
Is fluid retention a cardiovascular risk factor?
Abstract
Endothelial dysfunction, the earliest manifestation of atherosclerosis, can be initiated by both biochemicals and biomechanical forces. Atherosclerosis occurs predominantly at arterial branch points, arterial bifurcations and the curved segments of great arteries. These are the regions that blood flows turbulently. Turbulence promotes endothelial dysfunction by reducing shear stress upon endothelial cells. The endothelial glycocalyx mediates the effect of shear stress upon the endothelium.
A mathematical analysis of cardiovascular hemodynamics demonstrates that fluid retention increases turbulence of blood flow. While there is no empirical data confirming this relationship, fluid retention is associated with adverse cardiovascular events. Every medical condition that causes fluid retention is associated with increased risk of both atherosclerotic cardiovascular disease and venous thromboembolic disease. In addition, most medications that cause fluid retention are associated with increased adverse cardiovascular effects. Calcium channel blockers (CCBs) and pioglitazone are exceptions to this generalization. Even though data regarding CCBs and pioglitazone contradict the hypothesis that fluid retention is a cardiovascular risk factor, these medications have favorable cardiovascular properties which may outweigh the negative effect of fluid retention.
Determining whether or not fluid retention is a cardiovascular risk factor would require empirical data demonstrating a relationship between fluid retention and turbulence of blood flow. While this issue should be relevant to cardiovascular researchers, clinicians and patients, it is especially pertinent to the pharmaceutical industry. Four-dimensional magnetic resonance imaging and vector flow Doppler ultrasound have the capability to quantify turbulence of blood flow. These technologies could be utilized to settle the matter.
1Introduction
Endothelial dysfunction is the earliest detectable manifestation of atherosclerosis [1, 2]. Atherosclerosis and venous thrombosis are associated with one another. Consequently, atherosclerosis may induce venous thrombosis or the two conditions may share common risk factors [3, 4]. Proinflammatory cytokines, bacterial endotoxins, viruses, advanced glycation end products generated in diabetes and aging, cholesterol, oxidized lipoproteins that accumulate within arterial walls, vascular endothelial growth factor, estrogens, renin, prorenin, angiotensin II and biomechanical forces initiate endothelial dysfunction [5–9]. In addition, glucose and insulin may directly influence endothelial physiology [10]. Endothelial cell surface receptors bind lipids, estrogens, progestins, mineralocorticoids, thrombin, renin and prorenin [11–17]. When biochemicals bind to endothelial cells, a cascade of intracellular events ensues that culminates in endothelial dysfunction. The main limitation of a biochemical explanatory model of endothelial dysfunction is that atherosclerosis occurs primarily at arterial branch points, arterial bifurcations and at curves of great arteries. Biochemistry cannot explain why atherosclerosis is localized, whereas biomechanics can.
2Biomechanics and endothelial dysfunction
Blood flows either in a laminar manner or a turbulent manner. Laminar flow occurs in unbranched, tubular arteries, increases arterial wall shear stress and is atheroprotective. Laminar flow up-regulates endothelial genes that exert antithrombotic, antiadhesive, antiproliferative, anti-inflammatory and anti-oxidant effects [5, 18]. Turbulent flow occurs in regions prone to atherosclerosis: arterial branch points, arterial bifurcations and curved segments of major arteries [19]. Turbulence reduces shear stress upon endothelial cells. As a result, there is increased expression of inflammatory genes and increased production of adhesion molecules by endothelial cells, increased adhesion of platelets to endothelial cells and accelerated atherosclerotic plaque formation [5, 20].
Some of the turbulent blood flow that occurs within the heart is physiological. For instance, whirlpools in the left ventricle shape its walls and are vital for the proper movement and closing of the mitral valve. In addition, in the aortic bulbous, the turbulent flow that occurs during the ejection phase of systole helps to close the semilunar valve, thereby facilitating coronary blood flow. Thus, turbulence and whirlpools are not always negative.
At one time, it was thought that altered hemodynamics in areas prone to atherosclerosis disrupt endothelial integrity and facilitate the penetration of lipoproteins into vessel walls [21]. This hypothesis was discounted after it was recognized that the endothelium remains intact during the early formation of atherosclerotic lesions [22–24]. It has also been suggested that turbulent flow accelerates atherosclerosis by permitting lipoproteins to dwell near the arterial wall for longer time intervals [25].
3Endothelial glycocalyx, biomechanics and endothelial dysfunction
The endothelial glycocalyx (EG), a thin polysaccharide layer attached to the lumenal surface of vascular endothelial cells, is composed of glycoproteins and proteoglycans that are synthesized by endothelial cells. Some of these glycoproteins and proteoglycans are anchored to the endothelial cell walls, either via transmembrane domains or by covalent links to molecules associated with the outer portion of the cell membrane [26]. Other components of the EG attach to the endothelium indirectly via receptor molecules [26].
The EG provides a physical and electrostatic barrier between the endothelium and the blood elements, thereby reducing the permeability of the endothelium to erythrocytes, leukocytes, platelets, adhesion molecules, bacteria and viruses [27]. The EG also senses and transduces shear forces via connections to endothelial cell walls and to the cytoskeleton of endothelial cells, thereby mediating the effect of shear stress upon the endothelium [28]. Some of the molecular components of the EG extend perpendicularly from the endothelium in “shrub-like” configurations [29, 30]. These projections act as lever arms that amplify torque and convert shear forces into deformations of the endothelial cystoskeleton [29]. Glycocalyx mechanosensation and mechanotransduction results in activation of endothelial nitric oxide synthase (eNOS), increased production of nitric oxide and dilatation of blood vessels [31].
Increased shear stress promotes the synthesis of glycocalyx components, resulting in a thicker glycocalyx, whereas decreased shear stress causes glycocalyx degradation, resulting in thinner glycocalyx dimensions [32–34]. Areas of the vasculature with a thinner glycocalyx are associated with a pro-inflammatory endothelial cell phenotype and are more vulnerable to atherosclerotic plaque formation [34–36].
