
RAB27B expression in pancreatic cancer is predictive of poor survival but good response to chemotherapy
Abstract
BACKGROUND:
Pancreatic cancer is the 4th leading cause of cancer-related death with poor survival even after curative resection. RAB27A and RAB27B are key players in the exosome pathway where they play important roles in exosome secretion. Evidence suggests that RAB27A and RAB27B expression not only leads to tumor proliferation and invasion, but also plays an important role in antigen transfer necessary for anticancer immunity.
OBJECTIVE:
In this study, we analyze the expression of RAB27A and RAB27B in patients after pancreatic cancer surgery with or without adjuvant chemotherapy and its influence on overall survival.
METHODS:
We analyzed a total of 167 patients with pancreatic cancer for their RAB27A and RAB27B expression. We dichotomized the patients along the median and compared survival in patients with high and low RAB27A and RAB27B expression with or without adjuvant chemotherapy treatment.
RESULTS:
We found a significant improvement in overall survival in patients with a negative resection margin (
CONCLUSION:
These results suggest that RAB27B expression in pancreatic cancer might identify a subgroup of patients with poor survival who might respond well to adjuvant chemotherapy. If resectable, these patients could be considered for neoadjuvant chemotherapy to minimize the risk of not receiving adjuvant chemotherapy. Further prospective studies are needed to confirm these findings.
1.Introduction
Pancreatic cancer is the fourth most common cause of cancer-related death in developed countries with a 5-year overall survival (OS) of only 10% [1, 2]. Only 15–20% of patients are eligible for surgery, with a dismal 20% 5-year OS after curative resection [3]. The projected doubling of pancreatic cancer incidence by 2030 would make it the second leading cause of cancer-related deaths after lung cancer [4]. The poor survival of pancreatic cancer is due to late clinical presentation due to asymptomatic early disease and the aggressive biology combined with a dense, fibroblast rich tumor microenvironment leading to early metastasis and resistance to chemotherapy [5].
New methods to identify cancer-specific exosomes have shown excellent early detection of pancreatic cancer under study conditions but are still far from clinical translation [6]. Exosomes are small membrane vesicles with a size of 50–100 nm that play a role in intercellular communication by exchanging microRNA, mRNA, DNA fragments and proteins between the different tumor compartments [7].
At the core of exosome regulation are small GTPases belonging to the RAB family: RAB27A and RAB27B. Both have been shown to control important functions in the exosome pathway, particularly vesicle trafficking. RAB27A and RAB27B can switch between their active GTP-bound and inactive GDP-bound forms, acting as switches to regulate vesicle trafficking [8]. Silencing of the RAB27 effectors Slp4 and Slac2b significantly reduces exosome expression [9]. Several studies have shown that RAB27A and RAB27B control exosome secretion in several cancer cell types, including breast cancer, melanoma, bladder cancer, lung cancer and cervical cancer [10, 11, 12, 13, 14, 15]. Furthermore, in vitro studies in pancreatic cancer cell lines have shown that RAB27A and RAB27B expression in cancer cells increases proliferation and invasion, decreases apoptosis and leads to resistance to cisplatin therapy [16]. Accordingly, high RAB27A and RAB27B expression has been described as a marker of poor prognosis in several cancers, including pancreatic cancer [17, 18, 19, 20]. However, the existing literature in pancreatic cancer is based on a single cohort of patients without information on response to chemotherapy.
Exosomes play an essential role in intercellular communication, such as the interaction between tumor cells and the immune system. The regulation of the immune system by exosomes is a relatively new area of research. Exosomes have been shown to influence antigen presentation, immune activation, and immunosuppression [21]. Tumor exosomes are a source of tumor antigens that can be used to cross-activate cytotoxic T-cells [22]. Conversely, Rab27B knockout mice showed an impaired immune system with a weak response to bacterial LPS [23].
Finally, the response to chemotherapy is strongly influenced by the immune system, either by activating immune cells through antigen release from dying cancer cells, or by mediating off-target effects on immune cell populations [24, 25, 26, 27]. Conversely, chemotherapy can also improve the outcome of immunotherapy [28, 29]. In summary, exosomes play a plethora of complex roles in cancer growth, metastasis and immunomodulation, as well as some basic immunological roles such as antigen presentation and antitumor immunity.
In this study, we will shed some light on the clinical relevance of exosomes by investigating the clinical relevance of RAB27A and RAB27B on OS in the context of chemotherapy response in pancreatic cancer.
2.Material and methods
2.1Patients samples and tissue collection
This study was conducted in accordance with the Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK) [30]. This study was designed as an exploratory study. All patients gave their informed consent prior to resection and the study was approved by the Ethics Committee of the Technical University of Dresden (EK 59032007).
A total of 245 patients, who underwent curative resection for histologically proven ductal adenocarcinoma of the pancreas, were screened. 33 patients were excluded due to missing survival data (
Figure 1.
Flowchart of patient inclusion.
