
Cytokine absorption in critically ill old COVID-19 patients with renal failure: A retrospective analysis of 503 intensive care unit patients
Abstract
BACKGROUND:
COVID-19 is associated with cytokine release in critical disease states. Thus, cytokine absorption has been proposed as a therapeutic option. This study investigated the influence of cytokine absorption on mortality in old critical patients with COVID-19 and renal failure admitted to intensive care units (ICU).
METHODS:
This retrospective analysis of a prospective international observation study (the COVIP study) analysed ICU patients≥70 years with COVID-19. Data on Sequential Organ Failure Assessment (SOFA) score, clinical frailty scale (CFS), ICU therapy details including renal replacement therapy (RRT) with/without cytokine absorption were collected. The cytokine absorption group was compared to patients receiving RRT without cytokine absorption
RESULTS:
Among 3927 patients, 503 received RRT; among them 47 patients were treated with cytokine absorption. Mortality rates were high in both groups with increased rates in the cytokine group for ICU mortality and 30-day mortality, but not for 3-month mortality. Logistic regression analysis indicated that SOFA-score, but not cytokine absorption was associated with mortality.
CONCLUSIONS:
Critical COVID-19 patients with renal failure treated with cytokine absorption showed higher short term mortality rates when compared to patients with renal replacement therapy alone. Mortality is associated with disease severity, but not cytokine absorption in a multivariate analysis.
1Background
The COVID-19 pandemic has led to many millions confirmed cases and over 6 million associated deaths. Various therapeutic tools have been studied to improve outcomes of critically ill patients with COVID-19 [1, 2]. Pharmacological approaches ranged from hydroxychloroquine or anti-retroviral agents to “antibody cocktails“, such as REGN-COV-2, or corticosteroids like dexamethasone [1, 3, 4]. Pro-inflammatory markers such as C-reactive protein or D-dimer have been associated with severe courses of COVID-19 and poor outcome [5–7]. Moreover, an excessive release of cytokines, such as Interleukin 1 (IL-1), Interleukin 6 (IL-6), or tumor necrosis factor alpha (TNF-α), resulting in an excessive immune response has been described to cause a severe course of disease including acute respiratory distress syndrome (ARDS) [8, 9]. This uncontrolled release of cytokines leads to extensive systemic effects, such as vasodilatation and hyperinflammation, resulting in haemodynamic instability, endothelium and glycocalyx damages, and capillary leakage [10, 11]. Thus, cytokine level modulation became the focus of research as a potential treatment option to prevent severe disease courses and to reduce mortality in patients with a COVID-19 disease [9]. Besides pharmacological approaches, cytokine absorption therapy aiming to reduce the burden of immunological responses were tested as a promising therapeutic alternative, especially for severely ill patients [8, 12–14].
The rationale for the use of such devices is the immunomodulation by an amplified transmembrane clearance and an unselective or selective absorption of potentially harmful agents such as cytokines [15]. The filters consist of specific polymers or contain particular polycationic layers and can be applied in patients with renal failure receiving renal replacement therapy (RRT) by being added to the dialysis setting [16]. So far, a few clinical studies and two randomised controlled trials investigating cytokine filters as a possible treatment option in critically ill COVID-19 patients are available [14, 17–21].
The aim of the present study was to evaluate cytokine absorption use and its association with clinical outcomes in a real-world older multinational patient cohort, suffering from severe COVID-19 disease with renal failure.
2Methods
2.1Design and settings
This study was part of the Very old Intensive care Patients (VIP) project, which is registered on ClinicalTrials.gov (ID: NCT04321265). Furthermore, it was endorsed by the European Society of Intensive Care Medicine (ESICM, https://www.vipstudy.org). The goal of this international multicentre project was to gather knowledge about the course of COVID-19 cases in very old patients in intensive care unit (ICU) settings, and to detect specific risk factors for mortality and adverse events in this cohort to improve the outcome of these vulnerable patients. In all participating centres, prior ethical approval was obligatory before recruitment of the patients.
2.2Study population
All recruited patients were 1) aged≥70 years, 2) proven COVID-19 positive, and 3) admitted to an ICU due to the severity of the disease. The day of ICU admission reflected day one of data acquisition. The dataset contains patients from 19th of March 2020 until the 15th of July 2021.
2.3Data collection
In order to facilitate statistical analyses and to ensure comparability of all participating centres, the usage of an online electronic case report form (eCRF) was mandatory. For this specific study, only patients with a renal replacement therapy (RRT) during ICU stay were included for further analyses since cytokine absorption was applied as part of RRT.
