
Improving nutritional assessment in acute medical admissions at a district general hospital
Abstract
BACKGROUND:
Malnutrition adversely affects clinical outcomes, necessitating a prompt and accurate assessment of nutritional status on admission. A variety of tools exist to aid nutritional assessment, of which the malnutrition universal screening tool (MUST) is recommended, but remains difficult to implement in practice.
OBJECTIVE:
The aim of this audit was to improve the utilisation of the malnutrition universal screening tool (MUST) in the Acute Medical Unit (AMU) at Queen Elizabeth Hospital, King’s Lynn. Specifically, patients should have a completed and accurate MUST score within 6 hours of arrival to AMU and high-risk patients (MUST score ≥2) should be referred to dieticians within 48 hours of admission. The first cycle was conducted by March 2019 and the second cycle was completed 1 year later to allow assessment of interventions actioned after the first cycle.
METHODS:
We conducted a two-cycle audit evaluating the MUST completion and dietician referral rate of high-risk patients (defined as MUST ≥2) on the Acute Medical Unit in a district general hospital, with the standards of 80% and 100% respectively. A questionnaire was distributed after the first cycle exploring nurses’ current experience and competence in using MUST.
RESULTS:
In the first cycle, MUST scores were calculated correctly in 111/150 patients (74%) and 1/9 (11%) high-risk patients were referred to dieticians. After interventions, MUST scores were calculated correctly in 77/101 patients (76%) and 2/4 high-risk patients (50%) were referred to dieticians. The nurses (n = 19) who took part in the questionnaire felt confident in MUST completion, but the average score in an objective assessment was 67%.
CONCLUSIONS:
As per the literature, the first cycle demonstrated the under-utilisation of MUST in clinical practice. In response, we proposed additional face-to-face training for existing staff, the inclusion of an e-learning module within the staff’s induction, and provision of ward MUST ‘troubleshooting’ booklets. MUST utilisation rates improved upon re-auditing, but not to target standards. We will need to consider potential barriers to sustainable change and implement interventions such as identification of nursing champions to overcome them.
1.Background
Across the UK, approximately 3 million people are at risk of malnutrition, 93% of which live in the community [1]. Hence, prompt and accurate assessments of a patient’s nutritional status upon admission is an essential component of hospital patient care [2,3], with malnourished patients at risk of adverse outcomes such as healthcare-associated infections [4] or poor wound healing [5]. Several scoring tools exist to assess nutritional status upon admission to hospital, of which MUST is recommended by the British Association for Parenteral and Enteral Nutrition (BAPEN) and the European Society for Clinical Nutrition and Metabolism [2,5].
In clinical practice, the implementation of MUST in assessing the risk of malnutrition can be challenging. The varying levels of education and training in using the tool, competing priorities in a time-pressured environment and a preference for individual judgement have been cited in the literature as barriers to the effective clinical implementation of MUST [6–8].
Therefore, we conducted a prospective audit evaluating the completion rate of MUST scores at patient admission, and the subsequent referral rate of high-risk patients to the hospital dieticians. As nurses frequently carry out MUST assessments as part of their clerking pro forma, we designed a questionnaire exploring nurses’ views, subjective confidence and objective competence in using the tool.
2.Methods
At a designated time-point, the nursing files of all AMU patients were examined, and the following data were collected: patient bed number, patient arrival date and time (as stated on the admission booklet), data collection date and time, whether MUST assessment was completed and the reported MUST score.
Patients were excluded if their length of stay (LOS) in AMU was >10 days. If the patient was admitted <6 hours ago at the point of data collection and the MUST score was not completed, the file was re-examined after the patient had been admitted for at least 6 hours. The on-call dietician was contacted to determine if patients with a MUST ≥2 had been referred to their services and the length of time between AMU admission and referral.
The standards for the MUST completion and dietician referral rates were drawn from NICE clinical guideline 32 [3] and the MUST report [5]. The target standard for dietician referral was chosen to be 100%. A target standard of 80% was chosen for MUST completion since we recognised that accurate weight measurement may not always be possible in acutely ill patients.
Following the first audit cycle, a questionnaire, designed to assess nursing staff perceptions and competence in using MUST, was disseminated to AMU nurses. The questionnaire included a free-text section to inform about current nursing training in malnutrition and suggestions for improvement. Participation was voluntary.