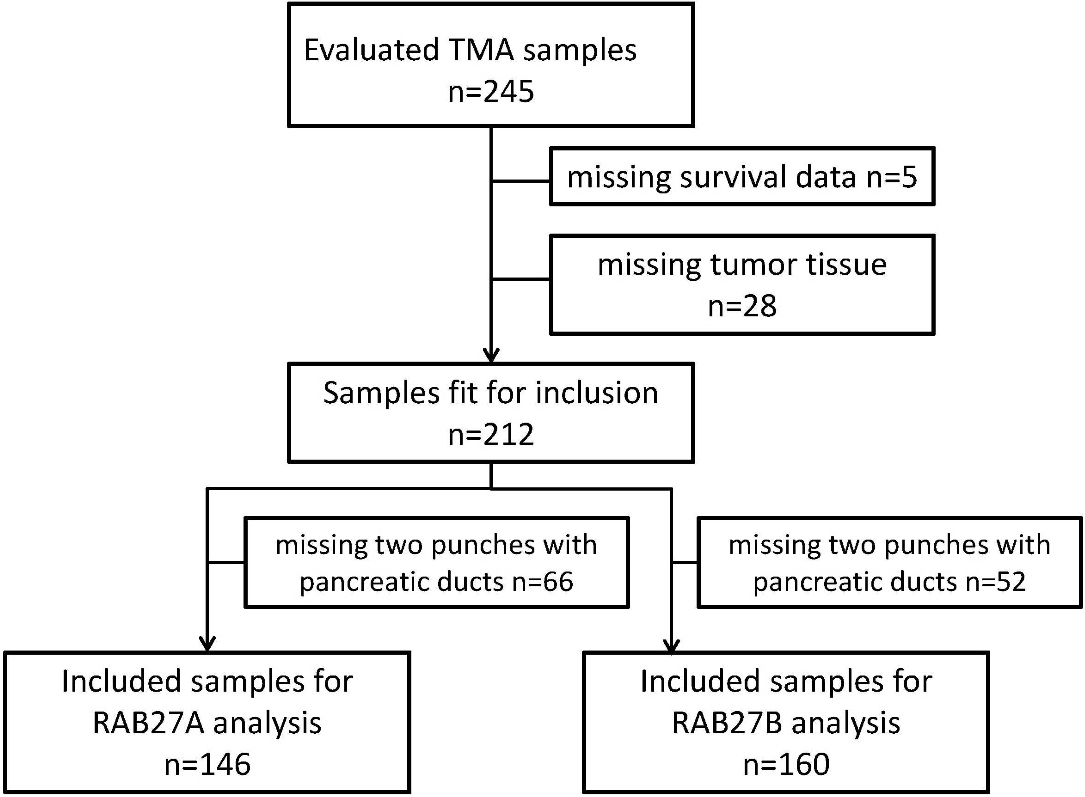
The tissue was studied in the form of tissue microarrays with individual tissue samples of 0.6 mm diameter. The microarray contained two samples from the same patient to reduce the risk of bias. Only patients with at least two separate tumor samples with pancreatic ducts were included in the final analysis. The tissue microarray was prepared by the Pathology Department of the University Hospital in Dresden, Germany. The histological evaluation of the samples was performed in a blinded fashion and the unblinding of the clinical data was performed after completion of the histological staining and evaluation.
2.2Tissue microarray and immunohistochemistry
Tissue microarrays (TMAs) were prepared by the Pathology Department of the University Hospital Dresden using a manual tissue microarray system (MTA-1 from Beecher). All samples were fixed in formaldehyde, punched in duplicates of 0.6 mm diameter and embedded in paraffin. Tissues from different organs were included in each TMA for reference. Hematoxylin-eosin staining was performed to assess both the presence of tumor tissue in the samples and the overall quality of the TMA.
Sections of 2
2.3Immunohistochemistry evaluation
Stained slides were scanned and evaluated using the Ventana Image Viewer (version 3.1.0.0; Ventana Medical System). H-scores were calculated using the following formula: [(0 x % negative cells)
Figure 2.
Examples of staining intensities (SI) in the tissue microarray (TMA).
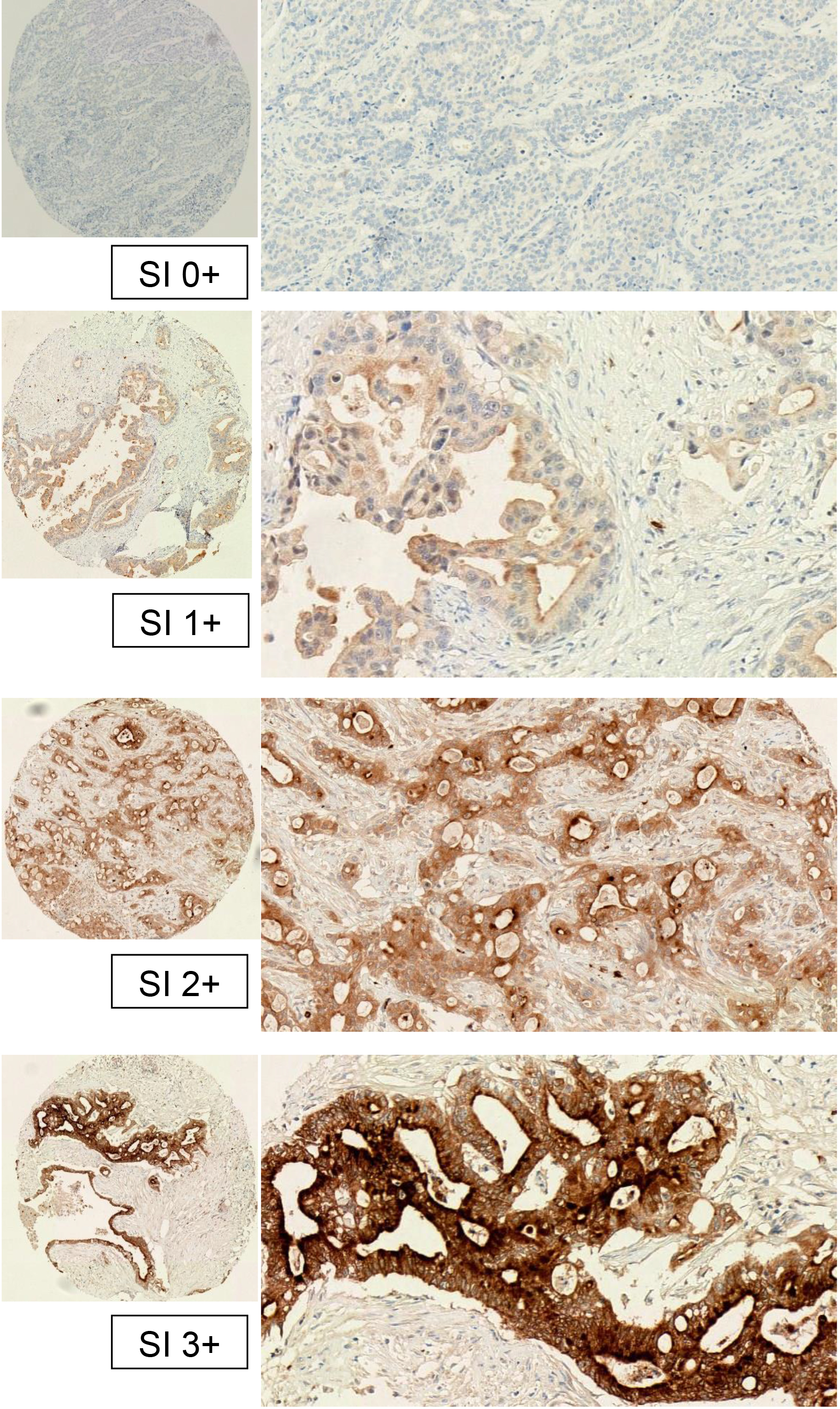
Table 1
Clinical characteristics broken down by high or low RAB27A and RAB27B expression
| Clinical data | ||||||||
|---|---|---|---|---|---|---|---|---|
| RAB27B low ( | RAB27B high ( | RAB27A low ( | RAB27A high ( | |||||
| AGE (mean, min-max) | 66 | (40–84) | 65 | (40–81) | 65 | (40–84) | 66 | (40–84) |
| SEX | ||||||||
| Male | 43 | (53%) | 45 | (57%) | 42 | (56%) | 39 | (55%) |
| Female | 38 | (47%) | 33 | (42%) | 33 | (44%) | 32 | (45%) |
| Missing | 1 | (1%) | ||||||
| Tumor stage | ||||||||
| T1 | 0 | (0%) | 0 | (0%) | 0 | (0%) | 0 | (0%) |
| T2 | 6 | (7%) | 5 | (6%) | 4 | (5%) | 4 | (6%) |
| T3 | 75 | (93%) | 73 | (92%) | 71 | (95%) | 67 | (94%) |
| T4 | 0 | (0%) | 1 | (1%) | 0 | (0%) | 0 | (0%) |
| Lymph node stage | ||||||||
| N0 | 28 | (35%) | 24 | (30%) | 22 | (29%) | 21 | (30%) |