All included patients received RRT due to renal failure at the discretion of the treating physician. 47 of them were treated with an additional cytokine absorption due to local protocols. No RRT was implemented for cytokine absorption therapy alone.
The Clinical Frailty Scale (CFS) [22, 23] prior to acute hospital admission was rated as well as the Sepsis-related organ failure assessment score (SOFA score) at the time of ICU admission. Moreover, pre-existing comorbidities such as chronic renal failure, arterial hypertension, pulmonary disease, and chronic heart failure were assessed. Body mass index (BMI) was calculated and its potential role as a mortality predictor was evaluated. Additionally, hospitalisation days prior to ICU admission and the number of days with symptoms were registered. During ICU stay, clinical variables describing the course of the disease were documented. Besides the need for an intubation, non-invasive ventilation (NIV) therapy, vasopressor use, prone positioning as well as insertion of a tracheostomy was recorded.
Withholding or withdrawal of treatment was documented. Mortality during ICU stay, after 30 days, and after 3 months was assessed.
2.4Data storage
The eCRF was created using the REDCap software [24]. Data storage was performed on a protected server at Aarhus University in Denmark. The servers were operated by the Information Technology Department and the Department of Clinical Medicine at Aarhus University, Denmark.
2.5Statistical analysis
Continuous data are described as median±interquartile range (IQR) and were checked for normal distribution. Differences between independent groups with non-normal distributions were calculated using Mann Whitney U-tests. Categorical data are expressed as percentages. For calculating differences between groups, the chi-square test was applied. Univariable and regression analyses were performed to assess association of cytokine absorption with mortality. We report (adjusted) odds ratios (OR) with respective 95% confidence intervals (CI). All tests were two-sided. A p-value of < 0.05 was considered statistically significant. Stata 16 was used for all statistical analyses (StataCorp LLC, 4905 Lakeway Drive, College Station, Brownsville, Texas, USA).
