opportunities. The instructor reviewed the educational packet with each participant and explained the use of the treatment log. EUC participants were encouraged to read the materials and asked to complete a daily log detailing any strategies employed, along with any comments. While participants were not asked or encouraged to change their behavior in any way, and the instructor clarified that participation in activities was not a requirement of the program, participants were not discouraged from engaging in activities if they so chose.
Data collection and measures
Data were collected on feasibility and acceptability of the study and interventions and on treatment expectations (see below). Participants completed two, 1-2 h in person assessment visits, at baseline after providing written informed consent, and again at 3 months. All participant assessments and entry of outcome data were conducted by trained research staff blinded to participant treatment assignment. Baseline data included information on demographics, lifestyle characteristics (smoking, alcohol and caffeine consumption, physical activity), medical history, current medication and supplement use, body mass index (BMI, calculated as weight in kg/height in m2), and duration of perceived memory problems. At the 3-month follow-up visit, participants were asked to record any changes in medication and/or supplement use and in exercise routines or other lifestyle factors using a form specifically designed for this purpose, as well as to complete a study evaluation questionnaire (see Measures of Feasibility/Acceptability). Outcome assessments, detailed below, were performed at baseline and 3 months. The data collection schedule is illustrated in Supplementary Table 1.
Measures of feasibility/acceptability and treatment expectancy
To evaluate expectation of benefit, participants completed the 6-item Credibility/Expectancy Questionnaire (CEQ) [30] following their first intervention training session. Retention and adherence were monitored via phone calls throughout the study. All participants completed daily logs recording their home practice (active treatment groups) and engagement in other brain health activities (EUC group) (see Interventions, above); logs were collected at the follow-up assessment visit. Adherence measures included completion of practice/treatment logs and, for active treatment groups, completion of homework practice (total sessions and mean sessions/week); data were also gathered on optional engagement in brain health/memory enhancement activities by EUC participants. Retention was defined as completion of the follow up assessment. To assess satisfaction and related endpoints, all participants were asked to complete a study evaluation questionnaire based on that used in our previous trials [1, 2, 10, 31] and including both structured and open-ended questions regarding participant perceptions of and experiences with the study and their respective programs; the latter included perceived benefits and challenges of their respective interventions, reasons for withdrawal from the study, barriers to practice, assessment burden, likelihood of continuing their practice, and other study-related concerns. In addition, participants were asked to report any adverse events to the study personnel and were queried regarding potential concerns during the regular telephone check-ins and at the follow-up assessment.
Outcome assessments
At baseline and 3 months, each participant completed a short battery of tests to assess cognitive function, psychosocial status, and health-related of life (QOL). Specific instruments are described below.
Cognition. We evaluated memory and cognitive function using three well-established, validated instruments, including measures of subjective memory function (Memory Functioning Questionnaire (MFQ) [28]), executive function (Trail Making Test Parts A and B (TMT) [29]), and psychomotor speed, attention, and working memory (the 90 s Wechsler Digit-Symbol Substitution Test (DSST) [30]). The MFQ is a 64-item self-report questionnaire scored using a 7-point Likert scale (higher scores indicate better perceived memory functioning) and including four subscales: General Frequency of Forgetting, Seriousness of Forgetting, Retrospective Functioning, and Mnemonics Usage. MFQ scores have been inversely related to brain amyloid burden in cognitively normal older adults [35–37], and shown to differentiate non-cognitively impaired adults from those with SCD [31], suggesting that the MFQ may offer a useful marker of preclinical cognitive decline. While both parts of the TMT, considered a sensitive measure of general cognitive functioning, are designed to assess attention and information processing speed, the TMT-B also measures additional cognitive domains, including cognitive flexibility and visual scanning [32–34], and has been linked to verbal-numeric reasoning [32]. Scores reflect the number of seconds required to complete each part, with lower scores indicating better performance. Finally, the 90 s DSST is a timed test in which participants are asked to translate numbers into symbols using a key provided; higher scores indicate better performance [30].
Psychosocial outcomes and QOL were measured using widely used self-report instruments and included: perceived stress (10 item Perceived Stress Scale (PSS) [35, 36]), sleep quality (9-item Pittsburgh Sleep Quality Index (PSQI) [37]), mood (65-item Profile of Mood States (POMS) [38]), well-being (the 18-item Psychological Well-Being Scale (PWBS) [39]), and health-related quality of life (36-item MOS Short Form-36 (SF-36) [40]).
These instruments are well-established scales shown to be sensitive to short term mind body and other behavioral interventions, and validated in a wide range of populations, including older adults with memory loss [2, 38, 41–58].
Data analysis
All quantitative data analyses were performed using IBM SPSS for Windows, Version 26. Differences in baseline characteristics by intervention group assignment and attrition status were evaluated using chi square (for categorical variables), student independent samples t tests (for continuous variables with a normal distribution), or Mann-Whitney U tests (for ordinal or continuous variables with evidence of skewing). Potential differences between treatment groups in treatment expectancies, retention, and adherence were assessed using chi-square (attrition) and one-way ANOVA (adherence, treatment expectancies). In preliminary analyses, within and between group changes over time at 3 months were assessed using Repeated Measures ANOVA; age and sex, factors thought to be prognostic (e.g., [63]), were included as covariates. The potential influence of other factors that appeared to differ between groups at baseline was also considered in ancillary analyses. Variables with a non-normal distribution were log-transformed for analysis, using the addition of a constant in the case of zero or negative values. In our intention-to-treat (ITT) analyses, we used multiple imputation to replace any missing data [59, 60]. Effect sizes were calculated using Cohen’s d. Alpha was set at 0.05 given the exploratory nature of this study. As KK and ML groups demonstrated similar changes overall in cognitive and psychosocial measures (Supplementary Table 2) and sample sizes were small, these groups were pooled for analysis of outcomes for purposes of this study.
As indicated above, acceptability and feasibility of the study and programs were evaluated by assessing: recruitment and enrollment; treatment expec-tancies; retention; adherence, defined as completion of practice sessions (active treatment groups) and daily logs during the 12-week active intervention period; and participant responses on study evaluation questionnaires. Optional engagement in brain health activities (EUC group) was also quantified for comparison with active treatment groups. Potential differences between treatment groups were analyzed using chi-square (attrition), one-way ANOVA (adherence, treatment expectancies), and Mann Whitney U tests (exit questionnaire items using ordinal scales). To assess the potential relationship of treatment expectancy scores to change over time in memory and cognitive functioning, mood, stress, well-being and QOL, age- and sex-adjusted correlations were performed using Pearson product-moment correlation. Responses to open-ended questions on the exit questionnaires were transcribed, coded, and categorized into themes for descriptive analysis using word/topic repetition [61].
RESULTS
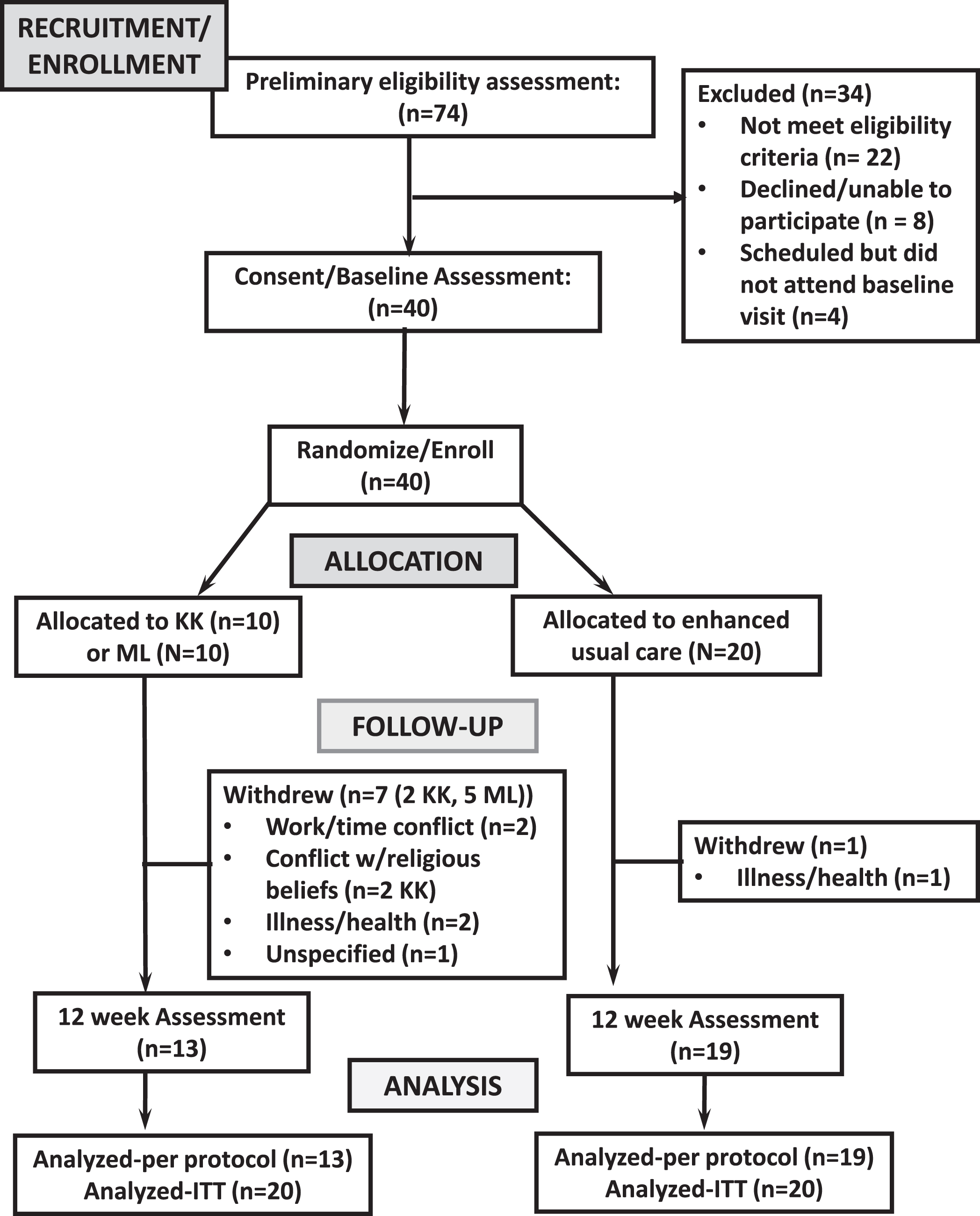
Seventy-four individuals contacted research personnel for information regarding the study over the course of 15 months; of these, 22 did not meet eligibility criteria, 8 declined participation, and 4 were scheduled for initial visits but were unable to attend. A total of 40 eligible adults with SCD were enrolled in the study (Fig. 1).
Fig. 1
Study flow diagram.
