
Benefits and harms of antipsychotic drugs in drug-naïve patients with psychosis: A systematic review
Abstract
OBJECTIVE:
To study the benefits and harms of antipsychotics in drug-naïve patients with psychosis.
METHODS:
This study is a systematic review and meta-analysis of placebo-controlled trials. Main outcome measures: Mortality, activities of daily living, quality of life, core psychiatric events, and relapse and recovery rates. Data sources: PubMed, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), two trial registers and references in potentially eligible articles. Data extraction: Two researchers extracted data independently. The outcomes were planned to be meta-analysed using Review Manager based on a fixed effect model.
RESULTS:
Our searches resulted in 493 unique records of which 447 were clearly not eligible. We read the full text of the 46 potentially eligible articles and found one eligible trial in drug-naïve patients, which was unreliable. It was a Chinese trial comparing olanzapine with placebo in 261 patients with first-episode schizophrenia. After 12 weeks, there was an extremely large difference favouring placebo, but the authors reported the opposite, that olanzapine was effective.
CONCLUSIONS:
The use of antipsychotics cannot be justified based on the evidence we currently have. Withdrawal effects in the placebo groups make existing placebo-controlled trials unreliable.
1Introduction
Antipsychotics are standard treatment for psychosis and schizophrenia spectrum disorders. However, although they have been on the market for over 60 years, it is still relevant to ask what their true effect is because the placebo-controlled trials that have led to marketing approval of antipsychotics are biased. There are two main reasons for this; lack of effective blinding and withdrawal effects.
Antipsychotics have conspicuous adverse effects, which makes it difficult to blind the placebo- controlled trials effectively. This is a general problem for trials of psychiatric drugs. It is relatively easy for the investigators to ascertain who got active drug and who got placebo. In one trial of alprazolam, for example, the blinding was broken for all the patients [1]. When the assessment of the outcome is subjective, there is a risk that the effect in trials that have not been effectively blinded is overestimated. In accordance with this, the effect of antidepressant drugs was notably smaller when the trials had been better blinded by adding atropine to the placebo, which gives similar side effects as the active drugs [2].
The lack of effective blinding is also a problem in trials of antipsychotics. In a 1964 trial of 344 newly admitted patients with schizophrenia, investigators funded by US National Institute of Mental Health reported that, compared with placebo, phenotiazines reduced apathy, improved motor movements and made patients less indifferent [3]. This is the opposite of what these drugs do to patients, which the psychiatrists had acknowledged a decade earlier [4].
The other important bias in trials of antipsychotics is related to withdrawal effects in patients randomised to placebo [5]. The trials have included patients who were already on an antipsychotic drug before they were randomised. Even if wash-out periods are used, this leads to withdrawal symptoms in the placebo group, as it may take a long time to recover from drug induced changes in the brain [6–8].
The withdrawal symptoms can be severe. In a Cochrane review of 55 trials (5,506 patients) comparing chlorpromazine with placebo for schizophrenia, the largest trial that had data on akathisia reported significantly less akathisia in the active group than in the placebo group, risk ratio 0.57, 95% CI 0.37 to 0.88 [9]. Considering all the trials together, akathisia did not occur more often in the chlorpromazine group than in the placebo group. Since we know that antipsychotics may cause akathisia - particularly in the withdrawal phase, i.e. in the placebo group [7] - and that a placebo cannot cause akathisia, this Cochrane review illustrates the impact of the withdrawal bias.
Another Cochrane review assessed the effects of antipsychotics in patients with “a majority of first and second episode schizophrenia spectrum disorders” [10]. Although this review was also biased in favour of active drugs because of lack of effective blinding and withdrawal effects, the authors reported that their results did not support a conclusion of antipsychotics being effective for an early episode psychosis. This Cochrane review is now outdated, as it only included trials published until 2007.
Since our knowledge about the benefits and harms of antipsychotics stems from flawed trials, we decided to study their effects in drug-naïve patients. We were particularly interested in objective outcomes such as job adherence, marital status and delinquency, as they would not be expected to be biased because of ineffective blinding.
2Methods
We wished to study the benefits and harms of antipsychotics in patients with psychosis who had not previously been treated with any such drug.