| N1 | 51 | (63% | 54 | (68%) | 52 | (69%) | 49 | (69%) |
| N2 | 2 | (3%) | 1 | (1%) | 1 | (1%) | 1 | (1%) |
| Metastases | ||||||||
| M0 | 70 | (86%) | 71 | (90%) | 68 | (91%) | 64 | (90%) |
| M1 | 6 | (7%) | 2 | (3%) | 2 | (3%) | 2 | (3%) |
| Mx | 5 | (6%) | 6 | (8%) | 5 | (7%) | 5 | (7%) |
| Grading | ||||||||
| G1 | 1 | (1%) | 1 | (1%) | 1 | (1%) | 1 | (1%) |
| G2 | 37 | (46%) | 46 | (58%) | 36 | (48%) | 34 | (48%) |
| G3 | 42 | (52%) | 30 | (38%) | 37 | (49%) | 35 | (49%) |
| Gx | 1 | (1%) | 2 | (3%) | 1 | (1%) | 1 | (1%) |
| Resection | ||||||||
| R0 | 50 | (62%) | 48 | (61%) | 45 | (60%) | 41 | (58%) |
| R1 | 19 | (24%) | 26 | (33%) | 21 | (28%) | 21 | (30%) |
| R2 | 8 | (10%) | 2 | (3%) | 7 | (9%) | 7 | (10%) |
| Rx | 4 | (5%) | 3 | (4%) | 2 | (3%) | 2 | (3%) |
| Adjuvant therapy | ||||||||
| Yes | 37 | (46%) | 42 | (53%) | 30 | (40%) | 28 | (39%) |
| No | 44 | (54%) | 37 | (47%) | 45 | (60%) | 43 | (60%) |
2.4Statistical analysis
For statistical analysis, the H-values for RAB27A and RAB27B were dichotomized along the median and along the previously described cutoff values for reference [33]. Statistical analysis was performed with SPSS version 28 (SPSS 28.0.1.0, IBM). Survival statistics were performed using Kaplan-Meier curves and the log-rank test. Hazard ratios, 95% confidence intervals (CI), and the corresponding
3.Results
3.1Patient characteristics
The tissue for the tissue microarray was collected consecutively at the University Hospital Dresden between 1998 and 2011. The mean age was 66 years (40–84), 73 patients (44%) were female and 93 (56%) were male, T stage was T2 in 13 patients (8%), T3 in 153 patients (92%) and T4 in 1 patient (1%), lymph node status was N0 in 55 patients (33%), N1 in 109 (65%) and N2 in 3 (2%) patients, Metastatic status was M0 (no metastases) in 147 patients (88%), M1 (distant metastases) in 8 (5%), and Mx (missing information) in 12 (7%) of the patients, the tumor grading was G1 in 2 (1%), G2 in 83 (50%), G3 in 79 (48%), and missing in 3 (2%) of the patients. Follow-up was complete in 88%, with a median follow-up of 67 months for the remaining patients.
100 (69%) patients had a R0 status, 47 (28%) patients had a R1 status and 12 (7%) patients had a R2 status postoperatively. 84 (50%) of the patients received adjuvant chemotherapy and 83 (50%) did not. Detailed results are shown in Table 1.