Baseline characteristics are given in Table 2. The majority of participants were non-Hispanic white (87.5%) and female (72.5%), with an average age of 64.2±1.4 (range 50–84) years. Most were employed at least part-time (55%), married or living with a partner (57.5%), and had received post-high school education (82.5%). Participants reported experiencing memory problems for a median of 3 years prior to enrollment. Eighty percent of participants reported at least one metabolic/vascular risk factors for AD, with 53%indicating two or more chronic conditions linked to ADRD risk. Common among these were dyslipidemia (58%), hypertension (45%), and diabetes (22.5%). In addition, 23%of participants indicated a history of diagnosed depression or anxiety disorder, and 30%reported no engagement in physical activity. Relative to EUC participants, those assigned to the active treatment arms were significantly older, with a greater proportion of women (ps≤0.05), but did not differ in other baseline characteristics (Table 2).
Table 2
Participant baseline characteristics: Pilot feasiblity RCT of a 12-week active treatment (Kirtan Kriya meditation or music listening) program versus an enhanced usual care program (EUC) in older adults with subjective cognitive decline
| Overall (N = 40) | Active Treatment (N = 20) | EUC (N = 20) | p | ||||
| N | % | N | % | N | % | ||
| Demographic characteristics | |||||||
| Age (range 50–84 years) | |||||||
| Mean±SE | 64.15±1.40 | 66.85±2.14 | 61.45±1.38 | 0.05 | |||
| Female Gender | 29 | 72.5% | 11 | 55.0% | 18 | 90.0% | 0.03 |
| Race/Ethnicity: Non-Hispanic White | 35 | 87.5% | 2 | 10.0% | 3 | 15.0% | 0.59 |
| Education | 0.75 | ||||||
| 12 years (High school) or less | 7 | 17.5% | 4 | 20.0% | 3 | 15.0% | |
| 13–15 years (some college) | 11 | 27.5% | 6 | 30.0% | 5 | 25.0% | |
| 16 + years (college) | 22 | 55.0% | 10 | 50.0% | 12 | 60.0% | |
| Mean±SE | 15.30 (0.36) | 15.45 (0.56) | 15.15 (0.47) | 0.68 | |||
| Employment status | 1.00 | ||||||
| Employed full or part time | 22 | 55.0% | 11 | 55.0% | 11 | 55.0% | |
| Retired/Homemaker/Other | 18 | 45.0% | 9 | 45.0% | 9 | 45.0% | |
| Marital status | 0.75 | ||||||
| Married/co-habiting | 23 | 57.5% | 12 | 60.0% | 11 | 55.0% | |
| Divorced/widowed/separated/single | 17 | 42.5% | 8 | 40.0% | 9 | 45.0% | |
| Lifestyle and health-related factors | |||||||
| Smoking status: Ever smoked | 12 | 30.0% | 4 | 20.0% | 8 | 40.0% | 0.17 |
| Caffeinated beverage consumption | |||||||
| Mean oz consumed/day±SE | 23.32±3.57 | 26.53±5.86 | 20.272±4.20 | 0.39 | |||
| Physical activity | 1.00 | ||||||
| None | 12 | 30.0% | 6 | 30.0% | 6 | 30.0% | |
| Mean minutes/week 7±SE | 147.88±23.33 | 136.75±28.02 | 159.00±37.89 | 0.64 | |||
| Body mass index (BMI) | |||||||
| Obese (BMI≥30) | 10 | 25.0% | 4 | 20.0% | 6 | 30.0% | 0.47 |
| Mean±SE | 27.44±6.33 | 25.83±0.99 | 29.05±1.69 | 0.12 | |||
| History of diagnosed: | |||||||
| Diabetes | 9 | 22.5% | 6 | 30.0% | 3 | 15.0% | 0.26 |
| Hypertension | 18 | 45.0% | 11 | 55.0% | 7 | 25.0% | 0.21 |
| High cholesterol | 12 | 30.0% | 7 | 35.0% | 5 | 25.0% | 0.49 |
| Depression | 7 | 17.5% | 5 | 25.0% | 2 | 10.0% | 0.21 |
| Anxiety | 7 | 17.5% | 4 | 20.0% | 3 | 15.0% | 0.68 |
| Number of cardiometabolic AD risk factors* | |||||||
| Mean±SE | 1.78±0.25 | 2.05±0.40 | 1.50±0.31 | 0.16 | |||
| Total number of major health-related risk factors for AD**: Mean±SE | 2.25±0.31 | 2.50±0.46 | 1.75±0.37 | 0.21 | |||
| Number of medications (regular use)t - | 0.31 | ||||||
| None | 8 | 20.0% | 4 | 20.0% | 4 | 20.0% | |
| One-two | 22 | 55.0% | 10 | 50.0% | 12 | 60.0% | |
| Three or more | 10 | 25.0% | 6 | 30.0% | 4 | 20.0% | |
| Years Experiencing Memory Problems (mean±SE) | 3.19 (0.33) | 3.33 (0.66) | 3.09 (0.35) | 0.73 | |||
*Including diabetes, hypertension, high cholesterol, obesity (BMI≥30), cardiovascular disease. ** Also including history of depression or anxiety disorder, current smoking, and lack of physical activity.
Likewise, baseline measures of overall subjective memory function, cognitive performance, mood, stress, sleep, and well-being did not differ between the active treatment and EUC groups either in those completing the study (Table 3) or in the full sample (ps≥0.3).
Table 3
Mean participant baseline scores on memory and cognitive function tests*, and on sleep, stress, mood, well-being, and quality of life questionnaires, stratified by group (Active treatment (Kirtan Kriya meditation or music listening) versus enhanced usual care (EUC))**
| Total Mean (SE) | Active treatment Mean (SE) | EUC Mean (SE) | p | |
| Cognitive Function | ||||
| Memory Functioning Questionnaire | ||||
| Total | 253.61 (8.38) | 244.32 (12.40) | 259.93 (11.29) | 0.37 |
| Frequency of Forgetfulness | 148.25 (4.88) | 144.69 (7.52) | 150.62 (6.69) | 0.56 |
| Seriousness of Forgetting | 72.28 (3.32) | 69.71 (4.99) | 73.99 (4.49) | 0.56 |
| Retrospective Memory Functioning | 12.93 (0.61) | 12.33 (0.81) | 13.33 (0.87) | 0.53 |
| Mnemonic Use | 20.17 (1.26) | 17.58 (1.87) | 21.89 (0.81) | 0.09 |
| Digit Symbol Substitution Test | 48.24 (1.90) | 47.75 (2.61) | 48.59 (2.74) | 0.95 |
| Trail-making Test (TMT), in seconds | ||||
| TMT-A | 27.87 (1.74) | 27.75 (3.15) | 27.94 (2.09) | 0.96 |
| TMT-B | 57.20 (4.01) | 57.58 (6.78) | 56.94±5.08 | 0.94 |
| Perceived Stress and Sleep Quality | ||||
| Perceived Stress Scale | 13.03 (1.13) | 12.67 (1.45) | 13.28 (1.57) | 0.80 |
| Pittsburgh Sleep Quality Index, Total | 8.07 (0.49) | 7.92 (2.61) | 8.17 (0.65) | 0.80 |
| Mood and Well-being | ||||
| Profile of Mood States (Total) | 22.77 (5.41) | 22.43 (6.28) | 23.02 (8.26) | 0.96 |
| Psychological Well-being Scale | 81.39 (1.73) | 83.58 (2.33) | 79.06(2.33) | 0.27 |
| Health related Quality of Life (SF-36) | ||||
| Mental Health Composite Score | 71.74 (3.11) | 74.70(4.92) | 70.41 (4.15) | 0.36 |
| Physical Health Composite Score | 69.20 (4.46) | 74.58 (5.12) | 66.80 (6.34) | 0.29 |
*Higher scores indicate poorer outcomes for the TMT, Perceived Stress Scale, Profile of Mood States, and Pittsburgh Sleep Quality Index. Lower scores indicate poorer outcomes for the Memory Functioning Questionnaire, Digit Symbol Substitution Test, Psychological Well-being Scale, and SF-36. **In participants completing study (N = 32).
Retention, adherence/engagement, and treatment expectations
Each participant received the intervention as allocated. Eighty percent of participants (N = 32) completed the 12-week intervention and follow-up assessment, with retention significantly higher in the EUC group than the active treatment groups (19/20 versus 13/20, p = 0.04). Reasons for dropout included: family emergency/personal illness (n = 3), conflict with religious beliefs (N = 2), other conflicts (withdrew week 1, N = 2), and unknown/lost to follow-up (n = 1). Those who dropped out were similar to completers in demographics, lifestyle factors, BMI, and health history (ps≥0.3). Of those remaining in the study, 27 (84.4%) submitted completed daily logs, including 12 active treatment participants and 15 EUC participants; completion rates did not differ significantly between groups (92%active treatment versus 79%EUC, p = 0.3). Engagement was high in the both the active intervention and EUC groups, with participants assigned to the active treatment programs completing an average of 6.0±0.4 practice sessions/week, and EUC participants, a mean of 7.5 (0.6) brain health activities/week. Of the 15 EUC participants submitting daily logs, all reported regular engagement in brain health activities recommended in their readings, often in combination. Among the most commonly reported activities were physical exercise (86.7%), including walking (40%), dancing (26.7%), and other forms of physical activity (73.3%); brain-training activities (80%), including puzzles, card games (60%), and memory exercises (33.3%); adoption of a new reading program (60%); and participating in social and volunteer activities (73.3%). Some participants also reported joining singing groups (N = 4) and learning new yoga or other meditative practices (N = 3), as well as making healthy dietary or other lifestyle changes (46.7%).
As detailed in Table 4, there were no significant differences between the two groups in any domain of treatment expectancy (all ps≥0.45). Moreover, treatment expectancy scores were not significantly correlated with change over time in measures of cognitive functioning, stress, mood, sleep, or QOL-physical health (ps≥0.1), although 2 of 6 items were related to changes in QOL-mental health (ps < 0.05). No adverse events were observed or reported.
Table 4
Treatment expectancies following first training session: Pilot feasibility RCT of a 12-week active treatment (Kirtan Kriya meditation or music listening) program versus Enhanced usual care in 40 adults with subjective cognitive decline
| Active treatment (N = 20) Mean (SE) | Enhanced Usual Care (N = 20) Mean (SE) | p | |
| Treatment Expectancies (Credibility/Expectancy Questionnaire) | |||
| Thoughts about relaxation practices* | |||
| 1 At this point, how logical does the course offered to you seem? | 6.80 (0.47) | 7.25 (0.34) | 0.45 |
| 2 At this point how successfully do you think this course will be in raising the quality of your functioning? | 5.85 (0.47) | 5.73 (0.51) | 0.86 |
| 3 How confident would you be in recommending this course to a friend who experiences similar problems? | 6.95 (0.56) | 6.95 (0.39) | 1.00 |
| 4 By the end of the course, how much improvement in your functioning do you think will occur (in percent)? | 48.75 (5.69) | 43.50 (6.78) | 0.56 |
| Feelings about relaxation practices* | |||
| 1 At this point, how much do you really feel that the course will help you to improve your functioning? | 5.58 (0.61) | 5.40 (0.55) | 0.83 |
| 2 By the end of the course, how much improvement in your functioning do you feel will occur? | 50.25 (7.77) | 42.50 (7.77) | 0.49 |
Satisfaction/acceptability
As indicated in Table 5, participant responses suggested high satisfaction with the study and study programs overall. Of those submitting study evaluation questionnaires (N = 12 active treatment, 18 EUC), most participants (93%) reported multiple positive comments in response to open-ended questions regarding their respective programs. These included appreciating the meditative experience (N = 7) and the opportunity to engage in new practices/activities (N = 13), finding the practice relaxing and peaceful (N = 12), and citing specific benefits (N = 10) such as improved memory, energy, and sleep. Several also indicated appreciation for the staff and the opportunity to participate in the study (N = 10). Notably, some EUC participants reported enjoying the flexible, unstructured nature of the practice (N = 3), gaining new awareness regarding healthy aging/brain health (N = 5), and discovering new strategies to improve brain health (N = 7).
