
Prognostic impact of invariant natural killer T cells in solid and hematological tumors; systematic review and meta-analysis
Abstract
BACKGROUND:
Invariant natural killer T (iNKT) cells are an immune subset that purportedly link the adaptive and the innate arms of the immune system. Importantly, iNKT cells contribute to anti-cancer immunity in different types of hematological and solid malignancies by secreting pro-inflammatory cytokines. Therefore, using such cells in treating different type of tumors would be an ideal candidate for cancer immunotherapy.
OBJECTIVE:
To assess the prognostic effect of iNKT cells across different types of solid and hematological tumors.
METHODS:
In systematic review and meta-analysis, articles assessed the prognostic effect of iNKT cells were systemically searched using the scientific databases including Google Scholar, ScienceDirect, PubMed, Cochrane Central, and Scopus.
RESULTS:
Strikingly, the analysis showed the positive impact of intratumoral or circulating iNKT cells on the survival rate in patients with all studied tumors with overall effect of a pooled hazard ratio of 0.89 (95% CI 0.81 to 0.98;
CONCLUSIONS:
Taken together, this study would present a new insight into the impact of iNKT cells correlate with caner patients’ survival rate and how such cells would be used as a therapeutic target in these patients.
1.Introduction
Invariant natural killer T (iNKT) cell is a unique population of lymphocytes with shared properties of natural killer cells (NK) and T lymphocytes [1]. iNKT cells are distinct from conventional
iNKT cells known to secrete plethora of cytokines that play a crucial role in inflammatory diseases and maintain immune homeostasis [3]. iNKT cells have a well-known role in anti-tumor immunity. For example, iNKT cells are remodeling the tumor microenvironment through producing cytokines such as IFN-
Importantly, a decrease of iNKT cell counts are associated with worse outcomes in squamous carcinoma and chronic lymphocytic leukemia (CLL), possibly as a result of persistent activation by CLL cells that express CD1d [20, 21]. Notably, myeloma cells decrease CD1d expression as the disease progresses, hence iNKT cell frequency is inextricably linked to cancer progression [13, 15, 22, 23, 24]. Additionally, antigen-presenting cells (APCs) loaded with
Therefore, in this systematic review and meta-analysis, we aimed to assess the prognostic effect of iNKT cells across different types of solid and hematological tumors. Hence, iNKT cells were correlated with patient survival rates. We then explored the factors related to iNKT cells variation in tumors, such as gender, smoking status, number of intratumoral or peripheral iNKT cells and combination therapy with IFN-
2.Materials and methods
2.1Search strategy and selection criteria
We systematically searched the scientific databases including Google Scholar, ScienceDirect, PubMed, Cochrane Central, and Scopus to select potential studies for this systematic review and meta-analysis. Different key words were used to identify the relevant articles including invariant natural killer T cells (iNKT), clinical application of iNKT, iNKT in immunotherapy as well as iNKT cells in cancer prognosis. Additionally, we were looking in the relevant database for a combination of iNKT cells with cancer key words such as tumor, malignancy, carcinoma, adenocarcinoma, squamous cell carcinoma, sarcoma, myeloma, lymphoma and leukemia. The potential 1017 articles related to iNKT cells and cancer were found in the time span from (2000–2023).
2.2Inclusion and exclusion criteria
In the systematic review and meta-analysis, all studies provided information about association of iNKT cells frequencies either in periphery or at tumor sites and their relationship to cancer prognosis were included. Studies included in this analysis must been published as an original and primary article and assess human subjects as well as published in English language. Articles evaluating the association of either tumor infiltrating iNKT cells or circulating iNKT cells with clinical features of cancer patients such as overall survival (OS), disease free survival (DFS), recurrence free survival (RFS) and relapse free survival (RFS) were included. The eligibility of each study was assessed independently by at least two investigators (AA, FA, RAA, RTA, SA, ZA). Animal studies, in vitro studies using cell lines, interventional studies, using engineered iNKT cells as cellular therapy in cancer, reports published as conference abstracts and letters, and studies reported insufficient data of survival rates were excluded.
2.3Data extraction and assessment
Table 1
Newcastle-ottawa quality assessment
| Study ID | Selection | Comparability | Outcome | Scoring |
|---|---|---|---|---|
| Metelitsa et al. [42] | ** | * | *** | Fair quality |
| Tachibana et al. [29] | *** | * | *** | Good quality |
| Molling et al. [43] | ** | * | ** | Fair quality |
| Najera et al. [44] | *** | ** | *** | Good quality |
| Xiao et al. [28] | ** | * | ** | Fair quality |
| Hishiki et al. [45] | *** | * | *** | Good quality |
| Dockry et al. [30] | *** | ** | *** | Good quality |
| Melo et al. [46] | *** | * | ** | Fair quality |
The data from included studies was extracted independently by two investigators (RMA, AA, FA, RAA, RTA, SA, ZA). Both of two investigators assessed each study according to the authors’ names, year of publication, sample size, type of study, type of cancer, and iNKT identification (in peripheral blood or intratumoral tissue). The Newcastle-Ottawa quality assessment scale (NOS) was used to assess each study included in this analysis individually by two investigators. The scored of total 8 studies ranged from good quality to fair quality, according to the evaluation criteria detailed in Table 1.