Table 2
Hazard ratios of clinical factors as well as RAB27B expression for overall survival. RAB27B was dichotomized along the median (RAB27B
| Overall survival | ||||
| Including all 167 patients | ||||
| HR | 95% CI | |||
| AGE | ||||
| | 97/68 | 1.17 | 0.84–1.63 | 0.36 |
| Missing | 2 | |||
| SEX | ||||
| Female vs. male | 73/93 | 1.07 | 0.77–1.49 | 0.68 |
| Missing | 1 | |||
| T-stage | ||||
| 3–4 vs. 1–2 | 154/13 | 1.085 | 0.60–1.96 | 0.79 |
| Lymph node stage | ||||
| N pos vs. neg | 112/55 | 1.3 | 0.91–1.85 | 0.14 |
| UICC stage | ||||
| Stage 2B-4 vs. 1-2A | 113/54 | 1.33 | 0.93–1.89 | 0.11 |
| Metastases | ||||
| M pos vs. neg | 8/147 | 0.97 | 0.48–1.99 | 0.94 |
| Grading | ||||
| G3–4 vs G1–2 | 79/85 | 1.23 | 0.89–1.71 | 0.21 |
| Missing | 3 | |||
| Resection | ||||
| R pos vs. neg | 59/100 | 1.44 | 1.02–2.03 | 0.037 |
| Missing | 8 | |||
| Adjuvant therapy | ||||
| Yes vs no | 84/83 | 0.71 | 0.51–0.98 | 0.039 |
| RAB27A | ||||
| High vs. low (med | 75/74 | 1.01 | 0.73–1.41 | 0.94 |
| High vs. low ( | 11/138 | 1.13 | 0.61–2.09 | 0.7 |
| RAB27B | ||||
| High vs. low (med | 79/81 | 1.08 | 0.76–1.52 | 0.68 |
| High vs. low ( | 83/77 | 1.11 | 0.79–1.54 | 0.56 |
3.2Correlation of clinical factors with overall survival
The influence of the different clinical factors on OS was investigated using the Cox regression model. While age, sex and tumor grade did not show a significant correlation with OS, positive lymph node involvement and higher UICC status both showed a trend towards worse survival (N
3.3Correlation of RAB27A and RAB27B expression with overall survival
To evaluate the RAB27A and RAB27B expression and its impact on OS, H-scores were dichotomized using previously described cutoff values for H-scores in pancreatic cancer [33, 34] and the median of the patient cohort. The cox regression model was used to evaluate any potential impact on survival. Surprisingly, neither RAB27A nor RAB27B expression was significantly associated with OS. These results remained unchanged whether the median or the previously described cutoff values were used (Table 2).
3.4Correlation of clinical factors within the subgroups of patients with high or low RAB27A and RAB27B expression
To evaluate the influence of RAB27A and RAB27B expression on chemotherapy response, we created subgroups of patients with high and low RAB27A and RAB27B expression, respectively. The clinical factors in the high and low RAB27A and RAB27B expression groups were relatively homogeneous. The group of patients with high RAB27B expression had slightly more low grade cancers (G1/G2) than the patients with low RAB27B expression (Table 3).
Table 3
Evaluation of RAB27B expression as a predictor for poor survival. Patients with high RAB27B expression are shown on the right, patients with low RAB27B expression are shown on the left. Hazard Ratios (HR), 95% confidence intervals (95% CI) and
| RAB27B low ( | RAB27B high ( | |||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI |
| HR | 95% CI |
| |||
| AGE | ||||||||
| | 46/33 | 1.25 | 0.77–2.03 | 0.35 | 48/30 | 1.06 | 0.65–1.72 | 0.82 |
| SEX | ||||||||
| F vs. M | 38/43 | 0.86 | 0.54–1.38 | 0.54 | 33/45 | 1.39 | 0.86–2.23 | 0.18 |
| T3–4 vs T1–2 | 75/6 | 1.39 | 0.56–3.46 | 0.48 | 74/5 | 0.68 | 0.27–1.71 | 0.41 |
| N pos vs. neg | 53/28 | 1.46 | 0.87–2.43 | 0.15 | 55/24 | 1.08 | 0.65–1.81 | 0.77 |
| M pos vs. neg | 6/70 | 1.27 | 0.55–2.96 | 0.57 | 2/71 | 0.57 | 0.14–2.33 | 0.43 |
| G3–4 vs G1–2 | 42/38 | 0.98 | 0.64–1.57 | 0.94 | 30/47 | 1.66 | 1.00–2.76 | 0.05 |
| R pos vs. neg | 27/50 | 1.72 | 1.04–2.85 | 0.04 | 28/48 | 1.11 | 0.67–1.83 | 0.69 |
| Adjuvant | ||||||||
| Yes vs no | 37/44 | 0.88 | 0.55–1.41 | 0.59 | 42/37 | 0.52 | 0.32–0.84 | 0.007 |
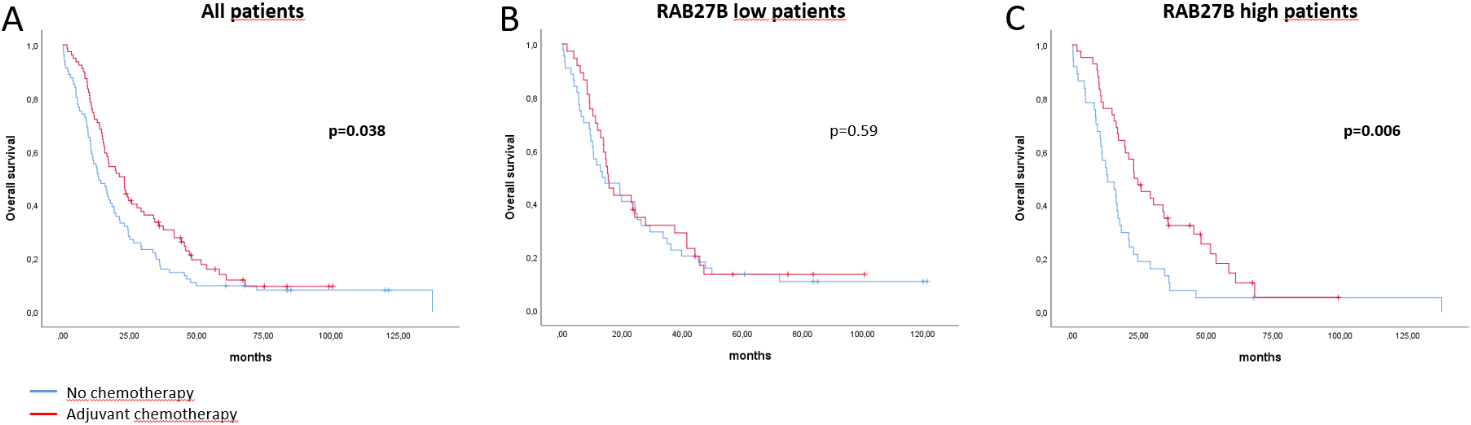
Figure 3.
