
FHIT and C-MYC expression in cervical histology and cytology as biomarkers for detecting high-grade intraepithelial neoplasia in human papillomavirus-positive women
Abstract
BACKGROUND:
The current cervical cancer screening strategies based on Papanicolaou (Pap) and Human papillomavirus (HPV) tests receive great achievement but still exhibit many limitations in clinical practice. Exploring new biomarkers as stratified management method in HPV primary screening is becoming the tendency of current research.
METHODS:
Immunocytochemistry (ICC) of FHIT and C-MYC were performed on exfoliated cervical cells from 197 eligible high-risk HPV positive women. Mann-Whitney U test, Pearson Chi-Square test, logistic regression analysis and receiver operating characteristic (ROC) curves were used to assess the diagnostic efficiency.
RESULTS:
ICC staining intensity of FHIT and C-MYC in high-grade cervical intraepithelial neoplasia (CIN) specimens was significantly different from low-grade CIN and normal specimens. Compared with Pap test, ROC analysis of ICC in detecting high-grade CIN resulted in a larger area under the curve (AUC) (0.805 and 0.814 vs 0.723,
CONCLUSIONS:
The utility of FHIT and C-MYC ICC analysis in cervical exfoliated cells of HPV-positive women displayed superior diagnostic potential and may improve clinical performance of cervical cancer screening.
1.Introduction
Due to screening and high-risk human papillomavirus (HR-HPV) vaccination, cervical cancer drop-ped from the ninth to the tenth leading cause of cancer deaths worldwide in the last decade. However, cervical cancer, a preventable and treatable disease, still causes approximately 526000 new diagnoses and 239000 deaths annually [1], with approximately 85% of the worldwide incidence occurring in developing countries [2]. According to statistics, in low-sociodemographic index (SDI) countries, 1 in 24 women develop cervical cancer during their lifetime, whereas only 1 in 115 do so in high-SDI countries [1]. The high incidence of this disease in low-SDI countries and the large gap between developed and developing countries indicate that current screening strategies have some limitations. In particular, Papanicolaou (Pap) cytology is limited by its low sensitivity, high subjectivity and requirement for well-trained cytologists [3]. Therefore, there is a clear need to develop new screening strategies to reduce the incidence and mortality of cervical cancer.
The discovery of etiologic association between HR-HPV infection and cervical cancer led to the application of the HR-HPV test for cervical cancer screening. Evidence has shown that compared to Pap cytology, the HR-HPV test provides superior protection against high-grade cervical intraepithelial neoplasia (CIN) [4]. In some European countries and America, HR-HPV test has been recommended as the preferred strategy for primary cervical cancer screening [5, 6, 7]. However, while most HPV infections are transient, HPV test does not discriminate between transient and persistent infection, and this makes it suboptimal as a stand-alone primary screening method. Therefore, it is very important to apply additional stratified management of HPV-positive women in primary cervical cancer screening. Pap cytology and HPV 16/18 genotyping have been recommended as stratified screening triage approach for HPV-positive women [8, 9]. However, Pap cytology lacks sensitivity, while HPV 16/18 genotyping lacks specificity. There is a substantial demand for a method of identifying novel biomarkers that will improve specificity without compromising sensitivity in stratified screening of high-risk HPV positive women. Researchers have identified several novel biomarkers related to molecular alterations caused by HPV; these include p16/ki67, ProexC, gene promoter methylation and microRNAs [10, 11, 12, 13]. However, none of these biomarkers has been widely accepted in clinical practice.
