
There’s a gap between digital health information and users — let’s close it
Abstract
Digital health tools have the potential to improve health decision-making. Early evidence suggests their use may even be able to improve health outcomes. However, some health information and digital tools are not understandable or accessible to the majority of the U.S. population. This report explores the current disconnect between online health information and users. The authors provide a summary of practical strategies to address this gap and suggest next steps for further research.
1.Introduction
Providing health information online - including strategies to prevent and manage diseases and tools to track progress toward wellness goals - can dramatically increase the reach of life-saving information. Almost all Americans (90%) use the internet, and most (81%) have searched online for health-related information in the last year [1,2].
The shift toward digital has led many health organizations, including U.S. government agencies, to move information and services online. But the barriers to access and use online information and tools can prevent leveraging their promise of enhanced reach and improved patient engagement.
This report explores the accessibility and usability challenges that digital health tools present for most people - and how we can overcome them to improve health literacy and health outcomes. The authors discuss practical, evidence-based strategies to improve the clarity and usability of digital health tools, as well as ideas for future research on emerging best practices. Note that for simplicity, we will use the term “digital health tools” to include health websites, apps, and interactive online tools.
The organizing question of this report is: How can we design digital health tools so their usability demands do not limit their reach?
2.Challenges and opportunities
Roughly one in two American adults struggle with literacy and read at an eighth-grade level or below [3]. And one in five adults read at a fifth-grade level or below [3]. Research suggests this has direct health implications. For example, Americans with low literacy skills are four times more likely to report fair or poor health than persons with the highest literacy skills [4].
The unique characteristics of digital health information, including context and complexity, make it challenging to communicate and understand. In 2015, the National Quality Health Website Survey identified and reviewed 100 top-ranked health-related websites. Researchers selected the sites based on traffic data, including unique visitors and pageviews. They then evaluated the websites using evidence-based criteria for improving the user experience through design, organization, and content. Fewer than half of the websites (42%) met the pre-selected quality criteria [5].
Additionally, the people most likely to have health problems — including lower income, older, rural, and non-white Americans — also are most likely to struggle to use digital health tools [6]. People with low health literacy are less likely to use online health information and tools, including patient portals and apps that track health behaviors [7,8].
To further complicate matters, people often access digital health information to inform or make health-related decisions. For example, research specific to health insurance decision-making clarifies that Americans struggle to understand health insurance - tasks like comparing insurance plans require consumers to navigate unfamiliar jargon, understand and use numbers (numeracy), and navigate an abundance of choice [9]. Since these activities typically happen online, the usability and accessibility problems with digital health tools become even more significant.
Despite these challenges, the potential of digital information and tools to transform health and health care is significant. Studies with diverse audiences - including young adults, gay men, and older adults - found a correlation between the use of digital health interventions and desired health behavior changes [10]. Among individuals with chronic pain, the use of multiple digital health tools is correlated with better self-reported pain management coping skills [11].
Digital health information also may influence people to get recommended preventive health services, such as vaccinations and screenings for communicable and chronic diseases [12,13]. In a 2017 comparison study (conducted by the Office of Disease Prevention and Health Promotion within the U.S. Department of Health and Human Services and CVS Health, a drug store chain), CVS saw significant increased uptake of flu and pneumococcal vaccinations after the store added myhealthfinder - an online tool that generates tailored recommendations for preventive services using health literacy best practices [13]. myhealthfinder was available at the CVS Minute Clinic website and promoted on CVSHealth.
As the body of evidence supporting the use of digital health tools increases, more Americans are able to better access these services. More than half (62%) of U.S. smartphone users used their phone to get information about a health condition in the past year [14].
The number of ‘smartphone-only’ internet users has been steadily increasing as well [1]. One in five American adults now go online exclusively using their phones [1]. According to the Pew Research Center, “reliance on smartphones for online access is especially common among younger adults, non-white, and lower-income Americans” [1].
Meanwhile, non-white and lower-income individuals are more at risk for health disparities [6]. It is a concern that the latter overlaps with people who are dependent on smartphones. Overall, some health information websites may not keep up with the increase in smartphone use: many websites are not mobile friendly and their pages are not built to scale down to small screen sizes. So, while there is more access to the internet, there is also potential for a new digital divide. While people can get online, most online information is not written or designed to meet their needs [6].