Kaplan Meier curves of patients with or without adjuvant chemotherapy that did and did not receive chemotherapy for A) all patients B) patients with low RAB27B expression and C) patients with high RAB27B expression.
While there was no significant correlation with OS in both RAB27A subgroups (Supplementary Table 1), the RAB27B subgroups showed significant differences.
In the subgroup of patients with high RAB27B expression, significantly worse OS was observed in patients with higher tumor grade (HR 1.66, 95% CI 1.00–2.76,
We then compared the grading in the patients with high RAB27B expression and found no difference in the distribution of patients receiving (G1/2 vs. G3/4: 25/18) and not receiving (G1/2 vs. G3/4: 22/14) adjuvant chemotherapy. Thus, we can safely exclude an allocation bias.
These results suggest that patients with high RAB27B expression are more sensitive to adjuvant chemotherapy. In contrast, patients with low RAB27B expression do not appear to respond to adjuvant chemotherapy.
Finally, we compared survival in the 4 subgroups, patients with low RAB27B expression without adjuvant chemotherapy, patients with low RAB27B expression who received adjuvant chemotherapy, patients with high RAB27B expression without adjuvant chemotherapy, and patients with high RAB27B expression who received adjuvant chemotherapy.
As discussed above, patients with low RAB27B expression did not show a survival difference between patients with or without adjuvant chemotherapy. However, patients with high RAB27B expression without adjuvant chemotherapy had significantly worse survival compared to patients who received adjuvant chemotherapy (
These data suggest that RAB27B is indeed a predictor of poor survival as well as a predictor of chemosensitivity.
4.Limitations of this study
The included patients were resected between 1998 and 2011, none of them received neoadjuvant chemotherapy, and almost all of them received gemcitabine as adjuvant chemotherapy. The FOLFIRINOX chemotherapy regimen consisting of oxaliplatin, fluorouracil, leucovorin and irinotecan was first described in 2011 [35], while the gemcitabine/nab-paclitaxel combination was introduced in 2013 [36]. At the same time, an increasing number of elderly patients are being diagnosed with pancreatic cancer and are still receiving gemcitabine therapy due to frailty or poor ECOG status. In addition, while newer therapies are more aggressive, they also rely on the immune system for their effect [37].
5.Discussion
Exosomes are a new player in intercellular communication that have been shown to influence tumor growth, metastasis and the antitumoral immune response [7]. Two small GTPases, RAB27A and RAB27B, are at the core of exosome regulation. Both have been shown to control important functions in the exosome pathway, particularly in vesicle trafficking. Silencing of RAB27A and/or RAB27B results in a significant decrease in exosome expression [9]. Several publications have examined the impact of RAB27B expression on survival in various cancers. However, this is the first publication to show that RAB27B is not only a prognostic marker for poor survival in pancreatic cancer, but also a predictor of response to chemotherapy.
The literature is divided on the role of RAB27B expression in cancer. While some studies show poor survival in cancers that overexpress RAB27B [17, 38], other studies show the opposite [39, 40]. These different results could be explained by the conflicting roles that exosomes play in the crosstalk between cancer cells and the immune system.
On the one hand, recent studies have shown that exosome transfer of the EGFR-19del to the dendritic cell (DC) surface leads to impaired DC function in EGFR-19del-expressing Lewis lung cancer tumors [41]. Furthermore, exosomal PD-L1 secretion from cancer cells is part of their immune-evasion strategy [42] and could induce resistance to immunotherapy by inhibiting cytotoxic T-cells in draining lymph nodes [43].
On the other hand, exosomes are required for the transfer of tumor cell antigens to dendritic cells, thereby initiating the antitumor cytotoxic T-cell response [44]. Tumor exosomes are a source of tumor antigens that can be used to cross-activate cytotoxic T cells [22]. A knockout model of Rab27B mice showed an impaired immune system with a weak response to bacterial LPS [23].
In conclusion, although exosomes can lead to therapy resistance, they are required for the antitumor immune response.
In this study, we could show that pancreatic cancers with high RAB27B expression tend to be more aggressive with poorer overall survival compared to patients with low RAB27B expression. At the same time, these cancers respond significantly better to chemotherapy, with no difference in survival between patients with high and low RAB27B expression who both received chemotherapy. This may be due to a more effective immune response following chemotherapy-induced cancer cell death.
The expression of RAB27B in tumors may therefore be useful in identifying patients who may benefit from chemotherapy. Major postoperative complications or general morbidity after surgery may prevent the administration of adjuvant chemotherapy. This is one of the reasons why neoadjuvant chemotherapy is being considered to be extended from borderline resectable pancreatic cancer patients to resectable patients. Only about 50–60% of patients receive adjuvant chemotherapy after resection for pancreatic cancer [45]. Conversely, side effects after neoadjuvant chemotherapy may prevent curative surgery [46]. RAB27B expression may help to identify patients who may benefit from neoadjuvant chemotherapy.
6.Conclusion
We conclude that RAB27B is a potential prognostic marker for response to chemotherapy in pancreatic cancer. High RAB27B expression may identify patients who may benefit from neoadjuvant chemotherapy. Further studies as well as prospective studies are needed to confirm these findings.
Author contributions
Conception: Mathieu Pecqueux.
Interpretation or analysis of data: Mathieu Pecqueux, Beate Wende, Sebastian Hempel, Florian Oehme, Ulrich Sommer, Daniela Aust, Franziska Baenke.
Preparation of the manuscript: Mathieu Pecqueux, Christoph Kahlert, Florian Oehme, Sebastian Hempel.