3Results
3.1Initial assessment on ICU admission
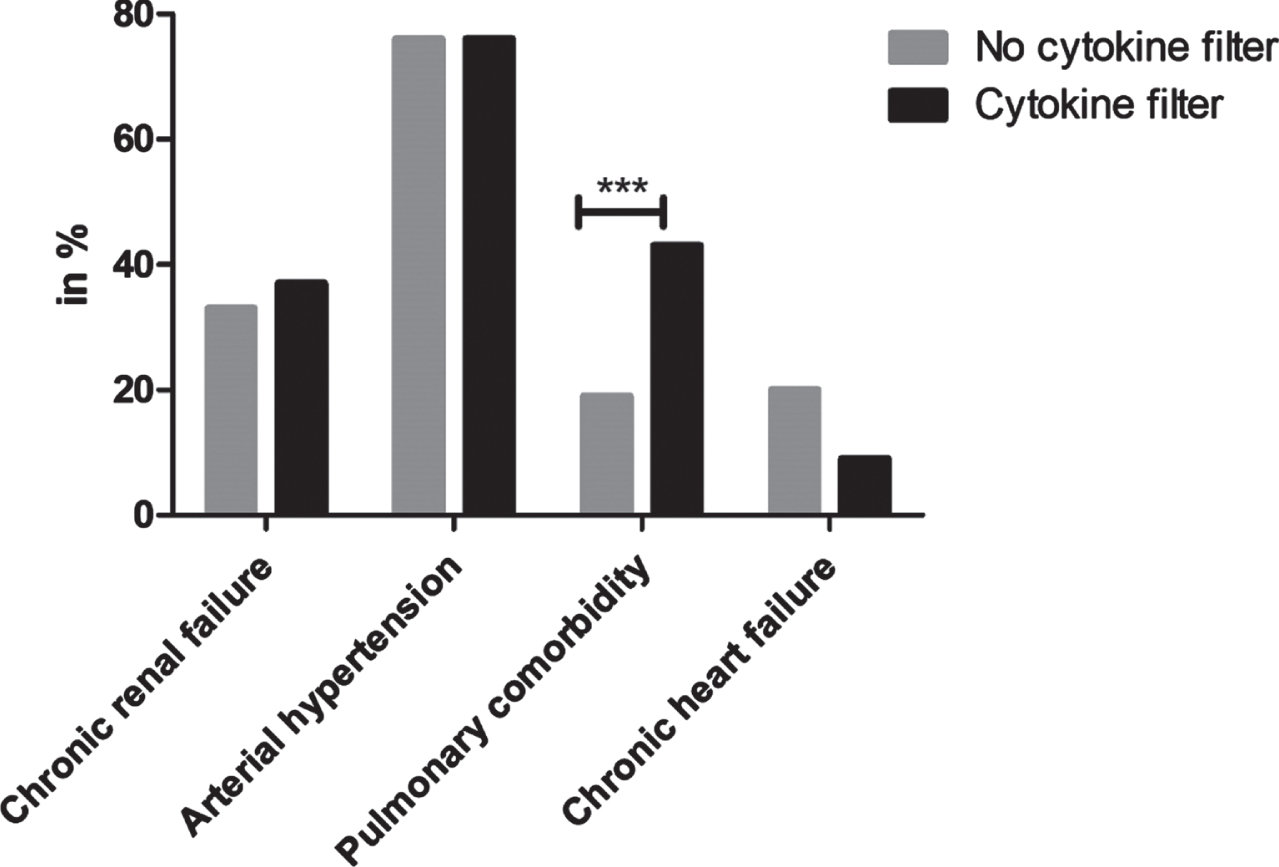
Patient characteristics are presented in Table 1. Among 3927 included in COVIP, 503 received RRT during their ICU stay (13%), 47 patients received an additional cytokine absorption (9%). The median age was 74 years [72–78 years] in the RRT only group and 75 years [72–78 years] in the cytokine group (p = 0.43). Patients receiving cytokine absorption therapy had a higher SOFA-score (9 [7–13] vs. 8 [5–10]; p = 0.02) at admission and were more frail prior to hospitalisation (CFS 5 [3–6] vs. 3 [2–5]; p < 0.001, Fig. 1). Moreover, they suffered from pulmonary comorbidity more frequently (43% vs.19%; p < 0.001, Fig. 2). The onset of COVID-19 was shorter in the cytokine group with fewer prior hospitalisation days (1 [1–3] vs. 2 [1–5]; p = 0.023) and the duration of symptoms was shorter before ICU admission (4 [2–7] vs. 6 [3–9] days; p = 0.022).
Table 1
Patient characteristics. Categorical variables are displayed as % (n), continuous variables as median (IQR)
| No cytokine filter (n = 456) | Cytokine filter (n = 47) | p-value | |
| Male sex (n) | 78% (354) | 70% (33) | 0.25 |
| Age in years | 74 (72-78) | 75 (72-78) | 0.43 |
| Age <80 years (n) | 86% (390) | 79% (37) | |
| Age >79 years (n) | 14% (66) | 21% (10) | |
| BMI | 28 (25-31) | 29 (26-32) | 0.38 |
| SOFA score | 8 (5-10) | 9 (7-13) | 0.02 |
| CFS | 3 (2-5) | 5 (3-6) | <0.001 |
| Comorbidities | |||
| Chronic renal failure | 33% (150) | 37% (17) | 0.58 |
| Arterial hypertension | 76% (346) | 76% (35) | 0.98 |
| Pulmonary comorbidity | 19% (86) | 43% (20) | <0.001 |
| Chronic heart failure | 20% (91) | 9% (4) | 0.058 |
Abbreviations: BMI –Body Mass Index (kg/m2); CFS –Clinical Frailty Scale; SOFA –Sequential Organ Failure Assessment.
Fig. 1
Initial assessment on ICU admission. Abbreviations: CFS –Clinical Frailty Scale; SOFA –Sequential Organ Failure Assessment. *=p<0.05; ***=p<0.001.