4Fluid retention, turbulence and cardiovascular disease
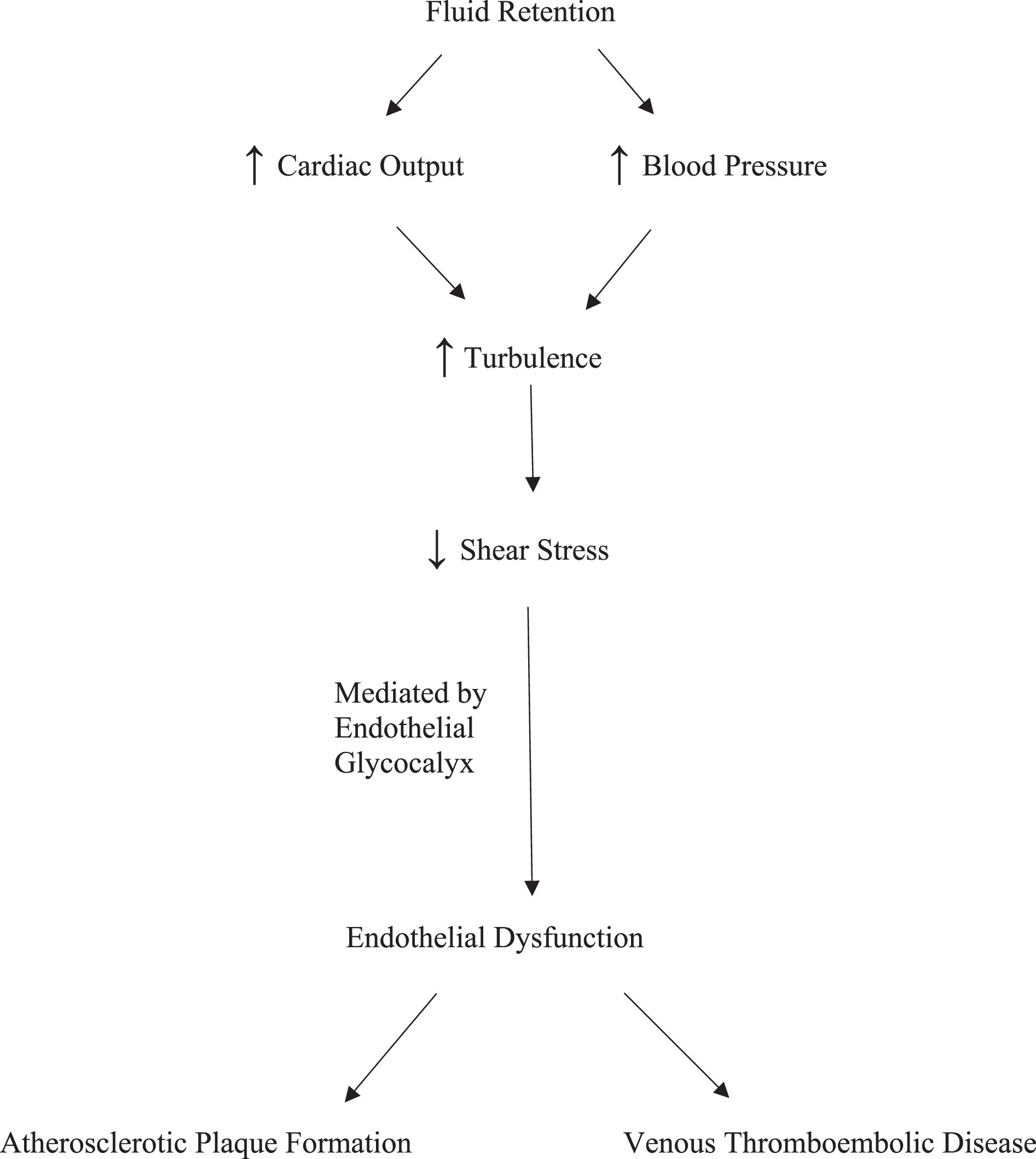
Fluid retention increases either cardiac output or blood pressure (BP) [37–39]. Cardiac output is the product of stroke volume and heart rate while cardiac work is determined by stroke volume and BP. A mathematical analysis of cardiovascular hemodynamics demonstrates that fluid retention increases cardiac work while simultaneously increasing velocity and turbulence of blood flow [40]. Although there is no empirical data confirming these relationships, fluid retention is associated with increased risk of adverse cardiovascular events. Figure 1 illustrates a proposed pathway linking fluid retention with endothelial dysfunction and cardiovascular disease.
Fig. 1
Proposed Pathway Linking Fluid Retention with Endothelial Dysfunction and Cardiovascular Disease.
Every medical condition that causes fluid retention, including heart failure, cirrhosis, nephrotic syndrome, hypothyroidism, type 2 diabetes mellitus (DM), prediabetes, obstructive sleep apnea, hyperaldosteronism and Cushing’s syndrome, is associated with increased risk of atherosclerotic cardiovascular disease (Table 1) [41–56]. With the possible exception of type 2 DM, all these medical conditions are also associated with venous thrombotic events (VTE) [41–56]. Two meta-analyses found a relationship between type 2 DM and VTE but a more recent meta-analysis did not [57–59]. In addition, a Mendelian randomization analysis found no relationship between type 2 DM and VTE [60].
Table 1
Cardiovascular disease and medical conditions that cause fluid retention
| Medical condition | Associated with atherosclerotic cardiovascular disease? | Associated with venous thromboembolic events? |
| Heart failure | yes [41–44] | yes [45] |
| Cirrhosis | yes [46] | yes [47] |
| Nephrotic syndrome | yes [48] | yes [49] |
| Hypothyroidism | yes [50] | yes [51] |
| Diabetes mellitus type 2 | yes | contradictory data [57–60] |
| Prediabetes | yes [52] | yes [52] |
| Obstructive sleep apnea | yes [53] | yes [54] |
| Hyperaldosteronism | yes [55] | yes [55] |
| Cushing’s syndrome | yes [56] | yes [56] |
The medical literature is equivocal as to whether or not sex-specific differences influence the cardiovascular complications of fluid retention. For example, one study found that men with prediabetes experience a higher frequency of cardiovascular comorbidities than women with prediabetes while another study found that cardiovascular risk was similar for men and women with prediabetes [61, 62].
For some medical conditions that promote fluid retention, particularly Cushing’s syndrome, type 2 DM and prediabetes, biochemistry is relevant. Mineralocorticoids have direct effects upon endothelial cells [15]. Since corticosteroids have mineralocorticoid activity, the increased corticosteroids in Cushing’s syndrome may have direct endothelial effects. With type 2 DM and prediabetes, glucose and insulin may have direct effects upon endothelial physiology [10]. With hypothyroidism and aldosteronism, it is not likely that biochemistry directly influences endothelial function. There are so few thyroid hormone receptors on the surface of endothelial cells that they are unlikely to be of functional significance [63]. Similarly, aldosterone does not alter the gene expression of endothelial cells [64].