We included randomised trials of any length with a parallel group design that had compared an antipsychotic with a blinded placebo. Participants of all ages, with or without co-morbidities or concomitant treatments were accepted. We included trials of drug-naïve patients with a first- episode psychosis, and also trials in patients with multiple episodes provided they had never been treated with an antipsychotic drug before. Trials of patients in prodromal stages, where no transition to psychosis had occurred at the time of randomisation, were excluded.
2.1Outcomes
The primary outcomes were mortality, activities of daily living (e.g. job adherence, marital status, delinquency), quality of life, core psychiatric events, [11] and relapse and recovery rates. Secondary outcomes were symptom relief on scales related to psychosis or schizophrenia, e.g. the Positive and Negative Syndrome Scale (PANSS), separating clinician-rated and self-rated symptom scores, admissions to hospital, sexual dysfunction, serious adverse events, and cognitive function including dementia.
2.2Data collection, extraction and analysis
We searched PubMed, Embase and the Cochrane Central Register of Controlled Trials (CENTRAL) on 10 October 2016 (see search strategies in Table 1) and updated the search in PubMed on 16 April 2019.
Table 1
Data searches
| There were no language restrictions. |
| PubMed |
| (schizophren* OR schizotyp* OR schizoi*) AND (“early episode” OR “primary episode” OR prodromal OR “first-episode”) limited to Randomized Controlled Trial. |
| Embase |
| (schizophren* or schizotyp* or schizoi*).mp. AND (“early episode” or “primary episode” or prodromal or “first-episode”).mp. limited to Randomized Controlled Trial. |
| Cochrane Library |
| (schizophren* OR schizotyp* OR schizoi*) AND (“early episode” OR “primary episode” OR prodromal OR “first-episode”) in Title, Abstract, Keywords limited to trials. |
| www.clinicaltrials.gov and www.clinicaltrialsregister.eu |
| antipsychotics AND first-episode. |
One observer screened titles and abstracts and consulted with the second observer when in doubt. Both observers read possibly eligible articles in full, assessed eligibility and extracted data independently of each other. One observer reviewed the reference lists of possibly eligible reports for additional eligible reports of trials. Disagreements were resolved by discussion.
All analyses were planned to be intention-to-treat analyses. When patients were missing, we assumed they did not recover. We planned to use Review Manager and to assess the risk of bias according to the Cochrane Handbook for Systematic Reviews of Interventions, adding sponsorship bias, and to grade the quality and certainty of the evidence and the strength of recommendations with the GRADE tool.
For dichotomous data, we planned to report risk ratios; for continuous data, mean differences, or standardised mean differences if different scales had been used; with 95% confidence intervals based on a fixed effect model. Heterogeneity was to be assessed as I-square, and if above 50%, possible reasons would be explored.
3Results
Our searches resulted in 493 unique records of which 447 were clearly not eligible (see flow chart in Fig. 1). We read the full text of the 46 potentially eligible articles. We excluded 45 of these articles: 22 were not trials in drug-naïve patients; 13 were not placebo-controlled trials; 5 were not randomised trials; 2 recruited participants at risk of converting to psychosis; 1 recruited healthy controls; and 2 were reviews. Our updated PubMed search in 2019 identified 34 records, all of which were irrelevant, as they were not about a placebo controlled trial. We found only one eligible randomised, placebo controlled trial in drug-naïve patients [12].
Fig. 1
PRISMA flow chart.