2.4Statistical analysis
All statistical analysis and graphical representation were analysed and generated using RevMan software version 5.4 version (Cochrane Collaboration, Oxford, United Kingdom). The hazard ratio (HR) and its 95% confidence interval (CI) were extracted from the selected studies in the meta-analysis to assess the association of iNKT cells and patients’ prognosis. A fixed model effect was used to sum up all outcomes from the selected reports. Standard of error (SE) were calculated from given HR and 95% CI. Further, heterogeneity between studies was calculated, where I2 value of 25%, 50% and 75% corresponded to low, moderate, and high degree of heterogeneity.
3.Results
3.1Study characteristics
Figure 1.
Flow chart of searching and study selection (PRISMA).
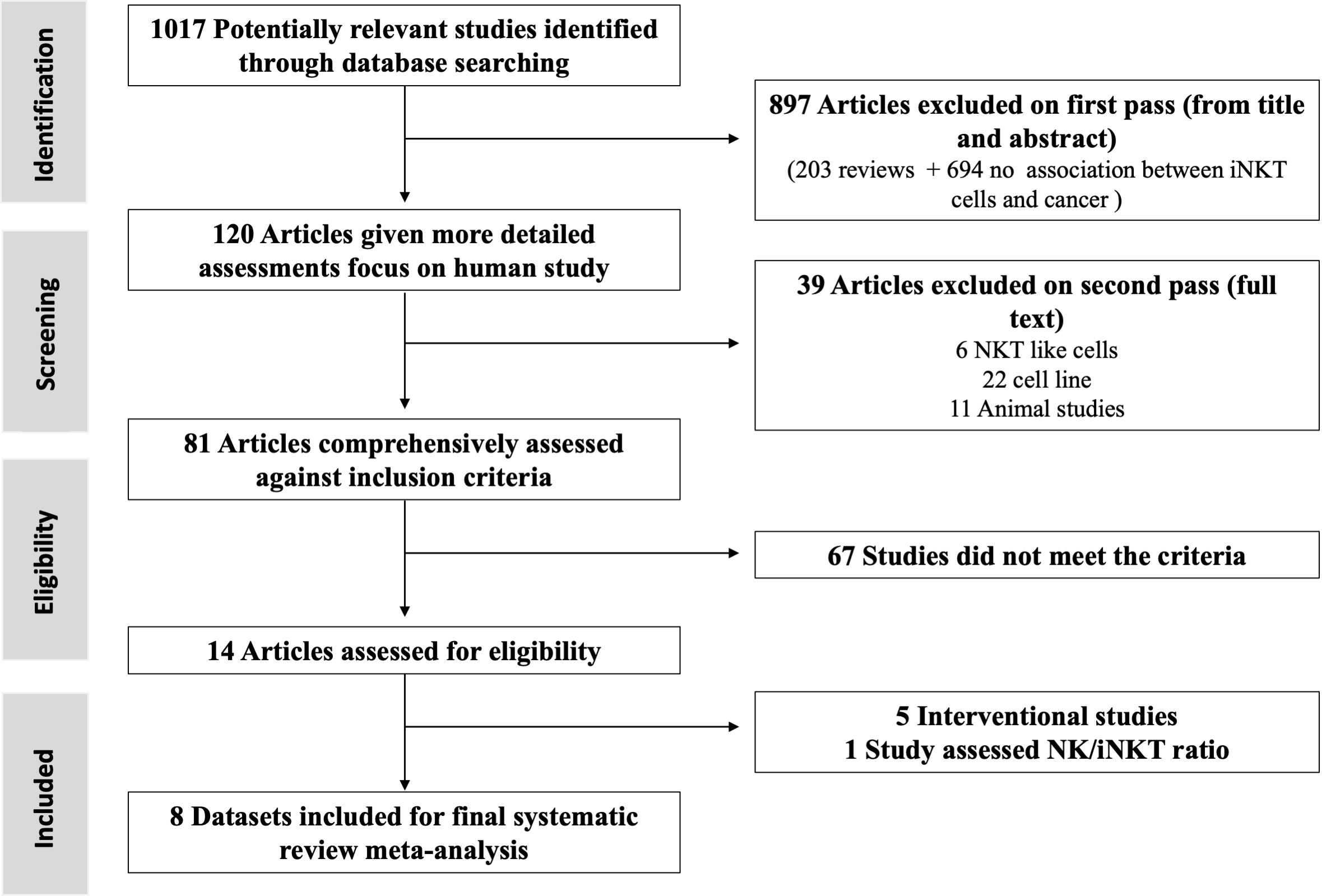
Initially, a total 1017 relevant articles were systematically identified through the scientific database, however 897 articles were excluded on the first pass based on the title and abstract (Fig. 1). The remaining 120 articles were given a more detailed assessment with evaluating association of iNKT cells with cancer prognosis. Following that, 81 studies were comprehensively assessed against inclusion criteria, however, only 14 articles were eligible studies and met the inclusion criteria. Yet, 5 studies out of 14 eligible articles were excluded as these studies did not report sufficient data to estimate the hazard ratio. Moreover, one study was assessing the NK/iNKT ratio. The final 8 datasets were included in the systematic review and meta-analysis encompassed different types of malignancies, including colorectal cancer, hepatocellular carcinoma, acute myeloid leukemia, head and neck squamous cell carcinoma, neuroblastoma, upper gastrointestinal cancers, and lung cancers.
