
The effect of external-focus using a paper balloon on the activity of upper limb and trunk muscles during static and dynamic tasks
Abstract
BACKGROUND:
External focus isometric exercises using a paper balloon can change trunk muscle activation in the chest squeeze; however, it is unknown whether this method affects muscle activities in conventional exercises.
OBJECTIVE:
To check variations of trunk muscle activity during front plank (static task) and shoulder press (dynamic task) both with and without instruction to avoid crushing an object.
METHODS:
Twenty-six healthy adult males aged 19–49 were recruited. Ten trunk muscle activities were measured using surface electromyography during a front plank and dynamic shoulder press exercises, both with and without external-focus instruction.
RESULTS:
Adding the external-focus using the paper balloon to the front plank significantly activated 8 out of the 10 muscles. In the downward shoulder press, 5 out of 10 muscles with 50% 1 RM, 2 out of 10 muscles with 100% 1 RM were significantly activated.
CONCLUSIONS:
Adding external-focus instruction using paper balloon increases trunk muscles in front plank and shoulder press while possibly improving trunk stability. Novel exercises using paper balloon may efficiently activate specific muscles without external loading thus possibly reducing the stress on the involved joints during exercise.
1.Introduction
Various lumbar stability exercises are used in lower back treatment programs, or performance improvement in sport [1, 2], and several studies have examined their effects [3, 4]. Rehabilitation professionals have used plank (bridge) exercises to activate the trunk muscles in both healthy individuals and those with lower back pain [5, 6]. Further, there are studies exploring how, theoretically, trunk activities can be enhanced by adding elements, such as unstable surfaces or changing body position. For example, Imai et al. have suggested that lumbar stabilization exercises improve trunk activities when performed on an unstable surface [7], or trunk muscle activation can be changed by different body positions [8].
The press exercise is a popular upper-body resistance exercise that enhances the upper limb and trunk muscles. Variations of pressing exercises exist and are commonly used in weight training for strength and power by strengthening the chest, shoulder, and trunk muscles; developing sport or exercise ability; or simply various activities of daily living. There are also several varieties of pressing exercises based on the available equipment for example a weightlifting bar, dumbbells, kettlebells, or cables. Some studies have also investigated muscle activities according to different body positions or in unstable conditions [9, 10]. In the past, standing and seated or unilaterally compared to bilaterally on muscle activation of the core during shoulder press exercise have been used. Further, press exercise movements can be divided into two phases: push the weight upward (concentric) and return to the start position (eccentric). A study by Luczak et al. examined upper extremity muscle activity between dumbbell bench, incline, and shoulder press exercises, divided into concentric and eccentric phases [11]. Behm et al. conducted a cross-sectional study of trunk and limb exercises, such as chest and shoulder presses, using both uni- and bilateral resistance, combined with the stable/unstable condition [12]. They stated that trunk exercises in unstable conditions were more effective in activating trunk muscles those in stable conditions. However, in resistance exercises for the moving limbs, such as the chest and shoulder press, unilateral conditions were more influential in trunk muscle activation.