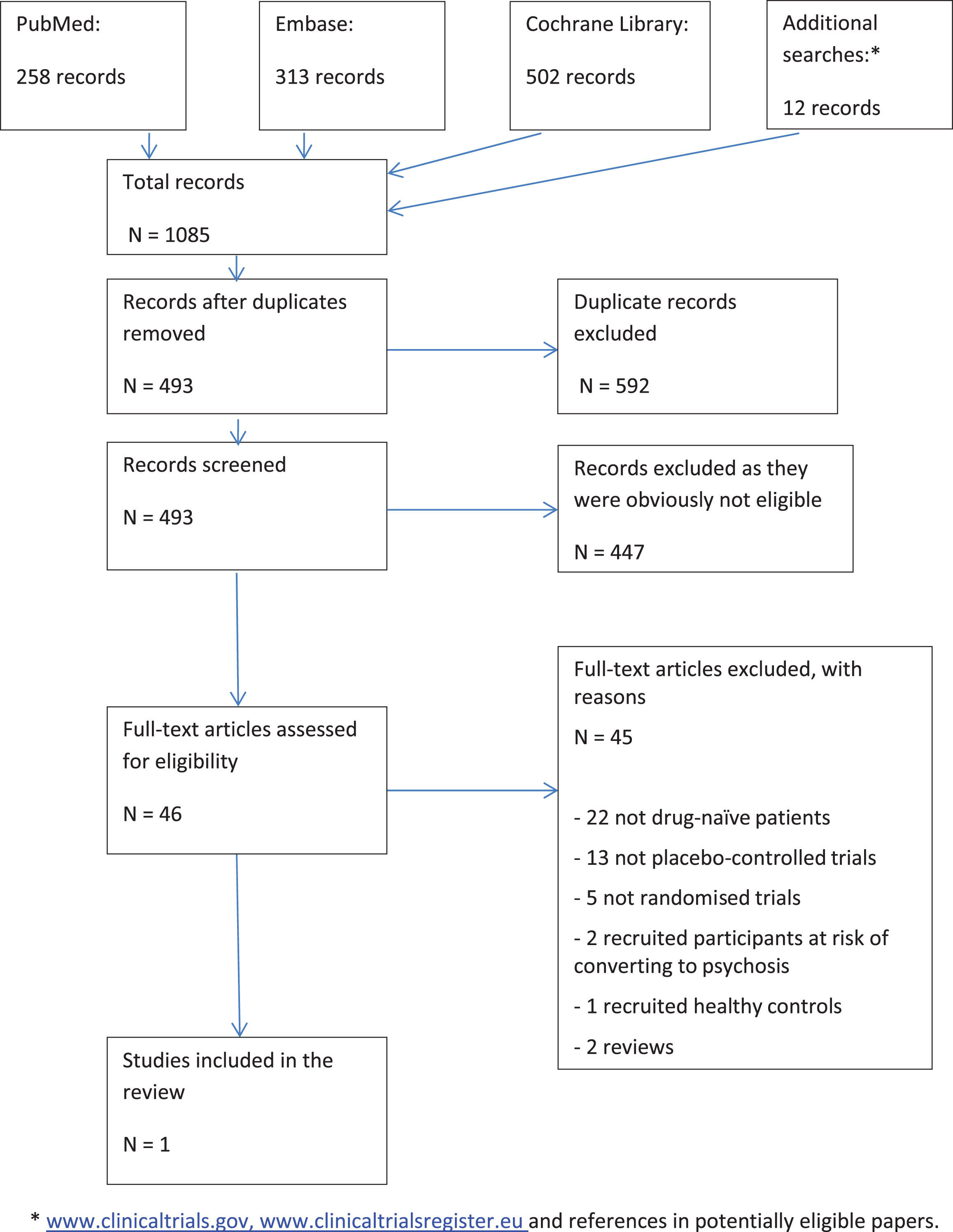
It was a Chinese trial comparing olanzapine with placebo in 129 versus 132 patients with first-episode schizophrenia [12]. The patients were randomised in blocks of two, which involves a high risk of breaking the blinding during the trial and also of breaking the concealment of the allocation. The patients needed to have a total PANSS score of at least 60 to be included in the trial. However, the PANSS score before treatment was only about 9, even though by definition it must be at least 30 (lowest score is 1 and there are 30 items). The score increased to 71.3 (SD 23.7) in the olanzapine group and to 29.4 (17.4) in the placebo group after 12 weeks. The authors reported that olanzapine was effective although patients in the placebo group fared much better according to their paper. We were unable to understand this trial and consider it unreliable. A difference of 42 in PANSS is extremely large, e.g. placebo-controlled trials in submissions to the FDA of newer antipsychotics including olanzapine found a difference of only 6 on the PANSS score favouring active drugs [13].
We describe also the three trials that came closest to being eligible. In the trial from 1964, which we mentioned in the Introduction, 50% of the patients experienced their first psychotic episode [3]. We could not obtain information on the untreated patients separately because the authors had died.
A trial from 1982 compared fluphenazine with placebo for its ability to prevent relapse after a first-episode schizophrenia [14]. According to information we received from the first author, Dr. Kane, the patients were treated and stabilised with antipsychotics before entering the study.
The third trial was published in 2008 [15]. Treatment-naïve patients with a first-episode psychosis as well as prodromal participants at risk of developing psychosis were recruited to one year of treatment with olanzapine or placebo, with a one-year follow-up. However, there were no patients with a first-episode psychosis; all patients were in a prodromal state, which was an exclusion criterion for our review.