Revision for important intellectual content: Franziska Baenke, Florian Oehme, Sebastian Hempel, Ulrich Sommer, Daniela Aust.
Supervision: Marius Distler, Jürgen Weitz, Christoph Kahlert.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/CBM-220460.
Acknowledgments
The study was fully funded by the Clinic for Visceral, Thoracic and Vascular Surgery, University Hospital Carl Gustav Carus, Dresden, Germany. We thank Heike Polster for her assistance in the collection of clinical patient data.
References
[1] | R.L. Siegel, K.D. Miller and A. Jemal, Cancer statistics, 2019 (US statistics), CA Cancer J Clin 69: ((2019) ), 7–34. |
[2] | R. Koch-Institut, Krebs in Deutschland für 2017/2018, (2017) . |
[3] | J.D. Mizrahi, R. Surana, J.W. Valle and R.T. Shroff, Pancreatic cancer, The Lancet 395: ((2020) ), 2008–2020. |
[4] | L. Rahib, B.D. Smith, R. Aizenberg, A.B. Rosenzweig, J.M. Fleshman and L.M. Matrisian, Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the united states, Cancer Res 74: ((2014) ), 2913–2921. |
[5] | K.J. Lafaro and L.G. Melstrom, The paradoxical web of pancreatic cancer tumor microenvironment, American Journal of Pathology 189: ((2019) ), 44–57. |
[6] | S.A. Melo, L.B. Luecke, C. Kahlert, A.F. Fernandez, T. Seth, J. Kaye, V.S. Lebleu, E.A. Mittendorf, J. Weitz, C. Reissfelder, C. Pilarsky, M.F. Fraga and D. Piwnica-, Detection of Cancer, 523: ((2016) ), 177–182. |
[7] | C. Kahlert and R. Kalluri, Exosomes in tumor microenvironment influence cancer progression and metastasis, J Mol Med 91: ((2013) ), 431–437. |
[8] | F. Barr and D.G. Lambright, Rab GEFs and GAPs, Curr Opin Cell Biol 22: ((2010) ), 461–470. |
[9] | M. Ostrowski, N.B. Carmo, S. Krumeich, I. Fanget, G. Raposo, A. Savina, C.F. Moita, K. Schauer, A.N. Hume, R.P. Freitas, B. Goud, P. Benaroch, N. Hacohen, M. Fukuda, C. Desnos, M.C. Seabra, F. Darchen, S. Amigorena, L.F. Moita and C. Thery, Rab27a and Rab27b control different steps of the exosome secretion pathway, Nat Cell Biol 12: ((2010) ), 19–30. |
[10] | M. Ostrowski, N.B. Carmo, S. Krumeich, I. Fanget, G. Raposo, A. Savina, C.F. Moita, K. Schauer, A.N. Hume, R.P. Freitas, B. Goud, P. Benaroch, N. Hacohen, M. Fukuda, C. Desnos, M.C. Seabra, F. Darchen, S. Amigorena, L.F. Moita and C. Thery, Rab27a and Rab27b control different steps of the exosome secretion pathway, Nat Cell Biol 12: ((2010) ), 19–30. |
[11] | Y. Zheng, E.C. Campbell, J. Lucocq, A. Riches and S.J. Powis, Monitoring the Rab27 associated exosome pathway using nanoparticle tracking analysis, Exp Cell Res 319: ((2013) ), 1706–1713. |
[12] | A. Bobrie, S. Krumeich, F. Reyal, C. Recchi, L.F. Moita, M.C. Seabra, M. Ostrowski and C. Théry, Rab27a supports exosome-dependent and -independent mechanisms that modify the tumor microenvironment and can promote tumor progression, Cancer Res 72: ((2012) ), 4920–4930. |
[13] | M.S. Ostenfeld, D.K. Jeppesen, J.R. Laurberg, A.T. Boysen, J.B. Bramsen, B. Primdal-Bengtson, A. Hendrix, P. Lamy, F. Dagnaes-Hansen, M.H. Rasmussen, K.H. Bui, N. Fristrup, E.I. Christensen, I. Nordentoft, J.P. Morth, J.B. Jensen, J.S. Pedersen, M. Beck, D. Theodorescu, M. Borre, K.A. Howard, L. Dyrskjøt and T.F. Ørntoft, Cellular Disposal of miR23b by RAB27-Dependent Exosome Release Is Linked to Acquisition of Metastatic Properties, Cancer Res 74: ((2014) ), 5758–5771. |
[14] | W. Li, Y. Hu, T. Jiang, Y. Han, G. Han, J. Chen and X. Li, Rab27A regulates exosome secretion from lung adenocarcinoma cells A549: involvement of EPI64, APMIS, (2014) , n/a-n/a. |
[15] | H. Peinado, M. Alečković, S. Lavotshkin, I. Matei, B. Costa-Silva, G. Moreno-Bueno, M. Hergueta-Redondo, C. Williams, G. García-Santos, C.M. Ghajar, A. Nitadori-Hoshino, C. Hoffman, K. Badal, B.A. Garcia, M.K. Callahan, J. Yuan, V.R. Martins, J. Skog, R.N. Kaplan, M.S. Brady, J.D. Wolchok, P.B. Chapman, Y. Kang, J. Bromberg and D. Lyden, Melanoma exosomes educate bone marrow progenitor cells toward a pro-metastatic phenotype through MET, Nat Med 18: ((2012) ), 883–891. |
[16] | J. Li, Q. Jin, F. Huang, Z. Tang and J. Huang, Effects of Rab27A and Rab27B on Invasion, Proliferation, Apoptosis, and Chemoresistance in Human Pancreatic Cancer Cells, Pancreas 46: ((2017) ), 1173–1179. |
[17] | H. Zhao, Q. Wang, X. Wang, H. Zhu, S. Zhang, W. Wang, Z. Wang and J. Huang, Correlation Between RAB27B and p53 Expression and Overall Survival in Pancreatic Cancer, Pancreas 45: ((2016) ), 204–210. |