Murofushi et al. introduced an isometric method using a paper balloon – an external focused instruction where control must be exerted to not crush an either a solid object or paper balloon, while maintaining a static position during chest squeeze exercise [13]. This method significantly activates the lower trapezius (LT) muscle without involving any complicated movements and causes agonist and antagonist muscle co-contractions between the LT and upper trapezius (UT), latissimus dorsi (Lat), and pectoralis major clavicular part of the pectoralis major (PM) muscles. Further lowering UT and PM muscles activation compared with the conventional isometric method.
However, no study has yet examined whether adding the external-fucus instruction to "not to crush the paper balloon while exerting maximum pressure” to the front plank (static task or trunk exercises) and shoulder press (dynamic task or limb exercises) on muscle activation. Therefore, this study aimed to examine the effect of external-focus using a paper balloon on the activity of upper limb and trunk muscles during static and dynamic tasks.
Figure 1.
Plank hand placement. a: Paper balloon front plank (PBFP) hand setup. b: Front plank (FP) hand setup. I: PBFP, II: FP.
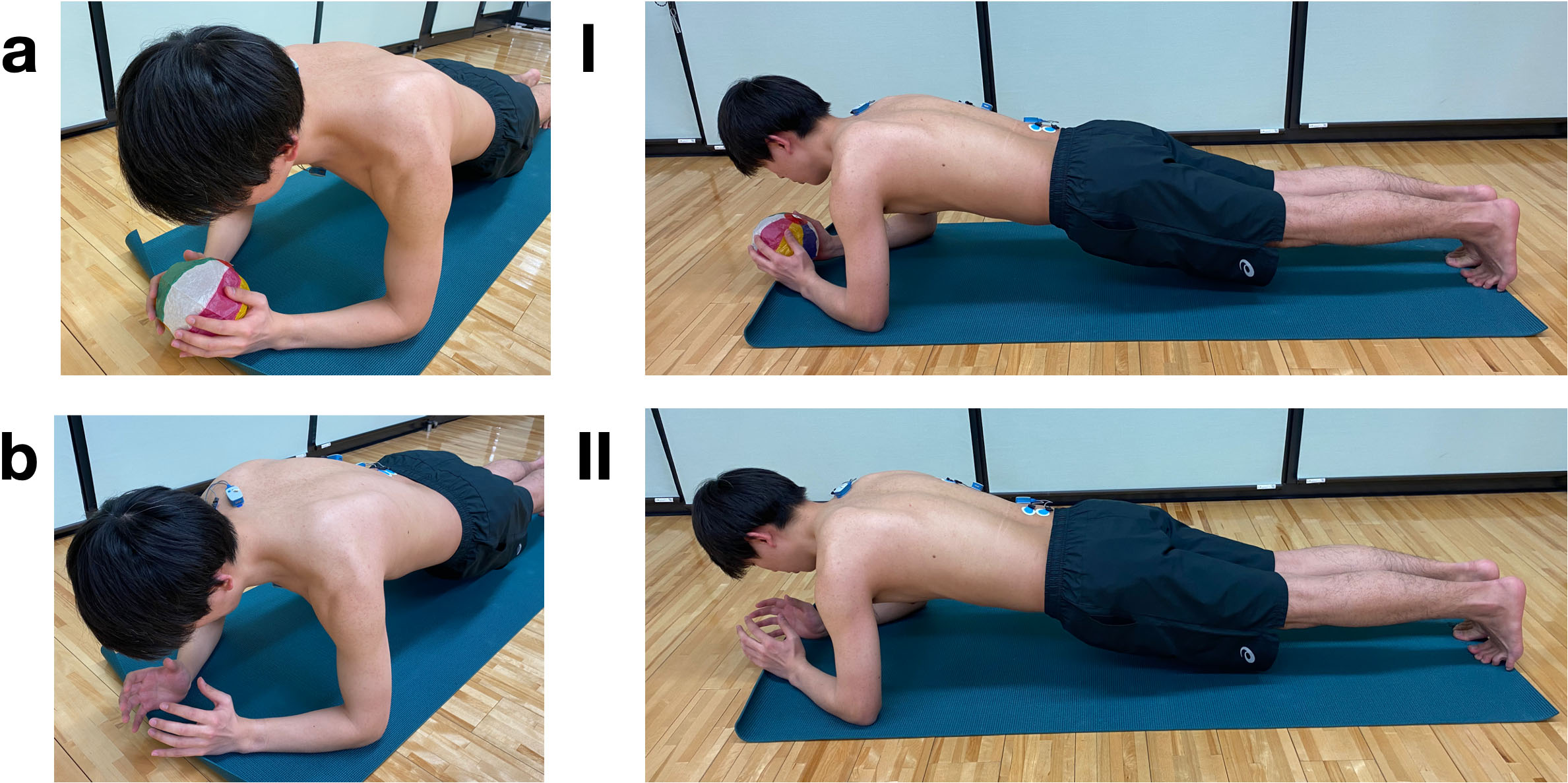
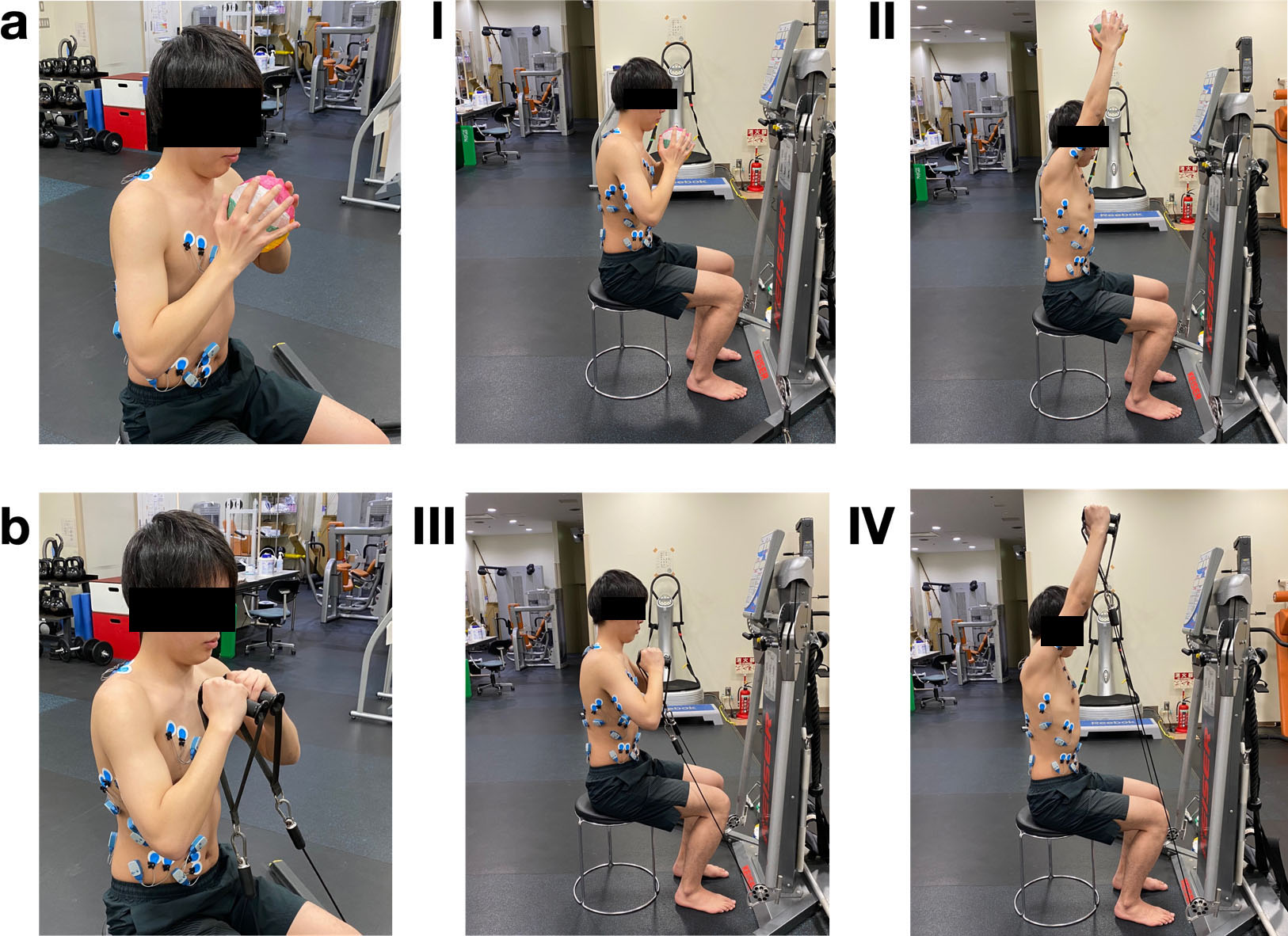
Figure 2.
a. Paper balloon shoulder press (PBSP) hand setup. b. Shoulder press (SP) 50/100 hand setup. I. PBSP low; II. PBSP high; III. SP50/100 low; IV. SP50/100 high.
2.Materials and methods
2.1Participants
In this study, front plank trials (Fig. 1) and shoulder press trials (Fig. 2) were conducted separately. A total of 26 participants for front plank trials and shoulder press trial participated in this study. In front plank trials, 24 healthy males participated (mean age 31.0
2.2Study design
This study was designed as a within-participant repeated-measures. Muscle activity was the dependent variable, and the form of exercise was the independent variable. The research ethics committee of Tokyo Medical and Dental University approved the study (approval number: M2019-295, March 4, 2020). All participants provided written informed consent for participation in the experiment prior to engagement in the study.
2.3Procedures
The front plank and shoulder press exercises were performed, and wireless surface electromyography (EMG) was used to analyze changes in muscle activation and its variability within the same participants and period. Muscle activation when performing the isometric method, using a soft paper balloon [14] with control exerted to avoid crushing the item between the hands, was compared with that achieved by a regular plank exercise and shoulder press loading with air compressor machine.
We requested that participants to hold their body in plank position and either: hold the soft paper balloon while exerting control to avoid crushing it as for set position in front plank (Fig. 1I), identified as the paper balloon front plank (PBFP); or perform a regular front plank exercise (Fig. 1b), identified as the front plank (FP).
For the seated shoulder press while exerting control to avoid crushing the soft paper balloon set position (Fig. 2I/II), identified as the paper balloon shoulder press (PBSP). For the air compressor machine loading on shoulder press, the 50% one repetition maximum (1RM) (Fig. 1d) was identified as SP50, and 100% 1RM (Fig. 2II/IV) is identified as SP100.