After renin and prorenin bind to endothelial cell surface receptors, endothelial genomic activity increases production of proinflammatory and profibrotic proteins [17, 65]. Fluid retention decreases renin release by the juxtaglomerular apparatus of the kidneys. To the extent that renin and prorenin binding to endothelial cells influences endothelial function, there should be a reduction of inflammatory and fibrotic protein expression by endothelial cells in response to fluid retention. Since fluid retention is associated with increased thromboembolic cardiovascular disease, renin and prorenin probably do not have much direct effect upon endothelial function following fluid retention.
One obvious cause of fluid retention is sodium chloride (salt) consumption. Higher salt intake is associated with increased risk of cardiovascular disease [66, 67]. This relationship is usually attributed to the hypertensive effect of salt ingestion. Nonetheless, increased intravascular volume without hypertension, a phenomenon that occurs in salt resistant individuals, might also be a contributory factor [39, 40]. Brain natriurtic peptide (BNP) and N-amino terminal fragment of prohormone BNP (NT-proBNP) levels reflect intravascular volume and BP. For this reason, BNP and NT-proBNP are used clinically to determine the incidence and severity of heart failure. In the absence of heart failure, and after adjusting for hypertension, higher BNP levels and higher NT-proBNP levels are associated with greater risk of cardiovascular disease [69, 70].
5Medications
A number of medications cause fluid retention, including cyclo-oxygenase-2 inhibitors (COX-2 inhibitors), non-selective non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, hormone replacement therapy with estrogens and progestins, oral contraceptives, insulins, sulfonylureas, gabapentin and pregabalin. As shown in Table 2, all these medications are associated with increased risk of thromboembolic cardiovascular disease [71–93]. Insulins, corticosteroids, estrogens and progestins may have direct effects upon endothelial cells [10, 12–15]. Rofecoxib increases cardiovascular risk even though it decreases some markers of inflammation associated with endothelial dysfunction [94]. This apparent contradiction is reconcilable by the observation that the cardiovascular risk of rofecoxib correlates with elevations in pro-BNP [95].
Table 2
Cardiovascular disease and medications that cause fluid retention
| Medication | Associated with atherosclerotic cardiovascular disease? | Associated with venous thromboembolic disease? |
| Cyclo-oxygenase-2 inhibitors | yes [71–76] | contradictory data [77, 78] |
| Non-steroidal antiflammatory drugs | yes [79–82] | yes [83, 84] |
| Corticosteroids | yes [82] | yes [85] |
| Hormone replacement therapy | yes [86, 87] | yes [87] |
| Oral contraceptives | yes [88] | yes [83, 89] |
| Insulins | yes [90] | no data available |
| Sulfonylureas | yes [91, 92] | no data available |
| Gabapentin | yes [93] | yes [93] |
| Pregabalin | yes [93] | yes [93] |
| Androgen therapy | contradictory data [96–98] | yes [98] |
| Pioglitazone | no [111, 112] | no data available |
| Rosiglitazone | yes [113] | no data available |
Androgen therapy promotes fluid retention but the research literature is mixed concerning cardiovascular risk. Retrospective studies have documented that testosterone supplementation is associated with a reduction of cardiovascular risk while others have documented the opposite [96, 97]. A prospective study found that testosterone replacement therapy has no effect upon atherosclerotic cardiovascular events but increases the incidence of pulmonary emboli [98].
6Antihypertensive medications
Several categories of antihypertensive medications cause fluid retention but improve cardiovascular outcomes. For calcium channel blockers (CCBs), alpha receptor antagonists and hydralazine, cardiovascular outcomes are more dependent upon BP reduction than fluid retention. Even so, if fluid retention contributes significantly to adverse cardiovascular outcomes, one would expect better cardiovascular outcomes with diuretics than with CCBs. This is not the case. Accordingly, either the hypothesis that fluid retention contributes to adverse cardiovascular events is flawed or else other factors play a more important role.
Antihypertensive medications have different effects upon lipids and BP variability. It is possible that these properties outweigh the effects of fluid retention. Diuretics raise cholesterol, angiotensin converting enzyme (ACE) inhibitors have a neutral effect on cholesterol in non-diabetic patients, and CCBs have a neutral effect on cholesterol [99]. Increased BP variability is associated with adverse cardiovascular outcomes [100]. Amlodipine reduces BP variability more than other CCBs, and CCBs reduce BP variability more than other classes of antihypertensive medications [101–103]. Non-loop diuretics reduce BP variability while ACE inhibitors, angiotensin receptor blockers (ARBs) and beta-blockers increase BP variability [101–103].
In the CAMELOT trial, the frequency of adverse cardiovascular outcomes was lower in the amlodipine cohort than the enalapril cohort [104]. The combination of benazepril and amlodipine in the ACCOMPLISH trial was more effective than the combination of benazepril and hydrochlorthiazide (HCTZ) in reducing adverse cardiovascular events despite slightly greater BP lowering in the benazepril-HCTZ group [105]. In addition, INSIGHT demonstrated equivalence in cardiovascular outcomes comparing nifedipine versus a diuretic while NORDIL found that diltiazem is more effective than diuretics or beta-blockers at preventing strokes [106, 107].
Not all clinical trials are consistent with a hierarchy of antihypertensive medications based upon BP variability and lipid properties. ACE inhibitors are more effective than non-amlodipine CCBs at preventing coronary heart disease, heart failure and major cardiovascular events [108]. Studies have shown that non-amlodipine CCBs are inferior to other types of antihypertensive drugs as first-line agents in reducing the risks of several major complications of hypertension [109]. In the ALLHAT trial, chlorthalidone was found to be comparable or superior to lisinopril and amlodipine in terms of several adverse cardiovascular events but BP reductions were not equivalent among the chlorthalidone, lisinopril and amlodipine cohorts [110].
7Thiazolidinediones
Pioglitazone and rosiglitazone both cause fluid retention but have discordant effects upon cardiovascular outcomes (Table 2). Pioglitazone decreases the risk of myocardial infarcts and strokes while rosiglitazone increases the risk of myocardial infarcts [111–113]. Rosiglitazone also increases the risk of cardiovascular death to a degree that borders on significance [113]. The favorable effect of pioglitazone upon cardiovascular outcomes contradicts the hypothesis that fluid retention increases cardiovascular risk. Consequently, either the hypothesis is flawed or else other factors play more important roles.