3.Literacy and digital health information
Most digital health tools fail to meet the needs of the majority of the population. To understand why this persists and to identify promising strategies for improvements, the authors believe it is helpful to look at these key areas of research:
How people with low literacy search for and read online health information
The unique challenges of accessing health information exclusively on mobile
The complexity of health-related decisions and strategies that can reduce the burden on consumers
The potential of decision aids to facilitate decision-making
The ability to find, interact with, and use health information online depends largely on users’ health literacy skills. Techniques like eye-tracking have helped researchers understand how literacy levels affect the way users look at online content (see Figure 1 below).
Fig. 1.
Techniques like eye-tracking have helped researchers understand how literacy levels affect the way users look at online content.
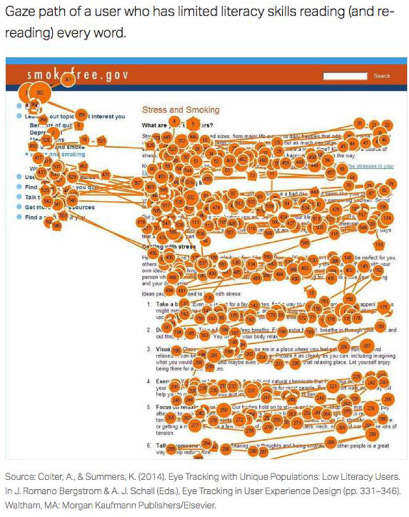
Users with stronger literacy skills tend to quickly scan pages and focus on the information most relevant to them [15]. In contrast, users with limited literacy skills are more likely to either skip whole sections on a page or, alternatively, to read every word [15–18]. Both behaviors can foster problems such as skipping sections that provide key health information. And trying to read every word can make content seem overwhelming.
The complexity of health information places a greater cognitive burden on people who read more slowly and who are likely to reread words, sections, or elements on a website (such as buttons or menus) [15]. These users are less able to remember what they have read and less likely to report a positive experience when they evaluate online health information [19].
Users with limited literacy skills also may have difficulty with website search and navigation. When using search features, users may find it challenging to pinpoint search terms, and users may struggle with spelling, or become overwhelmed by the number of search results [17,20,21]. Users may also get distracted by hyperlinks, clicking on multiple links and losing their place on the site [15,22].
The association between retention and reading speed is directly relevant to reliance on mobile for internet access. When information is easy to read, users comprehend it as well on mobile as they do on desktop platforms [23]. However, reading speed decreases significantly on mobile platforms as informational complexity increases [23]. This suggests the need for short, to-the-point health information is significantly greater for people who access health information on their smartphones [23].
Even as the number of mobile health (mHealth) apps continues to increase, fewer Americans are downloading and using them consistently [24,25]. Findings from a survey of both consumers and mHealth experts suggest the most promising way to increase the use of mobile health apps is to align them better with users’ needs. Liew et al. found consumers were primarily concerned with the familiarity of the interface, how easy it was to integrate into existing habits, and the accuracy of the information provided [24].
Consumers have to make complex decisions about their health and health care. Environmental supports, such as data visualization and decision aids, can facilitate decision-making about complex topics, including health insurance and treatment options [26,27]. Data visualization techniques communicate numbers and statistics visually, making it easier for users to see patterns and implications. For example, in a study with older adults, participants were able to make faster and more accurate decisions about Medicare plan options when presented with data visualization instead of tables. The latter was especially applicable when data visualization was used to describe one aspect of the plans at a time [26].
Several studies also suggest decision aids can be effective to help patients choose between treatment options. When there is more than one treatment available, decision aids help patients narrow the options down based on individual preferences and priorities. In a systematic review and meta-analysis, Van Weert et al. reviewed the literature on older adults and decision aids [28]. Van Weert et al. found the use of decision aids was correlated with increases in older adults’ knowledge and perception of risk, participation in shared decision-making, and ease of decision-making. Decision aids additionally help patients feel less conflicted about their decisions and more engaged in their care [29,30].
Digital health information offers more opportunities to put decision aids in patients’ hands when and where they need them. Patient portals provide consumers with 24-hour access to their electronic health records (EHR). Portals can help patients manage chronic diseases, follow through with medication plans, and get recommended screenings [12].
As health literacy professionals seek strategies to make health information easier to read and use, we also must look at ways to build decision aids and other environmental support into the tools consumers use to make everyday health decisions - from patient portals to health insurance exchanges.