2.4Paper balloon
For both PBFP and PBSP we chose a soft paper balloon – or kamifusen (UTF8min紙風船) – a classic Japanese toy balloon with a small hole made from rice paper (configuration of the paper balloon: diameter, 14 cm; weight, 5 g).
2.5Keiser machine
For the SP50 and SP100, we selected the air compressed Functional Trainer Keiser cable machine (Functional Trainer model 3020, height arms up 92 inches/2337 mm, width 96”/2439 mm, depth 47”/ 1194 mm, weight 369 lbs/168 kg, resistance/handle 50 lbs/22 kg; Keiser Corporation, Fresno, CA, USA), and set the cable arms in the lowest position using two cable handles to set the hand position similar to the PBSP (Fig. 2a/b).
2.6Trials
All experimental tests were performed in one day, with one session for both the FP and shoulder press tasks. The participants performed total of four trials for the front plank task – with two trials each for PBFP and FP – and six trials for shoulder press task with two trials each for PBSP, SP50, and SP100. All trials were done in random order. The duration of the trials was defined in order to prevent possible fatigue due to the maximum muscle exertion during the exercise task. A 90-s interval was allowed between each individual test performance [15]. The participants were also instructed to perform the PBFP and FP, PBSP, SP50, and SP100 within the same conditions to control the posture or the joint angles. The examiner evaluated the posture before starting each task and continuously controlled throughout each task.
2.6.1Front plank
With both PBFP and FP, the instruction for the position was given as follows “slowly lift your entire body from the floor, then keep the upper body and legs straight. Do not arch the back, wing the shoulder blades, and bend the hips or the knees. Keep the shoulders directly over the elbows with palms facing each other and the wrist slightly supinated in radial deviation.” Additionally, participants were told to hold a paper balloon while performing the front plank for PBFP. Verbal instructions were given to each participant before each trial to make sure that the proper technique was as follows: “using both hands, try to squeeze the paper balloon with maximum force, but do not crush it.” The joint angles and hand position remained the same by maintaining the object’s shape.
2.6.2Shoulder press
Every participant’s 1RM was measured before the trials to set the load for SP100. The load for the SP50 trial was determined using half the value of SP100. With PBSP, SP50, and SP100 participants were asked to remain in the same position during each trial. Initially, participants were guided to sit on the chair in a naturally upright position with the knees and hips bent at 90
For PBSP, participants were told to hold paper balloon while performing the shoulder press. Verbal instructions were given to each participant before each trial to make sure proper technique was conducted as follows “using both hands, try to squeeze the paper balloon with maximum force, but do not crush it, and keep same tension all the way up, then come back to the starting position.”
For each PBFP and PBSP session, we ensured that the paper balloon was properly inflated. All participants had no experience with the paper balloon method, but each watched an instructional movie prior to attending the experiment. Furthermore, participants had opportunities to practice the method for 5- to 10-min before start of the experiment for familiarization with the exercises.
Figure 3.
