
When spider webs unite, they can tie up a lion1: NLM’s work in information technology and health in Africa, 1997–2011
Abstract
In 1997, Donald A.B. Lindberg M.D., Director, U.S. National Library of Medicine (NLM) agreed to address the request of African malaria researchers for full access to the Internet and medical journals as part of the U.S. National Institutes of Health’s (NIH) contribution to the Multilateral Initiative on Malaria (MIM). This challenge matched my interests and previous experience in Africa. I joined NLM in 1997 to help establish the MIM Communications Network (MIMCom) in partnership with several NIH components and more than 30 other partners in Africa, the U.S., the United Kingdom (U.K.), and Europe. After a successful launch of MIMCom, NLM worked with African partners to create a series of innovative programs with scientists, librarians, journal editors, and medical students to build capacity on the continent and enhance global access to research in Africa.
1.Background
The challenge that drew me to the U.S. National Library of Medicine (NLM) and to working with its Director, Donald A.B. Lindberg, M.D., came from a meeting of African malaria researchers, funding agencies, and academic and non-governmental organization (NGO) partners in Dakar, Senegal, in January of 1997. African scientists wanted the same tools and support for carrying out research that scientists in the industrialized world enjoyed. African scientists wanted to be able to communicate with colleagues, have access to medical literature, collaborate on proposals, write papers and present their research to the world. They wanted to build capacity through mentoring and competing for grants, create multi-country networks, and send large amounts of data.
Out of this meeting came the Multilateral Initiative on Malaria (MIM) and the critical commitment of Harold Varmus, MD, then Director, U.S. National Institutes of Health (NIH), to assist the African researchers and to put money on the table to do so [1]. Dr. Varmus asked Don Lindberg and NLM to address African researchers’ request for Internet access, at the time often practically unusable or nonexistent, and access to medical journals. Don embraced the challenge, and that is where this chapter begins.
In 1997, malaria in Sub Saharan Africa was killing more than one child every minute, based on data available from the Institute for Health Metrics and Evaluation (IHME), Global Burden of Disease (GBD), and the World Health Organization (WHO) [2]. Yet malaria was a minor blip on the radar screen of global health, and most funding for research, control, and treatment in Africa was focused on HIV/AIDS which, of course, had been a scourge in the U.S. as well.
At that time, most major U.S.-based or U.S.-supported funding agencies that would later publicize malaria as a major health issue in Sub Saharan Africa were not yet in existence. The Bill & Melinda Gates Foundation was founded in 2000, The Global Fund to fight AIDS, Tuberculosis, and Malaria was started in 2002, the President’s Emergency Plan for AIDS Relief (PEPFAR) was launched in 2003, and the U.S. President’s Malaria Initiative was announced in 2005.
In Africa, many research sites had been set up by universities and institutes from the UK and Europe, often, but not always, following old colonial, i.e, top down, or non-governmental organization (NGO) models, i.e, often stand alone and not coordinated with one another or with the health priorities of the African countries where they were based. NLM strove to implement a collegial approach. What follows is a story of listening to the African scientists’ concerns and responding to their needs - an unusual modus operandi in 1997.
In the spring of 1997, I took the long escalator out of the Medical Center Metro station in Bethesda, MD, for a meeting at NLM. My family was in the process of relocating to Washington, DC, from Cambridge, Massachusetts. Kent Smith, then NLM Deputy Director, had told my husband Brian Kahin that NLM needed a person with IT, health information, and Africa experience to work on a mandate from the NIH Director. The mandate was to assist malaria researchers in Africa with enhanced Internet connectivity and access to medical literature. Although health IT in Africa today is a crowded (probably overcrowded) field, it was not then, and this specific expertise and on-the-ground experience were not to be found at NLM or NIH. However, as fortune would have it, the mandate from the African scientists mapped precisely with my earlier remit at SatelLife, a small NGO in Cambridge [3].
At SatelLife, I had been part of the team setting up HealthNet. We used a small low-earth orbit satellite, designed and manufactured by Surrey Satellite Technology Ltd in the UK, and simple ground stations on earth, each made up of a computer, “ham” radio, special modem, and send and receive antennae. I had initiated and been director of the HealthNet Information Service which comprised a document delivery service (volunteers using snail mail, diplomatic pouch, or any means possible), a Library Partnership Program between African librarians and librarians in the U.S. and U.K., and HealthNet News. HealthNet News was the first electronic publication for health in Sub Saharan Africa which published weekly and continuously for 20 years (now archived in NLM’s History of Medicine Division.) HealthNet, the first telecommunications system for health in Africa, was officially inaugurated in 1991.