3.2The prognostic effect of either tumor infiltrating or circulating iNKT cell on overall survival and recurrence free survival
Table 2
The basic characteristics for studies included in meta-analysis
| Study ID | Year of publication | Type of cancer | Sample size | Method for iNKT detection | OS | RFS | Median duration of follow up (years) |
|---|---|---|---|---|---|---|---|
| Metelitsa et al. [42] | 2004 | Neuroblastoma | 98 | RT-PCR (Intratumoral iNKT cells) | 0.007 | – | 5 years |
| Tachibana et al. [29] | 2005 | Colorectal carcinoma | 103 | Immunohistochemistry (Intratumoral iNKT cells) | 0.0006 | 0.018 | 1914 days (5 years and 3 months) |
| Molling et al. [43] | 2007 | Head and neck squamous cell carcinoma | 47 | Flow cytometry (Circulating iNKT cells) | 0.022 | 0.019 | 31 months (2 years and 7 months) |
| Najera et al. [44] | 2012 | Acute myeloid leukemia | 28 | Flow cytometry (Circulating iNKT cells) | 0.033 | 1 year | |
| Xiao et al. [28] | 2013 | Hepatocellular carcinoma | 224 | RT-PCR (Intratumoral iNKT cells) | 0.002 | 0.018 | 28 months (2 years and 4 months) |
| Hishiki et al. [45] | 2017 | Neuroblastoma | 107 | RT-PCR (Intratumoral iNKT cells) | 0.0089 | 224 months (18 years and 7 months) | |
| Dockry et al. [30] | 2018 | Lung cancer | 1926 | RT-PCR (Intratumoral CD1d expression) | 0.0013 | – | 57 months (7 years and 7 months) |
| Melo et al. [46] | 2020 | Upper gastrointestinal cancers | 139 | Flow Cytometry (Circulating iNKT cells) | 0.021 | – |
All studies included in the meta-analysis detailed in Table 2 and classified based on of the date of publication from the oldest to newest, type of cancer and
Figure 2.
Forest plot of overall survival sorted by year of study.
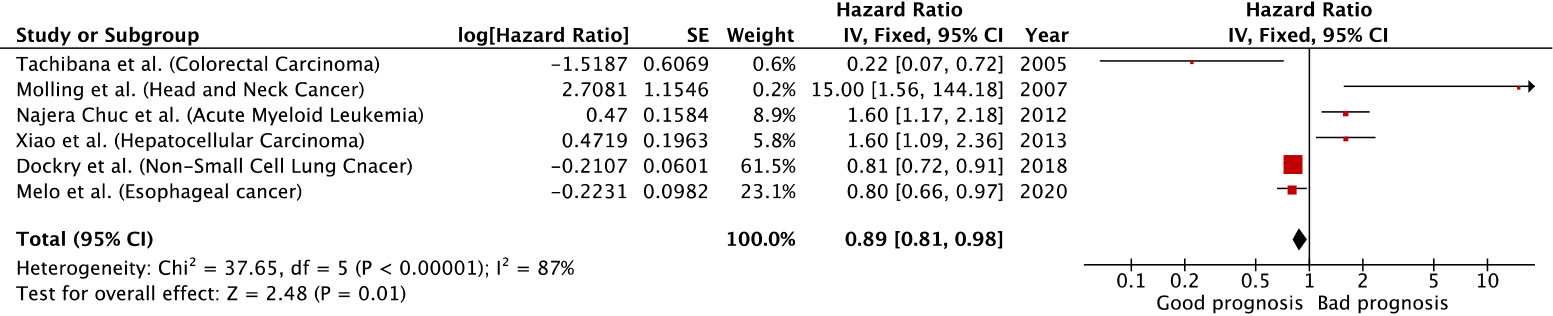
All the studies reported a significant impact of tumor infiltrating or circulating iNKT cells in patients with distinct types of malignancies on overall survival (Table 2). Of note, high density of infiltrating iNKT cells was found to be associated with an improved overall survival in patients with non-small lung cancer, oesophageal cancer and colorectal cancer compared to hepatocellular carcinoma, acute myeloid leukaemia and head and neck squamous cell carcinoma (Fig. 2).