Table 5
Participant perceptions regarding the study and their assigned interventions (Study evaluation questionnaire): Pilot feasibility RCT of a 12-week active treatment (Kirtan Kriya meditation or music listening) versus an enhanced usual care (EUC) program in adults with subjective cognitive decline
| Total (N = 30) | Active treatment (N = 12) | Enhanced Usual Care (n = 18) | ||||
| N | % | N | % | N | % | |
| Participant Perceptions Regarding Intervention/Study | ||||||
| Positive perceptions | ||||||
| Enjoyed the meditative experience | 7 | 23.3% | 5 | 41.7% | 2 | 11.1% |
| Relaxing, tranquil, peaceful | 12 | 40.0% | 10 | 83.3% | 2 | 11.1% |
| Taking on new lifestyle/practices, finding relaxation and enjoyment in new activities | 13 | 43.3% | 4 | 33.3% | 9 | 50.0% |
| Experienced benefits | 10 | 33.3% | 6 | 50.0% | 4 | 22.2% |
| Increased focus, energy (all domains) | 8 | 26.7% | 5 | 41.7% | 3 | 16.7% |
| Improved memory | 6 | 20.0% | 4 | 33.3% | 2 | 11.1% |
| Improved sleep | 5 | 16.7% | 3 | 25.0% | 2 | 11.1% |
| Improved awareness re healthy aging/brain health, access to useful information | 5 | 16.7% | 0 | 0.0% | 5 | 27.8% |
| Finding, trying new strategies to improve brain health | 7 | 23.3% | 0 | 0.0% | 7 | 38.9% |
| Enjoyed unstructured/flexible nature of practice | 3 | 10.0% | 0 | 0.0% | 3 | 16.7% |
| Able to do at home | 4 | 13.3% | 2 | 16.7% | 2 | 11.1% |
| Liked being in study; friendly informative staff | 10 | 33.3% | 4 | 33.3% | 6 | 33.3% |
| Concerns/Perceived Barriers to Practice | ||||||
| Conflict with religious beliefs/practice (KK) | 3 | 10.0% | 3 | 25.0% | 0 | 0.0% |
| Illness/Injury | 3 | 10.0% | 3 | 25.0% | 0 | 0.0% |
| Travel (expected and unexpected) | 6 | 20.0% | 4 | 33.3% | 2 | 11.1% |
| Finding Time/too busy/too tired | 9 | 30.0% | 6 | 50.0% | 3 | 16.7% |
| Delivery issues (equipment; mode; certain tracks) | 3 | 10.0% | 3 | 25.0% | 0 | 0.0% |
| Worry about mastery, concentration/focus | 3 | 10.0% | 3 | 25.0% | 0 | 0.0% |
| Desire additional staff check-in, instructions | 2 | 6.7% | 1 | 8.3% | 1 | 5.6% |
| Desire more structure/specific expectations | 5 | 16.7% | 0 | 0.0% | 5 | 27.8% |
| Worry not doing enough | 3 | 10.0% | 0 | 0.0% | 3 | 16.7% |
| Paperwork/logs | 2 | 6.7% | 0 | 0.0% | 2 | 11.1% |
| Uncertainty re benefits | 2 | 6.7% | 0 | 0.0% | 2 | 11.1% |
With respect to assessment burden and interest in continuing the intervention, 85%of those responding indicated the assessment duration was fine (versus too long or a bit too long); 87.5%(82%active treatment, 92%EUC) indicated they were likely or very likely to continue their respective programs. Responses were similar across groups (ps > 0.6). In response to queries regarding barriers to practice/least favored aspects of the study/program, the most commonly cited were finding the time and/or energy to engage (N = 9) and travel or illness/injury (N = 6) (Table 5). A few active treatment participants also cited issues with intervention delivery (N = 3) and concern about practice mastery (N = 3). In addition, three KK participants reported conflict with religious beliefs as a key barrier, with all citing concerns with the mantra, indicating that they initially heard the mantra as ‘Satan’; these concerns were echoed by the two participants who withdrew for religious reasons. Three participants in the ML program stated that, although they liked most selections offered, inclusion of a broader range of instrumental music options would be appreciated. Several EUC participants mentioned as issues a desire for more structure and specific instructions/expectations (N = 5) and concern that they were not doing enough (N = 3).
Change over time in cognitive function, psychological status, sleep, and QOL
As illustrated in Table 6, both the active treatment and EUC groups showed significant improvements over time in overall subjective memory functioning and mood (ps < 0.05). Participants assigned to active treatment also demonstrated marked and significant gains in multiple individual domains of memory function and mood (ps < 0.03), and marginally significant improvements in cognitive performance (DSST and TMT-B) and QOL (physical health component) (ps≤0.095), with effect sizes ranging from moderate (0.4-0.5) to large (0.8–1.1). Relative to the EUC group, those assigned to active treatment showed significantly greater gains in subjective memory function, both overall and in specific domains (Frequency and Seriousness of Forgetfulness) (ps < 0.025) and in certain domains of mood (Anger/Hostility and Fatigue) (ps < 0.05) as well as a tendency toward greater improvements in the TMT-B (p = 0.09), perceived stress (p < 0.08), overall mood (p = 0.06), and QOL-physical health (p = 0.065). While non-significant, relative improvements in the active treatment versus EUC group in virtually all other measures were in the expected direction (Table 6; also see Supplementary Table 2).
Table 6
Change over time in subjective memory and cognitive function, psychological status, sleep, and quality of life in older adults with subjective cognitive decline randomized to a 12-week active treatment (Kirtan Kriya meditation or music listening) program versus an enhanced usual care program (EUC)).
| Change from baseline to 3 months (Active treatment) | Change from baseline to 3 months (EUC) | ||||||
| Outcome Measures | Mean (SE) | p | ES | Mean (SE) | p | ES | pt |
| Perceived Memory Function | |||||||
| Memory Functioning Questionnaire | |||||||
| Total | 49.96 (14.90) | 0.007 | 1.0 | 20.11 (8.78) | 0.03 | 0.5 | 0.018 |
| Frequency of Forgetfulness | 21.09 (8.35) | 0.028 | 0.8 | 8.87 (3.88) | 0.035 | 0.5 | 0.025 |
| Seriousness of Forgetting | 22.23 (6.01) | 0.004 | 1.1 | 6.64 (4.38) | 0.15 | 0.4 | 0.01 |
| Retrospective Memory Functioning | 4.00 (1.46) | 0.019 | 0.8 | 2.05 (1.14) | 0.09 | 0.4 | 0.16 |
| Executive Function, Information Processing/Psychomotor Speed, Attention, Working Memory | |||||||
| Digit Symbol Substitution Test | 3.42 (2.16) | 0.095 | 0.4 | 2.27 (1.33) | 0.11 | 0.4 | 0.45 |
| Trail-making Test (TMT) | |||||||
| TMT-A | –3.08 (3.00) | 0.32 | 0.4 | –1.00 (1.55) | 0.53 | 0.15 | 0.14 |
| TMT-B | –9.92 (6.89) | 0.09 | 0.4 | 3.95 (6.02) | 0.52 | –0.15 | 0.08 |
| Stress, mood, well-being, and sleep quality | |||||||
| Perceived Stress Scale | –3.3 (1.62) | 0.11 | 0.6 | 0.05 (1.25) | 0.97 | 0.0 | 0.08 |
| Profile of Mood States | |||||||
| Total score | –21.51 (7.26) | 0.01 | 0.9 | –11.74 (5.52) | 0.05 | 0.4 | 0.06 |
| Psychological Well-being Scale | 3.83 (2.25) | 0.23 | 0.4 | –1.47 (1.53) | 0.35 | 0.2 | 0.15 |
| Pittsburgh Sleep Quality Index | |||||||
| Total score | –1.10 (0.94) | 0.27 | 0.4 | –0.14 (0.50) | 0.75 | 0.1 | 0.35 |
| Health related Quality of Life (SF-36) | |||||||
| Mental Health Component | 6.97 (4.57) | 0.15 | 0.5 | 2.10 (3.67) | 0.58 | 0.1 | 0.19 |
| Physical Health Component | 6.07 (3.34) | 0.09 | 0.6 | –0.71 (2.20) | 0.75 | 0.1 | 0.065 |
NOTE: Reductions in scores indicate improvement for the TMT, Perceived Stress Scale, Profile of Mood States, and Pittsburgh Sleep Quality Index; increases in scores indicate improvement for the Memory Functioning Questionnaire, Digit Symbol Substitution Test, Pscyhological Well-bieng Scale, and SF-36. t-Between group difference, 3 months (adjusted for age, sex). SE, standard error
ITT analyses using multiple imputation yielded similar results. Excluding from the analysis those who changed medications did not appreciably alter the findings, nor did adjustment for baseline depression. Moreover, although the distribution of some factors (including smoking status, BMI, diabetes, hypertension, diabetes, and depression) appeared to differ, albeit non-significantly, between groups, these factors were unrelated to baseline outcome scores or to change in outcomes.
DISCUSSION
Findings of this pilot feasibility trial support the feasibility and acceptability of incorporating a EUC arm in RCTs of meditation and ML for older adults with SCD and suggest these practices may be beneficial for improving certain outcomes in older adults with SCD. Retention in the EUC group was high, and engagement in recommended brain health activities was surprisingly robust given that participation in these activities was neither required nor encouraged. Treatment expectancies were similar to those of the active intervention groups, and responses on the study evaluation questionnaire suggested high satisfaction with the EUC program overall. Moreover, despite limited power and the very active engagement of the EUC group in this study, participants assigned to active treatment demonstrated significantly greater improvement in multiple domains of subjective memory function, and non-significant improvements in executive function, perceived stress, mood, and QOL (physical health component). Pre-post effect sizes for the active treatment group were primarily in the moderate to large range. These findings offer additional, albeit preliminary evidence that the gains observed in this and prior trials do not simply reflect time trends or practice effects. Observed improvements were not related to baseline treatment expectancies, suggesting that expectations of benefit did not appreciably influence outcomes in this study.