4.Practical strategies to improve digital health tools
The research summarized above illustrates the diverse challenges to provide quality, online health information. Yet, there are evidence-based strategies to address some of these challenges.
Much current knowledge is summarized in Health Literacy Online: A Guide for Simplifying the User Experience, created by the U.S. Office of Disease Prevention and Health Promotion (ODPHP). The latter guide first was published in 2010, and updated in 2015 to include challenges and strategies specific to mobile use and online forms [31]. The current authors highlight a few of these strategies below.
Health information often needs to include complicated terms and concepts, but this increases the need to write clearly. In addition to using plain language and taking the time to explain medical terms, the authors suggest writers need to:
Put the most important content at the beginning. Users may not read everything, so it is vital to immediately communicate the main message. Also, users with limited literacy skills may struggle with site scrolling — they are more likely to skip content as they try to find their place again to continue reading.
Write actionable content — and less of it. People use digital health information to make decisions, so it is important to focus on specific action steps and instructions.
Engage users with interactive content. This makes it more likely that users will read and remember important health information.
How health content is displayed and organized also affects readability. If something looks difficult to read, people are less likely to try [32–34]. Moreover, if it is difficult to find what users seek - particularly if they struggle to use search functions - they may give up before they succeed. Hence, the authors suggest:
Break up text into short chunks. This helps keep users from skipping over important content — and keep them from getting overwhelmed by a “wall of words.”
Design for mobile first. Adults with limited health literacy skills are more likely to be smartphone dependent. Ensure digital tools are optimized for mobile — including both display and performance (e.g., page load speeds).
Use labels that set clear expectations. Navigation labels prepare readers for what they will see when they click. Clear labels help users navigate and find what they’re looking for more easily.
One of the benefits of online health information is it creates opportunities to engage readers in novel ways. It is possible to reach people with key health information using multiple methods, such as video and data visualization. And interactive tools like decision aids can be available in context - exactly where people already are looking for related health information.
In addition, it is essential to test products with users - particularly those who are likely to have limited health literacy skills. When online health information is developed and revised based on input from those most likely to struggle with online health information, the results foster more inclusive, effective, accessible health information products.
5.Ideas for future research
The rise in the use of digital health tools offers diverse opportunities to conduct applied and outcomes research, particularly with individuals with limited literacy and limited health literacy skills. Specifically, the field needs more research on how users interact with health information on mobile platforms. As outlined above, mobile platforms pose unique challenges and opportunities. Additional usability research - including research with eye-tracking software - will help health literacy practitioners better understand how to leverage the widespread internet access now provided by smartphones. Although users may be more willing to scroll to get information than previously, there is a dearth of research whether this extends to persons with limited literacy skills [35].
We also need to explore the barriers to an uptake of patient portals and similar tools to improve care coordination. While patient portals have an unprecedented potential to put personal health information directly into patients’ hands, portals are underused by consumers - especially by people with limited health literacy skills [8,12]. More research is needed to understand how to increase consumer trust in these tools, ensure caregiver and proxy access, and improve the overall user experience.
In addition, it is important to build on the emerging outcomes research that suggests associations among the use of health literate digital health tools with improved health outcomes. A better documentation of the successes of digital health interventions reinforce a critical need for tools that follow best practices in health content and design.
6.Summary
The authors believe there is an unprecedented opportunity to reach people with the information and tools they need to manage their health more effectively. As more people seek health information online, there is parallel evidence that the use of digital tools facilitates improved health outcomes, and population access to the internet is increasing thanks to smartphones.
There is much to do and learn in order to realize an omnipresent opportunity. At the same time, there are strategies to make health information more accessible, usable, and actionable. Health organizations now have the opportunity to capitalize on the popularity of digital health tools with content and formats to help users become more informed and confident partners in managing their health.
Acknowledgements
The authors would like to thank Blythe Miller, MPH for editing this article and Tricia Loomis, MPP and Erik Wills, MPH for assistance with the research.