The electrode application sites for electromyography. I, posterior view of the upper back; II, posterior view of the lower back; III, lateral view; IV, frontal view of the chest; V, frontal view of the abdomen. A, upper trapezius; B, medial head of the triceps brachii; C, lower trapezius; D, multifidus; E, latissimus dorsi; F, serratus anterior; G, clavicular part of pectorals major; H, external oblique; I, rectus abdominis; J, internal oblique.
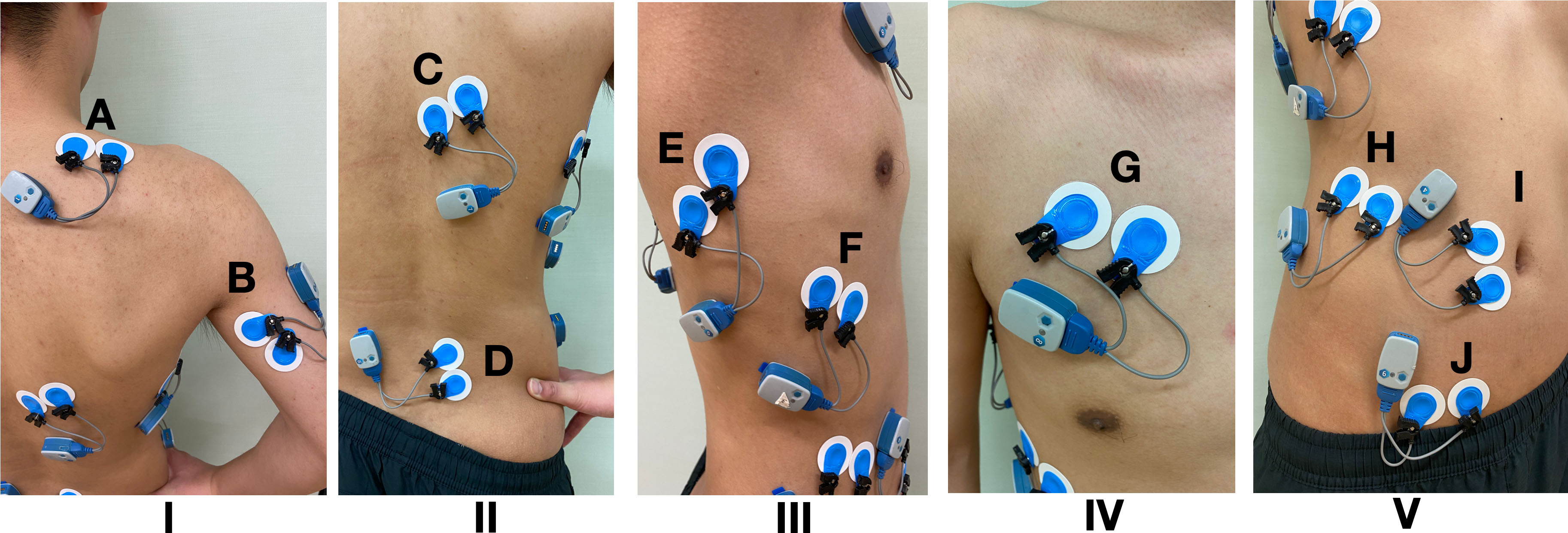
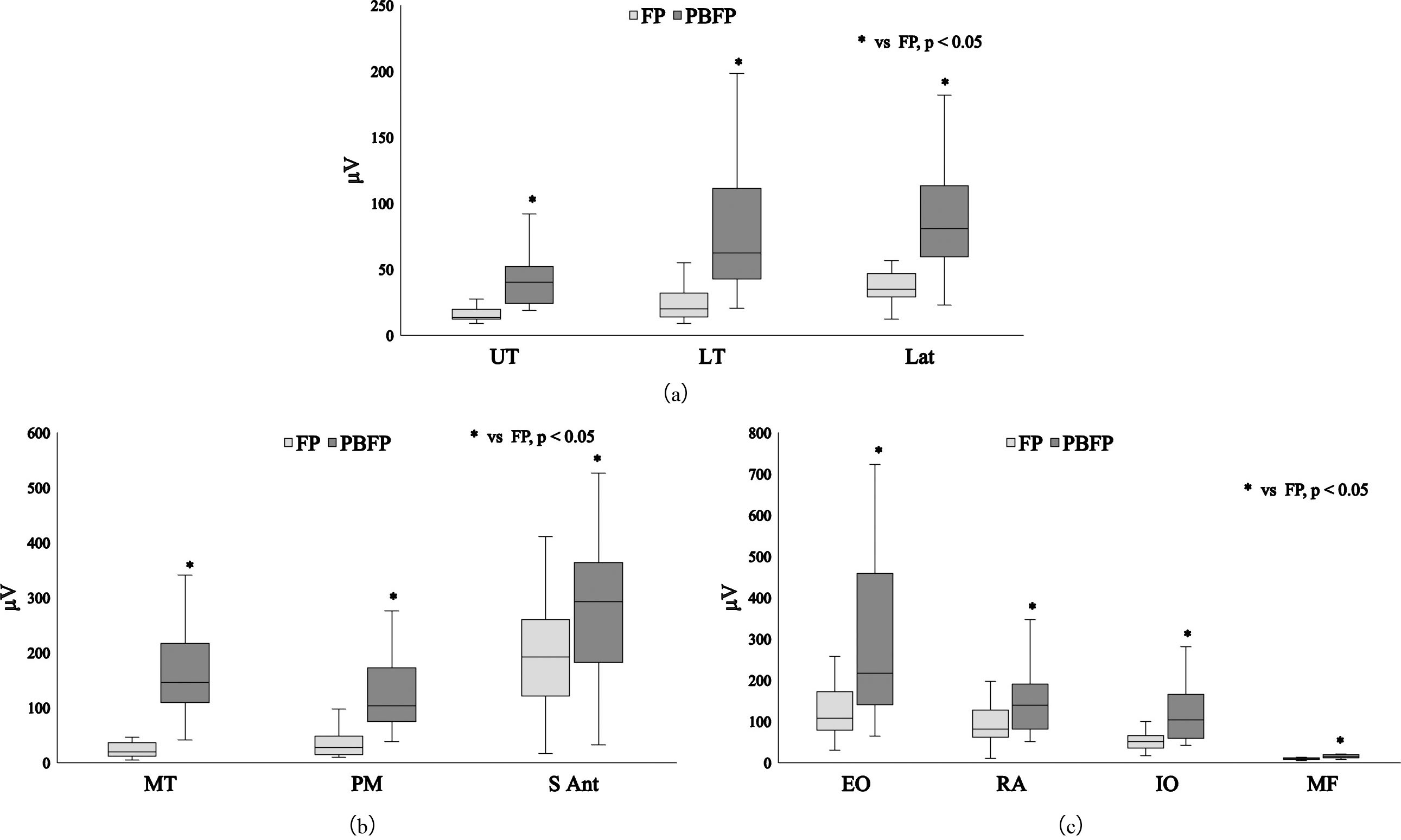
Figure 4.
a. Differences in muscle activity between exercise tasks in the scapulothoracic muscles in front plank. PBFP, paper balloon front plank; FP, front plank. UT, upper trapezius; LT, lower trapezius; Lat, latissimus dorsi. b. Differences in muscle activity between exercise tasks in the scapulohumeral muscles in front plank. PBFP, paper balloon front plank; FP, front plank. MT, medial head of the triceps brachii, PM, clavicular part of the pectoralis major; S Ant, serratus anterior. c. Differences in muscle activity between exercise tasks in trunk muscles in front plank. PBFP, paper balloon front plank; FP, front plank. EO, external oblique; RA, rectus abdominis; IO, internal oblique; MF, multifidus.
2.7Wireless surface EMG
For the EMG recording we used the Ultium, EM-U810M8 by Noraxon (USA Inc., Scottsdale, AZ, USA) with a sampling rate of 2 kHz and band-pass filtering of 10–500 Hz. Before placement of the electrodes, the skin was shaved, abraded, and cleaned with alcohol. The electrode application site for EMG was determined according to prior studies [16, 17] and the SENIAM [18] guidelines. Surface electrodes (Blue Sensor M-00-S, Ambu, Ballerup, Denmark) were attached 35-mm apart to the UT, LT, Lat, medial head of the triceps brachii (MT), PM, serratus anterior (S Ant), external oblique (EO), rectus abdominis (RA), internal oblique (IO) and multifidus (MF) muscles of the right side. The electrodes for each muscle were specifically attached, fixed parallel to the muscle fibers (Fig. 3). Skin impedance was verified to be less than 5-k
Table 1
Results of the statistical analysis for the front plank
| Muscle | Comparison between variables | Cohen’s | ||
|---|---|---|---|---|
| UT | FP vs. PBFP | 5.299 | 1.390 (0.739 to 1.996) | |
| LT | FP vs. PBFP | 4.866 | 1.041 (0.422 to 1.626) | |
| Lat | FP vs. PBFP | 4.701 | 1.361 (0.712 to 1.964) | |
| MT | FP vs. PBFP | 5.485 | 1.691 (1.007 to 2.320) | |
| PM | FP vs. PBFP | 5.134 | 1.087 (0.465 to 1.674) | |
| S Ant | FP vs. PBFP | 2.028 | 0.585 ( | |
| EO | FP vs. PBFP | 3.485 | 1.117 (0.491 to 1.705) | |
| RA | FP vs. PBFP | 2.382 | 0.765 (0.167 to 1.338) | |
| IO | FP vs. PBFP | 3.753 | 0.920 (0.311 to 1.499) | |
| MF | FP vs. PBFP | 4.248 | 1.152 (0.524 to 1.743) |
Figure 5.
a. Differences in muscle activity between exercise tasks in the scapulothoracic muscles in shoulder press upward. PBSP paper balloon shoulder press; SP50, shoulder press 50%; SP100, shoulder press 100%. UT, upper trapezius; LT, lower trapezius; Lat, latissimus dorsi. b. Differences in muscle activity between exercise tasks in the scapulohumeral muscles in shoulder press upward. PBSP paper balloon shoulder press; SP50, shoulder press 50%; SP100, shoulder press 100%; MT, medial head of the triceps brachii; PM, clavicular part of the pectoralis major; S Ant, serratus anterior. c. Differences in muscle activity between exercise tasks in trunk muscles in shoulder press upward. PBSP paper balloon shoulder press; SP50, shoulder press 50%; SP100, shoulder press 100%; EO, external oblique; RA, rectus abdominis; IO, internal oblique; MF, multifidus.