Several interventions were implemented based on the response from the questionnaire expressing a desire for on-the-job training and e-learning modules. We placed several copies of the MUST toolkit booklet in AMU to assist MUST calculation and increase awareness for dietician referral. Additionally, the NICE approved e-learning module on MUST calculation was distributed to AMU nursing staff.
3.Results
Cycle one of data collection took place in May 2019 on 3 separate occasions across 2 weeks. Cycle two of data collection post-intervention took place in March 2020 on 2 separate occasions across 2 weeks. It was prematurely terminated due to the COVID-19 pandemic.
In the first cycle, 152 patient charts were examined with 2 patients being excluded due to a LOS >10 days, resulting in 150 patients being included in the data analysis (Fig. 2). Of these, 9 patients were identified as being high-risk with a MUST score ≥2. The MUST completion rate was 74% (111/150). Only one in nine (11.1%) high-risk patients were referred to the dieticians as per the MUST guidelines [9].
Nineteen questionnaires were returned fully completed (Fig. 1). Overall, the nurses felt that MUST was easy to use and were confident in using it, taking <5 min or 5–10 min to complete. Just over half of nurses reported receiving prior training, including mandatory trust training sessions, training during university or on the ward learning. On the job training and e-learning modules were the most popular forms of additional training modalities requested. When competence was assessed objectively using 5 case-based multiple-choice questions, the mean score was 67%.
Fig. 1.
Questionnaire results outlining nurses’ experiences, confidence and competence in using the Malnutrition Universal Screening Tool (MUST) (n = 19).
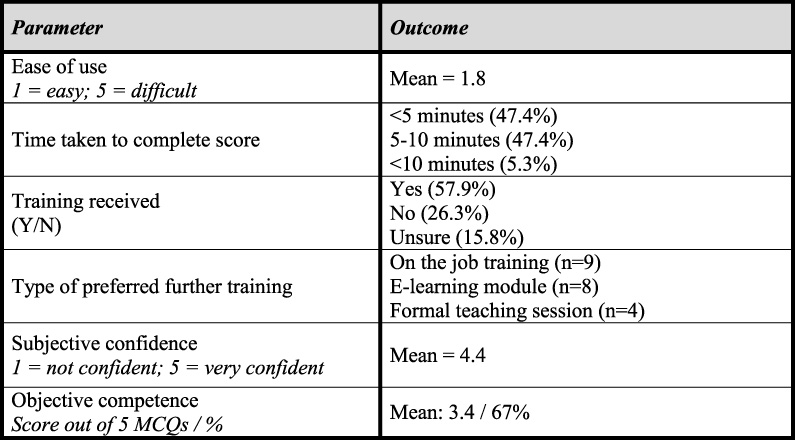
Fig. 2.
Table summarising Malnutrition Universal Screening Tool (MUST) completion and dietician referral rates across both audit cycles.
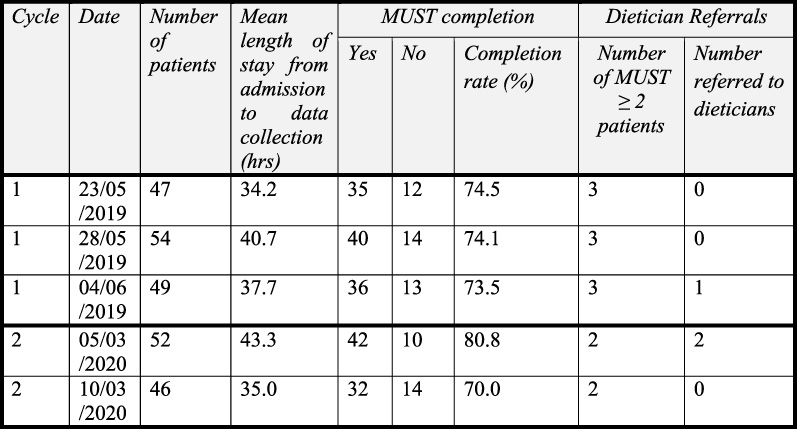
In the second cycle, 101 patient notes were examined (Fig. 2). 3 patients were excluded due to a LOS >10 days. Of the 98 patients included in this cycle, 4 patients were identified as being high-risk with a MUST score ≥2. The MUST completion score was 75.5% (74/98) and 50% (2/4) of the high-risk patients were referred to the dieticians.