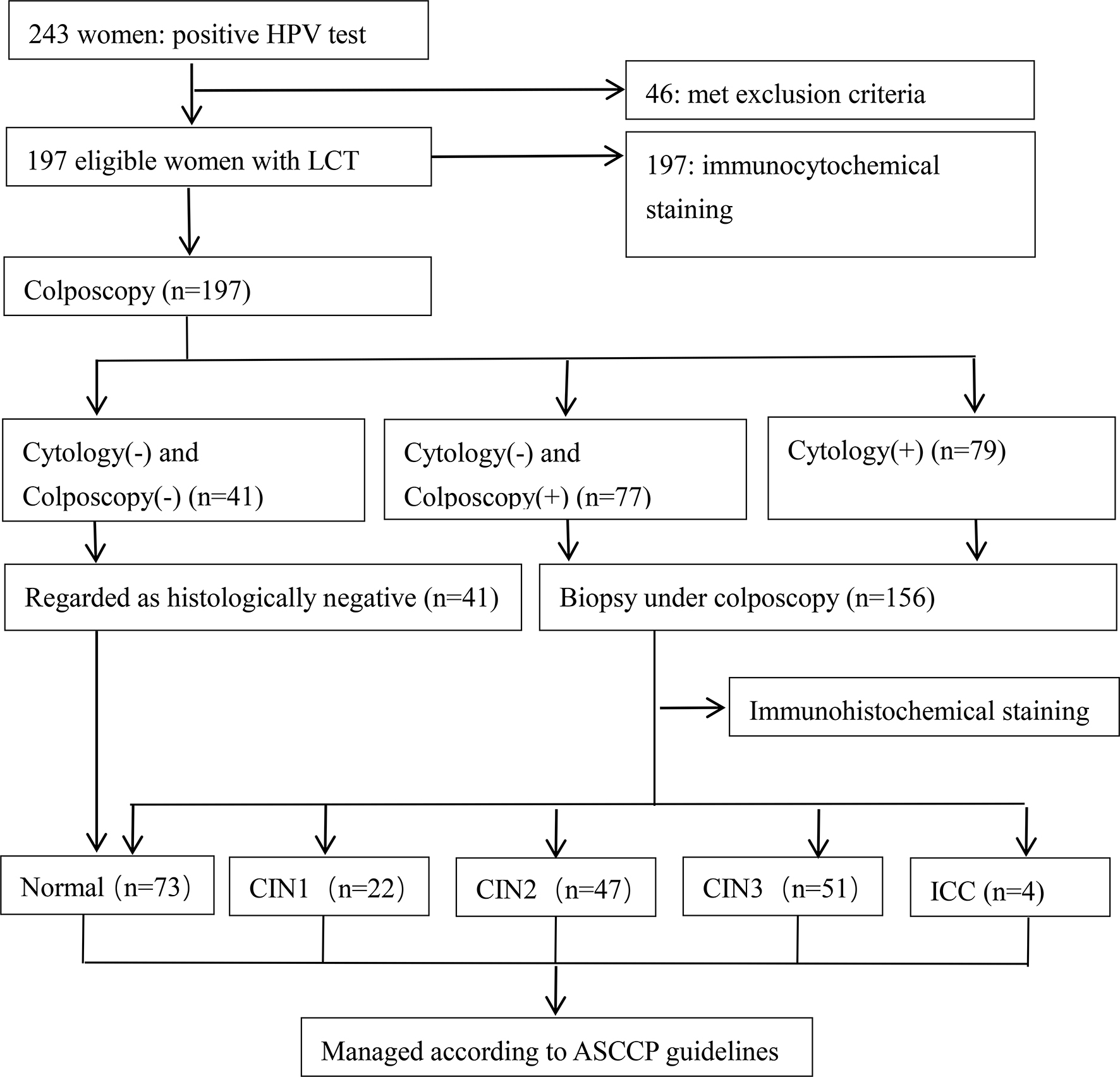
Figure 1.
Procedure of sample collection and results of biopsies. LCT: liquid-based cytology test; CIN: cervical intraepithelial neoplasia; ASCUS: abnormal squamous cells of uncertain significance; ASCCP: American Society for Colposcopy and Cervical Pathology. Cytology (-) indicates a negative Pap test result. Cytology (
The integration of HR-HPV DNA into the host genome results in overexpression of the viral oncoproteins E6 and E7, which bind to and inactivate p53 and pRb, respectively. The inactivation of p53 and pRb leads to cell cycle disruption and consequently tocervical cell malignant transformation [14]. However, this does not explain the entire etiological process of cervical carcinogenesis. An increasing number of studies confirm that the genetic or epigenetic alterations HPV integration causes in key oncogenes also play important roles in the development of cervical cancer. In a previous study, researchers used whole-genome sequencing and high-throughput viral integration detection to identify several high-frequency HPV integration breakpoints in cervical cancer tissues and cell lines. Among these hot-spot HPV integration breakpoints, FHIT and C-MYC were two well-known tumor-related genes. Researchers also confirmed that HPV integration into FHIT introns reduced FHIT protein expression, while HPV integration into the flanking regions of C-MYC increased C-MYC protein expression [15]. The FHIT gene is located at a common fragile site, FRA3B, and is frequently expressed at lower levels in preneoplasias and cancers. Many tumor-related biological functions are altered as a result of FHIT loss; these include apoptosis, epithelial-mesenchymal transition (EMT), genotoxic resistance and genome instability [16]. The C-MYC gene encodes a helix-loop-helix transcription factor that regulates many cellular functions, including cell growth, cell cycle progression, cell biosynthesis and apoptosis [17]. The HPV-induced dysregulation of FHIT and C-MYC expression indicates their potential value as biomarkers for cervical cancer screening.
The aim of this study is to search out new stratified screening triages for HPV-positive women. In order to implement this aim, we evaluate the clinical diagnosis value of FHIT and C-MYC ICC in detecting high-grade CIN among HPV-positive women and reveal their potential application as biomarkers for cervical cancer screening.
2.Materials and methods
2.1Subject recruitment and sample collection
Women who were test for both Pap cytology and HPV in the gynecologic outpatient clinic of our hospital from September 2015 to September 2017 were prospectively recruited. The study population (
2.2Pap cytology [liquid-based cytology (LBC)] and HPV cotest
Pap cytology specimens were collected by cytobrush and stored in BD SurePath Liquid-Based Cytology preservative fluid (BD Diagnostics, Sparks, MD). Thin-layer LBC was performed with a ThinPrep 2000 processor (Cytyc Corp, Boxborough, MA), and each cytological diagnosis was determined by two pathologists according to the Bethesda System (TBS, 2001). HPV tests were conducted with a Hybrid Capture 2 (HC2) assay (Digene, Gaithersburg, MD) to detect 13 types of HR-HPV, and more than 1 pg/mL HPV DNA in the specimen tested was regarded as positive result.