Since our searches did not identify any reliable, eligible trials, we supplemented them with searches in www.clinicaltrials.gov and www.clinicaltrialsregister.eu (see Table 1). We found one additional trial that could possibly have been included in our review [16]. It had recruited patients with symptoms for at least seven days, which meant that patients with a first-episode psychotic event could participate. The trial was prematurely ended due to lack of efficacy in March 2009. We requested information about treatment-naïve patients in the trial from six sources: the two trial registers, Pfizer USA, Pfizer Germany, the first author on the published article (Dr. Robert Findling) and the European Medicines Agency. No information was shared with us. We were directed to webpages where the requested information was not listed.
4Discussion
We did not find any reliable placebo-controlled trials of treatment-naïve patients with psychosis or schizophrenia. We therefore agree with the authors of an earlier Cochrane review that the effect of antipsychotics for these conditions has not been documented [10].
We did not include prophylactic studies of people at risk of converting to psychosis but found one such study [17, 18]. However, it was not of treatment-naïve patients, as previous use of antipsychotics was allowed [17]. Seven patients in both groups converted to psychosis [18]. Given that antipsychotics are toxic and do not have a documented effect in psychosis in reliable trials, we believe it is unethical to study their effects for prophylaxis.
More recently approved drugs (new drug applications submitted to the US Food and Drug Administration between 1991 and 2009) [13] have failed to show clinically relevant effects. Based on data from 5,970 patients, it has been shown that the minimal improvement on the Clinical Global Impressions Ratings correspond to about 15 points on the PANSS scale [19]. But as noted above, what was obtained in the placebo-controlled trials was only 6 points [13]. This is noteworthy because it is easy for scores to improve quite a bit if people are tranquillised and express their abnormal ideas less frequently, [20] and because, as explained earlier, all these trials had major flaws in favour of the active drugs.
The so-called maintenance or discontinuation studies, where patients after a period of time on a drug are randomised to continue with the drug or placebo, are also flawed because of withdrawal effects, even when they have a wash-out or taper period before randomisation [5]. Another problem with these studies is that the study period is too short. Antipsychotics cause permanent brain damage in a dose-related fashion, [21] and those brain changes that are reversible may take a long time to recover [7, 8]. In accordance with this, a large meta-analysis of the placebo-controlled discontinuation trials showed that the apparent benefit of continued treatment with antipsychotics on what was considered to be relapse prevention decreased over time and was close to zero after three years [6]. We consider it a misnomer to call such studies relapse prevention studies, as psychoses that occur in patients on placebo might be withdrawal psychoses, i.e. a harmful effect of previous exposure to an antipsychotic drug, rather than genuine psychoses.
Another reason why these studies are flawed is that they are conducted in a select group of “good responders” to the drugs. If all patients were included, and there was long follow-up, the studies might show that the patients, on average, benefitted from coming off the drugs.
We are aware of only one long-term discontinuation study, in 128 patients with schizophrenia, [22, 23]. but even this study was biased in favour of drug treatment. Remitted first-episode patients, i.e. a select group of patients, were randomised to dose reduction or discontinuation, or to maintenance therapy. The discontinuation strategy was carried out by gradual symptom-guided tapering of dosage and discontinuation if feasible. At the two-year follow up, the discontinuation group had a higher “relapse rate” than the maintenance group (43% versus 21%) [22]. However, at the seven-year follow-up, there was no difference (62% versus 69%). Furthermore, the study’s primary outcome was recovery, which is much more important than “relapse” that may be nothing else than a withdrawal psychosis, and more patients had recovered in the dose reduction/discontinuation group than in the maintenance group after seven years (40% versus 18%; P = 0.01) [23].
A randomised placebo-controlled trial of chlorpromazine from 1978 with long-term follow-up provides support for these findings [24]. At the three-year follow-up, when data from 80 of the 127 randomised young men with acute schizophrenic episodes were available, 11 of 41 men (27%) on placebo had been rehospitalised compared to 24 of 39 (62%) of those receiving chlorpromazine (P = 0.003, Fisher’s exact test).
4.1Observational studies
Since the randomised trials are flawed, it can be relevant to look at comparative observational studies. They suggest that the long-term outcome is much better if antipsychotics are avoided [25]. Confounding by indication is an important bias in such studies but the positive results have also been found in studies where the severity of the disease is similar in the compared groups.