We demonstrated in our previous 6-month RCT of 60 elders with SCD that both KK and ML were acceptable and feasible, with participants assigned to both groups showing high retention, excellent adherence, and high satisfaction with both programs [10]. It remains unclear why retention in the KK and ML groups was lower in this smaller pilot study, despite the shorter duration (3 months versus 6 months). However, participant feedback suggests that 1) offering a variety of delivery options for both programs, including MP3 files, may enhance retention, facilitate practice, and increase satisfaction; 2) more frequent check-ins may be required for some participants; and 3) the KK program may require modification in order to be acceptable to participants with certain religious beliefs. While determinants of meditation practice in older adults remain incompletely understood [62], conflict with religious beliefs has been cited as a barrier to yoga and meditation practice in prior studies (e.g., [62–64], and is an issue that warrants consideration in designing and implementing trials of these mind-body therapies. In the current study, five participants assigned to the KK group specifically expressed concern regarding the Sa-Ta-Na-Ma mantra (versus no participants in our prior studies), a concern that led two participants to eventually withdraw from the study. All 5 recommended having more mantra options, a strategy which we employed successfully in prior studies of mantra meditation for osteoarthritis in older adults [65, 66] and which could be helpful in future studies.
In addition, some participants in the ML program indicated that, while they enjoyed the instrumental pieces offered, including a larger variety of classical music selections would be helpful. With respect to the EUC program, retention and engagement were surprisingly high, perhaps reflecting in part the strong motivation of those with SCD to identify strategies for improving their cognitive function. In future studies, the EUC program could also incorporate interactive internet tools for self-guided brain-health activities, as has been proposed in recent recommendations for SCD clinical management [67].
The significant gains in subjective memory function, along with the apparent improvements in mea-sures of cognitive function, psychosocial status, and HrQOL observed with active treatment in this pilot RCT are consistent overall with those reported in our prior studies of adults with early memory loss [1, 2, 46]. To date, published controlled trials regarding the effects of meditation or ML on cognitive function targeting older adults with SCD have been limited, and those in other populations with or at risk for cognitive impairment remain relatively few [5–7, 68–71]. Nonetheless, our findings are broadly consistent with those of: a recent RCT of meditation in Chinese elders with sleep impairment [72]; pilot controlled trials of KK meditation versus ML in depressed dementia caregivers [73], adults with memory loss [74], and breast cancer survivors [75]; RCTs of KK meditation and yoga in MCI patients [76] and of mindfulness-based stress reduction in adults with stress disorders and cognitive concerns [77]; an RCT of mindfulness for patients with AD[78], and an early pilot RCT of Transcendental meditation in both cognitively impaired and unimpaired elderly [79]. Likewise, our findings are in overall agreement with those of RCTs investigating the cognitive effects of mindful or passive music listening in stroke patients [80–82] and three RCTs of interventions incorporating music-listening in Finnish and Taiwanese dementia patients [83, 84] and Spanish nursing home residents with cognitive impairment [85].
In contrast, other controlled trials of mindfulness meditation in generally healthy elders [86–88], stressed older adults [89], elders with MCI [90–92], dementia caregivers [93] and nursing home residents [94], showed little or no improvement in cognitive measures, nor did trials of therapist-delivered music programs in Italian elders with memory loss [95] and psychiatric in-patients with cognitive impairment [96] or of passive music listening in Taiwanese AD patients [97]. Cognitive gains observed with simple KK and ML in this study are comparable to those reported with tai chi [98–100], conventional exercise [99, 101], cognitive training [102, 103], and multicomponent interventions [104–106] in older adults with and without cognitive impairment.
Similarly, published RCTs regarding the potential benefits of meditation or music listening for improving psychosocial outcomes in older adults at risk for dementia are few, and those in elders with preclinical memory loss remain sparse [5–7, 107]. To our knowledge, apart from our recent trial, only one published RCT has assessed the effects of either intervention on psychosocial outcomes in elders with SCD [77]. While results of trials in at risk elders have been mixed, some have yielded findings broadly consistent with the results of our current RCT. For example, in recent RCTs of mindfulness meditation-based interventions (MBI) in stressed older adults [89] and elders with a depressive or anxiety disorder accompanied by subjective cognitive concerns [77], those completing a 5- [89] to 12-week [77] MBI program showed significant improvement in measures of mood [77, 89] and QOL [89] relative to those assigned to a waitlist [89] or health education program [77]. In two pilot RCTs of depressed dementia caregivers [73] and elders with MCI [76], those assigned to an 8- [73] to 12-week [76] KK-based program demonstrated reductions in depressive symptoms [73, 76], as well as increases in resilience [76] and QOL [73] at follow-up. While controlled trials regarding the effect of ML on psychosocial outcomes in older adults at risk for dementia are few, RCTs of Turkish [8] and British [9] long term care residents and Finnish post-stroke patients [81] showed significant reductions in symptoms of depression [8, 9, 81], anxiety [9], and confusion [81] following a 3- [9] to 8-week [8, 81] ML program.
In contrast, other RCTs of meditation or ML in elders at risk for dementia have shown little or no effect on psychosocial outcomes. For example, RCTs of 8-week [108] to 9-month [91] MBIs in adults with MCI, and of a 6-month mindful ML program in post-stroke patients [80] did not find significant improvement in stress [108] depression [91] or anxiety [91, 108]. Similarly, prior RCTs of physical activity [109, 110], group psychoeducation [111], or cognitive interventions [106, 111] for older adults with SCD [106, 110, 111] or MCI [109] have indicated little or only modest improvements in psychosocial status.
In addition, our findings of modest or no improve-ment in the EUC group despite their active engagement in brain health activities are in agreement with a number of prior trials. For example, several trials of both meditation and other non-pharmacologic interventions, including RCTs in adults at risk for cognitive decline, noted little change in cognition in those randomized to a comparator group. For example, prior RCTs of tai chi [112], conventional exercise [113–115], and meditation-based programs [73, 86, 87] in older, community-dwelling adults [86, 87, 116], retirement home residents [115], depressed caregivers [73], and elders with or at risk for memory loss [112, 114] showed little or no change over time in the TMT among participants in the control group, with some noting worsening over time in this measure [87, 112, 114, 116] in accordance with our findings. Likewise, in general agreement with the results of our study, numerous RCTs of meditation, ML, and other non-pharmacological interventions in adults at risk for cognitive impairment have shown psychological status and quality of life to remain unchanged or deteriorate over time in those assigned to a usual care or other comparator conditions [105, 110, 117–123].
Strengths and limitations
Strengths of this investigation include the rigorous study design, feasibility assessment using multiple measures and a mixed methods approach, and evaluation of both subjective and objective cognitive performance as well as psychosocial status and QOL. Participants were recruited from the community, potentially strengthening the generalizability and applicability of our findings. Additional strengths include the excellent retention rates in the EUC group and overall high adherence and engagement in participants completing the study. While participants expressed high satisfaction with the EUC comparator program and actively engaged in brain health practices recommended in the materials provided, collection of data on treatment expectancy also allowed adjustment for potential residual placebo effects. Both the active treatment and EUC groups received similar duration trainings, completed daily logs, were contacted regularly by study staff, and showed comparable engagement in recommended practices, helping to reduce potential bias related to staff attention, differential home practice, or other factors. Notably, the EUC intervention implemented in this study is consistent with the recent clinical recommendations for SCD management stipulating that individuals with SCD receive information on strategies to support brain health [69].
To help capture those at risk for cognitive decline, we ascertained presence of SCD using a questionnaire that incorporated criteria based on prior expert reviews and longitudinal studies, including several of the proposed criteria for ‘SCD-plus’ [14, 16]; the latter included worries regarding one’s memory problems, a factor shown to strengthen the link of SCD to incident MCI and AD [17, 19–23] and, along with SCD onset within the last 5 years, to be associated with elevated brain amyloid-β [25]. In addition, mean participant MFQ scores at baseline were comparable to those of elders with MCI [124, 125], and considerably lower than average scores reported in samples of older, similar aged community-dwelling adults [28] and cognitively normal elders [125–128], including those averaging substantially older than our participants [126–128] and those with elevated brain amyloid [128].
This pilot trial has a number of important limitations as well. Designed primarily to assess the feasibility of incorporating an EUC into a trial of KK and ML for SCD, sample sizes were small, reducing our ability to detect between group differences in outcomes and precluding meaningful assessment of potential differential effects of the active treatment arms. As discussed above, attrition in the active treatment groups was relatively high; while some reasons for withdrawal were unavoidable (e.g., illness and family emergencies), others, notably including conflict with religious beliefs, warrant careful consideration in future trials. Our study population comprised relatively well-educated, motivated volunteers with SCD, potentially restricting generalizability to other populations with preclinical memory loss. While we assessed subjective memory and cognitive performance, we did not perform diagnostic evaluations of cognitive status in our participants; it is thus possible that our study sample included some individuals with undiagnosed MCI. Moreover, while we assessed multiple cognitive domains, including working memory, we did not specifically include a measure of episodic memory. Although the DSST has been shown to be a significant mediator and a strong predictor of age-related variance in episodic memory, accounting for over 98%of the variance in this factor [129], direct measurement of this domain is important and will be incorporated in our planned larger RCT.
In addition, we did not include participant assessment of instructor enthusiasm and confidence in the intervention, factors that could potentially influence outcomes. However, we did administer a well-established instrument for assessing early participant perceptions of treatment credibility and likely effectiveness, which have been shown to influence outcomes in a number of studies (e.g., [130–133]). Moreover, if perceived differences in instructor enthusiasm and confidence influenced participant perceptions of the interventions, we would expect treatment expectations to vary accordingly; in contrast, expectancies were similar across groups. While we measured a range of mood domains using the POMS, we did not include an instrument specifically designed to assess depression, a limitation that we plan to address in future studies. However, scores on the POMS depression scale have been shown to correlate strongly with other depression scales, including the Beck’s Depression Inventory [134] and Geriatric Depression Scale, and to offer a potentially useful alternative to this instrument for detecting depression and measuring depressive symptomology in certain populations [135, 136], including older, community-dwelling adults [136].
While possible practice effects may have accoun-ted for some of the improvements witnessed, the incorporation of an EUC comparator coupled with the relatively long interval between assessments renders this possibility less likely. In addition, blinded treatment administration was not possible in this study, potentially biasing expectations of participants and raising the possibility of placebo effects. However, given our inclusion of an EUC group, the active engagement of EUC participants, the similarity of treatment expectancy scores in the active and EUC groups, and, importantly, the lack of association between these scores and overall change in the outcomes measured, expectations of treatment and associated placebo effects are unlikely to explain our findings.