2.3Construction of tissue micro-array (TMA) blocks
Tissue specimens obtained from biopsies wereformalin-fixed and paraffin-embedded. Hematoxylin and eosin-stained slides were processed and evaluated by pathologists to locate representative lesion areas. For each specimen, a 1 mm
2.4Immunohistochemistry (IHC)
IHC assays were performed on TMA slides after they were deparaffinized with xylene and rehydrated with a descending ethanol series. Antigen retrieval was conducted by high-pressure boiling in a citrate pretreatment solution to inhibit nonspecific antibody binding. Endogenous peroxidase activity was blocked with 3% hydrogen peroxide, and nonspecific antibody binding was blocked with goat serum. The TMA slides were then incubated overnight in a humidified chamber at 4
2.5Cell line analyses
Human cervical carcinoma HeLa cells and human embryonic kidney (HEK) 293 cells were chosen to verify the FHIT and C-MYC protein expression levels in cells. The HeLa cells and HEK 293 cells were generously gifted by the State Key Laboratory of Oncology in South China and cultured in Dulbecco’s modified Eagle’s medium (DMEM) (Gibco BRL, Rockville, MD) supplemented with 10% fetal bovine serum (HyClone Laboratories, Logan, UT, USA), 100 U/ml penicillin in a 5% CO
Table 1
Frequencies of each level of FHIT staining intensity in different cervical lesions
| Subgroup | FHIT IHC staining intensity, | ||||
|---|---|---|---|---|---|
| Negative | Weak | Moderate | Strong | Positive rate, % | |
| Normal ( | 1 (3.1) | 4 (12.5) | 16 (50.0) | 11 (34.4) | 84.4 |
| CIN1 ( | 2 (9.1) | 5 (22.7) | 10 (45.5) | 5 (22.7) | 68.2 |
| CIN2 ( | 4 (8.5) | 21 (44.7) | 19 (40.4) | 3 (6.4) | 47.0 |
| CIN3 ( | 10 (19.6) | 27 (52.9) | 12 (23.5) | 2 (3.9) | 27.4 |
| ICC ( | 1 (25.0) | 3 (75.0) | 0 | 0 | 0 |
Table 2
Frequencies of each level of MYC staining intensity in different cervical lesions
| Subgroup | MYC IHC staining intensity, | ||||
| Negative | Weak | Moderate | Strong | Positive rate, % | |
| Normal ( | 15 (46.9) | 14 (43.8) | 3 (9.4) | 0 | 9.4 |
| CIN1 ( | 7 (31.8) | 12 (54.5) | 3 (13.6) | 0 | 13.6 |
| CIN2 ( | 4 (8.5) | 8 (17.0) | 21 (44.7) | 14 (29.8) | 74.5 |
| CIN3 ( | 3 (5.9) | 7 (13.7) | 25 (49.0) | 16 (31.4) | 90.4 |
| ICC ( | 0 | 0 | 2 (50.0) | 2 (50.0) | 100 |
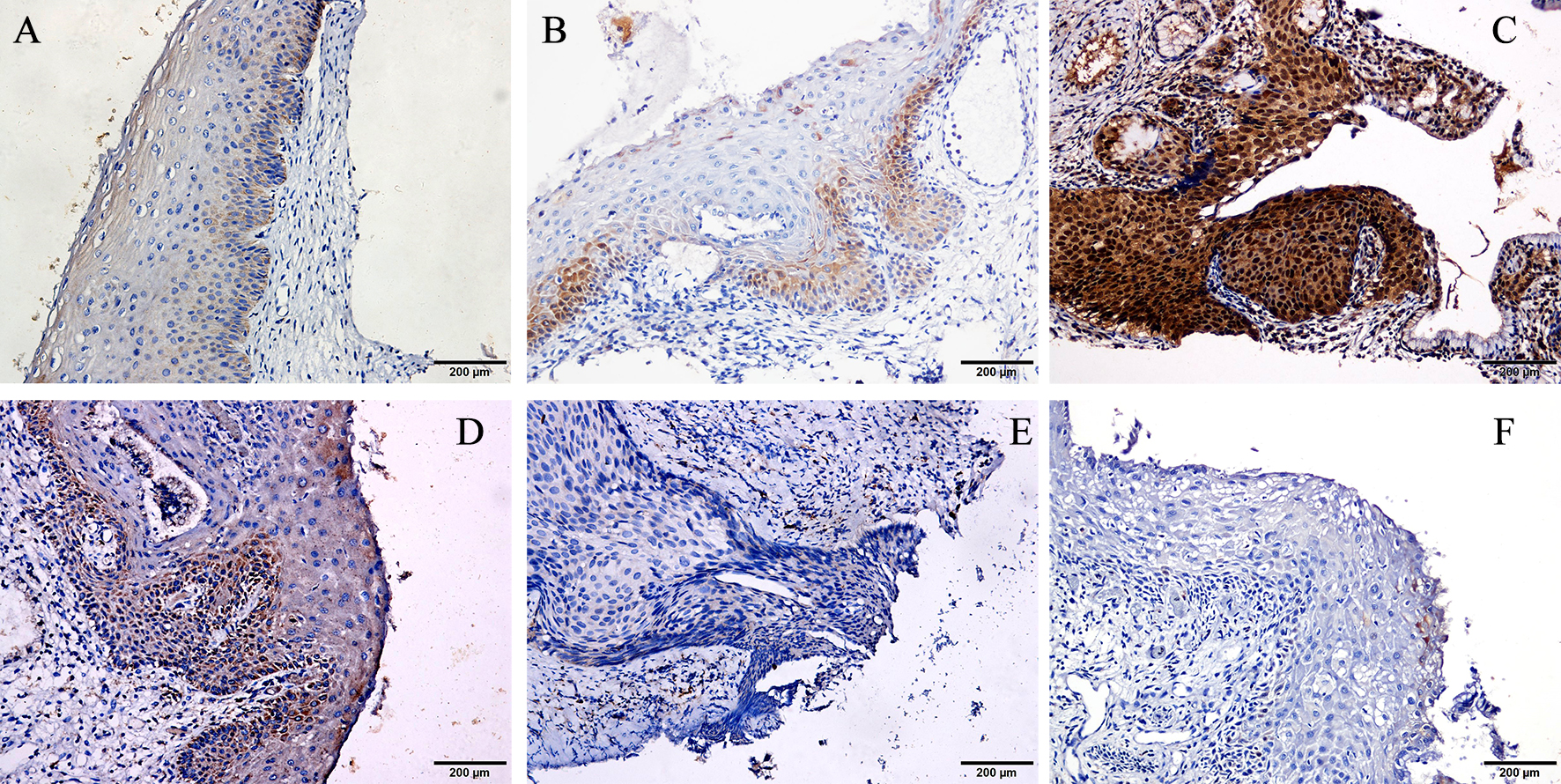
Figure 2.