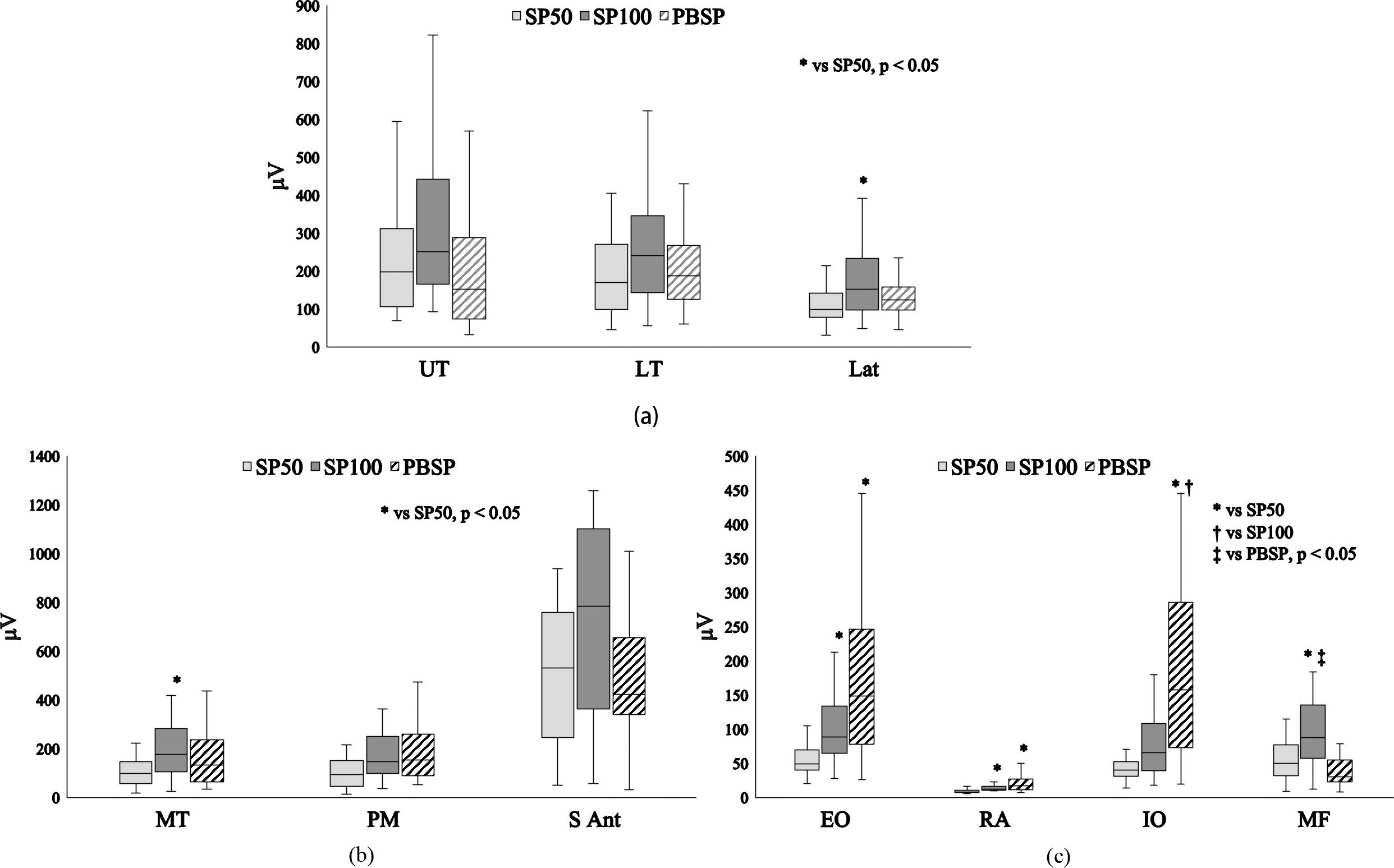
Table 2
The results of statistical analysis for shoulder press – upward
|
|
|
|
| ||||||||||
| UT | SP50 vs. SP100 | 0.538 ( | |||||||||||
| SP50 vs. PBSP | 5.784 | 0.055 |
| ||||||||||
| SP100 vs. PBSP | |||||||||||||
| LT | SP50 vs. SP100 | 0.659 (0.027 to 1.268) | |||||||||||
| SP50 vs. PBSP | 3.756 | 0.153 |
| 0.289 ( | |||||||||
| SP100 vs. PBSP | |||||||||||||
| Lat | SP50 vs. SP100 | 0.770 (0.129 to 1.381) | |||||||||||
| SP50 vs. PBSP | 6.180 | 0.034 | 0.267 | 0.432 ( | |||||||||
| SP100 vs. PBSP | 0.128 | ||||||||||||
| MT | SP50 vs. SP100 | 1.032 (0.370 to 1.655) | |||||||||||
| SP50 vs. PBSP | 8.584 | 0.014 | 0.133 | 0.559 ( | |||||||||
| SP100 vs. PBSP | 0.154 | ||||||||||||
| PM | SP50 vs. SP100 | 0.523 ( | |||||||||||
| SP50 vs. PBSP | 5.613 | 0.060 |
| 0.415 ( | |||||||||
| SP100 vs. PBSP | |||||||||||||
| S Ant | SP50 vs. SP100 | 0.617 ( | |||||||||||
| SP50 vs. PBSP | 4.053 | 0.132 |
| 0.083 ( | |||||||||
| SP100 vs. PBSP | |||||||||||||
| EO | SP50 vs. SP100 | 1.175 (0.499 to 1.806) | |||||||||||
| SP50 vs. PBSP | 18.907 | 1.360 (0.665 to 2.003) | |||||||||||
| SP100 vs. PBSP | 0.145 | 0.813 (0.169 to 1.426) | |||||||||||
| RA | SP50 vs. SP100 | 1.231 (0.5SP50 to 1.866) | |||||||||||
| SP50 vs. PBSP | 23.259 | 1.313 (0.624 to 1.953) | |||||||||||
| SP100 vs. PBSP | 0.193 | 0.732 (0.094 to 1.343) | |||||||||||
| IO | SP50 vs. SP100 | 0.038 | 0.911 (0.259 to 1.528) | ||||||||||
| SP50 vs. PBSP | 23.584 | 1.526 (0.813 to 2.181) | |||||||||||
| SP100 vs. PBSP | 1.104 (0.436 to 1.731) | ||||||||||||
| MF | SP50 vs. SP100 | 1.063 (0.398 to 1.688) | |||||||||||
| SP50 vs. PBSP | 17.916 | 0.150 | |||||||||||
| SP100 vs. PBSP |
2.8Statistical analyses
Statistical analyses were carried out using IBM SPSS (version 27.0; IBM Corp., Armonk, NY, USA). The Shapiro-Wilk test was performed to determine normality. Depending on the normality of the distribution, the unpaired
Table 3
The results of statistical analysis for shoulder press – downward
|
|
|
|
| ||||||||||
| UT | SP50 vs. SP100 | 0.723 (0.086 to 1.333) | |||||||||||
| SP50 vs. PBSP | 4.886 | 0.087 |
| 0.455 ( | |||||||||
| SP100 vs. PBSP | |||||||||||||
| LT | SP50 vs. SP100 | 0.951 (0.296 to 1.570) | |||||||||||
| SP50 vs. PBSP | 11.505 | 0.003 | 0.975 (0.318 to 1.595) | ||||||||||
| SP100 vs. PBSP | 0.910 | 0.034 ( | |||||||||||
| Lat | SP50 vs. SP100 | 0.933 (0.280 to 1.552) | |||||||||||
| SP50 vs. PBSP | 17.060 | 1.241 (0.559 to 1.876) | |||||||||||