We did not exclude participants on narcotic analgesics. However, in the current study, only two participants reported use of narcotic analgesics (one EUC, one ML), and neither exclusion of these participants from the analysis nor adjustment for analgesic use appreciably altered findings. Moreover, evidence regarding the effects of narcotic analgesics on cognition has been inconsistent to date. For example, in a recent systematic review of 10 studies regarding the effects of opioid use in older adults with cancer and chronic non-cancer pain, 6 studies showed no effect of opioid use on cognitive domains; the remaining 4 studies, all with higher mean opioid doses) showed mixed effects (both improvements and declines in cognitive performance) with opioid use [137].
Finally, those who reported a history of depression or anxiety or who indicated taking medication for these conditions were not excluded from the study, which could potentially contribute to the perceived declines in memory function in some participants. However, in this study, history of these disorders was not related to baseline cognitive scores, and we found no evidence for variation in feasibility outcomes by depression status, or for a confounding effect of current antidepressant medication use or history of depression or anxiety, suggesting these factors did not influence our findings. SCD has been linked to chronic psychological distress [138–140] and to increased depressive [141–145] and anxiety symptoms [142, 144, 145], a relationship that is likely bidirectional [1]. For example, perceived decline in memory and cognitive functioning can lead to increased anxiety, distress, and fear [146–148], in turn, further accelerating cognitive decline [148] and psychological distress. Moreover, in a recent large, longitudinal study of cognitively normal older adults, co-occurring depression was shown to significantly amplify the risk for incident MCI and ADRD associated with SCD (adjusted HRs for SCD with depression, SCD alone, depression alone, and versus no SCD or depression = 2.8, 2.0, and 1.4) [149]. These findings argue that adults with SCD and co-occurring depression or anxiety represent an at-risk group that should not be excluded from clinical trials of interventions designed to improve cognitive function in those with preclinical memory loss [1].
CONCLUSIONS
Findings of this pilot feasibility trial suggest that incorporating an EUC control arm is both feasible and acceptable in trials of meditation or ML for elders with SCD. While small sample sizes limit conclusions, results of this study also suggest that these practices may be more effective in improving certain cognitive and psychosocial outcomes than active engagement in a EUC comparator program. Clearly, additional larger RCTs with longer term follow-up are needed to confirm and extend the findings of this and our previous trials, and to investigate potential underlying mechanisms.
CONFLICT OF INTEREST
KE Innes, C. Montgomery, TK Selfe, M Flick, and S Wen have no conflicts of interest to declare; DS Khalsa is the Medical Director for the Alzheimer’s Research and Prevention Foundation.
ACKNOWLEDGMENTS
This work was supported by the Alzheimer’s Research and Prevention Foundation (ARPF). We also wish to thank Gina Paisley and Caterina DeFazio for their assistance with data collection. The contents are solely the responsibility of the authors and do not represent the official views of the ARPF.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/ADR-200249.
REFERENCES
[1] | Innes K , Selfe T , Khalsa D , Kandati SA ((2016) ) Effects of meditation versus music listening on perceived stress, mood, sleep and quality of life in adults with early memory loss: A pilot randomized controlled trial. J Alzheimers Dis 52: , 1277–1298. |
[2] | Innes K , Selfe T , Khalsa D , Kandati S ((2017) ) Meditation and music improve cognition in adults with subjective cognitive decline. A preliminary randomized controlled trial. J Alzheimers Dis 56: , 899–916. |
[3] | Si T , Xing G , Han Y ((2020) ) Subjective cognitive decline and related cognitive deficits. Front Neurol 11: , 247. |
[4] | Chan JS , Deng K , Wu J , Yan JH ((2019) ) Effects of meditation and mind–body exercises on older adults’ cognitive performance: A meta-analysis. Gerontologist 59: , e782–e790. |
[5] | Klimecki O , Marchant NL , Lutz A , Poisnel G , Chetelat G , Collette F ((2019) ) The impact of meditation on healthy ageing–the current state of knowledge and a roadmap to future directions. Curr Opin Psychol 28: , 223–228. |
[6] | Vasudev A , Torres-Platas SG , Kerfoot K , Potes A , Therriault J , Gifuni A , Segal M , Looper KJ , Nair V , Lavretsky H , Rej S ((2019) ) Mind-body interventions in late-life mental illnesses and cognitive disorders: A narrative review. Am J Geriatr Psychiatry 27: , 536–547. |
[7] | Sarkamo T ((2018) ) Cognitive, emotional, and neural benefits of musical leisure activities in aging and neurological rehabilitation: A critical review. Ann Phys Rehabil Med 61: , 414–418. |
[8] | Gok Ugur H , Yaman Aktas Y , Orak OS , Saglambilen O , Aydin Avci I ((2017) ) The effect of music therapy on depression and physiological parameters in elderly people living in a Turkish nursing home: A randomized-controlled trial. Aging Ment Health 21: , 1280–1286. |
[9] | Costa F , Ockelford A , Hargreaves DJ ((2018) ) The effect of regular listening to preferred music on pain, depression and anxiety in older care home residents. Psychol Music 46: , 174–191. |
[10] | Innes K , Selfe T , Khalsa D , Kandati SA ((2016) ) A randomized controlled trial of two simple mind-body programs, Kirtan Kriya meditation and music listening, for adults with subjective cognitive decline: Feasibility and acceptability. Compl Ther Med 26: , 98–107. |
[11] | Innes KE , Selfe TK , Brundage K , Montgomery C , Wen S , Kandati S , Bowles H , Khalsa DS , Huysmans Z ((2018) ) Effects of meditation and music-listening on blood biomarkers of cellular aging and Alzheimer’s disease in adults with subjective cognitive decline: An exploratory randomized clinical trial. J Alzheimers Dis 66: , 947–970. |
[12] | Abdulrab K , Heun R ((2008) ) Subjective memory impairment. A review of its definitions indicates the need for a comprehensive set of standardised and validated criteria. Eur Psychiatry 23: , 321–330. |
[13] | Reisberg B , Prichep L , Mosconi L , John ER , Glodzik-Sobanska L , Boksay I , Monteiro I , Torossian C , Vedvyas A , Ashraf N , Jamil IA , de Leon MJ ((2008) ) The pre-mild cognitive impairment, subjective cognitive impairment stage of Alzheimer’s disease. Alzheimers Dement 4: , S98–S108. |
[14] | Jessen F , Amariglio RE , van Boxtel M , Breteler M , Ceccaldi M , Chetelat G , Dubois B , Dufouil C , Ellis KA , van der Flier WM , Glodzik L , van Harten AC , de Leon MJ , McHugh P , Mielke MM , Molinuevo JL , Mosconi L , Osorio RS , Perrotin A , Petersen RC , Rabin LA , Rami L , Reisberg B , Rentz DM , Sachdev PS , de la Sayette V , Saykin AJ , Scheltens P , Shulman MB , Slavin MJ , Sperling RA , Stewart R , Uspenskaya O , Vellas B , Visser PJ , Wagner M , Subjective Cognitive Decline Initiative Working Group ((2014) ) A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement 10: , 844–852. |
[15] | Rabin LA , Smart CM , Crane PK , Amariglio RE , Berman LM , Boada M , Buckley RF , Chetelat G , Dubois B , Ellis KA , Gifford KA , Jefferson AL , Jessen F , Katz MJ , Lipton RB , Luck T , Maruff P , Mielke MM , Molinuevo JL , Naeem F , Perrotin A , Petersen RC , Rami L , Reisberg B , Rentz DM , Riedel-Heller SG , Risacher SL , Rodriguez O , Sachdev PS , Saykin AJ , Slavin MJ , Snitz BE , Sperling RA , Tandetnik C , van der Flier WM , Wagner M , Wolfsgruber S , Sikkes SAM ((2015) ) Subjective cognitive decline in older adults: An overview of self-report measures used across 19 international research studies. J Alzheimers Dis 48: (Suppl 1), S63–86. |
[16] | Molinuevo JL , Rabin LA , Amariglio R , Buckley R , Dubois B , Ellis KA , Ewers M , Hampel H , Kloppel S , Rami L , Reisberg B , Saykin AJ , Sikkes S , Smart CM , Snitz BE , Sperling R , van der Flier WM , Wagner M , Jessen F , Subjective Cognitive Decline Initiative Working Group ((2017) ) Implementation of subjective cognitive decline criteria in research studies. Alzheimers Dement 13: , 296–311. |
[17] | Jessen F , Steffen Wolfsgruber , Wiese B , Bickeld H , Mösch E , Kaduszkiewicz H , Pentzek M , Riedel-Heller SG , Luck T , Fuchs A , Weyerer S , Werle J , Bussche Hvd , Scherer M , Maier W , Wagner M ((2014) ) AD dementia risk in late MCI, in early MCI, and in subjective memory impairment. Alzheimers Dement 10: , 76–83. |
[18] | Alexander Kopparaa , Wagnera M , Langec C , Ernst A , Wiese B , König H-H , Brettschneider C , Riedel-Heller S , Luppa M , Weyerer S , Werl J , Bickel H , Mösch E , Pentzek M , Fuchs A , Steffen Wolfsgruber , Beauducel A , Scherer M , Maier W , Jessen F ((2015) ) Cognitive performance before and after the onset of subjective cognitive decline in old age. Alzheimers Dement 1: , 194–205. |
[19] | Snitz BE , Wang T , Cloonan YK , Jacobsen E , Chang CH , Hughes TF , Kamboh MI , Ganguli M ((2018) ) Risk of progression from subjective cognitive decline to mild cognitive impairment: The role of study setting. Alzheimers Dement 14: , 734–742. |
[20] | Jessen F , Wiese B , Bachmann C , Eifflaender-Gorfer S , Haller F , Kolsch H , Luck T , Mosch E , van den Bussche H , Wagner M , Wollny A , Zimmermann T , Pentzek M , Riedel-Heller SG , Romberg HP , Weyerer S , Kaduszkiewicz H , Maier W , Bickel H ((2010) ) Prediction of dementia by subjective memory impairment: Effects of severity and temporal association with cognitive impairment. Arch Gen Psychiatry 67: , 414–422. |
[21] | Koppara A , Wagner M , Lange C , Ernst A , Wiese B , König H-H , Brettschneider C , Riedel-Heller S , Luppa M , Weyerer S , Werl J , Bickel H , Mösch E , Pentzek M , Fuchs A , Wolfsgruber S , Beauducel A , Scherer M , Maier W , Jessen F ((2015) ) Cognitive performance before and after the onset of subjective cognitive decline in old age. Alzheimers Dement 1: , 194–205. |