Pioglitazone and rosiglitazone improve glycemic control and modestly decrease BP [114, 115]. The discordant cardiovascular effects of pioglitazone and rosiglitazone may be a result of their differing effects upon lipids [114]. Pioglitazone has a neutral effect upon low-density lipoprotein (LDL) -cholesterol whereas rosiglitazone raises LDL-cholesterol [114]. Pioglitazone lowers triglyceride levels whereas rosiglitazone has a neutral effect upon triglycerides [114].
It is possible that for both pioglitazone and rosiglitazone, BP lowering and improved glycemic control favorably influence cardiovascular outcomes, fluid retention negatively influences cardiovascular outcomes, and lipid effects are responsible for their divergent cardiovascular effect. For pioglitazone, it may be that the combined effect of its BP, glycemic, fluid and lipid properties decreases adverse cardiovascular outcomes. For rosigltiazone, it may be that the combined effect of these properties increases adverse cardiovascular outcomes.
8Implications for pharmaceutical industry and regulators
The possibility that fluid retention contributes to cardiovascular risk may have relevance for the pharmaceutical industry and for regulatory agencies such as the Food and Drug Administration (FDA). Since hypertension and elevated LDL-cholesterol are recognized cardiovascular risk factors, the FDA could require BP data, cholesterol data and fluid retention data for new drug applications. This might allow the FDA to predict the cardiovascular risk of medications. When warranted, cardiovascular safety data could be required prior to regulatory approval or, alternatively, the FDA could mandate an appropriate warning on the drug label.
9Empirical evidence of turbulence
The cardiovascular effects of pioglitazone and calcium channel blockers cast doubt upon the hypothesis that fluid retention is a cardiovascular risk factor. Absence of empirical data is an additional limitation. Four-dimensional magnetic resonance imaging (MRI), as well as vector flow Doppler ultrasound, have the capability to quantify turbulence of blood flow [116, 117]. These technologies could be used to clarify the effect of fluid retention. Measuring turbulence of blood flow before and after fluid administration, or measuring turbulence of blood flow before and after prescribing medications that cause fluid retention, would enable researchers to determine the effect of fluid retention.
10Conclusion
In summary, biochemicals and biomechanical forces trigger endothelial dysfunction but only biomechanics can explain why atherosclerosis is localized to arterial branch points, arterial bifurcations and the curved segments of great arteries. These are the regions that blood flows turbulently. Turbulence promotes endothelial dysfunction by reducing shear stress upon endothelial cells. The endothelial glycocalyx mediates the effect of shear stress upon the endothelium.
A mathematical analysis of cardiovascular hemodynamics demonstrates that fluid retention increases turbulence of blood flow. However, there is no empirical evidence of this relationship. Medical conditions that increase fluid retention are associated with increased risk of arterial and venous thromboembolic cardiovascular disease. Likewise, many medications that cause fluid retention either increase cardiovascular risk or are associated with increased cardiovascular risk. While the favorable cardiovascular effects of pioglitazone and calcium channel blockers contradict the hypothesis that fluid retention is a cardiovascular risk factor, these medications have properties that may compensate for fluid retention.
The primary limitation of the hypothesis that fluid retention is a cardiovascular risk factor is the absence of empirical data demonstrating that fluid retention increases turbulence of blood flow. Four dimensional MRI and vector flow Doppler ultrasound technologies could be utilized to settle the matter.
References
[1] | Stary HC . Natural history and histological classification of atherosclerosis lesions: An update. Arterioscler Thromb Vasc Biol. (2000) ;20: :1177–8. |
[2] | Virmani , Kolodgie FD , Burke AP , Farb A , Schwartz SM . Lessons from sudden coronary death: A comprehenisve morphological classifcation scheme for atherosclerotic lesions. Arterioscler Throm Vasc Biol. (2000) ;1262–75. |
[3] | Prandoni P , Bilora F , Marchiori A , Bernardi E , Petrobelli R , Lensing WA , et al. An association between atherosclerosis and venous thrombosis. N Engl J Med. (2003) ;348: :1435–41. |
[4] | Ageno W , Becattini C , Brighton T , Selby R , Kamphuiser PW . Cardiovascular risk factors and venous thromboembolism: A meta-analysis. Circulation. (2006) ;117: :93–102. |
[5] | Gimbrone MA and Garcia-Cardeňa G . Vascular endothelium, hemodynamics, and the pathobiology of atherosclerosis. Cardiovasc Pathol. (2013) ;22: :9–15. |
[6] | Hansson GK . Inflammation, atherosclerosis and coronary artery disease. N Eng J Med. (2005) ;352: :1685–95. |
[7] | Akarasereenont P , Techatraisak K , Thaworn A , Chotewuttakorn . The expression of COX-2 in VEGF-treated endothelial cells is mediated by tyrosine kinase. Mediators Inflamm. (2002) ;11: :17–22. |
[8] | Uraoka M , Ikeda K , Nakagawa Y , Koide M , Akakabe Y , Nakano-Kurimoto R , et al. Prorenin induces ERK activation in endothelial cells to enhance neovascularization independently of the renin-angiotensin system. Biochem Biophys Res Commun. (2009) ;390: :1202–7. |
[9] | Das Dores Lopes P , de Assis N , de Araūj F , Maquilon Moreno OL , de Oliveira Sant Jorge KT , Mirand E Castor MG , et al. COX/;iNOS dependence for angiotension-II-induced endothelial dysfunction. Peptides. (2022) ;157: :170863. |
[10] | De Nigris V , Pujadas G , La Sala L , Testa R , Genovese S , Ceriello A . Short-term high glucose exposure impairs insulin signaling in endothelial cells. Cardiovasc Diabetel. (2015) ;14: :114. DOI: 10.1186/s12933-015-0278-0. |