An interesting example is an 8-year study the World Health Organization (WHO) launched in 1969 [4, 26]. The patients fared much better in poor countries – India, Nigeria and Colombia – than in the United States and four other developed countries. At five years, about 64% of the patients in the poor countries were asymptomatic and functioning well compared to only 18% in the rich countries. Western psychiatrists dismissed the results arguing that patients in poor countries might have milder disease. The WHO therefore did another study, focusing on first episode schizophrenia diagnosed with the same criteria in ten countries [4, 27]. The results were similar; about two-thirds were fine after two years in the poor countries versus only one third in the rich countries. The WHO investigators tried to explain this huge difference by various psychosocial and cultural factors but didn’t succeed. The most obvious explanation, drug use, went unexplored.
People in poor countries couldn’t afford to buy antipsychotics, so only 16% of patients with schizophrenia were regularly maintained on antipsychotics as compared with 61% in rich countries [25].
The open dialogue family and network approach in Lappland is also interesting. It aims at treating psychotic patients in their homes, and the treatment involves the patient’s social network and starts within 24 hours after contact [28]. The 5-year results in 72 patients are much better than in 71 closely comparable patients in Stockholm [28, 29]. Antipsychotics were used in 33% versus 93% (ongoing use in 17% versus 75%), and after five years, 19% versus 62% were on disability allowance or sick leave.
4.2A paradigm shift is needed
For more than fifty years, the accepted paradigm has been that schizophrenia is a chronic or lifelong brain disorder that should be treated with antipsychotics, often for many years or even lifelong. Psychotherapy and other psychosocial interventions are seen as secondary and adjunctive interventions [30, 31].
However, if psychotic and schizophrenic symptoms are ways of coping with severe distress, [32–34] we would not expect to see a genuine effect of antipsychotics. Furthermore, we would expect to see relapses when the drugs are withdrawn, as the traumas have not been addressed; the patients have merely been sedated and separated from their thoughts and feelings [35]. Such symptoms are part of the rating scales clinicians use to rate improvement. We therefore suggest avoiding using such scales and focus on outcomes that matter to patients and which are less prone to bias. For depression, for example, patients mention quality of relationships, return to normal levels of functioning and quality of life as being important for them [36, 37]. Such outcomes take into account the experiences of the patients and the resolution of their traumatic events.
An additional point to consider for antipsychotic drugs is that they increase mortality. It is difficult to find out by how much because the trials have been biased by withdrawal effects, which include akathisia that is known to increase mortality [5, 7, 25]. People with dementia are less likely to have been treated with antipsychotics before randomisation and a meta-analysis of the newer antipsychotics found that, for every 100 patients treated for a few weeks, there was one additional death on the drug compared to placebo [38]. The FDA, which has access to more accurate data, found that it was two patients of 100 that died [39]. Antipsychotics increase mortality in many ways, e.g. through falls, weight gain, diabetes, cardiac arrhythmias and malignant neuroleptic syndrome.
If a tranquilliser is needed in an acutely disturbed phase, benzodiazepines seem to perform better than antipsychotics [40].
5Conclusions
We believe there is no justification for using antipsychotics in patients with psychosis or schizophrenia spectrum disorders, particular not as long-term treatment. Patients should not be subjected to forced treatment with antipsychotics, as it is impossible to argue that this is in the patient’s own interest.
Contributors
Both authors contributed to the study concept and design, writing of the protocol and manuscript, and to obtaining funding. PCG is the study supervisor and guarantor.
Funding
This study is part of a PhD thesis, funded by the University of Copenhagen. The funding source had no role in the design and conduct of the study; data collection, management, analysis, and interpretation; preparation, review, and approval of the manuscript; or the decision to submit the paper for publication.
Data sharing
Not relevant; all data are in the public domain. The protocol for the review can be obtained from the authors.
Conflict of interest
We have no relevant interests to declare.