[18] | H.M. Koh, B.G. Jang and D.C. Kim, Prognostic significance of Rab27 expression in solid cancer: A systematic review and meta-analysis, Sci Rep 10: ((2020) ), 14136. |
[19] | H.J. An, D.H. Song, H.M. Koh, G.H. Ko, J.-H. Lee, D.C. Kim, J.W. Yang, M.H. Kim, D.H. Seo, S.M. Jang and J.S. Lee, RAB27A is an independent prognostic factor in clear cell renal cell carcinoma, Biomark Med 13: ((2019) ), 239–247. |
[20] | Q. Wang, Q. Ni, X. Wang, H. Zhu, Z. Wang and J. Huang, High expression of RAB27A and TP53 in pancreatic cancer predicts poor survival, Medical Oncology 32: ((2015) ), 372. |
[21] | F.M. Barros, F. Carneiro, J.C. Machado and S.A. Melo, Exosomes and immune response in cancer: Friends or foes, Front Immunol 9: ((2018) ). |
[22] | F. Andre, N.E. Schartz, M. Movassagh, C. Flament, P. Pautier, P. Morice, C. Pomel, C. Lhomme, B. Escudier, T. le Chevalier, T. Tursz, S. Amigorena, G. Raposo, E. Angevin and L. Zitvogel, Malignant effusions and immunogenic tumour-derived exosomes, The Lancet 360: ((2002) ), 295–305. |
[23] | M. Alexander, A.G. Ramstead, K.M. Bauer, S.-H. Lee, M.C. Runtsch, J. Wallace, T.B. Huffaker, D.K. Larsen, T. Tolmachova, M.C. Seabra, J.L. Round, D.M. Ward and R.M. O’Connell, Rab27-dependent exosome production inhibits chronic inflammation and enables acute responses to inflammatory stimuli, The Journal of Immunology 199: ((2017) ), 3559–3570. |
[24] | M. Obeid, A. Tesniere, F. Ghiringhelli, G.M. Fimia, L. Apetoh, J.L. Perfettini, M. Castedo, G. Mignot, T. Panaretakis, N. Casares, D. Métivier, N. Larochette, P. van Endert, F. Ciccosanti, M. Piacentini, L. Zitvogel and G. Kroemer, Calreticulin exposure dictates the immunogenicity of cancer cell death, Nat Med 13: ((2007) ), 54–61. |
[25] | L. Apetoh, F. Ghiringhelli, A. Tesniere, M. Obeid, C. Ortiz, A. Criollo, G. Mignot, M.C. Maiuri, E. Ullrich, P. Saulnier, H. Yang, S. Amigorena, B. Ryffel, F.J. Barrat, P. Saftig, F. Levi, R. Lidereau, C. Nogues, J.-P. Mira, A. Chompret, V. Joulin, F. Clavel-Chapelon, J. Bourhis, F. André, S. Delaloge, T. Tursz, G. Kroemer and L. Zitvogel, Toll-like receptor 4–dependent contribution of the immune system to anticancer chemotherapy and radiotherapy, Nat Med 13: ((2007) ), 1050–1059. |
[26] | F. Ghiringhelli, L. Apetoh, A. Tesniere, L. Aymeric, Y. Ma, C. Ortiz, K. Vermaelen, T. Panaretakis, G. Mignot, E. Ullrich, J.-L. Perfettini, F. Schlemmer, E. Tasdemir, M. Uhl, P. Génin, A. Civas, B. Ryffel, J. Kanellopoulos, J. Tschopp, F. André, R. Lidereau, N.M. McLaughlin, N.M. Haynes, M.J. Smyth, G. Kroemer and L. Zitvogel, Activation of the NLRP3 inflammasome in dendritic cells induces IL-1β – dependent adaptive immunity against tumors, Nat Med 15: ((2009) ), 1170–1178. |
[27] | M. Ciampricotti, C.-S. Hau, C.W. Doornebal, J. Jonkers and K.E. de Visser, Chemotherapy response of spontaneous mammary tumors is independent of the adaptive immune system, Nat Med 18: ((2012) ), 344–346. |
[28] | S.C. Wei, C.R. Duffy and J.P. Allison, Fundamental mechanisms of immune checkpoint blockade therapy, Cancer Discov 8: ((2018) ), 1069–1086. |
[29] | L.A. Emens and G. Middleton, The interplay of immunotherapy and chemotherapy: Harnessing potential synergies, Cancer Immunol Res 3: ((2015) ), 436–443. |
[30] | L.M. McShane, D.G. Altman, W. Sauerbrei, S.E. Taube, M. Gion and G.M. Clark, REporting recommendations for tumor MARKer prognostic studies (REMARK), Nat Clin Pract Oncol 2: ((2005) ), 416–422. |
[31] | M. Uhlén, L. Fagerberg, B.M. Hallström, C. Lindskog, P. Oksvold, A. Mardinoglu, Å. Sivertsson, C. Kampf, E. Sjöstedt, A. Asplund, I. Olsson, K. Edlund, E. Lundberg, S. Navani, C.A.-K. Szigyarto, J. Odeberg, D. Djureinovic, J.O. Takanen, S. Hober, T. Alm, P.-H. Edqvist, H. Berling, H. Tegel, J. Mulder, J. Rockberg, P. Nilsson, J.M. Schwenk, M. Hamsten, K. von Feilitzen, M. Forsberg, L. Persson, F. Johansson, M. Zwahlen, G. von Heijne, J. Nielsen and F. Pontén, Tissue-based map of the human proteome, Science (1979) 347: ((2015) ). |
[32] | A.A. Thike, M.J. Chng, P.H. Tan and S. Fook-Chong, Immunohistochemical expression of hormone receptors in invasive breast carcinoma: Correlation of results of H-score with pathological parameters, Pathology 33: ((2001) ), 21–25. |