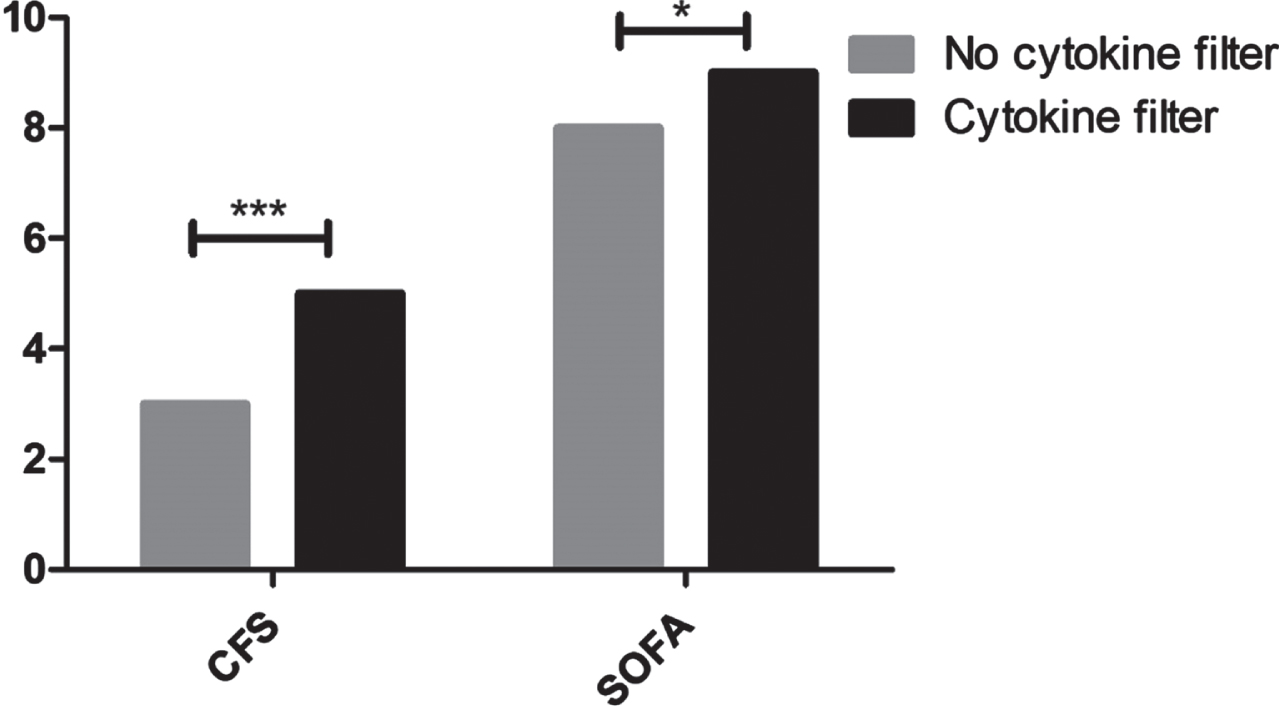
Fig. 2
Preexisting comorbidities prior to COVID-19 disease. ***=p<0.001.
3.2Continuous assessment during ICU stay
All 503 patients included for further analyses received RRT. No differences could be detected in terms of tracheostomy (28% vs. 32%; p = 0.57), vasopressor use (96% vs. 93%; p = 0.53), or prone positioning (49% vs. 62%; p = 0.18). Patients receiving cytokine absorption were intubated more frequently (100% vs. 92%; p = 0.049) and received NIV therapy prior to intubation more often (43% vs. 23%; p = 0.002).
3.3Withholding or withdrawal of treatment and mortality
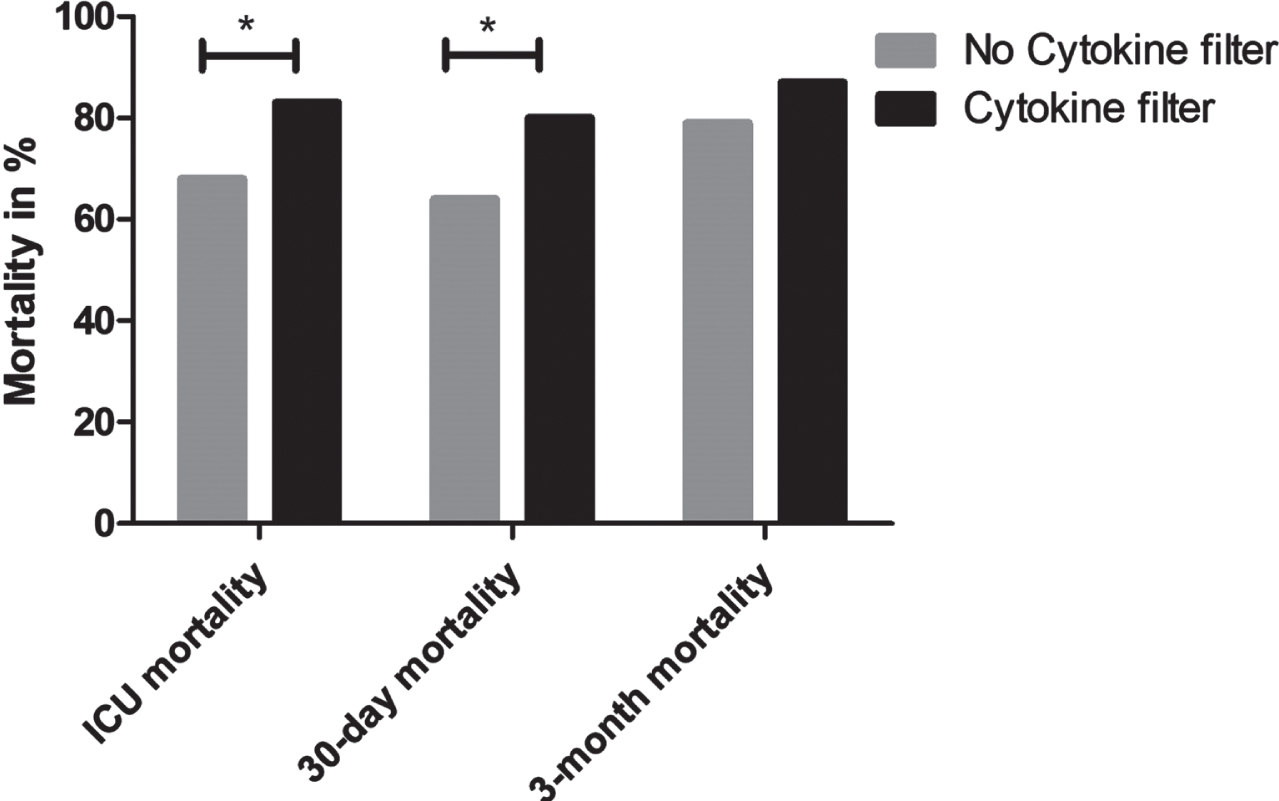
Withholding or withdrawal of treatment occurred less frequently in the cytokine group (4% vs. 28%; p < 0.001; 7% vs. 23%; p = 0.01, respectively). Mortality rates were high in both groups with increased rates in the cytokine absorption group both for ICU mortality (83% vs. 68%; p = 0.037), 30-day-mortality (80% vs. 64%; p = 0.028), but not for 3-month mortality (87% vs. 79%; p = 0.2; Fig. 3).
Fig. 3
ICU mortality, 30-day mortality, and 3-month mortality. *=p<0.05.
3.4Regression analysis
An additional regression analysis with 430 patients indicated that 30-day mortality was associated with SOFA-score (95% CI 1.04 to 1.17, p = 0.002), but not with cytokine absorption (95% CI 0.66 to 3.94, p = 0.291, Table 2).
Table 2
Logistic regression analysis for 30-day mortality (n = 430)
| Mortality 30 days | Odds ratio | Standard error | Z | P> | z | | [95% confidence interval] |
| Cytokine absorption | 1.616634 | 0.7357914 | 1.06 | 0.291 | 0.6625179 3.944807 |
| Age | 1.000447 | 0.0249066 | 0.02 | 0.986 | 0.9528031 1.050474 |
| Gender | 1.3827 | 0.3649277 | 1.23 | 0.220 | 0.8242811 2.319425 |
| SOFA | 1.100309 | 0.0343625 | 3.06 | 0.002 | 1.034979 1.169762 |
| CFS | 1.035227 | 0.0667712 | 0.54 | 0.591 | 0.9122921 1.174728 |
| Constant | 0.4797031 | 0.8796371 | -0.40 | 0.689 | 0.013186 17.45141 |
Abbreviations: SOFA –Sequential Organ Failure Assessment; CFS –Clinical Frailty Scale.