References
[1] | Fisher S , Greenberg RG . How sound is the double-blind design for evaluating psychotropic drugs? J Nerv Ment Dis. (1993) ;181: :345–50. |
[2] | Moncrieff J , Wessely S , Hardy R . Active placebos versus antidepressants for depression. Cochrane Database Syst Rev. (2004) ;1: :CD003012. |
[3] | Cole JO . Phenothiazine treatment in acute schizophrenia; effectiveness: The National Institute of Mental Health Psychopharmacology Service Center Collaborative Study Group. Arch Gen Psychiatry. (1964) ;10: :246–61. |
[4] | Whitaker R . Anatomy of an epidemic. New York: Broadway Paperbacks; (2010) . |
[5] | Gøtzsche PC . Deadly psychiatry and organised denial. Copenhagen: People’s Press; (2015) . |
[6] | Leucht S , Tardy M , Komossa K , Heres S , Kissling W , Salanti G , et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: A systematic review and meta-analysis. Lancet. (2012) ;379: :2063–71. |
[7] | Breggin P . Psychiatric drug withdrawal: A guide for prescribers, therapists, patients and their families. New York: Springer Publishing Company; (2012) . |
[8] | Breggin PR . Brain disabling treatments in psychiatry: Drugs, electroshock, and the psychopharmaceutical complex. 2nd ed. New York: Springer Publishing; (2007) . |
[9] | Adams CE , Awad GA , Rathbone J , Thornley B , Soares-Weiser K . Chlorpromazine versus placebo for schizophrenia. Cochrane Database Syst Rev. (2014) ;1: :CD000284. |
[10] | Bola J , Kao D , Soydan H . Antipsychotic medication for early episode schizophrenia. Cochrane Database Syst Rev. (2011) ;6: :CD006374. |
[11] | Maund E , Guski LS , Gøtzsche PC . Considering benefits and harms of duloxetine for treatment of stress urinary incontinence: A meta-analysis of clinical study reports. CMAJ. (2017) ;189: :E194–203. |
[12] | Wang C-H , Li Y , Yang J , Su L-S , Geng Y-G , Li H , et al. A randomized controlled trial of olanzapine improving memory deficits in Han Chinese patients with first-episode schizophrenia. Schizophr Res. (2013) ;144: :129–35. |
[13] | Khin NA , Chen YF , Yang Y , Yang P , Laughren TP . Exploratory analyses of efficacy data from schizophrenia trials in support of new drug applications submitted to the US Food and Drug Administration. J Clin Psychiatry. (2012) ;73: :856–64. |
[14] | Kane JM , Rifkin A , Quitkin F , Nayak D , Ramos-Lorenzi J . Fluphenazine vs placebo in patients with remitted, acute first-episode schizophrenia. Arch Gen Psychiatry. (1982) ;39: :70–3. |
[15] | Hawkins KA , Keefe RSE , Christensen BK , Addington J , Woods SW , Callahan J , et al. Neuropsychological course in the prodrome and first episode of psychosis: Findings from the PRIME North America Double Blind Treatment Study. Schizophr Res. (2008) ;105: :1–9. |
[16] | Findling RL , Cavus I , Pappadopulos E , Vanderburg DG , Schwartz JH , Gundapaneni BK , et al. Ziprasidone in adolescents with schizophrenia: Results from a placebo-controlled efficacy and long-term open-extension study. J Child Adolesc Psychopharmacol. (2013) ;23: :531–44. |
[17] | Phillips LJ , Nelson B , Yuen HP , Francey SM , Simmons M , Stanford C , et al. Randomized controlled trial of interventions for young people at ultra-high risk of psychosis: Study design and baseline characteristics. Aust N Z J Psychiatry. (2009) ;43: :818–29. |
[18] | McGorry PD , Nelson B , Phillips LJ , Yuen HP , Francey SM , Thampi A , et al. Randomized controlled trial of interventions for young people at ultra-high risk of psychosis: Twelve-month outcome. J Clin Psychiatry. (2013) ;74: :349–56. |
[19] | Leucht S , Kane JM , Etschel E , Kissling W , Hamann J , Engel RR . Linking the PANSS, BPRS, and CGI: Clinical implications. Neuropsychopharmacology. (2006) ;31: :2318–25. |
[20] | Moncrieff J . The bitterest pills. Basingstoke: Palgrave Macmillan; (2013) . |
[21] | Ho BC , Andreasen NC , Ziebell S , Pierson R , Magnotta V . Long-term antipsychotic treatment and brain volumes: A longitudinal study of first-episode schizophrenia. Arch Gen Psychiatry. (2011) ;68: :128–37. |