[33] | H. Zhao, Q. Wang, X. Wang, H. Zhu, S. Zhang, W. Wang, Z. Wang and J. Huang, Correlation Between RAB27B and p53 Expression and Overall Survival in Pancreatic Cancer, 45: ((2016) ), 204–210. |
[34] | Q. Wang, Q. Ni, X. Wang, H. Zhu, Z. Wang and J. Huang, High expression of RAB27A and TP53 in pancreatic cancer predicts poor survival, Med Oncol 32: ((2015) ), 372. |
[35] | T. Conroy, F. Desseigne, M. Ychou, O. Bouché, R. Guimbaud, Y. Bécouarn, A. Adenis, J.-L. Raoul, S. Gourgou-Bourgade, C. de la Fouchardière, J. Bennouna, J.-B. Bachet, F. Khemissa-Akouz, D. Péré-Vergé, C. Delbaldo, E. Assenat, B. Chauffert, P. Michel, C. Montoto-Grillot and M. Ducreux, FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer, New England Journal of Medicine 364: ((2011) ), 1817–1825. |
[36] | D.D. von Hoff, T. Ervin, F.P. Arena, E.G. Chiorean, J. Infante, M. Moore, T. Seay, S.A. Tjulandin, W.W. Ma, M.N. Saleh, M. Harris, M. Reni, S. Dowden, D. Laheru, N. Bahary, R.K. Ramanathan, J. Tabernero, M. Hidalgo, D. Goldstein, E. van Cutsem, X. Wei, J. Iglesias and M.F. Renschler, Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine, New England Journal of Medicine 369: ((2013) ), 1691–1703. |
[37] | H. Peng, C.A. James, D.R. Cullinan, G.D. Hogg, J.L. Mudd, C. Zuo, R. Takchi, K.E. Caldwell, J. Liu, D.G. DeNardo, R.C. Fields, W.E. Gillanders, S.P. Goedegebuure and W.G. Hawkins, Neoadjuvant FOLFIRINOX Therapy Is Associated with Increased Effector T Cells and Reduced Suppressor Cells in Patients with Pancreatic Cancer, Clinical Cancer Research 27: ((2021) ), 6761–6771. |
[38] | J.-X. Zhang, X.-X. Huang, M.-B. Cai, Z.-T. Tong, J.-W. Chen, D. Qian, Y.-J. Liao, H.-X. Deng, D.-Z. Liao, M.-Y. Huang, Y.-X. Zeng, D. Xie and S.-J. Mai, Overexpression of the secretory small GTPase Rab27B in human breast cancer correlates closely with lymph node metastasis and predicts poor prognosis, J Transl Med 10: ((2012) ), 242. |
[39] | W. Dong, J.-T. Cui, J. Yang, W.-M. Li, Y.-Y. Lu and W. Xiao, Decreased expression of Rab27A and Rab27B correlates with metastasis and poor prognosis in colorectal cancer, Discov Med 20: ((2015) ), 357–367. |
[40] | T.S. Worst, Y. Meyer, M. Gottschalt, C.-A. Weis, J. von Hardenberg, C. Frank, A. Steidler, M.S. Michel and P. Erben, RAB27A, RAB27B and VPS36 are downregulated in advanced prostate cancer and show functional relevance in prostate cancer cells, Int J Oncol 50: ((2017) ), 920–932. |
[41] | S. Yu, H. Sha, X. Qin, Y. Chen, X. Li, M. Shi and J. Feng, EGFR E746-A750 deletion in lung cancer represses antitumor immunity through the exosome-mediated inhibition of dendritic cells, Oncogene 39: ((2020) ), 2643–2657. |
[42] | G. Chen, A.C. Huang, W. Zhang, G. Zhang, M. Wu, W. Xu, Z. Yu, J. Yang, B. Wang, H. Sun, H. Xia, Q. Man, W. Zhong, L.F. Antelo, B. Wu, X. Xiong, X. Liu, L. Guan, T. Li, S. Liu, R. Yang, Y. Lu, L. Dong, S. McGettigan, R. Somasundaram, R. Radhakrishnan, G. Mills, Y. Lu, J. Kim, Y.H. Chen, H. Dong, Y. Zhao, G.C. Karakousis, T.C. Mitchell, L.M. Schuchter, M. Herlyn, E.J. Wherry, X. Xu and W. Guo, Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response, Nature 560: ((2018) ), 382–386. |
[43] | M. Poggio, T. Hu, C.-C. Pai, B. Chu, C.D. Belair, A. Chang, E. Montabana, U.E. Lang, Q. Fu, L. Fong and R. Blelloch, Suppression of Exosomal PD-L1 Induces Systemic Anti-tumor Immunity and Memory, Cell 177: ((2019) ), 414–427.e13. |
[44] | J. Wolfers and A. Lozier, Tumor-derived exosomes are a source of shared tumor rejection antigens for CTL cross-priming, Nat Med 38: ((2001) ), 297–303. |
[45] | R.P. Merkow, K.Y. Bilimoria, J.S. Tomlinson, J.L. Paruch, J.B. Fleming, M.S. Talamonti, C.Y. Ko and D.J. Bentrem, Postoperative complications reduce adjuvant chemotherapy use in resectable pancreatic cancer, Ann Surg 260: ((2014) ), 372–377. |
[46] | D.L. Birrer, H. Golcher, R. Casadei, S.R. Haile, R. Fritsch, S. Hussung, T.B. Brunner, R. Fietkau, T. Meyer, R. Grützmann, S. Merkel, C. Ricci, C. Ingaldi, M. di Marco, A. Guido, C. Serra, F. Minni, B. Pestalozzi, H. Petrowsky, M. DeOliveira, W.O. Bechstein, C.J. Bruns, C.E. Oberkofler, M. Puhan, M. Lesurtel, S. Heinrich and P.-A. Clavien, Neoadjuvant Therapy for Resectable Pancreatic Cancer: A New Standard of Care. Pooled Data From 3 Randomized Controlled Trials, Ann Surg 274: ((2021) ), 713–720. |