4Conclusions
In the present subgroup analysis of critically ill COVID-19 patients aged≥70 years, we investigated the impact of cytokine absorption in addition to standard RRT on ICU- and mid-term mortality.
The knowledge that cytokines contribute to a more critical course of disease in ARDS patients is not new; several studies highlight the role of cytokine release in immuno-pathological processes involved in severe lung injuries [25, 26]. Therefore, it is not surprising that recent studies described a potential role of cytokine release in COVID-19 and found an association between the level of cytokines and disease severity [27]. At first, mostly case reports and small case series have investigated the potential benefits of cytokine absorption in extenuating the burden of a threatening cytokine release [14, 17–19]. In a case series, published by Zhang et al., the authors described the disease course of five COVID-19-patients treated with a cytokine filter. The authors stated that cytokine absorption led to reduced levels of overexpressed cytokines, stabilised haemodynamics, and overall improved organ function [17]. These results were supported by a case series by Nassiri et al., who investigated 26 patients admitted to an ICU with moderate ARDS. They found significantly decreased levels of procalcitonin (PCT), ferritin, lactate, D-dimer as well as decreases in SOFA score and need for vasopressors as a marker for haemodynamic stabilisation post cytokine absorption treatment. Moreover, they assumed that an early initiation of cytokine absorption favored a benign outcome [19]. However, these uncontrolled studies included significantly younger patients, which makes an adequate comparison less robust. A recently published case-control study examined the effects of cytokine absorption on laboratory markers, SOFA scores, and mortality. Although the authors demonstrated decreases in C-reactive protein and fibrinogen, no clinical benefit or decreased mortality rates could be found [28].