| SP100 vs. PBSP | 0.270 | 0.359 ( | |||||||||||
| MT | SP50 vs. SP100 | 1.089 (0.422 to 1.715) | |||||||||||
| SP50 vs. PBSP | 12.814 | 0.002 | 0.959 (0.304 to 1.579) | ||||||||||
| SP100 vs. PBSP | 0.350 | ||||||||||||
| PM | SP50 vs. SP100 | 0.047 | 0.474 ( | ||||||||||
| SP50 vs. PBSP | 11.784 | 0.003 | 0.926 (0.273 to 1.543) | ||||||||||
| SP100 vs. PBSP | 0.152 | 0.407 ( | |||||||||||
| S Ant | SP50 vs. SP100 | 0.758 (0.118 to 1.369) | |||||||||||
| SP50 vs. PBSP | 5.354 | 0.069 |
| 0.212 ( | |||||||||
| SP100 vs. PBSP | |||||||||||||
| EO | SP50 vs. SP100 | 0.983 (0.326 to 1.604) | |||||||||||
| SP50 vs. PBSP | 25.885 | 1.454 (0.749 to 2.104) | |||||||||||
| SP100 vs. PBSP | 0.046 | 0.944 (0.290 to 1.562) | |||||||||||
| RA | SP50 vs. SP100 | 1.014 (0.354 to 1.636) | |||||||||||
| SP50 vs. PBSP | 31.210 | 1.654 (0.925 to 2.320) | |||||||||||
| SP100 vs. PBSP | 1.188 (0.511 to 1.819) | ||||||||||||
| IO | SP50 vs. SP100 | 0.102 | 0.773 (0.132 to 1.384) | ||||||||||
| SP50 vs. PBSP | 27.242 | 1.428 (0.726 to 2.076) | |||||||||||
| SP100 vs. PBSP | 1.184 (0.508 to 1.816) | ||||||||||||
| MF | SP50 vs. SP100 | 1.211 (0.532 to 1.845) | |||||||||||
| SP50 vs. PBSP | 11.755 | 0.003 | 0.205 | 0.520 ( | |||||||||
| SP100 vs. PBSP | 0.034 |
PBSP paper balloon shoulder press; SP50, shoulder press 50%; SP100, shoulder press 100%. UT, upper trapezius; LT, lower trapezius; Lat, latissimus dorsi; MT, medial head of the triceps brachii; PM, clavicular part of the pectoralis major; S Ant, serratus anterior; EO, external oblique; RA, rectus abdominis; IO, internal oblique; MF, multifidus.
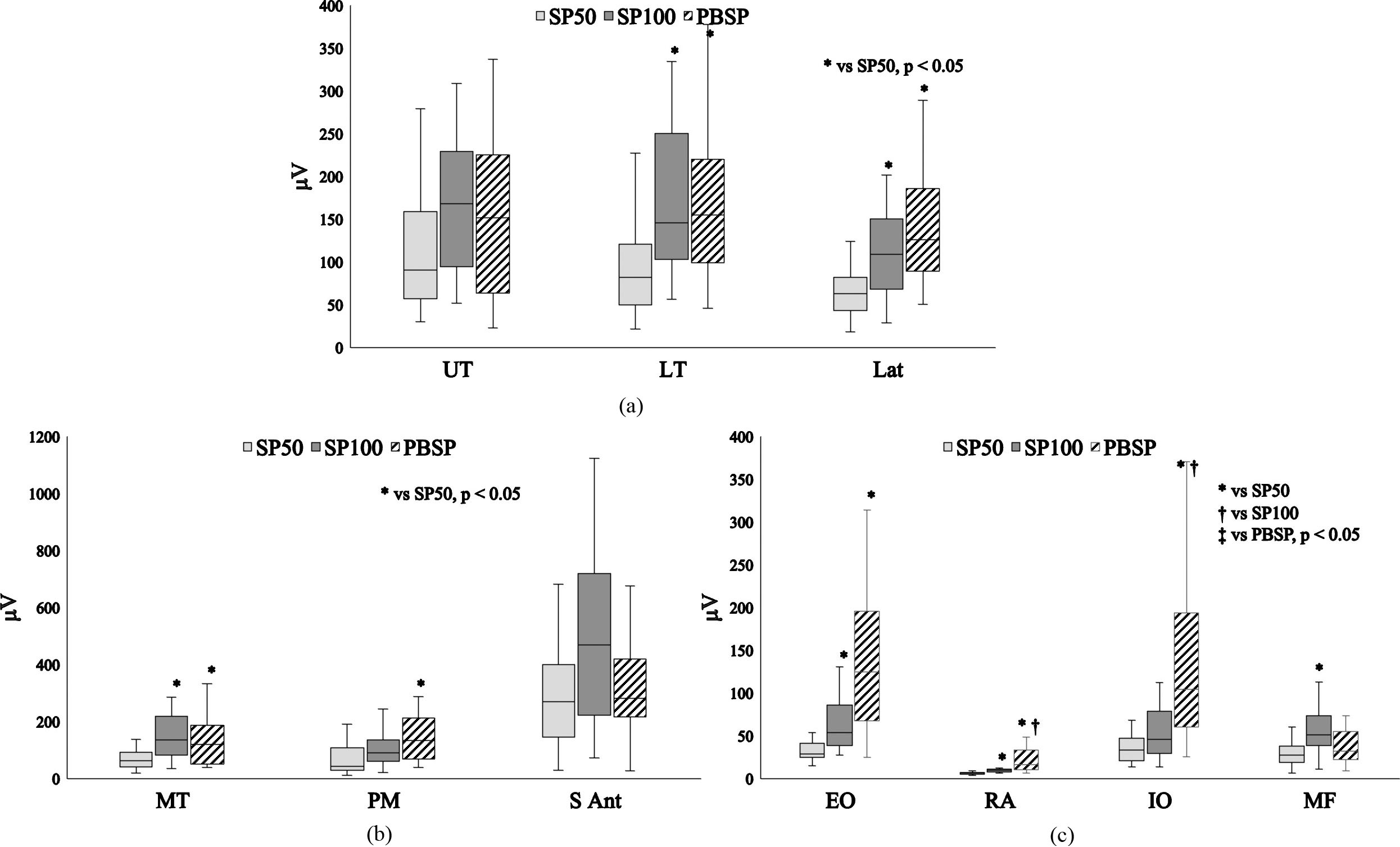
Figure 6.
a. Differences in muscle activity between exercise tasks in the scapulothoracic muscles shoulder press downward. PBSP paper balloon shoulder press; SP50, shoulder press 50%; SP100, shoulder press 100%; UT, upper trapezius; LT, lower trapezius; Lat, latissimus dorsi. b. Differences in muscle activity between exercise tasks in the scapulohumeral muscles shoulder press downward. PBSP paper balloon shoulder press; SP50, shoulder press 50%; SP100, shoulder press 100%; MT, medial head of the triceps brachii; PM, clavicular part of the pectoralis major; S Ant, serratus anterior. c. Differences in muscle activity between exercise tasks in trunk muscles shoulder press downward. PBSP paper balloon shoulder press; SP50, shoulder press 50%; SP100, shoulder press 100%; EO, external oblique; RA, rectus abdominis; IO, internal oblique; MF, multifidus.