During my days at SatelLife, I had met Don who was curious about the small satellite and its mission. Although he saw no possibilities for collaboration with NLM at that time, I never forgot his genuine interest. Fast forward only a few years to what would become the perfect opportunity for me to be part of a much larger collaboration: a need as expressed by African researchers for access to high quality Internet bandwidth and to current medical journals.
This chapter is another testimony to Don’s brilliance in bringing together technology with health information, but also his willingness to risk incorporating me, a government outsider with African experience in IT and health information, into the home base at NLM in fulfillment of an NIH directive.
2.Connecting African malaria researchers: Multilateral Initiative on Malaria Communications Network (MIMCom)
The Multilateral Initiative on Malaria Communications Network (MIMCom) was one of four main components of the MIM, an international alliance of organizations (governmental, non-governmental, and academic) and individual scientists concerned with malaria research. The other components were a secretariat, a granting agency (with NIH funding for young African researchers administered by a unit of the World Health Organization (WHO), and a reagent center [1]. MIM’s aims were to maximize the impact of scientific research on malaria in Africa by promoting capacity building and facilitating global collaboration and coordination. These objectives distinguished MIM from other eradication movements past and present. With marching orders from African scientists, NLM set out to play a role in supporting research objectives and capacity building.
When I think about Don and Africa, I hear his voice and the pithy (often humorous) bits of wisdom he would put forth. Don’s guiding phrases were like lanterns along the way and still are. Here are a few from those early days:
“What are the people on the ground trying to do that they can’t do now?” Don wanted to help people on the ground do what THEY found difficult, not what WE (“well-intentioned white people” - my words) wanted to do or thought they should do.
“Make something work somewhere first”. This was in response to chatter from others about beginning with the idea of a big network that MIMCom eventually turned out to be.
“First, get two research sites to communicate with one another.” His practicality was wonderful!
Don believed that we needed to move toward “where the puck is going to be”, in the immortal words of the legendary Canadian hockey player Wayne Gretzky.
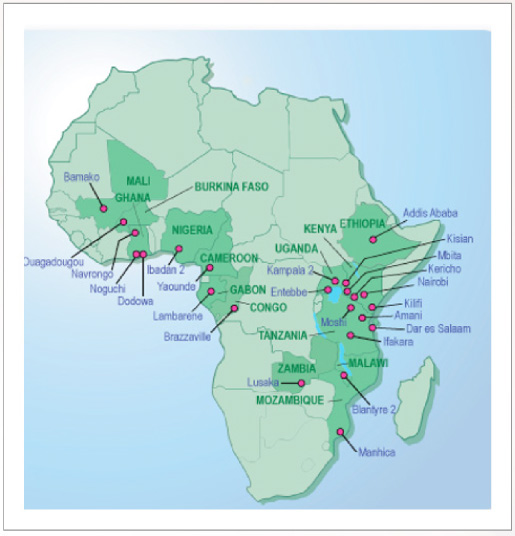
Under Don’s leadership, NLM responded to the mandate from the NIH Director and played a critical part along with the Fogarty International Center, the National Institute for Allergy and Infectious Diseases (NIAID), the Office of the NIH Director, and more than 30 other partners (funding agencies, foundations, and universities in Africa, the US, the UK, and Europe) in setting up MIMCom. MIMCom used a variety of technologies to enhance or introduce Internet connectivity and access to medical literature for malaria research sites in Africa where there was little or no access to either. Eventually comprising 27 research sites in 14 African countries, MIMCom was sustained by the research funders and partners at each site (Fig. 1).
Fig. 1.
MIMCom Sites in 2011.
Coincidentally, in the summer of 1997, just as MIM was gaining momentum, NLM, under Don’s leadership, took the bold step of making MEDLINE, its premier database, available free to the networked world. Now, anyone with access to the Internet could search MEDLINE and read abstracts. Getting full text articles was still a challenge. Partner universities with well-stocked medical libraries stepped into the breach. A few years later, full text access became easier for all with the advent of NLM’s PubMed Central. The WHO-organized HINARI program also assisted lesser developed countries with access to medical literature.