Supporting these findings, the first randomised controlled trial investigating the effects of cytokine absorption in terms of IL-6 levels and 30-day survival in 34 COVID-19 patients requiring venovenous extracorporal membrane oxygenation (ECMO) showed negative results. The authors not only showed a lack of reduction in IL-6 in the cytokine absorption group when compared to the control group, but also demonstrated a significantly higher mortality in the cytokine absorption group. Therefore, despite the promising case reports and theoretical considerations, they concluded that cytokine absorption should not be initiated in the first days of ECMO in severely ill COVID-19 patients [20]. Another randomised controlled trial by Stockmann et al. investigated the influence of cytokine absorption in COVID-19 patients in vasoplegic shock and multiple organ failure. They could neither demonstrate a faster resolution of shock nor significant effects on inflammatory markers, catecholamine requirements, or mortality [21].
In line with these trials, in our study, we were unable to show associations between cytokine absorption and improved outcomes in old COVID-19 ICU patients. Moreover, patients receiving an additional cytokine absorption had statistically worse outcomes regarding ICU mortality and 30-day mortality.
A number of reasons may explain our findings. We recorded significantly higher SOFA scores at ICU admission and higher baseline CFS scores prior to hospitalisation for the cytokine group as well as significantly increased rates of preexisting pulmonary diseases. Therefore, one could argue that cytokine absorption was applied in more frail patients with a higher burden of preexisting comorbidities as a last resort therapy approach. This assumption is underlined by the performed regression analysis, showing that higher SOFA scores are a marker for worse outcomes. In contrast, cytokine filter use was not associated with outcome in this multivariable model.
NIV-therapy and intubation were used more often in the cytokine group (p = 0.002 and p = 0.0049, respectively). Combining these facts with the findings of significantly fewer days in hospital prior to ICU admission, as well as fewer days of symptom recognition as compared to the RRT group, one might suggest that this group suffered from a more severe and more acute course of COVID-19. This assumption is supported by our findings that withholding or withdrawal of treatment were significantly rarer in the cytokine group. Although this might be surprising at first, one could postulate that a decision to withdraw therapy was ethically more challenging in the context of a shorter and more fulminant course of COVID-19. Moreover, the ICU team might have wanted to wait for the effects of cytokine absorption prior to making decisions regarding therapy limitation. Regardless, these assumptions remain speculative.
The number of patients treated in the prone position was similar in both groups. Prone positioning has been shown to improve oxygenation in ARDS. In COVID-19 pneumonia benefits were seen in both sedated and intubated patients, as well as in awake patients [29–31] and has been declared as effective and safe [32, 33]. The combination of prone positioning and NIV-therapy was a less common strategy previously [34] and its use has increased during the COVID-19 pandemic [35, 36].
Our findings are in line with previous investigations emphasising the role of the SOFA score as a predictor of severity of disease and mortality in COVID-19 pneumonia [37, 38]. The same applies for the widely used CFS, which has been shown to positively correlate with mortality and adverse outcome [39]. A recently published meta-analysis by Pranata et al. illustrated an increase in mortality by 12% with every 1-point increase in the CFS [40]. Bearing these facts in mind, the significantly increased mortality in the cytokine absorption group is less surprising, but still depicts the limits of this treatment.
A limitation of our study is that we did not measure blood cytokine levels before and after cytokine absorption. Therefore, we can only assume that cytokine absorption was effective. Whereas some uncontrolled studies have proven the efficacy of cytokine absorption in decreasing the burden of inflammatory markers [17, 19], both available randomised controlled trials could not show significantly reduced interleukin levels after cytokine absorption in COVID-19 patients [20, 21]. One of these trials investigated the effects of cytokine absorption on IL-6-levels and mortality in COVID-19 patients receiving ECMO and did not only show a lack of reduction in IL-6, but also significantly increased mortality rates in this group [20]. Therefore, these results are in line with our findings of higher mortality in patients receiving an additional cytokine absorption and –at least –suggest a prudent use of this therapeutic option.
In summary, our multicentre study shows an increased mortality in patients receiving cytokine absorption in addition to regular RRT in the setting of old COVID-19 ICU patients during ICU stay and at 30 days, but not at 3 months. However, these findings should be regarded in the context of possible confounders, such as a more severe course of disease, higher frailty, and a lower level of withholding or withdrawal of treatment in the cohort with an additional cytokine absorption treatment.