References
[1] | Pew Research Center. Internet/broadband fact sheet, http://www.pewinternet.org/fact-sheet/internet-broadband/. Retrieved April 22, 2019. |
[2] | A. Polansky, J. Leslie and G. Heimann, The great American search for healthcare information. https://www.webershandwick.com/wp-content/uploads/2018/11/Healthcare-Info-Search-Report.pdf. Retrieved April 17, 2019. |
[3] | M. Kutner, E. Greenberg and J. Baer, National assessment of adult literacy: a first look at the literacy of America’s adults in the 21st century, National Center for Education Statistics. https://nces.ed.gov/NAAL/PDF/2006470.PDF. Retrieved April 23, 2019. |
[4] | OECD. Country note, United States: survey of adult skills first results. http://www.oecd.org/skills/piaac/Country%20note%20-%20United%20States.pdf. Retrieved April 23, 2019. |
[5] | T. Devine, J. Broderick, L.M. Harris, H. Wu and S.W. Hilfiker, Making quality health websites a national public health priority: toward quality standards, J Med Internet Res. 18: (8) ((2016) ), e211. doi:10.2196/jmir.5999. |
[6] | K. Latulippe, C. Hamel and D. Giroux, Social health inequalities and eHealth: a literature review with qualitative synthesis of theoretical and empirical studies, J Med Internet Res 19: (4) ((2017) ), e136http://doi.org/10.2196/jmir.6731. |
[7] | M. Mackert, A. Mabry-Flynn, S. Champlin, E.E. Donovan and K. Pounders, Health literacy and health information technology adoption: the potential for a new digital divide, J Med Internet Res 18: (10) ((2016) ), e264. doi:10.2196/jmir.6349. |
[8] | S.E. Davis, C.Y. Osborn, S. Kripalani, K.M. Goggins and G.P. Jackson, Health literacy, education levels, and patient portal usage during hospitalizations, AMIA Annual Symposium Proceedings ((2015) ), 1871–1880. |
[9] | G.L. Loewenstein, J.Y. Friedman, B. McGill, S. Ahmad, S. Linck, S. Sinkula, J. Beshears, J.J. Choi, J. Kolstad, D. Laibson, B.C. Madrian, J.A. List and K.G. Volpp, Consumers’ misunderstanding of health insurance, Journal of Health Economics 32: : ((2013) ), 850–862. doi:10.1016/j.jhealeco.2013.04.004. |
[10] | J.R.D. McIntosh, S. Jay, N. Hadden and P.J. Whittaker, Do E-Health interventions improve physical activity in young people: a systematic review, Elsevier BV 148: ((2017) ), 140-148,https://doi.org/10.1016/j.puhe.2017.04.001. |
[11] | M.L. Ranney, C. Duarte, J. Baird, E.J. Patry and T.C. Green, Correlation of digital health use and chronic pain coping strategies, mHealth 2: ((2016) ), 35. doi:10.21037/mhealth.2016.08.05. |
[12] | S.S. Coughlin, J.J. Prochaska, L.B. Williams, G.M. Besenyi, V. Heboyan, D.S. Goggans, W. Yoo and G. De Leo, Patient web portals, disease management, and primary prevention, Risk Management and Healthcare Policy 10: ((2017) ), 33-40, http://doi.org/10.2147/RMHP.S130431. |
[13] | J.M. Polinski, L.M. Harris, W.H. Shrank, A. Sussman and J. Barron, Impact of a patient engagement tool on preventive service uptake, Healthcare 6: (3) ((2018) ), 162-167, https://doi.org/10.1016/j.hjdsi.2017.12.002. |
[14] | Pew Research Center. The smartphone difference. http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015/. Retrieved April 22, 2019. |
[15] | A. Colter and K. Summers, Eye tracking with unique populations: low literacy users, in: Eye Tracking in User Experience Design, J. Romano Bergstrom and A.J. Schall (eds), Morgan Kaufmann Publishers/Elsevier, Waltham, MA, (2014) , pp. 331–346. |
[16] | K. Summers and M. Summers, Making the web friendlier for lower-literacy users, Intercom 51: (6) ((2004) ), 19–21. |
[17] | K. Summers and M. Summers, Reading and navigational strategies of web users with lower literacy skills, Proceedings of the American Society for Information Science and Technology 42: (1) ((2006) )http://doi.org/10.1002/meet.1450420179. |
[18] | K. Summers, J. Langford, J. Wu, C. Abela and R. Souza, Designing web-based forms for users with lower literacy skills, Proceedings of the American Society for Information Science and Technology 43: (1) ((2006) ), 1–12. |