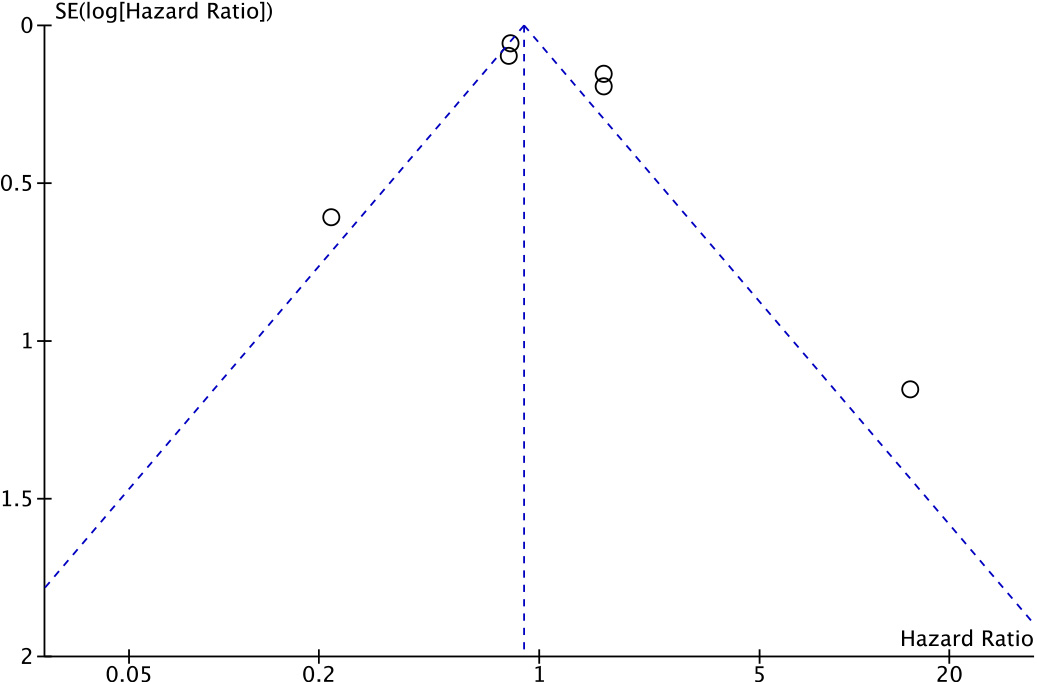
Figure 3.
Funnel plot to detect the presence of publication bias in the meta-analysis of overall survival.
Indeed, the forest plot evaluating the hazard ratio in all studied tumors showed that the positive effect of iNKT cells on the survival rate with a pooled hazard ratio of 0.89 (95% CI 0.81 to 0.98;
Figure 4.
Forest plot of recurrence free survival sorted by year of study.

Figure 5.
Funnel plot to detect the presence of publication bias in the meta-analysis of recurrence free survival.
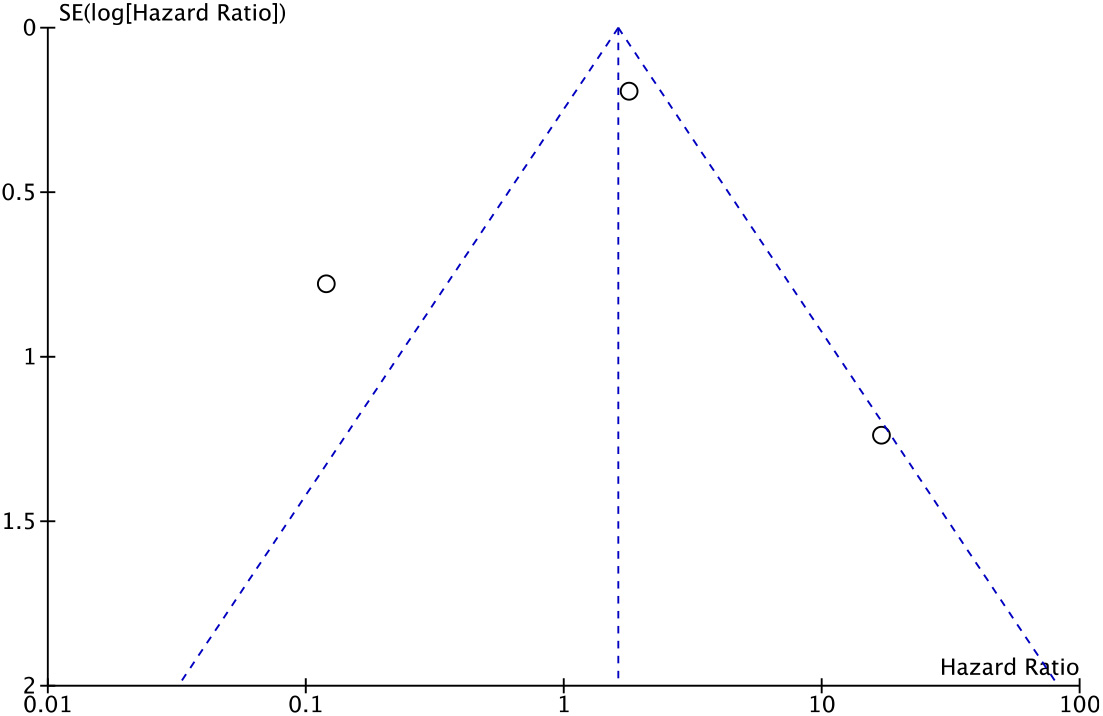
The recurrence-free survival (RFS) was reported only in three studies which had a negatively correlation with hazard ratio of 1.61 (95% CI 1.12 to 2.32) and
3.3Factors affect the significant impact of iNKT cells on overall survival
Table 3
Subgroup analysis of iNKT cells impact on different types of cancer
| Type of cancer | Number of patients | HR (95% CI) of OS | OS ( | HR (95% CI) of RFS | RFS ( |
|---|---|---|---|---|---|
| Non-small cell lung carcinoma (NSCLC) [30] | |||||
| Gender | |||||
| 1. Male | 1100 | 0.8 (0.68–0.94) | 0.0057 | – | – |
| 2. Female | 715 | 0.89 (0.7–1.11) | 0.29 | – | – |
| Smoking status | |||||
| 1. Smoker | 820 | 0.8 (0.65–0.99) | 0.037 | – | – |
| 2. Non-smoker | 205 | 1.03 (0.59 – 1.79) | 0.92 | – | – |
| Hepatocellular carcinoma [28] | |||||
| 1. Low Intratumoral iNKT & Low IFN- | 79 | I vs. III 2.784 (1.603–4.835) | – | I vs. III 3.141 (1.882–5.242) | |
| 2. High intratumoral iNKT & low IFN- | 83 | II vs. III 2.481 (1.410–4.366) | II vs. III 0.002 | II vs. III 2.139 (1.263–3.620) | II vs. III 0.016 |
| 3. High Intratumoral iNKT & high IFN- | 62 | I vs. II vs. II 0.001 | – | I vs. II vs. II 0.001 | |
| Head and neck squamous cell carcinoma (HNSCC) [43] | |||||
| iNKT cells/ml depend on health status (age matched) | |||||
| 1. HNSCC patients (103 iNKT cells/ml) | 47 | 0.0092 | – | – | |
| 2. Healthy controls (373 iNKT cells/ml) | 33 | ||||
| Levels of iNKT/106 T cells | |||||
| 1. Low iNKT ( | 22 | – | Low v Intermediate | – | Low v Intermediate |
| 2. Intermediate iNKT (48 to 242) | 11 | Low v High | Low v High | ||
| 3. High iNKT ( | 12 | ||||
Several factors might have a potential effect on iNKT cells frequencies within tumor microenvironment. For example, male patients with non-small cell lung carcinoma (NSCLC) had high expression of CD1d molecules which associated with significantly improved of overall survival compared to female patients with
Interferon
4.Discussion
The systematic review and meta-analysis were set out to assess the prognostic effect of iNKT cells across different types of solid and hematological tumors and correlate it with patients’ overall survival (OS).This study suggested that iNKT cells have a positive impact on the overall survival rate in different types of cancer including colorectal cancer, oesophageal cancer and lung cancer. This finding is supported by a number of clinical trials showed the potency of iNKT cells to be used as immunotherapeutic agent by increasing the overall survival rate and enhancing anti-tumor activity [31, 32, 33, 34, 35, 36]. For example, activating iNKT cells by administrating
However, combination therapy of administration of