However, combining our results with the available pre-existing literature [20, 21, 28], it might be reasonable to question the potential benefits of cytokine absorption in COVID-19 patients.
4.1Limitations
To the best of our knowledge, our study is the largest trial investigating the association of cytokine absorption with outcome in severe COVID-19 disease. However, our study has several limitations.
We did not measure pre- and post-cytokine absorption cytokine levels. Therefore, the success of cytokine absorption remains unclear. Also, there was no information regarding the haemodynamic response to cytokine absorption treatment and the kind of filters used. Secondly, we had some baseline biases in terms of pre-existing comorbidities, CFS, and SOFA scores. Thirdly, we have no information on why the cytokine therapy was chosen for these patients and when therapy was withdrawn or withheld.
Conflict of interest
There are no connections of the authors with any companies or industries. This study was conducted without any industrial funding.
Acknowledgments
The authors thank Antonio Artigas, Bernardo Bollen Pinto, Joerg C. Schefold, Philipp Heinrich Baldia, Peter Vernon van Heerden, Muhammed Elhadi, Sandra Oeyen, Brian Marsh, Finn H. Andersen, and Rui Moreno for their support, help, ideas, and contribution to the work.
Trial registration number
NCT04321265.
Ethical statement
Approval number of the Ethical Committee: 2020-892.
References
[1] | Kivrak A , Ulas B , Kivrak H A comparative analysis foranti-viral drugs: Their efficiency against SARS-CoV-2, IntImmunopharmacol (2021) ;90: , 107232. |
[2] | Cascella M , et al. Features, Evaluation, and Treatment of Coronavirus (COVID-19), in StatPearls. StatPearls Publishing Copyright© 2021, StatPearls Publishing LLC.: Treasure Island (FL). |
[3] | Weinreich DM , et al. REGN-COV2, a Neutralizing Antibody Cocktail, in Outpatients with Covid-19, N Engl J Med. (2021) ;384: (3):238–251. |
[4] | Jorgensen SCJ , Kebriaei R , Dresser LD Remdesivir: review of pharmacology, pre-clinical data, and emerging clinical experience for COVID-19, Pharmacotherapy (2020) ; 40: (7):659–671. |
[5] | Alzoughool F et al. Cerebrovascular comorbidity, high blood levels of C-reactive protein and D-dimer are associated with disease outcomes in COVID-19 patients. Clin Hemorheol Microcirc (2021) ;77: (3):311–322. |
[6] | RasyidA et al. Association of coagulation factors profile with clinical outcome in patient with COVID-19 and acute stroke: A second wave cohort study. Clin Hemorheol Microcirc 2022. |
[7] | Xing Y et al. D-dimer daily continuous tendency predicts the short-term prognosis for COVID-19 independently: A retrospective study from Northeast China, Clin Hemorheol Microcirc (2021) ;79: (2):269–277. |
[8] | Soy M et al. Cytokine storm in COVID- pathogenesis and overview of anti-inflammatory agents used in treatment, Clin Rheumatol (2020) ;39: (7):2085–2094. |
[9] | Ye Q , Wang B , Mao J The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19, J Infect (2020) ;80: (6):607–613. |
[10] | Suntharalingam G et al. Cytokine storm in a phase 1 trial of the anti-CD28 monoclonal antibody TGN1412, N Engl J Med (2006) ;355: (10):1018–28. |
[11] | Astapenko D et al. Endothelial glycocalyx damage in patients with severe COVID-19 on mechanical ventilation –A prospective observational pilot study, Clin Hemorheol Microcirc (2022) ;81: (3):205–219. |
[12] | Nile SH et al. COVID- Pathogenesis, cytokine storm and therapeutic potential of interferons, Cytokine Growth Factor Rev (2020) ;53: ,66–70. |
[13] | Stockmann H et al. CytoResc –“CytoSorb” Rescue for critically ill patients undergoing the COVID-19 Cytokine Storm: A structured summary of a study protocol for a randomized controlled trial, Trials (2020) ;21: (1):577. |
[14] | Rizvi S et al. Cytosorb filter: An adjunct for survival in the COVID-19 patient in cytokine storm? a case report, Heart Lung (2021) ;50: (1):44–50. |
[15] | Rimmelé T , Kellum JA Clinical review: blood purification forsepsis, Crit Care (2011) ;15: (1):205. |
[16] | Schubert A-K et al. Grundlagen der Nierenersatztherapie inder perioperativen Intensivmedizin (Renal replacement therapies inperioperative intensive care units), (2018) ;59: 574–586. |