Representative images of immunohistochemistry (IHC) of cervical samples obtained from normal women and patients with cervical intraepithelial neoplasia (CIN). (A) FHIT expression in CIN3 tissue. (B) FHIT expression in CIN1tissue. (C) FHIT expression in normal tissue. (D) C-MYC expression in CIN3 tissue. (E) C-MYC expression in CIN1 tissue. (F) C-MYC expression in normal tissue. Original magnification
2.6Immunocytochemistry (ICC)
After HPV tests and LBC tests were performed, two additional cytology slides were produced from each residual specimen using a ThinPrep 2000 processor (Cytyc Corp, Boxborough, MA, USA). The ICC staining procedures also included fixation, desiccation, antigen retrieval, endogenous peroxidase blocking, antibody incubation, HRP detection, DAB incubation and hematoxylin counterstaining. After ICC staining, the slides were analyzed and scored independently by two experienced pathologists blinded to the Pap test results and histological diagnosis. All cells were observed and evaluated in three random fields, and each cell was scored based on the intensity of immune staining. Staining intensity was classified as negative, weak, moderate, or strong, with negative scored as 0 points, weak as 1 point, moderate as 2 points, and strong as 3 points. The scores for each cell in one field were added together and divided by the total cell number in this field to produce the staining score of the corresponding field. The average score of three random fields from each slide was calculated as the “staining score” used to represent the staining intensity of the corresponding slide.