[22] | Luck T , Riedel-Heller SG , Luppa M , Wiese B , Bachmann C , Jessen F , Bickel H , Weyerer S , Pentzek M , Konig HH , Prokein J , Eisele M , Wagner M , Mosch E , Werle J , Fuchs A , Brettschneider C , Scherer M , Breitner JC , Maier W ((2014) ) A hierarchy of predictors for dementia-free survival in old-age: Results of the AgeCoDe study. Acta Psychiatr Scand 129: , 63–72. |
[23] | van Harten AC , Mielke MM , Swenson-Dravis DM , Hagen CE , Edwards KK , Roberts RO , Geda YE , Knopman DS , Petersen RC ((2018) ) Subjective cognitive decline and risk of MCI: The Mayo Clinic Study of Aging. Neurology 91: , e300–e312. |
[24] | Verfaillie SC , Timmers T , Slot RE , Van Der Weijden CW , Wesselman LM , Prins ND , Sikkes SA , Yaqub M , Dols A , Lammertsma AA , Scheltens P , Ossenkoppele R , van Berckel BNM , van der Flier WM ((2019) ) Amyloid-β load is related to worries, but not to severity of cognitive complaints in individuals with subjective cognitive decline: The SCIENCe project. Front Aging Neurosci 11: , 7. |
[25] | Miebach L , Wolfsgruber S , Polcher A , Peters O , Menne F , Luther K , Incesoy E , Priller J , Spruth E , Altenstein S ((2019) ) Which features of subjective cognitive decline are related to amyloid pathology? Findings from the DELCODE study. Alzheimers Res Ther 11: , 66. |
[26] | Vickers AJ ((2006) ) How to randomize. J Soc Integr Oncol 4: , 194–198. |
[27] | Khalsa DS , Newberg A ((2011) ) Kirtan Kriya meditation: A promising technique for enhancing cognition in memory-impaired older adults. In Enhancing Cognitive Fitness in Adults: A Guide to the Use and Development of Community-Based Programs, Hartman-Stein PE, Rue AL, eds. Springer New York, pp. 419–431. |
[28] | Gilewski MJ , Zelinski EM , Schaie KW ((1990) ) The Memory Functioning Questionnaire for assessment of memory complaints in adulthood and old age. Psychol Aging 5: , 482–490. |
[29] | Reitan RM ((1958) ) Validity of the Trail Making Test as an indicator of organic brain damage. Percept Mot Skills 8: , 271–276. |
[30] | Wechsler D (1981) WAIS-R manual: Wechsler adult intelligence scale-revised, Psychological Corporation, New York. |
[31] | Michell B , Sambuchi N , Geda Y , Muraccioli I , Paban V , Jouve E , Sambuc R , Chen H-M , Bartolin A , Gallant C , Jean J-CS , Rouyer C , Brosset C , Azorin J-M , Alescio-Lautier B , Petersen R ((2014) ) Subjective cognitive impairment in a French sample. Neurol Clin Neurophysiol 82: , P2.174. |
[32] | Hagenaars SP , Cox SR , Hill WD , Davies G , Liewald DCM , CHARGE consortium Cognitive Working Group, Harris SE , McIntosh AM , Gale CR , Deary IJ ((2018) ) Genetic contributions to Trail Making Test performance in UK Biobank. Mol Psychiatry 23: , 1575–1583. |
[33] | Bell-McGinty S , Podell K , Franzen M , Baird AD , Williams MJ ((2002) ) Standard measures of executive function in predicting instrumental activities of daily living in older adults. Int J Geriatr Psychiatry 17: , 828–834. |
[34] | Lezak MD , Howieson DB , Loring DW ((2004) ), Neuropsychological Assessment (4th ed.). Oxford University Press, New York. |
[35] | Cohen S , Kamarck T , Mermelstein R ((1983) ) A global measure of perceived stress. J Health Soc Behav 24: , 385–396. |
[36] | Cohen S ((1988) ) Perceived stress in a probability sample of the United States. In The Social Psychology of Health, Spacapan S, Oskamp S, eds. Sage Publications , Thousand Oaks, pp. 31–67. |
[37] | Buysse DJ , Reynolds CF 3rd , Monk TH , Berman SR , Kupfer DJ ((1989) ) The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res 28: , 193–213. |
[38] | Berger BG , Motl RW ((2000) ) Exercise and mood: A selective review and synthesis of research employing the Profile of Mood States. J Appl Sport Psychol 12: , 69–92. |
[39] | Ryff CD , Keyes CL ((1995) ) The structure of psychological well-being revisited. J Pers Soc Psychol 69: , 719–727. |
[40] | Ware JE Jr. , Sherbourne CD ((1992) ) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30: , 473–483. |
[41] | Lane JD , Seskevich JE , Pieper CF ((2007) ) Brief meditation training can improve perceived stress and negative mood. Alt Ther Health Med 13: , 38–44. |
[42] | Beusterien KM , Steinwald B , Ware JE Jr. ((1996) ) Usefulness of the SF-36 Health Survey in measuring health outcomes in the depressed elderly. J Geriatr Psychiatry Neurol 9: , 13–21. |
[43] | Kosinski M , Keller SD , Ware JE Jr , Hatoum HT , Kong SX ((1999) ) The SF-36 Health Survey as a generic outcome measure in clinical trials of patients with osteoarthritis and rheumatoid arthritis: Relative validity of scales in relation to clinical measures of arthritis severity. Med Care 37: , MS23–MS39. |
[44] | Agid Y , Dubois B , Anand R , Gharabawi G , Investigators IR ((1998) ) Efficacy and tolerability of rivastigmine in patients with dementia of the Alzheimer type. Curr Ther Res Clin Exp 59: , 837–845. |
[45] | Sharma VK , Das S , Mondal S , Goswami U , Gandhi A ((2006) ) Effect of Sahaj Yoga on neuro-cognitive functions in patients suffering from major depression. Indian J Physiol Pharmacol 50: , 375–383. |
[46] | Innes KE , Selfe TK , Brown C , Rose K , Thompson-Heisterman A ((2012) ) The effects of meditation on perceived stress and related indices of psychological status and sympathetic activation in persons with Alzheimer’s disease and their caregivers: A pilot study. Evid Based Compl Alt Med 2012: , 927509. |
[47] | Galantino ML , Baime M , Maguire M , Szapary PO , Farrar JT ((2005) ) Short Communication: Association of psychological and physiological measures of stress in health-care professionals during an 8-week mindfulness meditation program: Mindfulness in practice. Stress Health 21: , 255–261. |
[48] | Hilcove K , Marceau C , Thekdi P , Larkey L , Brewer MA , Jones K ((2020) ) Holistic nursing in practice: Mindfulness-based yoga as an intervention to manage stress and burnout. J Holistic Nurs, doi: 10.1177/0898010120921587 |
[49] | Lynch J , Prihodova L , Dunne PJ , Carroll Á , Walsh C , McMahon G , White B ((2018) ) Mantra meditation for mental health in the general population: A systematic review. Eur J Integr Med 23: , 101–108. |
[50] | Milbury K , Chaoul A , Biegler K , Wangyal T , Spelman A , Meyers CA , Arun B , Palmer JL , Taylor J , Cohen L ((2013) ) Tibetan sound meditation for cognitive dysfunction: Results of a randomized controlled pilot trial. Psychooncology 22: , 2354–2363. |
[51] | Modi S , Joshi U , Narayanakurup D ((2018) ) To what extent is mindfulness training effective in enhancing self-esteem, self-regulation and psychological well-being of school going early adolescents? J Indian Assoc Child Adolesc Ment Health 14: , 89–108. |
[52] | Nanthakwang N , Siviroj P , Matanasarawoot A , Sapbamrer R , Lerttrakarnnon P , Awiphan R ((2020) ) Effectiveness of deep breathing and body scan meditation combined with music to improve sleep quality and quality of life in older adults. Open Pub Health J 13: , 232–239. |
[53] | Sarmento CVM , Moon S , Pfeifer T , Smirnova IV , Colgrove Y , Lai SM , Liu W ((2020) ) The therapeutic efficacy of Qigong exercise on the main symptoms of fibromyalgia: A pilot randomized clinical trial. Integr Med Res 9: , 100416. |
[54] | Sieczkowska SM , Casagrande PDO , Coimbra DR , Vilarino GT , Andreato LV , Andrade A ((2019) ) Effect of yoga on the quality of life of patients with rheumatic diseases: Systematic review with meta-analysis. Compl Ther Med 46: , 9–18. |
[55] | Takemura N , Cheung DST , Smith R , Deng W , Ho KY , Lin J , Kwok JYY , Lam TC , Lin CC ((2020) ) Effectiveness of aerobic exercise and mind-body exercise in cancer patients with poor sleep quality: A systematic review and meta-analysis of randomized controlled trials. Sleep Med Rev 53: , 101334. |
[56] | Travis F , Valosek L , Konrad A , Link J , Salerno J , Scheller R , Nidich S ((2018) ) Effect of meditation on psychological distress and brain functioning: A randomized controlled study. Brain Cogn 125: , 100–105. |
[57] | Wang WL , Chen KH , Pan YC , Yang SN , Chan YY ((2020) ) The effect of yoga on sleep quality and insomnia in women with sleep problems: A systematic review and meta-analysis. BMC Psychiatry 20: , 195. |
[58] | Zou L , Loprinzi PD , Yeung AS , Zeng N , Huang T ((2019) ) The beneficial effects of mind-body exercises for people with mild cognitive impairment: A systematic review with meta-analysis. Arch Phys Med Rehabil 100: , 1556–1573. |
[59] | van Ginkel JR , Kroonenberg PM ((2014) ) Analysis of variance of multiply imputed data. Multivariate Behav Res 49: , 78–91. |
[60] | Carpenter JR , Kenward MG ((2013) ) Multiple imputation and its application. John Wiley & Sons, Chichester, U.K. |
[61] | Ryan GW , Bernard HR ((2003) ) Techniques to identify themes. Field Methods 15: , 85–109. |
[62] | Hunt CA , Hoffman MA , Mohr JJ , Williams A-l ((2020) ) Assessing perceived barriers to meditation: The Determinants of Meditation Practice Inventory-Revised (DMPI-R). Mindfulness 11: , 1139–1149. |
[63] | Rietschel CH ((2016) ) Quantifying barriers to meditation as a health behavior: Exploratory and confirmatory factor analysis of the determinants of meditation practice inventory. Master’s Thesis, Department of Counseling, Higher Education, and Special Education University of Maryland, College Park. |
[64] | Patel NK , Akkihebbalu S , Espinoza SE , Chiodo LK ((2011) ) Perceptions of a community-based yoga intervention for older adults. Act Adapt Aging 35: , 151–163. |
[65] | Innes KE , Selfe TK , Kandati S , Wen S , Huysmans Z ((2018) ) Effects of mantra meditation versus music listening on knee pain, function, and related outcomes in older adults with knee osteoarthritis: An exploratory randomized clinical trial (RCT). Evid Based Complement Alternat Med 2018: , 7683897. |