[11] | Abumrad NA , Cabodevilla AG , Samovski D , Pietka T , Basu D , Goldberg IJ . Endothelial cell receptors in tissue lipid uptake and metabolism. Circ Res. (2021) ;128: :433–50. |
[12] | Andersson H , Garscha U , Brittebo E . Effects of PCB126 and 17β-oestradiol on endothelium-derived vasoactive factors in human endothelial cells. Toxicology. (2011) ;28S: (1-2):46–56. |
[13] | Tamura M , Deb S , Sebastian S , Okamura K , Bulun SE . Estrogen up-regulates cyclooxygenase-2 via estrogen receptor in human uterine microvascular endothelial cells. Fertil Steril. (2004) ;81: :1351–6. |
[14] | You Y , Tan W , Guo Y , Luo M , Shang F-F , Xia Y , et al. Progestone promotes endothelial nitric oxide synthase expression through enhancing nuclear progesterone receptor-SP-1 formation. Am J Physiol Heart Circ Physiol. (2020) ;319: :H341–8. |
[15] | Faulkner JL , Belin de Chantemèle EJ . Mineralocorticoid receptor and endothelial dysfunction in hypertension. Curr Hypertens Rep. (2019) ;21: :78. |
[16] | Syeda F , Grosjean J , Houliston RA , Keogh RJ , Carter TD , Paleolog E , et al. Cyclooxygenase-2 induction and prostacyclin release by protease-activated receptors in endothelial cells require cooperation between mitogen-activated protein kinase and NF-κB pathways. J Biol Chem. (2006) ;281: :11792–804. |
[17] | Hitomi H , Liu G , Nishiyama A . Role of (pro)renin receptor in cardiovascular cells from the aspect of signaling. Front Bioscience. (2010) ;2: :1246–9. |
[18] | Topper JN , Cai J , Falb D . Gimbrione MA. Identification of vascular endothelial genes differentially repsonsive to fluid mechanical stimule: Cycclooxygenase-2, manganese super oxide dismutase, and endothelial cell nitric oxide synthase are selectively up-regulated by steady laminar shear stress. Proc Natl Acad Sci. (1996) ;93: :10417–22. |
[19] | Davies PF . Flow-mediated endothelial mechanotransduction. Physiol Rev. (1995) ;75: :519–560. |
[20] | Gimbrone MA , Garcia-Cardeňa G . Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res. (2016) ;118: :620–36. |
[21] | Ross R , Glomset JA . The pathogenesis of atherosclerosis (first of two parts). N Engl J Med. (1976) ;295: :369–77. |
[22] | Silkworth JB , McLean B , Stehbens . The effect of hypercholesterolemia on aortic endothelium studied en face. Athersclerosis. (1975) ;22: ;335–33. |
[23] | Davies PF , Bowyer DE . Scanning electron microscopy: Arterial endothelial integrity after fixation at physiological pressure. Atherosclerosis. (1975) ;21: :463–69. |
[24] | Stehbens WE . Hemodynamics and atherosclerosis. Biorheology. (1982) ;95–101. |
[25] | Caro CG , Fitz-Gerald JM , Schroter RC . Atheroma arterial wall shear. Observation, correlation and proposal of a shear dependent mass transfer mechanism for atherogenesis. Proceedings fo the Royal Society of London Series B., Biological Sciences. (1971) ;109–59. |
[26] | Foote CA , Soares RN , Ramirez-Perez FI , Ghiarone T , Aroor A , Manrique-Acevedo C , et al. Endothelial glycocalyx. Compr Physiol. (2023) ;12: :3781–811. |
[27] | Zhao F , Zhong L , Luo Y . Endothelial glycocalyx as an important factor in composition of blood-brain barrier. CNS Neurosci Ther. (2021) ;27: :26–35. |
[28] | Secomb TW , Hsu R , Pries AR . Effect of the endothelial surface layer on transmission of fluid shear stress to endothelial cells. Biorheology. (2001) ;38: :143–50. |
[29] | Weinbaum S , Zhang X , Han Y , Vink H , Cowin SC . Mechanotransduction and flow across the endothelial glycocalyx. Proc Natl Acad Sci-USA. (2003) ;100: :7988–95. |
[30] | Fan J , Sun Y , Xia Y , Tarbell JM , Fu BM . Endothelial surface glycocalyx (ESG) components and ultra-structure revealed by stochastic optical reconstruction microscopy (STORM). Biorheology. (2019) ;56: (2-3), 77–88. |
[31] | Dragovich MA , Chester D , Fu BM , Wu C , Xu Y , Goligorsky MS , Zhang XF . Mechanotransduction of the endothelial glycocalyx mediates nitric oxide production through activation of TRP channels. Am J Physiol Cell Physiol. (2016) ;311: :C846–53. |
[32] | Gouverneur M , Spaan MA , Pannekoek H , Fontijn RD , Vink H . Fluid shear stress stimulates incorporation of hyaluronan into endothelial cell glycocalyx. Am J Physiol Circ Physiol. (2006) ;290: :H458–52. |
[33] | Wang G , Kostidis S , Tiemeier GL , Sol W , de Vries MR , Giera M , et al. Shear stress regulation of endothelial glycocalyx structure is determined by glucobiosynthesis. Arterioscler Thromb Vasc Biol. (2020) ;40: :350–64. |
[34] | Psefteli PM , Kitscha P , Vizcay G , Fleck R , Chapple SJ , Mann GE , et al. Glycocalyx sialic acids regulate Nrf2-mediated signaling by fluid shear stress in human endothelial cells. Redo biology. (2021) ;38: :101816. |
[35] | van de Berg RM , Spaan JA , Rolf TM , Vink H . Atherogenic region and diet diminish glycocalyx dimension and increase intima-to-media ratios at murine carotid artery bifurcation. Am J Physiol Circ Physiol. (2006) ;290: :H915–20. |
[36] | Cancel LM , Ebong EE , Mensah S , Hirschberg C , Tarbell JM . Endothelial glycocalyx, apoptosis and inflammation in an atherosclerotic mouse model. Atherosclerosis. (2016) ;252: :136–46. |
[37] | Guyton AC , Granger HJ , Coleman TG . Autoregulation of the total systemic circulation and its relation to control of cardiac output and arterial pressure. Circ Res. (1971) ;28: (Suppl 1):93–7. |
[38] | Kumar A , Anel R , Bunnell E , Habet K , Neumann A , Wolff D , et al. Effect of large volume infusion on left ventricular volumes, performance and contractility parameters in normal volunteers. Intensive Care Med. (2004) ;30: :1361–9. |
[39] | Blankfield RP . Implications of calculated intravascular volume changes upon atherosclerotic cardiovascular disease. Clin Hemorheol Microcirc. (2008) ;38: :75–81. |