Don was interested in focusing on quality malaria research sites in Africa that had funding partners - a guiding principle for MIMCom. To celebrate and incorporate the African scientists’ mandate, the project would follow a collegial rather than a colonial or NGO paradigm. That is, we would work with scientists in Africa to find out what it was they were trying, but unable, to accomplish. The focus would be on supporting science rather than gadgetry. The project would not be simply “plug and play” but would involve training, support, and feedback to enable the scientists to carry out their work and achieve their specific scientific objectives.
In the background, I kept my own research question close at hand: How can an IT intervention make a difference in the morbidity and mortality of a disease or a health system (at a Level II Clinic, for example) in a specific place (Mifumi village, Uganda, for example)? The endpoint should be improved health. If we aren’t asking ourselves this question, why are we doing this work? Technology is only a tool.
The challenges were not only in choosing the most suitable and affordable technology for each site but in setting up a system capable of delivering the service each site required while creating synergies for specific research agendas. I recruited Mark Bennett, an English colleague from SatelLife days and an early IT pioneer in Africa, as technical director. Our work plan entailed visits to each site before any technology was considered. Initial surveys documented scientific aims as well as capacity available (or not) to carry out those aims. The team evaluated the availability of local telecommunications to browse the web, send email and large data files, and download large documents.
The first questions were always: What is the need - i.e., what do people need to do that they can’t do now? Can the technology proposed to address this need be made to work on the ground, given the vicissitudes of electricity? Is the technology solution sustainable – technically and financially? Most important, do the recipients actually view the technology as critical to what they are trying to do, so they might pay money for it and make sure it is integrated into their budgets?
A separate very small aperture terminal (VSAT) satellite system was the answer for two and eventually 10 of the sites. Buying VSAT capacity as a group benefited everyone and underscored the concept of cooperation, even at the technical level [4]. The hope, of course, was that better communication would help prevent wheel reinvention and enhance active collaboration.
We assembled an Advisory Committee of African senior malaria scientists from seven countries across the continent. They offered their expertise on content for a project website, MIMCom Malaria Research Resources, and a weekly newsletter, MIMCom Malaria News (still active as MalariaWorld). They identified their disease priorities, including malaria, HIV/AIDS, TB, and diarrheal disease. Although there was nothing surprising in their list, we believed it critical that priorities were identified by African scientists rather than by funding agencies.
MIMCom was not beholden to any one technology, and was not funded by a single institution, but by a consortium of funders who supported research at each site. Two examples:
• In Ghana at the Noguchi Memorial Institute in Accra and the field site Navrongo Health Research Center in Navrongo: U.S. Naval Medical Research Institute (NMRI)/Naval Medical Research Center (NMRC), NIAID, and the U.S. Agency for International Development (USAID).
• In Kenya, at the Kenyan Medical Research Institute (KEMRI) sites in Nairobi, Kilifi, Kisian, and Kericho and the International Center of Insect Physiology and Ecology (ICIPE) in Mbita, funders included the U.S. Centers for Disease Control (CDC), U.S. Walter Reed Army Institute of Research (WRAIR), the Wellcome Trust (U.K.), and U.S. National Institute of Allergy and Infectious Diseases/National Institutes of Health (NIAID/NIH).
Given the diversity of partners and funding sources, the administration of MIMCom was difficult to set up and manage and had a number of moving parts. But through the desperate need of the scientists and the education of funders (i.e., connectivity needs to be a line item on research proposals!), this modest experiment became sustainable.
3.Impact of MIMCom on African researchers
In a January 22, 2001 interview with the author, Dr. Andrew Githeko, Senior Scientist, KEMRI-CDC research site in Kisian, Kenya (one of the first two sites connected on MIMCom) stated:
Now I am functioning as well as anyone in the U.S. and Europe regarding communications. We are a part. We manage projects, some set in Maryland, some set in UK. We forward mail to each other, we plan, and agree and disagree. We run projects in Africa. We are a part. We can discuss plans. It is not one man writing a letter, giving instructions. There is a difference here…. It’s a completely different way of communicating [5].