4.Discussion
Despite wide usage, the MUST score remains difficult to implement effectively in clinical practice. The results from the first cycle reflect this difficulty, with a MUST completion (74%) and dietician referral rate (11.1%) of high-risk patients below the target standards of 80% and 100% respectively.
There were several potential barriers identified preventing the completion of MUST scores accurately. This included significant gaps of knowledge and insufficient formal training in using the MUST scores from the nursing staff, alongside environmental factors such as a busy ward environment. These factors, in particular the gaps of knowledge, have been identified in previous literature and studies done on improving MUST implementation [6–8].
After the first cycle, we implemented several interventions targeting the gaps of knowledge, including MUST toolkit booklets to facilitate MUST calculation and increase awareness for dietician referral, and the introduction of the NICE approved e-learning module on malnutrition. Following these interventions, the MUST completion rate increased to 75.5% but remained below the target standard of 80%. The referral rate of high-risk patients to dieticians improved to 50%.
Whilst these results demonstrated an improvement, they were still below our original targets. As these interventions were predominantly educationally focused, significant long-term improvements will likely only be seen with sustained implementation. This would have been especially challenging during the COVID-19 pandemic, with ward changes and high staff turnover.
Further work and cycles should focus on sustaining and improving the educational measures implemented in the first cycle. This may include finding ways to better deliver the teaching content or identifying nursing champions that could promote the usage of MUST in the ward. Additional work should also look at mitigating the busy ward environment through increasing the ease of completing MUST and method of referring high-risk patients. This could involve modifications to the MUST booklet or streamlining the dietitian referral pathway.
5.Conclusion
The full implementation of MUST in clinical environments with competing priorities for nurses remains a challenge. Through the use of a questionnaire, we identified a knowledge gap that was targeted with educational materials which resulted in improvements in MUST completion rates. Future work will need to look into mitigating environmental factors to facilitate increased completion rates.
Acknowledgements
The authors thank Dr Fatima Ilham for conducting data collection cycle two. They are grateful to Gail Morris Senior Sister for coordinating the implementation of interventions and clinical support.
Conflict of interest
The authors disclose no conflicts of interest.
References
[1] | Russell CA, Elia M. Nutrition Screening Survey in the Uk and Republic of Ireland in 2010 [Internet]. British Association for Parenteral and Enteral Nutrition (BAPEN); (2012) . |
[2] | Cederholm T, Barazzoni R, Austin P, Ballmer P, Biolo G, Bischoff SC ESPEN guidelines on definitions and terminology of clinical nutrition. Clin Nutr. (2017) ;36: (1):49–64. doi:10.1016/j.clnu.2016.09.004. |
[3] | National Institute for Health and Care Excellence (NICE). Nutrition Support for Adults Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition [CG32] [Internet]. 2017 [cited 2019 Apr 1]. Available from: https://www.nice.org.uk/guidance/cg32. |
[4] | Fitzpatrick F, Skally M, O’Hanlon C, Foley M, Houlihan J, Gaughan L Food for thought. Malnutrition risk associated with increased risk of healthcare-associated infection. J Hosp Infect [Internet]. (2019) ;101: (3):300–304. doi:10.1016/j.jhin.2018.12.012. |
[5] | Elia M , The MUST Report—Nutritional Screening of Adults: A Multidisciplinary Responsibility [Internet]. MAG, a Standing Committee of BAPEN. 2003 [cited 2019 Apr 3]. Available from: https://www.bapen.org.uk/pdfs/must/must-report.pdf. |
[6] | Smith A. Potential barriers to effective MUST implementation. Br J Community Nurs. (2014) ;19: (Supp 11):S28–31. doi:10.12968/bjcn.2014.19.sup11.s28. |
[7] | Cooper PL, Raja R, Golder J, Stewart AJ, Shaikh RF, Apostolides M Implementation of nutrition risk screening using the Malnutrition Universal Screening Tool across a large metropolitan health service. J Hum Nutr Diet. (2016) ;29: (6):697–703. doi:10.1111/jhn.12370. |
[8] | Frank M, Sivagnanaratnam A, Bernstein J. Nutritional assessment in elderly care: A MUST! BMJ Qual Improv Reports. (2015) ;4: (1):u204810.w2031. doi:10.1136/bmjquality.u204810.w2031. |
[9] | Malnutrition Advisory Group (MAG). The “MUST” explanatory booklet [Internet]. 2011. Available from: https://www.bapen.org.uk/pdfs/must/must_explan.pdf. |