[66] | Selfe T , Innes K ((2013) ) Effects of meditation on symptoms of knee osteoarthritis: A pilot study. Alt Compl Ther 19: , 139–146. |
[67] | Jessen F , Amariglio RE , Buckley RF , van der Flier WM , Han Y , Molinuevo JL , Rabin L , Rentz DM , Rodriguez-Gomez O , Saykin AJ , Sikkes SAM , Smart CM , Wolfsgruber S , Wagner M ((2020) ) The characterisation of subjective cognitive decline. Lancet Neurol 19: , 271–278. |
[68] | Leggieri M , Thaut MH , Fornazzari L , Schweizer TA , Barfett J , Munoz DG , Fischer CE ((2019) ) Music intervention approaches for Alzheimer’s disease: A review of the literature. Front Neurosci 13: , 132. |
[69] | Xu B , Sui Y , Zhu C , Yang X , Zhou J , Li L , Ren L , Wang X ((2017) ) Music intervention on cognitive dysfunction in healthy older adults: A systematic review and meta-analysis. Neurol Sci 38: , 983–992. |
[70] | Gard T , Holzel BK , Lazar SW ((2014) ) The potential effects of meditation on age-related cognitive decline: A systematic review. Ann N Y Acad Sci 1307: , 89–103. |
[71] | Chiesa A , Calati R , Serretti A ((2011) ) Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings.. Clin Psychol Rev 31: , 449–464. |
[72] | Sun JX , Kang JX , Wang P , Zeng H ((2013) ) Self-relaxation training can improve sleep quality and cognitive functions in the older: A one-year randomised controlled trial. J Clin Nurs 22: , 1270–1280. |
[73] | Lavretsky H , Epel ES , Siddarth P , Nazarian N , Cyr NS , Khalsa DS , Lin J , Blackburn E , Irwin MR ((2013) ) A pilot study of yogic meditation for family dementia caregivers with depressive symptoms: Effects on mental health, cognition, and telomerase activity. Int J Geriatr Psychiatry 28: , 57–65. |
[74] | Newberg AB , Wintering N , Khalsa DS , Roggenkamp H , Waldman MR ((2010) ) Meditation effects on cognitive function and cerebral blood flow in subjects with memory loss: A preliminary study. J Alzheimers Dis 20: , 517–526. |
[75] | Henneghan AM , Becker H , Harrison ML , Inselmann K , Fico B , Schafer H , King E , Patt D , Kesler S ((2020) ) A randomized control trial of meditation compared to music listening to improve cognitive function for breast cancer survivors: Feasibility and acceptability. Complement Ther Clin Pract 41: , 101228. |
[76] | Eyre HA , Siddarth P , Acevedo B , Van Dyk K , Paholpak P , Ercoli L , St Cyr N , Yang H , Khalsa DS , Lavretsky H ((2017) ) A randomized controlled trial of Kundalini yoga in mild cognitive impairment. Int Psychogeriatr 29: , 557–567. |
[77] | Wetherell JL , Hershey T , Hickman S , Tate SR , Dixon D , Bower ES , Lenze EJ ((2017) ) Mindfulness-based stress reduction for older adults with stress disorders and neurocognitive difficulties: A randomized controlled trial. J Clin Psychiatry 78: , e734–e743. |
[78] | Quintana-Hernández DJ , Miró-Barrachina MT , Ibáñez-Fernández IJ , Pino AS , Quintana-Montesdeoca MP , Rodríguez-de Vera B , Morales-Casanova D , Pérez-Vieitez Mdel C , Rodríguez-García J , Bravo-Caraduje N ((2016) ) Mindfulness in the maintenance of cognitive capacities in Alzheimer’s disease: A randomized clinical trial. J Alzheimers Dis 50: , 217–232. |
[79] | Alexander CN , Langer EJ , Newman RI , Chandler HM , Davies JL ((1989) ) Transcendental meditation, mindfulness, and longevity: An experimental study with the elderly. J Pers Soc Psychol 57: , 950–964. |
[80] | Baylan S , Haig C , MacDonald M , Stiles C , Easto J , Thomson M , Cullen B , Quinn TJ , Stott D , Mercer SW , Broomfield NM , Murray H , Evans JJ ((2020) ) Measuring the effects of listening for leisure on outcome after stroke (MELLO): A pilot randomized controlled trial of mindful music listening. Int J Stroke 15: , 149–158. |
[81] | Sarkamo T , Tervaniemi M , Laitinen S , Forsblom A , Soinila S , Mikkonen M , Autti T , Silvennoinen HM , Erkkila J , Laine M , Peretz I , Hietanen M ((2008) ) Music listening enhances cognitive recovery and mood after middle cerebral artery stroke. Brain 131: , 866–876. |
[82] | Sarkamo T , Soto D ((2012) ) Music listening after stroke: Beneficial effects and potential neural mechanisms. Ann N Y Acad Sci 1252: , 266–281. |
[83] | Sarkamo T , Tervaniemi M , Laitinen S , Numminen A , Kurki M , Johnson JK , Rantanen P ((2014) ) Cognitive, emotional, and social benefits of regular musical activities in early dementia: Randomized controlled study. Gerontologist 54: , 634–650. |
[84] | Chu H , Yang CY , Lin Y , Ou KL , Lee TY , O’Brien AP , Chou KR ((2014) ) The impact of group music therapy on depression and cognition in elderly persons with dementia: A randomized controlled study.. Biol Res Nurs 16: , 209–217. |
[85] | Perez-Ros P , Cubero-Plazas L , Mejias-Serrano T , Cunha C , Martinez-Arnau FM ((2019) ) Preferred music listening intervention in nursing home residents with cognitive impairment: A randomized intervention study. J Alzheimers Dis 70: , 433–442. |
[86] | Mallya S , Fiocco AJ ((2016) ) Effects of mindfulness training on cognition and well-being in healthy older adults. Mindfulness 7: , 453–465. |
[87] | Moynihan JA , Chapman BP , Klorman R , Krasner MS , Duberstein PR , Brown KW , Talbot NL ((2013) ) Mindfulness-based stress reduction for older adults: Effects on executive function, frontal alpha asymmetry and immune function. Neuropsychobiology 68: , 34–43. |
[88] | Polsinelli AJ , Kaszniak AW , Glisky EL , Ashish D ((2020) ) Effects of a brief, online, focused attention mindfulness training on cognition in older adults: A randomized controlled trial. Mindfulness 11: , 1182–1193. |
[89] | Oken BS , Wahbeh H , Goodrich E , Klee D , Memmott T , Miller M , Fu R ((2017) ) Meditation in stressed older adults: Improvements in self-rated mental health not paralleled by improvements in cognitive function or physiological measures. Mindfulness 8: , 627–638. |
[90] | Wells RE , Kerr CE , Wolkin J , Dossett M , Davis RB , Walsh J , Wall RB , Kong J , Kaptchuk T , Press D , Phillips RS , Yeh G ((2013) ) Meditation for adults with mild cognitive impairment: A pilot randomized trial. J Am Ger Soc 61: , 642–645. |
[91] | Klainin-Yobas P , Kowitlawakul Y , Lopez V , Tang CT , Hoek KE , Gan GL , Lei F , Rawtaer I , Mahendran R ((2019) ) The effects of mindfulness and health education programs on the emotional state and cognitive function of elderly individuals with mild cognitive impairment: A randomized controlled trial. J Clin Neurosci 68: , 211–217. |
[92] | Fam J , Sun Y , Qi P , Lau RC , Feng L , Kua EH , Mahendran R ((2020) ) Mindfulness practice alters brain connectivity in community-living elders with mild cognitive impairment. Psychiatry Clin Neurosci 74: , 257–262. |
[93] | Oken BS , Fonareva I , Haas M , Wahbeh H , Lane JB , Zajdel D , Amen A ((2010) ) Pilot controlled trial of mindfulness meditation and education for dementia caregivers. J Altern Complement Med 16: , 1031–1038. |
[94] | Ernst S , Welke J , Heintze C , Gabriel R , Zollner A , Kiehne S , Schwantes U , Esch T ((2008) ) Effects of mindfulness-based stress reduction on quality of life in nursing home residents: A feasibility study. Forsch Komplementmed 15: , 74–81. |
[95] | Optale G , Urgesi C , Busato V , Marin S , Piron L , Priftis K , Gamberini L , Capodieci S , Bordin A ((2010) ) Controlling memory impairment in elderly adults using virtual reality memory training: A randomized controlled pilot study. Neurorehabil Neural Repair 24: , 348–357. |
[96] | Bruer RA , Spitzriagel E , Cloninger CR ((2007) ) The temporal limits of cognitive change from music therapy in elderly persons with dementia or dementia-like cognitive impairment: A Randomized controlled trial. J Music Ther 44: , 308–328. |
[97] | Li CH , Liu CK , Yang YH , Chou MC , Chen CH , Lai CL ((2015) ) Adjunct effect of music therapy on cognition in Alzheimer’s disease in Taiwan: A pilot study. Neuropsychiatr Dis Treat 11: , 291–296. |
[98] | Wayne PM , Walsh JN , Taylor-Piliae RE , Wells RE , Papp KV , Donovan NJ , Yeh GY ((2014) ) Effect of tai chi on cognitive performance in older adults: Systematic review and meta-analysis. J Am Geriatr Soc 62: , 25–39. |
[99] | Kelly ME , Loughrey D , Lawlor BA , Robertson IH , Walsh C , Brennan S ((2014) ) The impact of exercise on the cognitive functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res Rev 16: , 12–31. |
[100] | Cheng ST , Chow PK , Song YQ , Yu EC , Chan AC , Lee TM , Lam JH ((2014) ) Mental and physical activities delay cognitive decline in older persons with dementia. Am J Geriatr Psychiatry 22: , 63–74. |
[101] | Gates N , Fiatarone Singh MA , Sachdev PS , Valenzuela M ((2013) ) The effect of exercise training on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Am J Geriatr Psychiatry 21: , 1086–1097. |
[102] | Kelly ME , Loughrey D , Lawlor BA , Robertson IH , Walsh C , Brennan S ((2014) ) The impact of cognitive training and mental stimulation on cognitive and everyday functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res Rev 15: , 28–43. |
[103] | Reijnders J , van Heugten C , van Boxtel M ((2013) ) Cognitive interventions in healthy older adults and people with mild cognitive impairment: A systematic review. Ageing Res Rev 12: , 263–275. |
[104] | Law LLF , Barnett F , Yau MK , Gray MA ((2014) ) Effects of combined cognitive and exercise interventions on cognition in older adults with and without cognitive impairment: A systematic review. Ageing Res Rev 15: , 61–75. |
[105] | Ngandu T , Lehtisalo J , Solomon A , Levalahti E , Ahtiluoto S , Antikainen R , Backman L , Hanninen T , Jula A , Laatikainen T , Lindstrom J , Mangialasche F , Paajanen T , Pajala S , Peltonen M , Rauramaa R , Stigsdotter-Neely A , Strandberg T , Tuomilehto J , Soininen H , Kivipelto M ((2015) ) A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 385: , 2255–2263. |
[106] | Cohen-Mansfield J , Cohen R , Buettner L , Eyal N , Jakobovits H , Rebok G , Rotenberg-Shpigelman S , Sternberg S ((2015) ) Interventions for older persons reporting memory difficulties: A randomized controlled pilot study. Int J Geriatr Psychiatry 30: , 478–486. |