3.Results
Significant differences in muscles activities were noted between exercises with and without the external-focus instruction using paper balloon. The medians value, and interquartile ranges of muscle activity of each exercise and the statistical analysis results are shown in Figs 4–6 and Tables 1–3. The front planks are shown in Fig. 4 and Table 1, and the shoulder presses are shown in Figs 5 and 6 and Table 2. Based on the work of Harrison et al. [23] the effect size and its 95% confidence interval were considered “beneficial” in terms of tasks and sides as follows. For the front plank (static task), the activation of the UT, LT, Lat, MT, PM, EO, IO, and MF was significantly higher in PBFP than in FP. On the other hand, for the shoulder press (dynamic task), in the upwards direction (concentric), the activation of the IO was significantly higher in PBSP than in SP50 and SP100. The activation of the EO and RA in PBSP was significantly higher than SP50. The activation of the MT, EO, RA, and MF in SP100 was significantly higher than SP50. MF had a significantly lower activation in PBSP than SP100. In the downward direction (eccentric), the activation of the RA and IO was significantly higher in PBSP than in SP50 and SP100. The activation of the LT, Lat, MT, PM, and EO in PBSP was significantly higher than SP50. Finally, the activation of the LT, Lat, MT, EO, RA, and MF in SP100 was significantly higher than SP50.
4.Discussion
The main finding of this study indicates that adding external-focus instruction using a paper balloon during both front plank and shoulder press lead to a change in muscle activation. Specifically, the performance of the two exercises was associated with differences in muscle activation for both the static and dynamic tasks, with or without using the paper balloon method.
In a previous study, Murofushi et al. investigated an externally focused instruction while exerting control to avoid crushing an item, such as a paper balloon, while maintaining a static position during a chest squeeze exercise [13]. This method significantly activated the LT without involving any complicated movement. Furthermore, agonist and antagonist muscle co-contractions were found in the LT and UT, Lat, and PM.
In this study, isometric exercise with an external-focus instruction was performed using a paper balloon while exerting control to not crush the item in the front plank (static task) and shoulder press (dynamic task) exercises. In the field of sport, exercise, or rehabilitation, efforts are made to efficiently apply resistance to the body in order to produce a training effect. There are several ways to activate the trunk muscles including breathing, changing posture, or using an unstable surface [7, 24]. In this study, the front plank (static task), using an external-focus with the cognitive task paper balloon method, has activated trunk muscles effectively. Furthermore, in the shoulder press (dynamic task) exercise, despite the moving of arms upward and downward, keeping external-focus with paper balloon and trying to not crush it, also effectively activated the trunk muscles. Generally, muscle contraction signals are directly proportional to force rate [25, 26]. However, with the external focused paper balloon method, the muscle is activated with no force production, but similar or increased contraction for the LT, Lat, MT, PM, RA, EO, and IO in the shoulder press of this study. If a muscle can be activated efficiently without force production, namely there is no resistive force from pushing the paper balloon, then less force can be applied to the joint. Therefore, it is possible to reduce the stress on the joints during exercise. Repletion, we speculate that from a clinical point of view, using external-focus with its own cognitive task namely, not crushing the object, can benefit various individuals of different ages, athletes, or rehabilitation. The next step should be an intervention study for this method, to determine whether it can increase muscle mass or enhance strength. Further, since this is a high order cognitive task, future studies should investigate the association of brain activation using methods like fMRI.
This study had several limitations. First, we only examined the participants in a single position while exerting maximum effort for the FP and only during a seated position for the shoulder press exercise. However, different body positions may lead to different muscle activation results. Second, we did not normalize the EMG signals because data were collected/compared for the same participant during the same period within a short period [27]. Third, the EMG variations in the two exercises were examined in two different groups of participants and thus did not allow between-exercise analysis. These factors should be assessed and investigated in future studies.
5.Conclusion
Adding the external-focus using the paper balloon to the front plank significantly activated 8 out of the 10 muscles. In the downward shoulder press, 5 out of 10 muscles with 50% 1 RM, 2 out of 10 muscles with 100% 1 RM were significantly activated. Trunk strengthening can occur during both exercise (static) and limb (dynamic) tasks; therefore, adding this external-focus instruction method during these exercises may improve trunk stability.
Author contributions
CONCEPTION: Koji Murofushi.
PERFORMANCE OF WORK: Koji Murofushi, Tomoki Oshikawa, Hiroshi Akuzawa, Kenji Hirohata and Daisuke Yamaguchi.
INTERPRETATION OR ANALYSIS OF DATA: Koji Murofushi, Tomoki Oshikawa, Hidetaka Furuya and Sho Mitomo.
PREPARATION OF THE MANUSCRIPT: Koji Murofushi, Tomoki Oshikawa, Hiroshi Akuzawa, Kenji Hirohata, Daisuke Yamaguchi and Sho Mitomo.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Koji Murofushi, Tomoki Oshikawa, Hiroshi Akuzawa, Kenji Hirohata and Sho Mitomo.
SUPERVISION: Koji Murofushi, Koji Kaneoka, Kazuyoshi Yagishita and Hidetaka Furuya.
Ethical considerations
All participants provided written informed consent for participation in this study prior to beginning the trials. This study was approved by the research ethics committee (approval number: M2019-295, dated March 4, 2020) of the participating institution and pursuant to the principles of the Declaration of Helsinki (52nd World Medical Association General Assembly, Edinburgh, Scotland, October 2000) for medical research involving human subjects.
Funding
This study did not receive funding.
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors confirm no conflict of interest with any financial organization regarding the material discussed in the manuscript.