In line with our observation that iNKT had different impact according to types of cancer, many studies demonstrated the influences of these cells depends on the site of cancer. For instance, there was an increase in peripheral iNKT cells number in benign ovarian cancer compared to advanced stage of ovarian cancer [38]. However, intratumoral iNKT cells showed an increase number compared to peripheral iNKT cells in the same cancer patients [38]. Therefore, the overall survival rate or recurrence-free survival may depend on the methods of iNKT cells detection and whether such cell was detected at tumor site or periphery. Having said that, the studies included in this meta-analysis were using different detection methods at different sites which might affect the consistency and accuracy of the study.
In this meta-analysis, the methods of detection varied between immunohistochemistry, real time polymerase chain reaction (RT-PCR) and flow cytometry which might impact on the overall effect. Importantly, different detection techniques would have different sensitivity and specificity. For example, RT-PCR is considered a gold stander for detection a certain type of cell or marker [39]. However, a recent study has been conducted comparing the accuracy of flow cytometry and RT-PCR in children with acute lymphoplastic leukemia [40]. Interestingly, the study showed the feasibility of both methods to be used in diagnosis as well as disease mentoring with no noticeable differences [40].
Other factor might have a noted impact on iNKT cells functionality in tumor microenvironment is their response to either endogenous or exogenous glycolipids such as
To our knowledge, this meta-analysis is the first study to demonstrate the prognostic impact of iNKT cells across different types of both hematological and solid tumors. However, there was a number of limitations associated with this study. First, the number of the studies that have been included and have met our criteria was limited which affect the overall effect and accuracy of this study. Notably, this study was using only observational study where it would be useful to compare the impact of iNKT cells on both observational and interventional studies. However, in all clinical trials were searching, there was a lack of information which limited the use of these studies. More meta-analysis should be done to evaluated different factors might affect the influence of iNKT cells in different sort of cancers.
In conclusion, either circulating or tumor infiltrating iNKT cells have been linked to improved overall survival rate in patients suffering from invasive malignancies such as NSCLC and hepatocellular carcinoma. Therefore, iNKT cells have been found to be a perfect candidate for cancer immunotherapy. However, a number of questions are needed to be answered in order to fully evaluated the use of such cells as a new treatment that might improve the clinical outcomes of cancer patients.
Author contributions
Conception: RMA.
Interpretation or analysis of data: All authors contributed to the interpretation or analysis of data Preparation of the manuscript: All authors contributed to preparation of the manuscript.
Revision for important intellectual content: RMA, NA, YA and HE.
Supervision: RMA.