His view of MIMCom was corroborated in this excerpt from the 2002 report of a review of the overall MIM program:
“We’re not so far away, anymore,” said one researcher. “We’re finally ‘here’”.
Increasing the connectivity of African scientists, both with each other and with scientists in the rest of the world is a role that MIM has played well. Electronic access to journals and a new ability to communicate easily with other scientists, together with MIM-provided opportunities for face-to-face meetings at workshops and conferences, has greatly facilitated Africa capacity development.
High-speed Internet connection to the WWW and e-mail has created an almost entirely new set of opportunities for the scientists located in the MIMCom centers. Many of the sites feel that they would no longer be able to function without this facility and regard the enhancement of connectivity as a significant step toward reducing the inequities of research advantages in the North compared to the South.
The creation of MIMCom has provided isolated scientists with tools that bring the whole world closer. Reliable communication with collaborators and vastly improved access to the scientific literature have both increased the reach of African scientists and facilitated their participation in the broader scientific world, especially by improving their ability to publish in world-class journals, a key part of being a mainstream scientist [6].
MIMCom facilitated malaria research in: epidemiology; antimalarial drug resistance; pathogenesis and immunology; entomology and vector studies; natural products and drug development; and health systems and social sciences. A survey of researchers at MIMCom sites conducted from August 2002–February 2003 showed MIMCom was making a significant difference in professional performance among collaborations with colleagues, short courses taken, proposals written and funded, papers published, and clinical trials. Connectivity counteracted isolation and improved self-esteem [7].
And it all started with helping two sites decide what they needed to do and then supporting them in communication with one another. Seven years later, connectivity at the MIMCom sites across the continent was sustainable, and the sites were on their own to choose how they wanted to develop their telecom futures [8].
4.MIMCom as a spark for additional NLM capacity-building in Africa
Don liked the strategy of linking new initiatives to existing successful programs. The three initiatives that follow - with African medical librarians, journal editors, and medical students - were possible due to the success of MIMCom. They were patterned on my earlier work at SatelLife and coordinated with extant core programs at NLM. All focused on specific need and on local sustainability, ownership, and autonomy.
4.1.NLM African associate fellows and the network of african medical librarians
Don admired the NLM Associate Fellowship program, a long-standing year-long post-masters training program for librarians. This program was primarily domestic, but Don approved adding an international slot. In 2001, he supported a proposal to focus the international slot on Africa, strongly advocating that African Associate Fellows participate in same curriculum with U.S. Fellows on-site at NLM.
As part of my earlier work at SatelLife, I had gotten to know a number of medical librarians across Africa. In the countries where SatelLife had nodes, the librarians often ran the ground stations, mastering the technology to pull down messages and HealthNet News from the satellite and distributing them in hard copy to physicians and scientists.
Nancy Kamau, a librarian from the Kenya Medical Research Institute (KEMRI) whom I had known since 1990, became the first NLM Associate Fellow from Africa. While at NLM, she was able to assist KEMRI’s African Journal of Health Sciences in submitting XML tagged data to NLM for inclusion in MEDLINE/PubMed, while helping NLM develop guidance to assist other journals in developing countries to do the same. Don was very pleased with this outcome and Nancy’s role in bringing it about.
Nancy’s view of her experience as a Fellow echoes sentiments of researchers connected by MIMCom: “When I was at home in my library, I felt like I am all alone, but when I came here [to NLM] I knew that there are so many people out there who can assist me if I needed something. There is so much I can do…”.
All told, six medical librarians from the African continent have participated in the NLM Associate Fellows Program. These librarians and other NLM partner librarians in Africa came from academic institutions in Kenya, Mali, Morocco, Mozambique, Nigeria, Uganda, Zambia, and Zimbabwe.
In 2009, with NLM's support, we formed the Network of African Medical Librarians (NAML), an independent consortium with a secretariat in the Office of the Vice Chancellor at Kenyatta University in Kenya. Organized as a network with former NLM Associate Fellows from Africa at the core, the librarians maximized their strength as a group, sharing their expertise across the continent. They have assumed leadership positions in the Association for Health Information and Libraries in Africa (AHILA) as well as its country chapters. The Network’s vision is to strengthen health sciences education, research, and outreach for better health outcomes in Africa. Their mission is to expand the frontiers of health information through outreach to and training of African librarians, the academic community, health care professionals, and health policy makers. The Network has been active in improving electronic access to research and health care information in Africa (Fig. 2). Their training manual Finding, Organizing, and Using Health Information was made freely available on the web.