[40] | Blankfield RP . Calculated effect of fluid retention upon velocity of blood flow and turbulence: Implications for atherosclerosis. Clin Hemorheol Microcirc. (2011) ;47: :79–86. |
[41] | Hjalmarsson C , Fu M , Sandstrőm TZ , Schaufelberger M , Ljungman M , Andersson B , et al. Risk of stroke in patients with heart failure and sinus rhythm: Data from the Swedish Heart Failure Registry. ESC Heart Fail. (2021) ;8: :85–94. |
[42] | Greenberg B , Peterson ED , Berger JS , Laliberté F , Zhao Q , Germain G , et al. Ejection fraction, B-type natriuretic peptide and risk of stroke and acute myocardial infarction among patients with heart failure. Clin Cardiol. (2019) ;42: :277–84. |
[43] | Berger JS , Peterson E , Laliberté F , Germain G , Lejeune D , Schein J , et al. Risk of ischemic stroke in patients newly diagnosed with heart failure: Focus on patients without atrial fbrillation. J Cardiac Fail. (2019) ;25: (6), 436–47. |
[44] | Kang S-H , Kim J , Park JJ , Oh I-Y , Yoon C-H , Kim H-J , et al. Risk of stroke in congestive heart failure with and without atrial fbrillation. Int J Cardiol. (2017) ;248: :182–7. |
[45] | Fanola CL , Norby F , Shah AM , Chang PP , Lutsey PL , Rosamond WD , et al. Incident heart failure and long-term risk for venous thromboembolism. J Am Coll Cardiol. (2020) ;75: (2):148–58. |
[46] | Xiong J , Xu W , Huang H , Bian J , Wang A , Bai Y , et al. Cirrhosis and risk of stroke: A systematic review and meta-analysis. Atherosclerosis. (2018) ;275: :296–303. |
[47] | Ambrosino P , Tarantino L , Di Minno G , Paternoster M , Graziano V , Graziano V , et al. The risk of venous thromboembolism in patients with cirrhosis: A systematic review and meta-analysis. Thromb Haemost. (2017) ;117: :139–48. |
[48] | Go AS , Tan TC , Chertow GM . Primary nephrotic syndrome and risks of ESKD, cardiovascular events, and death: The Kaiser Permanente Nephrotic Syndrome study. J Am Soc Nephrol. (2021) ;32: :2303–14. |
[49] | Kerlin BA , Ayoob R , Smoyer WE . Epidemiology and pathophysiology of nephrotic syndrome-associated thromboembolic disease. Clin J Am Soc Nephrol. (2012) ;7: :513–20. |
[50] | Ning Y , Cheng YJ , Liu LJ , Sara JDS , Cao ZY , Zheng WP , et al. What is the association of hypothyroidism with risks of cardiovascular events and mortality? A meta-analysis of 55 cohort studies involving 1,898,314 participants. BMC Med. (2017) ;15: :1–15. |
[51] | Danescu LG , Badshah A , Danescu C , Janjua M , Marandici AM , Matta F , et al. Venous thromboembolism in patients hospitalized with thyroid dysfunction. Clin Appl Thromb Hemost. (2009) ;15: :676–80. |
[52] | Cai X , Zhang Y , Li M , Hy Wu J , Mai L , Li J , et al. Association between prediabetes and risk of all cause mortality and cardiovascular disease: Updated meta-analysis. BMJ. (2020) ;5: ;370:m2297. doi: 10.1136/bmj.m2297. |
[53] | Shah N , Yiggi HK , Concato J , Mohsenin V . Obstructive sleep apnea as a risk factor for coronary events or cardiovascular death. Sleep Breath. (2010) ;14: :131–6. |
[54] | Lippi G , Mattiuzzi C , Franchini M . Sleep apnea and venous thromboembolism. A systematic review. Thrombo Haemost. (2015) ;114: :958–63. |
[55] | Byrd JB , Turcu AF , Auchus RJ . Primary aldosteronism: A practical approach to diagnosis and management. Circulation. (2018) ;138: :823–5. |
[56] | Capatina C , Fleseriu M . Thromboembolic disease in hypercortisolism. Curr Opin Endocrinol Diabetes Obes. (2021) ;28: :330–6. |
[57] | Ageno W , Becattini C , Brighton T , Selby R , Kamphuisen P W . Cardiovascular risk factors and venous thromboembolism: A meta-analysis. Circulation. (2008) ;117: :93–102. |
[58] | Bai J , Ding X , Du X , Zhao X , Wang Z , Ma Z . Diabetes is associated with increased risk of venous thromboembolism:A systematic review and meta-analysis. Thromb Res. (2015) ;135: (1), 90–5. |
[59] | Bell EJ , Folsom AR , Lutsey PL , Selvin E , Zakai NA , Cushman M , Alonso A . Diabetes mellitus and venous thromboembolism: A systematic review and meta-analysis. Diabetes Res Clin Pract. (2016) ;111: :10–8. |
[60] | Hu S , Tan J-S , Hu M-J , Guo T-T , Chen L , Hua L , et al. The causality between diabetes and venous thromboembolism: A bidirectional two-sample Mendelian randomization study. Thromb Haemost. (2023) ;123: (9):913–9. doi: 10.1055/a-2040-4850. |
[61] | Rentsch CT , Garfield V , Mathur R , Eastwood SV , Smeeth L , Chaturvedi N , Bhaskaran K . Sex-specific risks for cardiovascular disease across glycaemic spectrum: A population-based cohort study using the UK Biobank. Lancet Reg Health Eur. (2023) ;32: :100693. doi: 10.1016/j.lanepe.2023.100693. eCollection 2023 SePMID: 37671124. |
[62] | Fong JK , Desai R , Faisaluddin M , Parekh T , Mahmood A , Shah V , et al. Sex disparities in cardiovascular disease outcomes among geriatric patients with prediabetes. Prim Care Diabetes. (2021) ;15: :95–100. |
[63] | Diekman MJ , Doulabi B , Platvoet-Ter Shiphorst M , Fliers E , Bakker O , Wiersinga WM . The biological relevance of thyroid hormone receptors in immortalized human umbilical vein endothelial cells. J Endocrinol. (2001) ;168: :427–33. |
[64] | Verhovez A , Williams TA , Morello F , Monticone S , Brizzi MF , Dentelli P , et al. Aldosterone does not modify gene expression in human endothelial cells. Horm Metab Res. (2012) ;44: :234–8. |
[65] | He M , Zhang L , Shao Y , Wang X , Huang Y . Inhibition of renin/prorenin receptor attenuated mesangial cell proliferation and reduced associated fibrotic factor release. Eur J Pharmacol. (2009) ;606: :155–61. |
[66] | Ma Y , He FJ , Sun Q , Yuan C , Kineker LM , Curhan GC , et al. 24-hour urinary sodium and potassium excretion and cardiovascular risk. N Engl J Med. (2022) ;386: :252–63. |
[67] | Mills KT , Chen J , Yang W , Appel LJ , Kusek JW , Alper A , et al. Sodium excretion and the risk of cardiovascular disease in patients with chronic kidney disease. JAMA. (2016) ;315: :2200–10. |