[22] | Wunderink L , Nienhuis FJ , Sytema S , Slooff CJ , Knegtering R , Wiersma D . Guided discontinuation versus maintenance treatment in remitted first-episode psychosis: Relapse rates and functional outcome. J Clin Psychiatry. (2007) ;68: :654–61. |
[23] | Wunderink L , Nieboer RM , Wiersma D , Sytema S , Nienhuis FJ . Recovery in remitted first-episode psychosis at 7 years of follow-up of an early dose reduction/discontinuation or maintenance treatment strategy: Long-term follow-up of a 2-year randomized clinical trial. JAMA Psychiatry. (2013) ;70: :913–20. |
[24] | Rappaport M , Hopkins HK , Hall K , Belleza T , Silverman J . Are there schizophrenics for whom drugs may be unnecessary or contraindicated? Int Pharmacopsychiatry. (1978) ;13: :100–11. |
[25] | Whitaker R . Mad in America: Bad Science, Bad Medicine, and the Enduring Mistreatment of the Mentally Ill. Cambridge: Perseus Books Group; (2002) . |
[26] | Jablensky A , Sartorius N , Ernberg G , Anker M , Korten A , Cooper JE , et al. Schizophrenia: Manifestations, incidence and course in different cultures. Psychol Med Monogr Suppl. (1992) ;20: :1–95. |
[27] | Hopper K , Wanderling J . Revisiting the developed versus developing country distinction in course and outcome in schizophrenia: Results from ISoS, the WHO collaborative followup project. International Study of Schizophrenia. Schizophr Bull. (2000) ;26: :835–46. |
[28] | Seikkula J , Aaltonen J , Alakare B , Haarakangas K , Keränen J , Lehtinen K . Five-year experience of first-episode nonaffective psychosis in open-dialogue approach: Treatment principles, follow-up outcomes, and two case studies. Psychotherapy Research. (2006) ;16: :214–28. |
[29] | Svedberg B , Mesterton A , Cullberg J . First-episode non-affective psychosis in a total urban population: A 5-year follow-up. Soc Psychiatry Psychiatr Epidemiol. (2001) ;36: :332–7. |
[30] | Work Group in Schizophrenia. Practice guideline for the treatment of patients with schizophrenia. American Psychiatric Association 2010, pp. 184. Available from: https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/schizophrenia.pdf. |
[31] | National Institute for Health and Care Excellence. Psychosis and schizophrenia in adults: Prevention and management. UK: NICE; 2014 Feb. Report No.: CG178. Available from: https://www.nice.org.uk/guidance/cg178. |
[32] | Holzinger A , Loffler W , Muller P , Priebe S , Angermeyer MC . Subjective illness theory and antipsychotic medication compliance by patients with schizophrenia. J Nerv Ment Dis. (2002) ;190: :597–603. |
[33] | Varese F , Smeets F , Drukker M , Lieverse R , Lataster T , Viechtbauer W , et al. Childhood adversities increase the risk of psychosis: A meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr Bull. (2012) ;38: :661–71. |
[34] | Schäfer I , Fisher HL . Childhood trauma and psychosis - what is the evidence? Dialogues Clin Neurosci. (2011) ;13: :360–5. |
[35] | Romme M , Escher S , Dillon J , Corstens D , Morris M . Living with voices: 50 stories of recovery. Reprint ed. Herefordshire: PCCS Books; (2010) . |
[36] | Demyttenaere K , Donneau A-F , Albert A , Ansseau M , Constant E , van Heeringen K . What is important in being cured from depression? Discordance between physicians and patients (1). J Affect Disord. (2015) ;174: :390–6. |
[37] | Zimmerman M , McGlinchey JB , Posternak MA , Friedman M , et al. How should remission from depression be defined? The depressed patient’s perspective. Am J Psychiatry. (2006) ;163: (1):148–50. |
[38] | Schneider LS , Dagerman KS , Insel P . Risk of death with atypical antipsychotic drug treatment for dementia: Meta-analysis of randomized placebo-controlled trials. JAMA. (2005) ;294: :1934–43. |
[39] | Increased mortality in patients with dementia-related psychosis. FDA Alert 2005; 11 April. https://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm152291.htm. |
[40] | Dold M , Li C , Tardy M , Khorsand V , Gillies D , Leucht S . Benzodiazepines for schizophrenia. Cochrane Database Syst Rev. (2012) ;11: :CD006391. |