Fig. 2.
Artwork commissioned for the African Digital Health Library project.
4.2.Strengthening african medical journals: African Journal Partnership Program (AJPP)
From time to time, African medical journal editors would give me copies of their journals to take back to NLM. They were keen to be indexed in MEDLINE. Don wanted to strengthen African medical journals, so they could be part of the main game (MEDLINE), as opposed to living in a separate regional database that few would see. He believed everyone would benefit from access to African research.
As in other developing regions, African journals often lack the necessary resources to carry out peer review and publish regularly. To address these needs, NLM collaborated with the Fogarty International Center and the National Institute of Environmental Health Sciences at NIH to create the African Journal Partnership Program (AJPP) in 2004. AJPP was envisioned as a health and medical journal capacity building program in Africa. The initial four African journals self selected, and five major medical journals from the US and the UK joined them in partnership. The Council of Scientific Editors was engaged as the AJPP secretariat [9].
As with MIMCom, the mission of AJPP came from the African journal editors: to promote publication excellence in African health and medical journals and allow for wider dissemination of African research results. The founding meeting was held at the British Medical Association and hosted by the British Medical Journal (BMJ) in London.
Our strategy for reaching the editors' goals was to create partnerships between interested African health and medical journals and leading journals published in the United States and the United Kingdom. We believed that learning would be two-way with this partnership opportunity, and that this strategy would serve the program's goal - to strengthen the African journals, so that they could be accepted into MEDLINE and make African research results available to the world. Valuable research carried out in endemic countries is not often available to a wider international audience.
We worked directly with all partners to facilitate the collaboration of African journal editors with their counterparts at international journals; to improve the technical production capability of African journals; to support training of writers, reviewers, and journalists in the field; to encourage the editors in planning for succession and sustainability; and to help journals earn acceptance for indexing into MEDLINE and other major databases. The partnership began with four African journals; six more were added later. As of 2011, five participating journals from Ethiopia, Ghana, Malawi, Mali, and Uganda had been accepted into MEDLINE.
In an August 5, 2013 interview, James Tumwine, Editor in Chief of African Health Sciences and Professor of Paediatrics and Child Health, Makerere University College of Health Sciences, Kampala, Uganda, described his AJPP experience to the author:
The AJPP has been a catalyst and has enabled us to, through small funds, do a lot of work. Our journal has grown. We have been indexed on MEDLINE, and recently we were indexed on ISI and have an impact factor. To us, that means quite a lot. It means we are equals, among equals.
When we started the journal, the impetus was to have an African journal publishing African material. We were finding it extremely difficult to have our scientific material published in western journals for various reasons.
I am really so glad that we are now able to publish like other journals. It has been quite difficult, but AJPP has done a lot to help us along the way…. AJPP gives us a lot of visibility, and also credibility, and, of course, citations. So, it is being visible but also being sustainable that has been, to me, the biggest achievement …. Our initial partnership was with the British Medical Journal, and we learned enormously from the BMJ. They are an extremely large journal with a very huge building. We are a very small journal in a small building. But we really appreciated their ideas and their suggestions and used them to maximize time and human resources…. We have learned to use small bureaucracy to do big things….
I am married to free access. If we can publish material and make it available, freely available, then we are training our students and our staff and keeping them up to date. They will be high class scientists and health workers. That’s what motivates me.
4.3.MedlinePlus african tutorials developing a culture of research and community involvement: African medical students
One afternoon in a noisy hallway as classes were changing at Makerere’s School of Medicine in Kampala, Uganda, I showed eager students NLM’s popular MedlinePlus website. They were especially engaged by the interactive tutorials. Why not create tutorials for diseases in Africa? Malaria and diarrhea were the obvious first choices based on the list of disease priorities from our advisory panel of African scientists and clinicians at the beginning of MIMCom.
Don was a strong believer in training, mentoring, and encouraging student work and ideas throughout his career, and his support was critical. Prior to joining NLM, I had enjoyed meeting medical students while in Uganda and had strong working relationships with their elders: the Dean of Makerere University’s School of Medicine as well as the Head of the Albert Cook Medical Library. The idea could grow from here.