References
[1] | S.B. Wilson and T.L. Delovitch, Janus-like role of regulatory iNKT cells in autoimmune disease and tumour immunity, Nature Reviews Immunology 3: ((2003) ), 211–222. |
[2] | Y.J. Lee, H. Wang, G.J. Starrett, V. Phuong, S.C. Jameson and K.A. Hogquist, Tissue-specific distribution of iNKT cells impacts their cytokine response, Immunity 43: ((2015) ), 566–578. |
[3] | C.-Y. Hsu, Y.-S. Chueh, M.-L. Kuo, P.-T. Lee, H.-S. Hsiao, J.-L. Huang and S.-J. Lin, Expansion of invariant natural killer T cells from systemic lupus erythematosus patients by alpha-Galactosylceramide and IL-15, Plos One 16: ((2021) ), e0261727. |
[4] | V.V. Parekh, M.T. Wilson, D. Olivares-Villagómez, A.K. Singh, L. Wu, C.-R. Wang, S. Joyce and L. Van Kaer, Glycolipid antigen induces long-term natural killer T cell anergy in mice, The Journal of Clinical Investigation 115: ((2005) ), 2572–2583. |
[5] | F. Fais, F. Morabito, C. Stelitano, V. Callea, S. Zanardi, M. Scudeletti, P. Varese, E. Ciccone and C.E. Grossi, CD1d is expressed on B-chronic lymphocytic leukemia cells and mediates α-galactosylceramide presentation to natural killer T lymphocytes, International Journal of Cancer 109: ((2004) ), 402–411. |
[6] | F. Fais, C. Tenca, G. Cimino, V. Coletti, S. Zanardi, D. Bagnara, D. Saverino, D. Zarcone, G. De Rossi and E. Ciccone, CD1d expression on B-precursor acute lymphoblastic leukemia subsets with poor prognosis, Leukemia 19: ((2005) ), 551–556. |
[7] | H. Nur, L. Rao, M.A. Frassanito, H. De Raeve, D. Ribatti, J.K. Mfopou, E. Van Valckenborgh, E. De Bruyne, A. Vacca and K. Vanderkerken, Stimulation of invariant natural killer T cells by α-Galactosylceramide activates the JAK-STAT pathway in endothelial cells and reduces angiogenesis in the 5T33 multiple myeloma model, British Journal of Haematology 167: ((2014) ), 651–663. |
[8] | Y. Hayakawa, K. Takeda, H. Yagita, M.J. Smyth, L. Van Kaer, K. Okumura and I. Saiki, IFN-γ–mediated inhibition of tumor angiogenesis by natural killer T-cell ligand, α-galactosylceramide, Blood, The Journal of the American Society of Hematology 100: ((2002) ), 1728–1733. |
[9] | K. Kobayashi, Y. Tanaka, S. Horiguchi, S. Yamamoto, N. Toshinori, A. Sugimoto and Y. Okamoto, The effect of radiotherapy on NKT cells in patients with advanced head and neck cancer, Cancer Immunology, Immunotherapy 59: ((2010) ), 1503–1509. |
[10] | N. Nishi, H.J. Van Der Vliet, Y. Koezuka, B.M.E. Von Blomberg, R.J. Scheper, H.M. Pinedo and G. Giaccone, Synergistic effect of KRN7000 with interleukin-15,-7, and-2 on the expansion of human Vα24+ Vβ11+ T cells in vitro, Human Immunology 61: ((2000) ), 357–365. |
[11] | K.M. Dhodapkar, B. Cirignano, F. Chamian, D. Zagzag, D.C. Miller, J.L. Finlay and R.M. Steinman, Invariant natural killer T cells are preserved in patients with glioma and exhibit antitumor lytic activity following dendritic cell-mediated expansion, International Journal of Cancer 109: ((2004) ), 893–899. |
[12] | J.P. Scott-Browne, J.L. Matsuda, T. Mallevaey, J. White, N.A. Borg, J. McCluskey, J. Rossjohn, J. Kappler, P. Marrack and L. Gapin, Germline-encoded recognition of diverse glycolipids by natural killer T cells, Nature Immunology 8: ((2007) ), 1105–1113. |
[13] | Y. Kinjo, D. Wu, G. Kim, G.-W. Xing, M.A. Poles, D.D. Ho, M. Tsuji, K. Kawahara, C.-H. Wong and M. Kronenberg, Recognition of bacterial glycosphingolipids by natural killer T cells, Nature 434: ((2005) ), 520–525. |
[14] | Y. Kinjo, E. Tupin, D. Wu, M. Fujio, R. Garcia-Navarro, M.R.-E.-I. Benhnia, D.M. Zajonc, G. Ben-Menachem, G.D. Ainge and G.F. Painter, Natural killer T cells recognize diacylglycerol antigens from pathogenic bacteria, Nature Immunology 7: ((2006) ), 978–986. |
[15] | W.L. Kok, L. Denney, K. Benam, S. Cole, C. Clelland, A.J. McMichael and L.-P. Ho, Pivotal Advance: Invariant NKT cells reduce accumulation of inflammatory monocytes in the lungs and decrease immune-pathology during severe influenza A virus infection, Journal of Leukocyte Biology 91: ((2012) ), 357–368. |