3.Statistical analysis
In this study, FHIT and C-MYC immunocytochemical staining scores of two groups were compared by the nonparametric Mann-Whitney U test. ROC curves were used to assess the diagnostic efficiency of immunocytochemical staining in detecting high-grade intraepithelial neoplasia (CIN2
4.Results
The results of Pap test and colposcopies and histological diagnoses are shown in Fig. 1. Among the 197 HR-HPV-positive eligible women who underwent colposcopy, 156 underwent a directed biopsy under colposcopy for abnormal cytology results (
First, IHC staining was performed to analyze the corresponding protein expression in cervical lesions at different stages. Representative FHIT and C-MYC staining patterns are shown in Fig. 2. In IHC staining of different stages of cervical lesions, the FHIT expression-positive rates in normal cervical tissue, CIN1, CIN2, CIN3 and invasive cancer were 84.4%, 68.2%, 47.0%, 27.4% and 0%, respectively, and there was a tendency for positive rates to be correlated with the grade of cervical lesion (
Figure 3.
Representative images of ICC in HeLa and HEK293 cells. (A) Blank control in HeLa cells. (B) FHIT expression in HeLa cells. (C) MYC expression in HeLa cells. (D) Blank control in HEK293 cells. (E) FHIT expression in HEK293 cells. (F) MYC expression in HEK293 cells. Original magnification
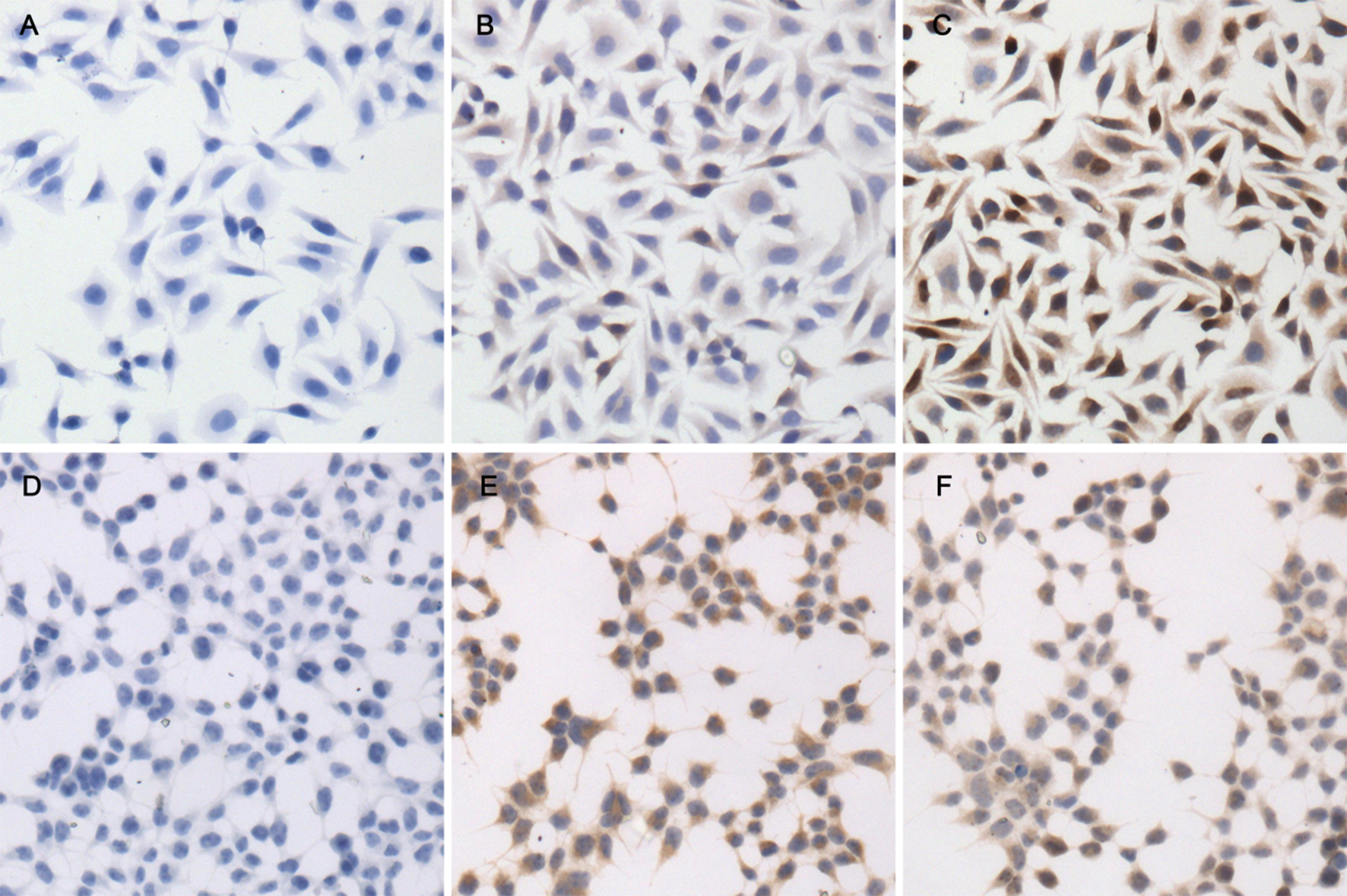
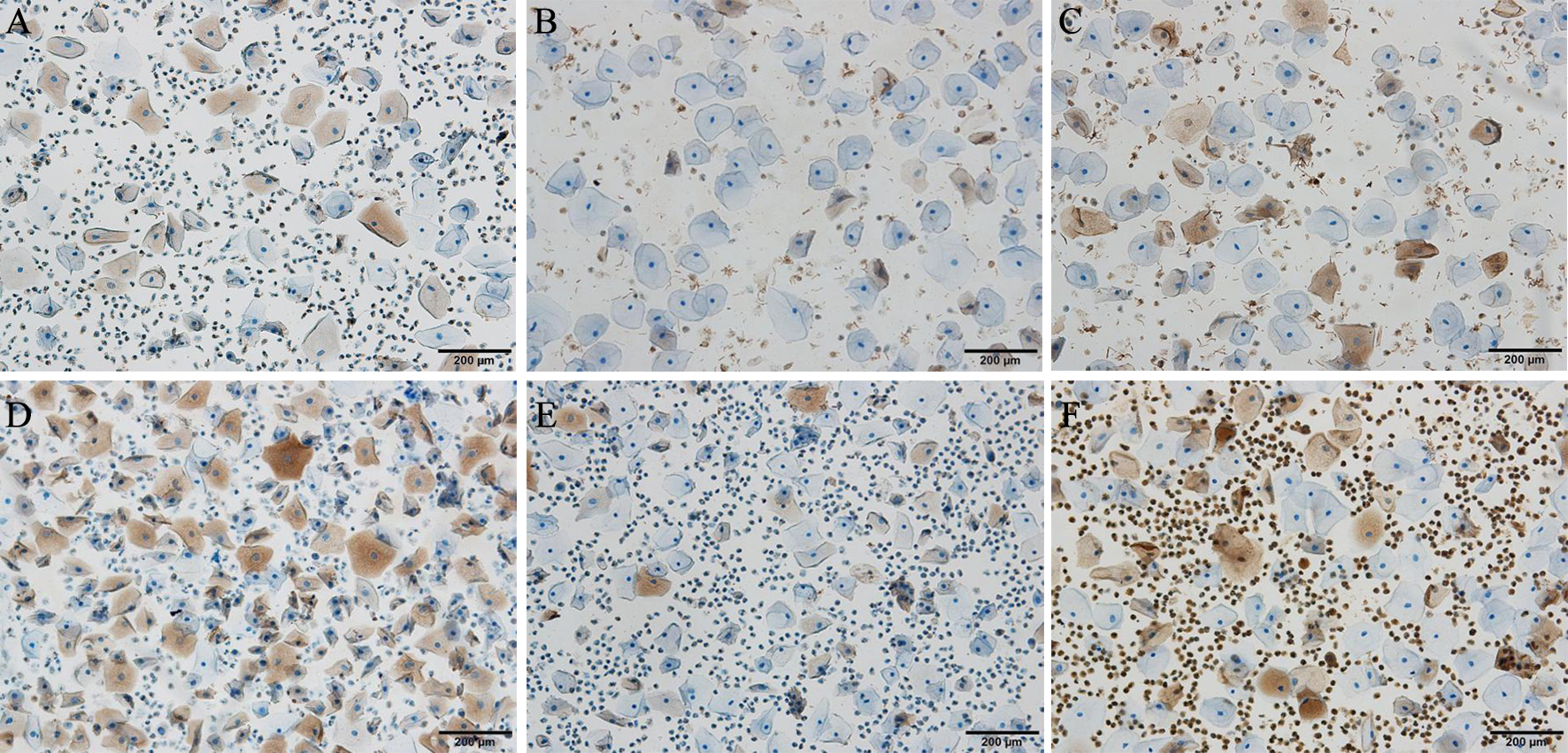
Figure 4.