We brought together the students and their faculty advisors with Ugandan artists, actors, and translators to create tutorials on malaria and diarrhea. When they were ready to go online and become part of the MedlinePlus database, NLM’s MedlinePlus team back in Bethesda was ready to collaborate.
Early versions of these tutorials were field-tested by the students as part of their medical school program called COBES (Community-Based Education and Service) during which students engage in field work at the village level. For several weeks during each year of their medical training, students go back to the same village for two-way learning. After a favorable response and learning what worked and what didn’t during the field-testing, the students made laminated booklets and posters, and a local producer incorporated audio versions with actors speaking in local languages. The students were now ready to use the “information intervention” for rural communities to be used as part of COBES. But we needed just the right platform for implementation.
Fortunately, African colleagues had taken me out to a village called Mifumi in Eastern Uganda. Mifumi had a good health center with medicines, electricity, and a small staff of health workers and nurses, overseen by a Nurse Sister. The students, their medical skills, and their “information intervention” were warmly welcomed. Back at the School of Medicine, we were able incorporate this village officially into the COBES program. During their first visit to Mifumi, the students created a survey to ascertain a baseline of malaria knowledge in the village. The results of this survey informed the final content of the tutorials.
The booklets and posters were distributed throughout the COBES program. The students learned about working at the village level and the local beliefs people held about their health. Some students had never lived in a village and might find their passion for care at that level. Others would go on to work on the wards of a hospital and never see much of village health care again. The Dean believed that exposure to health issues at the village level was imperative to medical training.
In addition to providing a learning experience for the students at all levels, this initiative also produced Don’s favorite example of how local beliefs can affect health: in various regions of Africa, there exists the belief that mangos cause malaria (Fig. 3).
Fig. 3.
Page from the MedlinePlus african tutorial on malaria.
From an interview by the author in 2007 with three medical student project leaders – Nixon Niyonzima, Nelson Igaba, and William Lubega– at Mulago Hospital, Kampala, Uganda:
Niyonzima: The original draft [of the tutorial] was tailored by doctors and by medical students not culturally adapted at that time. What was put in the draft was what was in the books, not community beliefs…. When it is the mango season, it is the rainy season, so you can really connect the two. We have malaria highest during the rainy season, we have mosquitoes highest during that time, and people attribute malaria to mangoes and rainfall. And then, of course, there are people who tell you that malaria is caused by mosquitoes, and this is what we expected people to know. But then there are those who will tell you maybe it is God; you have done something wrong, and God is punishing you.
Igaba: If you go there and tell someone to put water in the fridge and he has never seen a fridge, you’d better tell the person, you keep water in a pot. Because they have seen pots. You just teach them how to keep the pot clean. We thought of redrafting the tool, which has helped us fit the culture of the people we talk to, and they understand, because we are talking to them through what they are used to.
Lubega: We carried out a baseline survey on malaria to find out how much the people knew about malaria, their attitudes on malaria, their practices. We go into the community, we collect what their beliefs are, and we look at the main information from the medical profession. Then we integrate the two in a multidisciplinary approach to reach out to the people within the communities….
We are very excited about the posters because people saw things in the posters that they could relate to in their own communities. For example, the mangoes. The [health workers] have been telling people about malaria, but they didn’t have anything tangible that the patients could walk in, see, and easily relate to. People remember the visuals and learn to associate the vector with the disease, which was very important for us.
Niyonzima: a part of the NLM Tutorials for Africa project elevates someone from a position of powerlessness and inability to one of endless possibilities. That is, knowledge is power. And when you get the knowledge, you are able to create a difference in somebody’s thinking and somebody’s actions. We have been able to reach out to several communities to educate them, empower them, and give them the ability to change their livelihood, to change their situations. People might feel powerless because they think that malaria is a punishment from God. Now they can do something about it because they are empowered, they have the knowledge. We think the goal is to make a difference in society.
In a later collaboration with Ugandan health informatics experts and under the guidance of the Nurse Sister, students conducted an observational study in actual use of bednets to prevent malaria, employing a digital pen application (in partnership with NLM technical staff) for collecting data [10]. This project concluded with a community meeting in Mifumi village in which the students presented their research findings to the village. More than 150 people came and stayed for two hours [11].