[16] | E.Y. Kim, J.T. Battaile, A.C. Patel, Y. You, E. Agapov, M.H. Grayson, L.A. Benoit, D.E. Byers, Y. Alevy and J. Tucker, Persistent activation of an innate immune response translates respiratory viral infection into chronic lung disease, Nature Medicine 14: ((2008) ), 633–640. |
[17] | S.-I. Fujii, K. Shimizu, C. Smith, L. Bonifaz and R.M. Steinman, Activation of natural killer T cells by α-galactosylceramide rapidly induces the full maturation of dendritic cells in vivo and thereby acts as an adjuvant for combined CD4 and CD8 T cell immunity to a coadministered protein, The Journal of Experimental Medicine 198: ((2003) ), 267–279. |
[18] | I.F. Hermans, J.D. Silk, U. Gileadi, M. Salio, B. Mathew, G. Ritter, R. Schmidt, A.L. Harris, L. Old and V. Cerundolo, NKT cells enhance CD4+ and CD8+ T cell responses to soluble antigen in vivo through direct interaction with dendritic cells, The Journal of Immunology 171: ((2003) ), 5140–5147. |
[19] | M. Kurosaki, S. Horiguchi, K. Yamasaki, Y. Uchida, S. Motohashi, T. Nakayama, A. Sugimoto and Y. Okamoto, Migration and immunological reaction after the administration of αGalCer-pulsed antigen-presenting cells into the submucosa of patients with head and neck cancer, Cancer Immunology, Immunotherapy 60: ((2011) ), 207–215. |
[20] | V. Cerundolo, J.D. Silk, S.H. Masri and M. Salio, Harnessing invariant NKT cells in vaccination strategies, Nature Reviews Immunology 9: ((2009) ), 28–38. |
[21] | J. Mattner, K.L. DeBord, N. Ismail, R.D. Goff, C. Cantu III, D. Zhou, P. Saint-Mezard, V. Wang, Y. Gao and N. Yin, Exogenous and endogenous glycolipid antigens activate NKT cells during microbial infections, Nature 434: ((2005) ), 525–529. |
[22] | V. Sriram, W. Du, J. Gervay-Hague and R.R. Brutkiewicz, Cell wall glycosphingolipids of Sphingomonas paucimobilis are CD1d-specific ligands for NKT cells, European Journal of Immunology 35: ((2005) ), 1692–1701. |
[23] | H. Lotter, N. González-Roldán, B. Lindner, F. Winau, A. Isibasi, M. Moreno-Lafont, A.J. Ulmer, O. Holst, E. Tannich and T. Jacobs, Natural killer T cells activated by a lipopeptidophosphoglycan from Entamoeba histolytica are critically important to control amebic liver abscess, PLoS Pathogens 5: ((2009) ), e1000434. |
[24] | H. Lotter, T. Jacobs, I. Gaworski and E. Tannich, Sexual dimorphism in the control of amebic liver abscess in a mouse model of disease, Infection and Immunity 74: ((2006) ), 118–124. |
[25] | L.A. Albacker, V. Chaudhary, Y.-J. Chang, H.Y. Kim, Y.-T. Chuang, M. Pichavant, R.H. DeKruyff, P.B. Savage and D.T. Umetsu, A fungal glycosphingolipid directly activates natural killer T cells and rapidly induces airways disease, Nature Medicine 19: ((2013) ), 1297. |
[26] | Y. Zhang, S. Wang, X.-M. Li, C.-M. Cui, C. Feng and B.-G. Wang, New sphingolipids with a previously unreported 9-methyl-C 20-sphingosine moiety from a marine algous endophytic fungus Aspergillus niger EN-13, Lipids 42: ((2007) ), 759–764. |
[27] | D. Jorgovanovic, M. Song, L. Wang and Y. Zhang, Roles of IFN-γ in tumor progression and regression: a review, Biomarker Research 8: ((2020) ), 1–16. |
[28] | Y.-S. Xiao, Q. Gao, X.-N. Xu, Y.-W. Li, M.-J. Ju, M.-Y. Cai, C.-X. Dai, J. Hu, S.-J. Qiu and J. Zhou, Combination of intratumoral invariant natural killer T cells and interferon-gamma is associated with prognosis of hepatocellular carcinoma after curative resection, PLoS One 8: ((2013) ), e70345. |
[29] | T. Tachibana, H. Onodera, T. Tsuruyama, A. Mori, S. Nagayama, H. Hiai and M. Imamura, Increased intratumor Vα24-positive natural killer T cells: a prognostic factor for primary colorectal carcinomas, Clinical Cancer Research 11: ((2005) ), 7322–7327. |
[30] | É. Dockry, S. O’Leary, L.E. Gleeson, J. Lyons, J. Keane, S.G. Gray and D.G. Doherty, Epigenetic induction of CD1d expression primes lung cancer cells for killing by invariant natural killer T cells, Oncoimmunology 7: ((2018) ), e1428156. |
[31] | T. Toyoda, T. Kamata, K. Tanaka, F. Ihara, M. Takami, H. Suzuki, T. Nakajima, T. Ikeuchi, Y. Kawasaki and H. Hanaoka, Phase II study of α-galactosylceramide-pulsed antigen-presenting cells in patients with advanced or recurrent non-small cell lung cancer, Journal for Immunotherapy of Cancer 8: ((2020) ). |