[107] | Farhang M , Miranda-Castillo C , Rubio M , Furtado G ((2019) ) Impact of mind-body interventions in older adults with mild cognitive impairment: A systematic review. Int Psychogeriatr 31: , 643–666. |
[108] | Chouinard AM , Larouche E , Audet MC , Hudon C , Goulet S ((2019) ) Mindfulness and psychoeducation to manage stress in amnestic mild cognitive impairment: A pilot study. Aging Ment Health 23: , 1246–1254. |
[109] | Song D , Yu DSF , Li PWC , Lei Y ((2018) ) The effectiveness of physical exercise on cognitive and psychological outcomes in individuals with mild cognitive impairment: A systematic review and meta-analysis. Int J Nurs Stud 79: , 155–164. |
[110] | Lautenschlager NT , Cox KL , Flicker L , Foster JK , van Bockxmeer FM , Xiao J , Greenop KR , Almeida OP ((2008) ) Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: A randomized trial. JAMA 300: , 1027–1037. |
[111] | Bhome R , Berry AJ , Huntley JD , Howard RJ ((2018) ) Interventions for subjective cognitive decline: Systematic review and meta-analysis. BMJ Open 8: , e021610. |
[112] | Lam LCW , Chau RCM , Wong BML , Fung AWT , Lui VWC , Tam CCW , Leung GTY , Kwok TCY , Chiu HFK , Ng S , Chan WM ((2011) ) Interim follow-up of a randomized controlled trial comparing Chinese style mind body (Tai Chi) and stretching exercises on cognitive function in subjects at risk of progressive cognitive decline. Int Psychogeriatr y 26: , 733–740. |
[113] | Klusmann V , Evers A , Schwarzer R , Schlattmann P , Reischies FM , Heuser I , Dimeo FC ((2010) ) Complex mental and physical activity in older women and cognitive performance: A 6-month randomized controlled trial. J Gerontol Biol Sci Med Sci 65: , 680–688. |
[114] | Maki Y , Ura C , Yamaguchi T , Murai T , Isahai M , Kaiho A , Yamagami T , Tanaka S , Miyamae F , Sugiyama M , Awata S , Takahashi R , Yamaguchi H ((2012) ) Effects of intervention using a community-based walking program for prevention of mental decline: A randomized controlled trial. J Am Geriatr Soc 60: , 505–510. |
[115] | Brown AK , Liu-Ambrose T , Tate R , Lord SR ((2009) ) The effect of group-based exercise on cognitive performance and mood in seniors residing in intermediate care and self-care retirement facilities: A randomised controlled trial. Br J Sports Med 43: , 608–614. |
[116] | Klusmann V , Evers A , Schwarzer R , Schlattmann P , Reischies FM , Heuser I , Dimeo FC ((2010) ) Complex mental and physical activity in older women and cognitive performance: A 6-month randomized controlled trial. J Gerontol Biol Sci Med Sci 65: , 680–688. |
[117] | Coyle H , Traynor V , Solowij N ((2015) ) Computerized and virtual reality cognitive training for individuals at high risk of cognitive decline: Systematic review of the literature. Am J Geriatr Psychiatry 23: , 335–359. |
[118] | Diamond K , Mowszowski L , Cockayne N , Norrie L , Paradise M , Hermens DF , Lewis SJG , Hickie IB , Naismith SL ((2015) ) Randomized controlled trial of a healthy brain ageing cognitive training program: Effects on memory, mood, and sleep. J Alzheimers Dis 44: , 1181–1191. |
[119] | Strandberg T , Ngandu T , Antikainen R , Laatikainen T , Lindström J , Pajala S , Tuomilehto J , Soininen H , Kivipelto M ((2015) ) Health-related quality of life in a multidomain intervention trial to prevent cognitive decline (the FINGER Study). Eur Geriatr Med 6S1: , S5–S31. |
[120] | Greenaway MC , Duncan NL , Smith GE ((2013) ) The memory support system for mild cognitive impairment: Randomized trial of a cognitive rehabilitation intervention. Int J Geriatr Psychiatry 28: , 402–409. |
[121] | Kurz A , Pohl C , Ramsenthaler M , Sorg C ((2009) ) Cognitive rehabilitation in patients with mild cognitive impairment. Int J Geriatr Psychiatry 24: , 163–168. |
[122] | Chan MF , Wong ZY , Onishi H , Thayala NV ((2012) ) Effects of music on depression in older people: A randomised controlled trial. J Clin Nurs 21: , 776–783. |
[123] | Chan MF , Chan EA , Mok E ((2010) ) Effects of music on depression and sleep quality in elderly people: A randomised controlled trial. Complement Ther Med 18: , 150–159. |
[124] | Rapp S , Brenes G , Marsh AP ((2002) ) Memory enhancement training for older adults with mild cognitive impairment: A preliminary study. Aging Ment Health 6: , 5–11. |
[125] | Merrill DA , Siddarth P , Saito NY , Ercoli LM , Burggren AC , Kepe V , Lavretsky H , Miller KJ , Kim J , Huang S ((2012) ) Self-reported memory impairment and brain PET of amyloid and tau in non-demented middle-aged and older adults. Int Psychogeriatr 24: , 1076. |
[126] | Smith GE , Petersen RC , Ivnik RJ , Malec JF , Tangalos EG ((1996) ) Subjective memory complaints, psychological distress, and longitudinal change in objective memory performance. Psychol Aging 11: , 272–279. |
[127] | Snitz BE , Weissfeld LA , Cohen AD , Lopez OL , Nebes RD , Aizenstein HJ , McDade E , Price JC , Mathis CA , Klunk WE ((2015) ) Subjective cognitive complaints, personality and brain amyloid-beta in cognitively normal older adults. Am J Geriatr Psychiatry 23: , 985–993. |
[128] | Amariglio RE , Becker JA , Carmasin J , Wadsworth LP , Lorius N , Sullivan C , Maye JE , Gidicsin C , Pepin LC , Sperling RA , Johnson KA , Rentz DM ((2012) ) Subjective cognitive complaints and amyloid burden in cognitively normal older individuals. Neuropsychologia 50: , 2880–2886. |
[129] | Baudouin A , Clarys D , Vanneste S , Isingrini M ((2009) ) Executive functioning and processing speed in age-related differences in memory: Contribution of a coding task. Brain Cogn 71: , 240–245. |
[130] | Smeets RJEM , Beelen S , Goossens MEJB , Schouten EGW , Knottnerus JA , Vlaeyen JWS ((2008) ) Treatment expectancy and credibility are associated with the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. Clin J Pain 24: , 305–315. |
[131] | Uebelacker LA , Weinstock LM , Battle CL , Abrantes AM , Miller IW ((2018) ) Treatment credibility, expectancy, and preference: Prediction of treatment engagement and outcome in a randomized clinical trial of hatha yoga vs. health education as adjunct treatments for depression. J Affect Disord 238: , 111–117. |
[132] | Goossens ME , Vlaeyen JW , Hidding A , Kole-Snijders A , Evers SM ((2005) ) Treatment expectancy affects the outcome of cognitive-behavioral interventions in chronic pain. Clin J Pain 21: , 18–26. |
[133] | Constantino MJ , Coyne AE , Boswell JF , Iles BR , Vîsla A ((2018) ) A meta-analysis of the association between patients’ early perception of treatment credibility and their posttreatment outcomes. Psychotherapy (Chic) 55: , 486. |
[134] | Beck AT , Steer RA , Brown G (1996) Beck depression inventory–II. Psychological Assessment. |
[135] | Griffith NM , Szaflarski JP , Szaflarski M , Kent GP , Schefft BK , Howe SR , Privitera MD ((2005) ) Measuring depressive symptoms among treatment-resistant seizure disorder patients: POMS Depression scale as an alternative to the BDI-II. Epilepsy Behav 7: , 266–272. |
[136] | Gibson SJ ((1997) ) The measurement of mood states in older adults. J Gerontol B Psychol Sci Soc Sci 52: , P167–174. |
[137] | Pask S , Dell’Olio M , Murtagh FEM , Boland JW ((2020) ) The effects of opioids on cognition in older adults with cancer and chronic noncancer pain: A systematic review. J Pain Symptom Manage 59: , 871–893 e871. |
[138] | Paradise MB , Glozier NS , Naismith SL , Davenport TA , Hickie IB ((2011) ) Subjective memory complaints, vascular risk factors and psychological distress in the middle-aged: A cross-sectional study. BMC Psychiatry 11: , 108–114. |
[139] | Elfgren C , Gustafson L , Vestberg S , Passant U ((2010) ) Subjective memory complaints, neuropsychological performance and psychiatric variables in memory clinic attendees: A 3-year follow-up study. Arch Gerontol Geriatr 51: , E110–E114. |
[140] | Hurt CS , Burns A , Brown RG , Barrowclough C ((2012) ) Why don’t older adults with subjective memory complaints seek help? Int J Geriatr Psychiatry 27: , 394–400. |
[141] | Schofield PW , Marder M , Dooneief G , Jacobs DM , Sano M , Stern Y ((1997) ) Association of subjective memory complaints with subsequent cognitive decline in community-dwelling elderly individuals with baseline cognitive impairment. Am J Psychiatry 154: , 609–615. |
[142] | Reisberg B , Gauthier S ((2008) ) Current evidence for subjective cognitive impairment (SCI) as the pre-mild cognitive impairment (MCI) stage of subsequently manifest Alzheimer’s disease. Int Psychogeriatr 20: , 1–16. |
[143] | Zandi T ((2004) ) Relationship between subjective memory complaints, objective memory performance, and depression among older adults. Am J Alzheimers Dis Other Demen 19: , 353–360. |
[144] | Clarnette RM , Almeida OP , Forstl H , Paton A , Martins RN ((2001) ) Clinical characteristics of individuals with subjective memory loss in Western Australia: Results from a cross-sectional survey.. Int J Geriatr Psychiatry 16: , 168–174. |
[145] | Montejo P , Montenegro M , Fernandez MA , Maestu F ((2011) ) Subjective memory complaints in the elderly: Prevalence and influence of temporal orientation, depression and quality of life in a population-based study in the city of Madrid. Aging Ment Health 15: , 85–96. |
[146] | Zuniga K , Mackenzie M , Kramer A , McAuley E ((2014) ) Subjective memory impairment and well-being in community-dwelling older adults. Ann Behav Med 47: , S37–S37. |
[147] | Aarts S , van den Akker M , Hajema KJ , van Ingen AM , Metsemakers JFM , Verhey FRJ , van Boxtel MPJ ((2011) ) Multimorbidity and its relation to subjective memory complaints in a large general population of older adults. Int Psychogeriatr 23: , 616–624. |
[148] | Sinoff G , Werner P ((2003) ) Anxiety disorder and accompanying subjective memory loss in the elderly as a predictor of future cognitive decline. Int J Geriatr Psychiatry 18: , 951–959. |
[149] | Liew TM ((2019) ) Depression, subjective cognitive decline, and the risk of neurocognitive disorders. Alzheimers Res Ther 11: , 70. |