This work in Mifumi village inspired expansion from malaria and diarrhea into other tutorials designed to help both health professionals, research scientists, and communities address local health problems, including mental health in war-torn Northern Uganda, tuberculosis, and Burkitt’s Lymphoma, the latter in collaboration with the National Cancer Institute.
5.Epilogue
What started as an access and connectivity effort in collaboration with NIH spawned related capacity building programs with medical librarians, medical journal editors, and medical students – in academia and in the village – all developed in the rich soil of NLM. Don was supportive of each one. He knew I wanted to help our colleagues in Africa - and he did, too. NLM was the perfect stage for giving voice to the women and men of African science and medicine. We demonstrated a collegial approach which tried in every way to eschew old colonial paradigms.
Today, the playing field is not exactly level, but many African researchers, clinicians, health workers, not to mention academics and students, have some tools that enable them to carry out much of the quotidian business of science and medicine. They can communicate with one another and collaborators all over the world; they can network with colleagues, learn of deadlines for grant proposals and submit applications, and write papers for publication. Their contributions are critical. The next chapter will be written by those who use the tools we have shared to navigate the noisy information environment and create new solutions unique to Africa.
I had the privilege of being an “Africa advocate”, as my WHO colleague put it when she heard I had been recruited to NLM. I loved working there and was proud to represent NLM on the African continent. NLM was truly the jewel in the crown of NIH and the best face the U.S. government could possibly have in Africa.
My gratitude to our late leader Donald A.B. Lindberg M.D., Director, U.S. National Library of Medicine, who was open to new possibilities, encouraged imagination, and gave me a long leash!
References
[1] | A. Heddini, G.T. Keusch and C.S. Davies, The multilateral initiative on malaria: Past, present, and future, Am J Trop Med Hyg 71: (2 Suppl) ((2004) ), 279–282, Available from: https://www.ncbi.nlm.nih.gov/books/NBK3741/. |
[2] | M. Roser and H. Ritchie, Malaria. in: Our world in data. [Internet]. Global Data Change Lab, Oxford (UK), 2019 [cited 2021 May 14]. Available from: https://ourworldindata.org/malaria. |
[3] | T. Groves, SatelLife: Getting relevant information to the developing world, BMJ 313: (7072) ((1996) ), 1606–1609. doi:10.1136/bmj.313.7072.1606. |
[4] | E.R. Siegel, J. Royall and M. Bennett, Enhancing communications and connectivity in Africa: The multilateral initiative on malaria (MIM) model, Stud Health Technol Inform 84: (Pt 1) ((2001) ), 48–52. |
[5] | J. Royall, Faces of change, Am J Public Health 95: (4) ((2005) ), 559–561. doi:10.2105/AJPH.2004.054478. |
[6] | M. Bockarie, Q. Bond, S. Mutambu, T. Nchinda, I. Quakyi, M. Rodriguez-Lopez Review of the Multilateral Initiative on Malaria (MIM). Fogarty International Center, National Institutes of Health, Bethesda, MD, (2002) . |
[7] | J. Royall, I. van Schayk, M. Bennett, N. Kamau and M. Alilio, Crossing the digital divide: The contribution of information technology to the professional performance of malaria researchers in Africa, African Health Sciences 5: (3) ((2005) ), 246–254. |
[8] | J. Royall, M. Bennett, I. van Schayk and M. Alilio, Tying up lions: The first chapter of a malaria research communications network in Africa, Am J Trop Med Hyg 71: (2 Suppl) ((2004) ), 259–267. |
[9] | T.J. Goehl and A. Flanagin, Enhancing the quality and visibility of African medical and health journals, Environ Health Perspect 116: (12) ((2008) ), A514–A515. doi:10.1289/ehp.12265. |
[10] | S. Ndira, D. Ssebadduka, N. Niyonzima, N.K. Sewankambo and J. Royall, Tackling malaria in Mifumi village: A report on a concerted effort by healthcare providers, the community, and information experts, Afr Health Sci 14: (4) ((2014) ), 882–888. doi:10.4314/ahs.v14i4.16. |
[11] | J. Royall, Strategies for positive outcomes: Can information technology make a difference in health in Africa, Stud Health Technol Inform 149: : ((2009) ), 58–73. |