[32] | S. Motohashi, K. Nagato, N. Kunii, H. Yamamoto, K. Yamasaki, K. Okita, H. Hanaoka, N. Shimizu, M. Suzuki and I. Yoshino, A phase I-II study of α-galactosylceramide-pulsed IL-2/GM-CSF-cultured peripheral blood mononuclear cells in patients with advanced and recurrent non-small cell lung cancer, The Journal of Immunology 182: ((2009) ), 2492–2501. |
[33] | K. Nagato, S. Motohashi, F. Ishibashi, K. Okita, K. Yamasaki, Y. Moriya, H. Hoshino, S. Yoshida, H. Hanaoka and S.-I. Fujii, Accumulation of activated invariant natural killer T cells in the tumor microenvironment after α-galactosylceramide-pulsed antigen presenting cells, Journal of Clinical Immunology 32: ((2012) ), 1071–1081. |
[34] | M. Takami, F. Ihara and S. Motohashi, Clinical application of iNKT cell-mediated anti-tumor activity against lung cancer and head and neck cancer, Frontiers in Immunology 9: ((2018) ), 2021. |
[35] | Y. Gao, J. Guo, X. Bao, F. Xiong, Y. Ma, B. Tan, L. Yu, Y. Zhao and J. Lu, Adoptive transfer of autologous invariant natural killer T cells as immunotherapy for advanced hepatocellular carcinoma: a phase I clinical trial, The Oncologist 26: ((2021) ), e1919–e1930. |
[36] | M.A. Exley, P. Friedlander, N. Alatrakchi, L. Vriend, S. Yue, T. Sasada, W. Zeng, Y. Mizukami, J. Clark and D. Nemer, Adoptive transfer of invariant NKT cells as immunotherapy for advanced melanoma: a phase I clinical trial, Clinical Cancer Research 23: ((2017) ), 3510–3519. |
[37] | K. Yamasaki, S. Horiguchi, M. Kurosaki, N. Kunii, K. Nagato, H. Hanaoka, N. Shimizu, N. Ueno, S. Yamamoto and M. Taniguchi, Induction of NKT cell-specific immune responses in cancer tissues after NKT cell-targeted adoptive immunotherapy, Clinical Immunology 138: ((2011) ), 255–265. |
[38] | I. Winkler, J. Woś, A. Bojarska-Junak, A. Semczuk, T. Rechberger, W. Baranowski, E. Markut-Miotła, J. Tabarkiewicz, E. Wolińska and M. Skrzypczak, An association of iNKT+/CD3+/CD161+ lymphocytes in ovarian cancer tissue with CA125 serum concentration, Immunobiology 225: ((2020) ), 152010. |
[39] | T. Nolan, R.E. Hands and S.A. Bustin, Quantification of mRNA using real-time RT-PCR, Nature Protocols 1: ((2006) ), 1559–1582. |
[40] | J.M.C. Rocha, S.G. Xavier, M.E.d.L. Souza, M. Murao and B.M. de Oliveira, Comparison between flow cytometry and standard PCR in the evaluation of MRD in children with acute lymphoblastic leukemia treated with the GBTLI LLA–2009 protocol, Pediatric Hematology and Oncology 36: ((2019) ), 287–301. |
[41] | A. Singh, N. Shukla and S. Das, Altered invariant natural killer T cell subsets and its functions in patients with oral squamous cell carcinoma, Scandinavian Journal of Immunology 78: ((2013) ), 468–477. |
[42] | L.S. Metelitsa, H.-W. Wu, H. Wang, Y. Yang, Z. Warsi, S. Asgharzadeh, S. Groshen, S.B. Wilson and R.C. Seeger, Natural killer T cells infiltrate neuroblastomas expressing the chemokine CCL2, The Journal of Experimental Medicine 199: ((2004) ), 1213–1221. |
[43] | J.W. Molling, J.A. Langius, J.A. Langendijk, C.R. Leemans, H.J. Bontkes, H.J. van der Vliet, B.M.E. von Blomberg, R.J. Scheper and A.J. van den Eertwegh, Low levels of circulating invariant natural killer T cells predict poor clinical outcome in patients with head and neck squamous cell carcinoma, Journal of Clinical Oncology 25: ((2007) ), 862–868. |
[44] | A.E. Najera Chuc, L.A.M. Cervantes, F.P. Retiguin, J.V. Ojeda and E.R. Maldonado, Low number of invariant NKT cells is associated with poor survival in acute myeloid leukemia, Journal of Cancer Research and Clinical Oncology 138: ((2012) ), 1427–1432. |
[45] | T. Hishiki, N. Mise, K. Harada, F. Ihara, M. Takami, T. Saito, K. Terui, M. Nakata, S. Komatsu and H. Yoshida, Invariant natural killer T infiltration in neuroblastoma with favorable outcome, Pediatric Surgery International 34: ((2018) ), 195–201. |
[46] | A.M. Melo, M.J. Conroy, E.K. Foley, É. Dockry, E.P. Breen, J.V. Reynolds, J. Lysaght and D.G. Doherty, CD1d expression and invariant natural killer T-cell numbers are reduced in patients with upper gastrointestinal cancers and are further impaired by commonly used chemotherapies, Cancer Immunology, Immunotherapy 69: ((2020) ), 969–982. |