[17] | Zhang H et al. The absorbing filter Oxiris in severe coronavirus disease patients: A case series, Artif Organs (2020) ;44: (12):1296–1302. |
[18] | Karabulut Keklik ES , Dal H , Bozok Ş Cytokine Hemoadsorption inthe Management of a Pregnant Woman with COVID-19 Pneumonia: CaseReport, SN Compr Clin Med 2020;1–5. |
[19] | Nassiri AA et al. Blood purification with CytoSorb in critically ill COVID-19 patients: A case series of 26 patients, Artif Organs 2021. |
[20] | Supady A et al. Cytokine adsorption in patients with severe COVID-19 pneumonia requiring extracorporeal membrane oxygenation (CYCOV): a single centre, open-label, randomised, controlled trial, Lancet Respir Med (2021) ;9: (7):755–762. |
[21] | Stockmann H et al. CytoSorb Rescue for COVID-19 Patients With Vasoplegic Shock and Multiple Organ Failure: A Prospective, Open-Label, Randomized Controlled Pilot Study, Crit Care Med (2022) ;50: (6):964–976. |
[22] | Flaatten H et al. The impact of frailty on ICU and 30-day mortality and the level of care in very elderly patients (≥80 years), Intensive Care Med (2017) ;43: (12):1820–1828. |
[23] | Guidet B et al The contribution of frailty, cognition, activity of daily life and comorbidities on outcome in acutely admitted patients over 80 years in European ICUs: the VIP2 study, Intensive Care Med (2020) ;46: (1):57–69. |
[24] | Harris PA et al. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support, J Biomed Inform (2009) ;42: (2):377–81. |
[25] | Chien JY et al. Temporal changes in cytokine/chemokine profiles and pulmonary involvement in severe acute respiratory syndrome, Respirology (2006) ;11: (6):715–22. |
[26] | Zhang Y et al. Analysis of serum cytokines in patients with severe acute respiratory syndrome, Infect Immun (2004) ;72: (8):4410–5. |
[27] | Quirch M , Lee J , Rehman S Hazards of the cytokine storm and cytokine-targeted therapy in patients with COVID- Review, J Med Internet Res.e (2020) ; 22: (8):20193. |
[28] | Abdullayev R et al. Cytokine Adsorption in Critically Ill COVID-19 Patients, a Case-Control Study, J Intensive Care Med 2022;8850666221085185. |
[29] | Singh P , Jain P , Deewan H Awake prone positioning in COVID-19 patients, Indian J Crit Care Med (2020) ;24: (10):914–918. |
[30] | Coppo A et al. Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID-19 (PRON-COVID): a prospective cohort study, Lancet Respir Med (2020) ;8: (8):765–774. |
[31] | Weiss TT et al. Prone positioning for patients intubated for severe acute respiratory distress syndrome (ARDS) secondary to COVID- a retrospective observational cohort study, Br J Anaesth (2021) ;126: (1):48–55. |
[32] | Scaravilli V et al. Prone positioning improves oxygenation in spontaneously breathing nonintubated patients with hypoxemic acute respiratory failure: A retrospective study, J Crit Care (2015) ;30: (6):1390–4. |
[33] | Fernandez R et al. Prone positioning in acute respiratory distress syndrome: a multicenter randomized clinical trial, Intensive Care Med (2008) ;34: (8):1487–91. |
[34] | Ding L et al. Efficacy and safety of early prone positioning combined with HFNC or NIV in moderate to severe ARDS: a multi-center prospective cohort study, Crit Care (2020) ;24: (1):28. |
[35] | Paternoster G et al. Awake pronation with helmet continuous positive airway pressure for COVID-19 acute respiratory distress syndrome patients outside the ICU: A case series, Med Intensiva (Engl Ed) 2020. |
[36] | Gürün Kaya A et al. Prone positioning in non-intubated patients with COVID-19, Tuberk Toraks (2020) ;68: (3):331–336. |
[37] | Izcovich A et al. Prognostic factors for severity and mortality in patients infected with COVID- A systematic review, PLoS One (2020) ;15: (11):e0241955. |
[38] | Zhou F et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study, Lancet (2022) 395: (10229);1054–1062. |
[39] | De Smet R et al. Frailty and mortality in hospitalized older adults with COVID- retrospective observational study, J Am Med Dir Assoc (2020) ;21: (7):928–932.e1. |
[40] | Pranata R et al. Clinical frailty scale and mortality in COVID- A systematic review and dose-response meta-analysis, Arch Gerontol Geriatr (2021) ;93: :104324. |