Representative images of ICC in cervical exfoliated cells obtained from normal women and patients with cervical intraepithelial neoplasia (CIN). (A) FHIT expression in exfoliated cells obtained from normal tissue. (B) FHIT expression in exfoliated cells obtained from CIN1 tissue. (C) FHIT expression in exfoliated cells obtained from CIN3 tissue. (D) C-MYC expression in exfoliated cells obtained from normal tissue. (E) C-MYC expression in exfoliated cells obtained from CIN1 tissue. (F) C-MYC expression in exfoliated cells obtained from CIN3 tissue. Original magnification
Next, ICC was performed to evaluate FHIT and C-MYC expression in HeLa and HEK293 cells. As shown in Fig. 3, strong dark brown positive staining for FHIT was observed in the cytoplasm of HEK293 cells, while only light brown staining was observed in HeLa cells. For C-MYC, strong dark brown positive staining was observed in the nuclei of HeLa cells, while only light brown staining was observed in HEK293 cells. These figures demonstrate that FHIT and C-MYC expression levels are different between normal human cells and cervical carcinoma cells.
Furthermore, we performed ICC on cytology slides obtained from eligible patient samples (see representative images in Fig. 4). This study included 95 patients with CIN1
Table 3
Comparison of FHIT and c-MYC immunocytochemical staining scores in cervical exfoliated cells obtained from patients with CIN1
| Variable | CIN1 | CIN2 |
|
|---|---|---|---|
| Age, | 40.0 (35.0–46.0) | 42.5 (32.5–47.25) | 0.483 |
| FHIT | 0.750 (0.500–0.890) | 0.310 (0.208–0.510) | |
| C-MYC | 0.350 (0.230–0.540) | 1.005 (0.578–1.290) |
FHIT: fragile histidine triad; CIN: cervical intraepithelial neoplasia; CIN1
Table 4
Results of FHIT and c-MYC immunocytochemical staining and LCT in different cervical lesions
| Subgroup | Result | FHIT, no (%) | C-MYC, no (%) | LCT, no (%) |
|---|---|---|---|---|
| Normal ( |
| 17 (23.29) | 14 (19.18) | 13 (17.81) |
|
| 56 (76.71) | 59 (80.82) | 60 (82.19) | |
| CIN1 ( |
| 7 (31.82) | 5 (22.73) | 8 (36.36) |
|
| 15 (68.18) | 17 (77.27) | 14 (63.64) | |
| CIN2 ( |
| 33 (70.21) | 30 (63.83) | 26 (55.32) |
|
| 14 (29.79) | 17 (36.17) | 21 (44.68) | |
| CIN3 and ICC ( |
| 48 (87.27) | 45 (81.82) | 44 (80.00) |
|
| 7 (12.73) | 10 (18.18) | 11 (20.00) |
FHIT: fragile histidine triad; LCT: liquid-based cytology test; CIN: cervical intraepithelial neoplasia; ICC: invasive cervical cancer.
Figure 5.
The receiver operating characteristic (ROC) curves of immunocytochemistry (ICC) staining and a liquid-based cytology test (LCT) for detecting high-grade cervical intraepithelial neoplasia (CIN).