[68] | Mentes A , O’Donnell M , Rangarajan S , McQueen M , Dagenais G , Wielgosz A , et al. Urinary sodium excretion, blood pressure, cardiovascular disease, and mortality: A community-level prospective epidemiologyical cohort study. Lancet. (2018) ;392: :496–506. |
[69] | Wang TJ , Larson MG , Levy D , Benjamin EJ , Leip EP , Omland T , et al. Plasma natriuretic peptide levels and the risk of cardiovascular events and disease. N Engl J Med. (2004) ;655–63. |
[70] | Kistorp C , Raymond I , Pedersen F , Gustafsson F , Faher J , Hildbrandt P . N-terminal pro-brain natriuretic peptide, C-reactive protein, and urinary albumin levels as predictors of mortality and cardiovascular events in older adults. JAMA. (2005) ;293: :1609–16. |
[71] | Bombardier C , Lane L , Reicin A , Shapiro D , Burgos-Vargas R , Davis B , et al. Comparison of upper gastrointestinal toxicity of rofexoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med. (2000) ;343: :1520–8. |
[72] | Solomon SD , McMurray JJV , Pferrer MA , Wittes J , Fowler R , Finn P , et al. Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N Engl J Med. (2005) ;152: :1071–80. |
[73] | Nussmeier NA , Whelton AA , Brown MT , Langford RM , Hoeft A , Parlow JL , et al. Complications of the COX-2 inhibitors parecoxib and valdecoxib after cardiac surgery. N Engl J Med. (2005) ;352: :1081–91. |
[74] | McGettigan P , Henry D . Cardiovascular risk and inhibition of cyclooxygenase: A systemic review of the observational studies of selective and non-selective inhibitors of cyclooxygenase. JAMA. (2006) ;1633–44. |
[75] | Juni P , Nartey L , Reichenbach S , Sterchi R , Dieppe PA , Egger M . Risk of cardiovascular events and rofecoxib: Cumulative meta-analysis. Lancet. (2004) ;364: :2021–9. |
[76] | Bertagnolli MM , Eagle CJ , Zauber AN , Redston M , Solomon SD , Kim K , et al. Celecoxib for the prevention of sporadic colorectal adenomas. N Engl J Med. (2006) ;355: :873–84. |
[77] | Goy J , Paikin J , Crowther M . Rofecoxib does not appear to increase the risk of venous thromboembolism: A systematic review of the literature. Thromb Res. (2014) ;134: (5), 997–1003. |
[78] | Kinsey TL , Sturmer T , Funk MJ , Poole C , Simpson RJ , Glynn RJ . Incidence of venous thromboembolism following initiation of non-steroidal anti-inflammatory drugs in U.S. women. Rheumatology. (2020) ;59: :2502–11. |
[79] | McKearney PA , Baigent C , Godwin J , Halls H , Emberson JR , Patrono C . Do selective cyclo-oxygenase inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherosclerosis? BMJ (2006) ;332: :1302–8. |
[80] | Antman EM , Bennett JS , Daugherty A , Furberg C , Roberts H , Taubert KA . Use of nonsteroidal antiinfammatory drugs: An update for clinicians: A scientifc statement from the american heart association. Circulation. (2007) ;115: (12):1634–42. |
[81] | Cooper C , Chapurlat R , Al-Daghri N , Herrero-Beaumont G , Bruyere O , Fannou F , et al. Safety of oral non-selective non-steroidal anti-infammatory drugs in osteoarthritis: What does the literature say? Drugs Aging. (2019) ;36: (S1):15–24. |
[82] | Roubille C , Richer V , Starnino T , McCourt C , McFarlane A , Fleming P , et al. The effects of tumour necrosis factor inhibitors, methotrexate, non-steroidal anti-inflammatory drugs and corticosteroids on cardiovascular events in rheumatoid arthritis, psoriasis and psoriatic arthritis: A systematic review and meta-analysis. Ann Rheum Dis. (2015) ;74: :480–9. |
[83] | Meaidi A , Mascolo A , Sessa M , Toft-Petersen AP , Skals R , Gerds TA , et al. Venous thromboembolism with use of hormonal contraception and non-steroidal anti-inflammatory drugs: Nationwide cohort study. BMJ. (2023) ;382: :e074450. doi: 10.1136/bmj-2022-074450. |
[84] | Ungprasert RP , Srivali N , Wijarnpreecha K , Charoenpong P , Knight EL . Non-steroidal anti-inflammatory drugs and risk of venous thromboembolism: A systematic review and meta-analysis. Rheumatology. (2015) ;54: :736–42. |
[85] | Waljee AK , Rogers MA , Lin P , Singal AG , Stein JD , Marks RM , Ayanian JZ , Nallamothu BK . Short term use of oral corticosteroids and related harms among adults in the United States: Population based cohort study. BMJ. (2017) ;357: :j1415. doi: 10.1136/bmj.j1415. |
[86] | Anderson GL , Limacher M , Assaf AR , Bassford T , Beresford SAA , Black H , et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: The Women’s Health Initiative randomized controlled trial. JAMA. (2004) ;291: (14):1701–12. |
[87] | Rossouw JE , Anderson GL , Prentice RL , LaCroix AZ , Kooperberg C , Stefanick ML , et al. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results From the Women’s Health Initiative randomized controlled trial. JAMA. (2002) ;288: :321–33. |
[88] | Roach REJ , Helmerhorst FM , Lijfering WM , Stijnen T , Algra A , Dekkers OM . Combined oral contraceptives: The risk of myocardial infarction and ischemic stroke. Cochrane Database Syst Rev. (2015) . https://doi.org/10.1002/14651858.CD011054.pub2. |
[89] | Dragoman MV , Tepper NK , Fu R , Curtis KM , Chou R , Gaffield . A systematic review and meta-analysis of venous thrombosis risk among users of combined oral contraception. Gynecology. (2018) ;141: (3):287–94. DOI: 10.1002/ijgo.12455. |
[90] | Roumie CL , Greevy RA , Grijalva CG , Hung AM , Liu X , Murff H , et al. Association between intensification of metformin treatment with insulin vs sulfonylureas and cardiovascular events and all-cause mortality among patients with diabetes. JAMA. (2014) ;311: :2288–96. |
[91] | Pantalone KM , Kattan MW , Yu C , Wells BJ , Arrigain S , Jain A , et al. The risk of developing coronary, disease or congestive heart failure and overall mortality in type 2 diabetic patients receiving rosiglitazone, pioglitazone, metformin or sulfonylureas: A retrospective analysis. Acta Diabetol. (2009) ;46: :145–54. |