References
[1] | Butcher SJ, Craven BR, Chilibeck PD, Spink KS, Grona SL, Sprigings EJ. The effect of trunk stability training on vertical takeoff velocity. J Orthop Sports Phys Ther. (2007) ; 37: (5): 223-31. doi: 10.2519/jospt.2007.2331. |
[2] | Hides JA, Stanton WR, McMahon S, Sims K, Richardson CA. Effect of stabilization training on multifidus muscle cross-sectional area among young elite cricketers with low back pain. J Orthop Sports Phys Ther. (2008) ; 38: (3): 101-8. doi: 10.2519/jospt.2008.2658. |
[3] | Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. (2007) ; 37: (12): 754-62. doi: 10.2519/jospt.2007.2471. |
[4] | Juker D, McGill S, Kropf P, Steffen T. Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during a wide variety of tasks. Med Sci Sports Exerc. (1998) ; 30: (2): 301-10. doi: 10.1097/00005768-199802000-00020. |
[5] | Youdas JW, Coleman KC, Holstad EE, Long SD, Veldkamp NL, Hollman JH. Magnitudes of muscle activation of spine stabilizers in healthy adults during prone on elbow planking exercises with and without a fitness ball. Physiother Theory Pract. (2018) ; 34: (3): 212-22. doi: 10.1080/09593985.2017.1377792. |
[6] | Calatayud J, Casaña J, Martín F, Jakobsen MD, Colado JC, Andersen LL. Progression of core stability exercises based on the extent of muscle activity. Am J Phys Med Rehabil. (2017) ; 96: (10): 694-9. doi: 10.1097/PHM.0000000000000713. |
[7] | Imai A, Kaneoka K, Okubo Y, Shiina I, Tatsumura M, Izumi S, et al. Trunk muscle activity during lumbar stabilization exercises on both a stable and unstable surface. J Orthop Sports Phys Ther. (2010) ; 40: (6): 369-75. doi: 10.2519/jospt.2010.3211. |
[8] | Okubo Y, Kaneoka K, Imai A, Shiina I, Tatsumura M, Izumi S, et al. Electromyographic analysis of transversus abdominis and lumbar multifidus using wire electrodes during lumbar stabilization exercises. J Orthop Sports Phys Ther. (2010) ; 40: (11): 743-50. doi: 10.2519/jospt.2010.3192. |
[9] | Dicus JR, Holmstrup ME, Shuler KT, Rice TT, Raybuck SD, Siddons CA. Stability of resistance training implement alters emg activity during the overhead press. Int J Exerc Sci. (2018) ; 11: (1): 708-716. PMID: 29997723; PMCID: PMC6033506. |
[10] | Williams MR Jr., Hendricks DS, Dannen MJ, Arnold AM, Lawrence MA. Activity of shoulder stabilizers and prime movers during an unstable overhead press. J Strength Cond Res. (2020) ; 34: (1): 73-78. doi: 10.1519/JSC.00000000000026 60. PMID: 29889776. |
[11] | Luczak J, Bosak A, Riemann BL. Shoulder muscle activation of novice and resistance trained women during variations of dumbbell press exercises. J Sports Med (Hindawi Publ Corp). (2013) ; 2013: : 612650. doi: 10.1155/2013/612650. Epub 2013 May 15. PMID: 26464884; PMCID: PMC4590897. |
[12] | Behm DG, Leonard AM, Young WB, Bonsey WA, MacKinnon SN. Trunk muscle electromyographic activity with unstable and unilateral exercises. J Strength Cond Res. (2005) ; 19: (1): 193-201. doi: 10.1519/1533-4287(2005)19<193:TMEAWU>2.0.CO;2. PMID: 15705034. |
[13] | Murofushi K, Yamaguchi D, Hirohata K, Furuya H, Mitomo S. Variations in upper limb and trunk muscles activation during isometric exercise with or without exertion of control. Isokinet Exert Sci. (2022) ; 1-2. doi: 10.3233/IES-210215. |
[14] | Fukumori KI. Kamifusen, the self-inflating Japanese paper balloon. Phys Today. (2017) ; 70: (1): 78-9. doi: 10.1063/PT.3.3437. |
[15] | Aguilera-Castells J, Buscà B, Morales J, Solana-Tramunt M, Fort-Vanmeerhaeghe A, Rey-Abella F, et al. Muscle activity of Bulgarian squat. Effects of additional vibration, suspension and unstable surface. PLoS One. (2019) ; 14: ; e0221710. doi: 10.1371/journal.pone.0221710. |
[16] | Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. (2007) ; 37: (12): 754-62. doi: 10.2519/jospt.2007.2471. |
[17] | Ekstrom RA, Donatelli RA, Soderberg GL. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. (2003) ; 33: (5): 247-58. doi: 10.2519/jospt.2003.33.5.247. |
[18] | Surface Electromyography for the Non-Invasive Assessment of Muscles: Recommendations for sEMG Sensors, Sensor Placement and Location. [homepage on the Internet] Available from: http://wwwseniam.org. |
[19] | Cram JR, Kasman GS. Introduction to surface electromyography. Gaithersburg, MD: Aspen Publishers Inc.; (1998) . |
[20] | Ekstrom RA, Bifulco KM, Lopau CJ, Andersen CF, Gough JR. Comparing the function of the upper and lower parts of the serratus anterior muscle using surface electromyography. J Orthop Sports Phys Ther. (2004) ; 34: (5): 235-43. doi: 10.2519/jospt.2004.34.5.235. |
[21] | McCurdy K, O’Kelley E, Kutz M, Langford G, Ernest J, Torres M. Comparison of lower extremity EMG between the 2-leg squat and modified single-leg squat in female athletes. J Sport Rehabil. (2010) ; 19: (1): 57-70. doi: 10.1123/jsr.19.1.57. |
[22] | Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York (NY): Lawrence Eribaum Associates; (1988) . |
[23] | Harrison AJ, McErlain-Naylor SA, Bradshaw EJ, Dai B, Nunome H, Hughes GT, et al. Recommendations for statistical analysis involving null hypothesis significance testing. Sports Biomech. (2020) ; 19: (5): 561-8. doi: 10.1080/14763141.2020.. |
[24] | Baritello O, Stoll J, Martinez-Valdes E, Müller S, Mayer F, Müller J. Neuromuscular activity of trunk muscles during side plank exercise and an additional motoric-task perturbation. Dtsch Z Sportmed. (2019) ; 70: : 153-8. doi: 10.5960/dzsm.2019.382. |
[25] | De Luca CJ, LeFever RS, McCue MP, Xenakis AP. Behaviour of human motor units in different muscles during linearly varying contractions. J Physiol. (1982) ; 329: : 113-28. doi: 10.1113/jphysiol.1982.sp014293. PMID: 7143246; PMCID: PMC1224770. |
[26] | Lenhardt SA, McIntosh KC, Gabriel DA. The surface EMG-force relationship during isometric dorsiflexion in males and females. Electromyogr Clin Neurophysiol. (2009) ; 49: (5): 227-34. PMID: 19694210. |
[27] | Halaki M, Ginn K. Normalization of EMG signals: to normalize or not to normalize and what to normalize to. In: Naik GR, editor. Computational intelligence in electromyography analysis – A perspective on current applications and future challenges. Rijeka: InTech Open; (2012) ; pp. 175-94. doi: 10.5772/49957. |