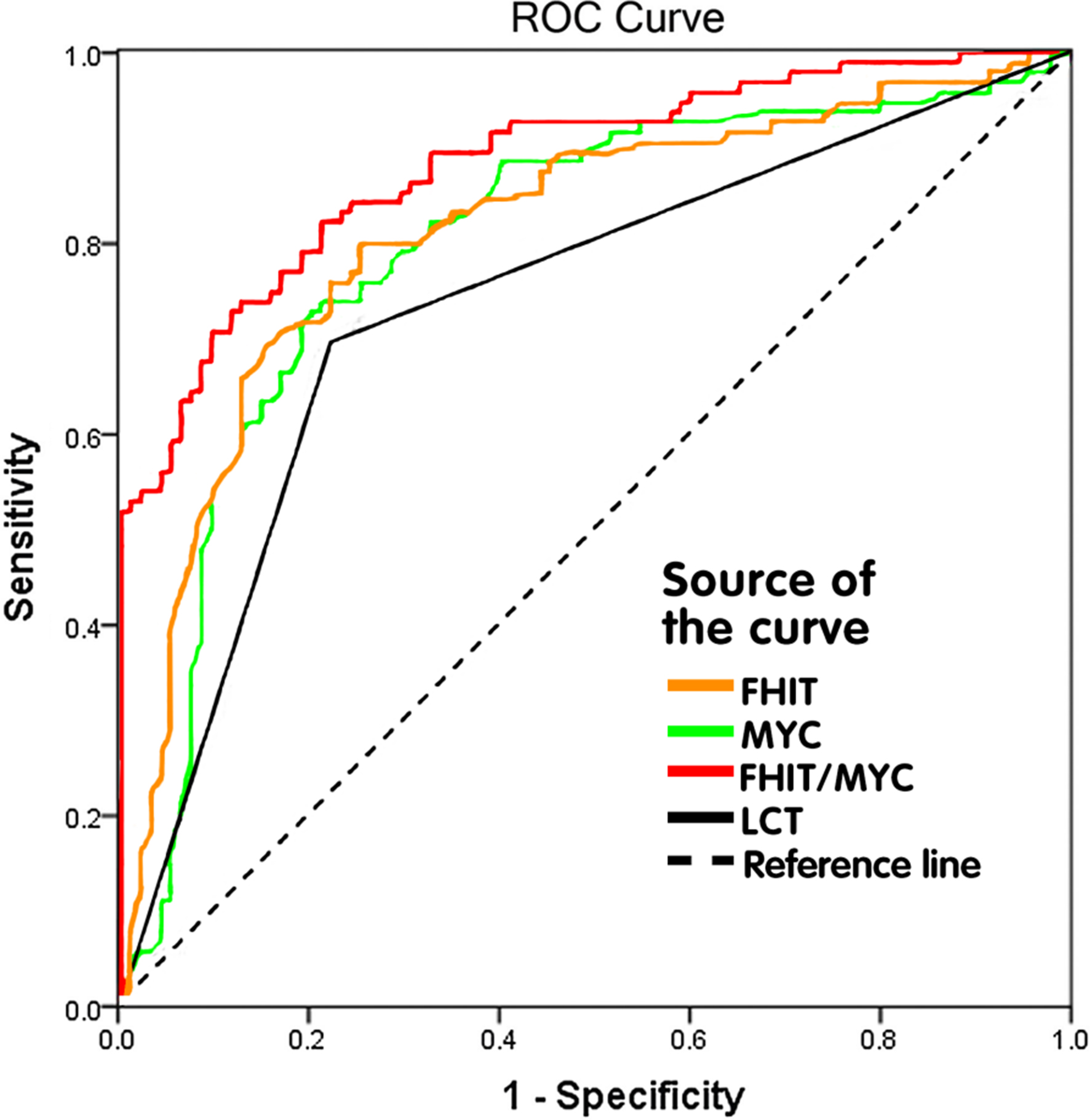
To evaluate the diagnostic efficiency of FHIT and C-MYC ICC staining in cervical exfoliated cells as a strategy for detecting CIN2
Table 5
Comparison of the diagnostic efficiency of FHIT and c-MYC expression and LCT for detecting high-grade CIN
| Test | AUC (95%CI) |
| Sensitivity, % |
| Specificity, % |
| PPV, % |
| NPV, % |
|
|---|---|---|---|---|---|---|---|---|---|---|
| FHIT | 0.805 (0.743–0.867) | 79.41 | 0.04 | 74,74 | 0.61 | 77.14 | 0.90 | 77.17 | 0.17 | |
| C-MYC | 0.814 (0.752–0.876) | 73.53 | 0.28 | 80.00 | 0.72 | 79.79 | 0.58 | 73.79 | 0.40 | |
| FHIT/C-MYC | 0.875 (0.825–0.925) | 73.50 | 0.58 | 89.50 | 0.03 | 88.24 | 0.04 | 75.89 | 0.31 | |
| LCT | 0.723 (0.651–0.795) | 66.67 | 77.89 | 76.40 | 68.52 |
FHIT: fragile histidine triad; LCT: liquid-based cytology test; CIN: cervical intraepithelial neoplasia; AUC: area under curve; PPV: positive predictive value; NPV: negative predictive value; P value from Pearson’s chi-squared test.