[19] | C.S. Meppelink, E.G. Smit, N. Diviani and J.C. Van Weert, Health literacy and online health information processing: unraveling the underlying mechanisms, Journal of Health Communication 21: : ((2016) ), 109–120. doi:10.1080/10810730.2016.1193920. |
[20] | M.S. Birru, V.M. Monaco, L. Charles, H. Drew, V. Njie, T. Bierria, E. Detlefsen and R.A. Steinman, Internet usage by low-literacy adults seeking health information: an observational analysis, J Med Internet Res 6: (3) ((2004) )), 1-7, http://doi.org/10.2196/jmir.6.3.e25. |
[21] | D.M. Modesto and S.B.L. Ferreira, Guidelines for search features development – a comparison between general users and users with low reading skills, Procedia Computer Science 27: (Dsai 2013) ((2014) ), 334-342, http://doi.org/10.1016/j.procs.2014.02.037. |
[22] | B.M. Chaudry, K.H. Connelly, K.A. Siek and J.L. Welch, Mobile interface design for low-literacy populations, in: Proceedings of the 2nd ACM SIGHIT Symposium on International Health Informatics - IHI ’12 (2012) , p. 91. |
[23] | K. Moran, Reading content on mobile devices. Nielsen Norman Group. https://www.nngroup.com/articles/mobile-content. Retrieved April 22, 2019. |
[24] | M.S. Liew, J. Zhang, J. See and Y.L. Ong, Usability challenges for health and wellness mobile apps: mixed-methods study among mHealth experts and consumers, JMIR Mhealth Uhealth 7: (1) ((2019) ), e12160. doi:10.2196/12160. |
[25] | Research 2 Guidance. The mHealth app market is getting crowded reaching the 259,000 apps. https://research2guidance.com/mhealth-app-market-getting-crowded-259000-mhealth-apps-now. Retrieved April 17, 2019. |
[26] | M.M. Price, J.J. Crumley-Branyon, W.R. Leidheiser and R. Pak, Effects of information visualization on older adults’ decision-making performance in a Medicare plan selection task: a comparative usability study, JMIR Hum Factors 3: (1) ((2016) ), e16. doi:10.2196/humanfactors.5106. |
[27] | S. Wood, Y. Hanoch, A. Barnes, P.J. Liu, J. Cummings, C. Bhattacharya and T. Rice, Numeracy and Medicare part D: the importance of choice and literacy for numbers in optimizing decision making for medicare’s prescription drug program, Psychology and Aging 26: (2) ((2011) ), 295–307. doi:10.1037/a0022028. |
[28] | J.C.M. Van Weert, B.C. van Munster, R. Sanders, R. Spijker, L. Hooft and J. Jansen, Decision aids to help older people make health decisions: a systematic review and meta-analysis, BMC Medical Informatics and Decision Making 16: ((2016) ), 45, http://doi.org/10.1186/s12911-016-0281-8. |
[29] | I. Nota, C.H.C. Drossaert, E. Taal, H.E. Vonkeman, C.J. Haagsma and M.A.F.J. van de Laar, Evaluation of a patient decision aid for initiating disease modifying anti-rheumatic drugs, Arthritis Research Therapy 18: ((2016) ), 252http://doi.org/10.1186/s13075-016-1138-3. |
[30] | M.B. Simmons, A. Elmes, J.E. McKenzie, L. Trevena and S.E. Hetrick, Right choice, right time: evaluation of an online decision aid for youth depression, Health Expectations: An International Journal of Public Participation in Health Care and Health Policy 20: (4) ((2017) ), 714-723, http://doi.org/10.1111/hex.12510. |
[31] | U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Health literacy online: a guide to simplifying the user experience. https://health.gov/healthliteracyonline. Retrieved April 22, 2019. |
[32] | J. Redish, Letting go of the Words: Writing Web Content that Works,2nd ed. Morgan Kaufmann Publishers/Elsevier, Waltham, MA, (2012) . |
[33] | K. Summers and M. Summers, Making the web friendlier for low-literacy users, Intercom 51: (6) ((2004) ), 19–21. |
[34] | US Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Health.gov redesign: prevention prototype usability study results report. Prepared by Z-Tech Corp. Rockville, MD. 2007. |
[35] | T. Fessenden, Scrolling and attention. Nielsen Norman Group. https://www.nngroup.com/articles/scrolling-and-attention. Retrieved April 22, 2019. |