[92] | Schramm TK , Gislason GH , Vaag A , Rasmussen JN , Folke F , Hansen ML , et al. Mortality and cardiovascular risk associated with different insulin secretagogues compared with metformin in type 2 diabetes, with or without a previous myocardial infarction: A nationwide study. Eur Heart J. (2011) ;32: (15);1900–8. |
[93] | Pan Y , Davis PB , Kaebler DC , Blankfield RP , Xu R . Cardiovascular risk of gabapentin and pregabalin in patients with diabetic neuropathy. Cardiovasc Diabetol. (2022) ;21: :170. doi: 10.1186/s12933-022-01610-9. |
[94] | Monakier D , Maes M , Klutstein MW , Balkin JA , Rudensky B , Meerkin D , et al. Rofecoxib, a COX-2 inhibitor, lowers C-reactive protein and interleukin-6 levels in patients with acute coronary syndromes. Chest. (2004) ;125: :1610–5. |
[95] | Brune K , Katus HA , Moecks J , Spanuth E , Jaffe AS , Giannitis E , et al. N-terminal Pro-B-type natriuretic peptide concentrations predict the risk of cardiovascular adverse events from antiinflammatory drugs: A pilot trial. Clin Chem. (2008) ;54: :1149–57. |
[96] | Basaria S , Gagliano-Jucá . Testosterone replacement therapy and cardiovascular risk. Nat Rev Cardiol. (2019) ;16: :555–74. |
[97] | Kloner RA , Carson C , Dobs A , Kopecky S , Mohler ER . Testosterone and cardiovascular disease. J Am Coll Cardiol. (2016) ;67: :545–7. |
[98] | Lincoff AM , Bhasin S , Flevaris P , Mitchell LM , Basaria S , Boden WE , et al. Cardiovascular safety of testosterone-replacement therapy. N Eng J Med. (2023) ;389: :107–17. |
[99] | Kasiske BL , Ma JZ , Kalil RSN , Louis TA . Effects of antihypertensive therapy on serum lipids. Ann Int Med. (1995) ;122: :133–41. |
[100] | Stevens SL , Wood S , Koshiaris C , Law K , Glasziou P , Stevens P , et al. Blood pressure variability and cardiovascular disease: Systematic review and meta-analysis. BMJ. (2016) ;354: :i4098. |
[101] | Webb AJS , Fischer U , Mehta Z , Rothwell . Effects of antihypertensive-drug class on interindividual variation in blood pressure and risk of stroke: A systematic review and meta-analysis. Lancet. (2010) ;375: :906–15. |
[102] | de la Sierra A . Blood pressure variability as a risk factor for cardiovascular disease: Which antihypertensive agents are more effective? J Clin Med. (2023) ;12: (19):6167. |
[103] | Zhang L , Yang J , Li L , Liu DD , Xie XP , Dong P , et al. Comparison of amlodipine versus other calcium channel blockers on blood pressure variability in hypertensive patients in China: A retrospective propensity score-matched analysis. J Comp Eff Res. (2018) ;7: :651–60. |
[104] | Nissen SE , Tuzcu EM , Libby P , Thompson PD , Ghali M , Garza D , et al. Effect of antihypertensive agents on cardiovascular events in patients with coronary artery disease and normal blood pressure: The CAMELOT study: A randomized controlled trial. JAMA. (2004) ;292: :2217–26. |
[105] | Jamerson K , Weber MA , Bakris GL . Benazepril plus amlodipine of hydrochlorthiazide for hypertension in high-risk patients. N Engl J Med. (2008) ;359: :2417–28. |
[106] | Brown MJ , Palmer CR , Castaigne A , de Leeuw PW , Mancia G , Rosenthal T , et al. Morbidity and mortality in patients randomized to double-blind treatment with long-acting calcium-channel blocker or diuretic in the International Nifedipine GITS study: Intervention as a Goal in Hypertension Treatment (INSIGHT). Lancet. (2000) ;356: :366–72. |
[107] | Hansson L , Hedner T , Lund-Johansen P , Kjeldsen EJ , Lindholm LH , Syvertsen JO , et al. Randomised trial of effects of calcium antagonists compared with diuretics and beta-blockers on cardiovascular morbidity and mortality in hypertension: The Nordic Diltiazem (NORDIL) study. Lancet. (2000) ;356: :359–65. |
[108] | Blood Pressure Lowering Trialists Collaboration. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: Results of prospectively designed overviews of randomised trials. Lancet. (2000) ;355: :1955–64. |
[109] | Pahor M , Psaty BM , Alderman MH , Applegate WE , Williamson JD , Cavazzini C , et al. Health outcomes associated with calcium antagonists compared with other first-line antihypertensive therapies: A meta-analysis of randomized controlled trials. Lancet. (2000) ;356: :1949–54. |
[110] | The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research GrouMajor outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic. The antihypertensive and ipid-lowering treatment to prevent heart attack trial (ALLHAT). JAMA. (2002) ;288: :2981–97. |
[111] | de Jong M , van der Worp B , van der Graaf Y , Visseren FLJ , Westerink J . Pioglitazone and the secondary prevention of cardiovascular disease: A meta-analysis of randomized-controlled trials. Cardiovasc Diabetol. (2017) ;16: :134. |
[112] | Zhou Y , Huang Y , Ji X , Wang X , Shen L , Wang Y . Pioglitazone for the primary and secondary prevention of cardiovascular and renal outcomes in patients with or at high risk of type 2 diabetes mellitus: A meta-analysis. J Clin Endocrinol Metab. (2020) ;105: :dgz252. |
[113] | Nissen SE , Wolski K . Efect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. (2007) ;356: :2457–71. |
[114] | Qayyum R , Adomaityte J . A meta-analysis of thiazolidinediones on blood pressure. J Clin Hypertens. (2006) ;8: :19–28. |
[115] | Chiquette E , Ramirez G , DeFronzo R . A meta-analysis comparing the effect of thiazolidinediones on cardiovascular risk factors. Arch Int Med. (2004) ;164: :2097–104. |
[116] | Ha H , Ziegler M , Welander M , Bjarnegard N , Carlhall C-J , Lindengerger M , et al. Age-related vascular changes affect turbulence in aortic blood flow. Front Physiol. (2018) ;9: :36. doi: 10.3389/fphys.2018.00036. eCollection 2018. |
[117] | Hong S , Dong Y , Song D , Liu M , Gao W , Li W , et al. Precise evaluation of blood flow patterns in human carotid bifurcation based on high-frame-vector flow imaging. J Clin Ultrasound. (2023) ;51: :1070–7. |