5.Discussion
In recent years, the preferred strategy for primary cervical cancer screening has gradually shifted from Pap cytology to the HPV test. Compared to cytology, the HPV test is a highly sensitive and objective test with little interobserver variation. HPV primary screening has been recommended as the preferred strategy for national cervical cancer screening programs in the U.S. and some European countries. According to the 3-year prospective ATHENA study conducted in the U.S., HPV primary screening is as effective as the HPV and Pap cotest screening strategy in detecting CIN3
ICC staining is ideal as a tool for stratified screening triage in HPV-positive women. ICC staining is conducted using liquid-based cytology slides prepared from cervical exfoliated cells, which are easy to obtain via a minimally invasive procedure and relatively inexpensive to process. Furthermore, the evaluation of ICC avoids the need to interpret cell morphological changes and could be automated by computer, thereby reducing interobserver discrepancies and dependence on cytologists. A number of ICC molecular biomarkers have been proposed for cervical cancer screening. However, a qualified biomarker should reflect the integration status of HR-HPV as well as the level of cellular atypia, rather than the presence of HR-HPV. P16 and Ki-67 immunostaining of cervical cytology specimens has become one of the most promising triage techniques being used in cervical cancer screening in recent years. Coexpression of the anti-proliferative p16 protein and the proliferation marker Ki-67 indicates high-risk HPV DNA expression and HPV-induced cell cycle deregulation [19]. Many studies have confirmed that p16/Ki-67 dual-stained cytological specimens have high specificity for CIN3
FHIT and C-MYC are two hot spot genes shown to be located in high frequency loci for HPV integration in previous study. FHIT, which is located at 3p14.2, works as a tumor suppressor gene and is frequently reduced in expression in many types of malignancies, such as lung cancer [22], esophageal cancer [23], and oropharyngeal squamous cell carcinoma [24]. FHIT gene inactivation was found to be strongly correlated with 5’-CpG island hypermethylation, and reduced FHIT expression was significantly correlated with the transition of CIN to cervical cancer [25]. C-MYC, which located at 8q24, encodes a member of the helix-loop-helix/leucine zipper oncogenic transcription factor family. The transcription factor C-MYC regulates a variety of cellular processes associated with immortalization and transformation, such as the cell cycle, cell differentiation, metabolism, angiogenesis, and genomic instability [26, 27, 28, 29]. Previous reports showed that C-MYC was upregulated in CIN and cervical cancer specimens, and that the C-MYC amplification rate increased with the CIN grade [30]. These findings imply that variation in FHIT and C-MYC expression is associated with the severity of cervical lesions and plays an important role in CIN evolution to cervical cancer. As far as we know, this is the first study to show that ICC for FHIT and C-MYC could be used for cervical cancer screening. We used ROC curve analysis to explore the potential of FHIT and C-MYC as diagnostic biomarkers to differentiate low-grade CIN from high-grade CIN. Compared to Pap cytology, FHIT detection had a higher AUC and significantly higher sensitivity in identifying high-grade CIN, whereas C-MYC showed no such significant difference in diagnostic performance parameters except for in AUC values. The combination of these biomarkers further improved the AUC, specificity and PPV further without decreasing sensitivity and NPV. The combination FHIT/C-MYC test had significantly higher specificity and PPV than was found for any individual test or Pap cytology, which is very appealing for stratified screening triage in HR-HPV positive women.
There are some limitations to our study. The study population was composed of women who asked for cervical lesion screening in outpatient clinics, and the screening results were all HR-HPV-positive. This may have led to biases, such as higher HSIL and CIN3
In conclusion, our study demonstrates that in histology and cytology samples, FHIT and C-MYC protein expression is correlated with the severity of cervical lesions during the transition from low-grade CIN to high-grade CIN. The utility of FHIT and C-MYC ICC staining in cervical exfoliated cells for detecting CIN2
Acknowledgments
We appreciate the help of Prof. Li Yu and Dr. Tian Tian for pathological diagnoses and guidance.
Conflict of interest
The authors report no conflicts of interest.
References
[1] | C. Fitzmaurice, C. Allen, R.M. Barber et al., Global, regional and national cancer incidence mortality years of life lost years lived with disability and disability-Adjusted life-years for 32 cancer groups 1990 to 2015: A systematic analysis for the global burden of disease study, Jama Oncol 3: ((2017) ), 524–548. |
[2] | C. Fitzmaurice, D. Dicker, A. Pain et al., The global burden of cancer 2013, Jama Oncol 1: ((2015) ), 505–527. |
[3] | M.H. Mayrand, E. Duarte-franco, I. Rodrigues et al., Human papillomavirus DNA versus papanicolaou screening tests for cervical cancer, N Engl J Med 357: ((2007) ), 1579–1588. |
[4] | P.E. Castle, M.H. Stoler, T.J. Wright, A. Sharma, T.L. Wright and C.M. Behrens, Performance of carcinogenic human papillomavirus (HPV) testing and HPV16 or HPV18 genotyping for cervical cancer screening of women aged 25 years and older: A subanalysis of the ATHENA study, Lancet Oncol 12: ((2011) ), 880–890. |
[5] | G. Ronco, P. Giorgi-rossi, F. Carozzi et al., Results at recruitment from a randomized controlled trial comparing human papillomavirus testing alone with conventional cytology as the primary cervical cancer screening test, J Natl Cancer Inst 100: ((2008) ), 492–501. |
[6] | Practice Bulletin No. 168, cervical cancer screening and prevention, Obstet Gynecol 128: ((2016) ), e111–e130. |
[7] | W.K. Huh, K.A. Ault, D. Chelmow et al., Use of primary high-risk human papillomavirus testing for cervical cancer screening: Interim clinical guidance, Gynecol Oncol 136: ((2015) ), 178–182. |
[8] | J. Monsonego, [EUROGIN 2010: Roadmap on cervical cancer prevention], Gynecol Obstet Fertil 39: ((2011) ), 462–467. |
[9] | J.T. Cox, P.E. Castle, C.M. Behrens, A. Sharma, T.J. Wright and J. Cuzick, Comparison of cervical cancer screening strategies incorporating different combinations of cytology HPV testing and genotyping for HPV 16/18: Results from the ATHENA HPV study, Am J Obstet Gynecol 208: ((2013) ), 181–184. |
[10] | R. Luttmer, M.G. Dijkstra, P.J. Snijders et al., p16/Ki-67 dual-stained cytology for detecting cervical (pre)cancer in a HPV-positive gynecologic outpatient population, Mod Pathol 29: ((2016) ), 870–878. |
[11] | R.E. Badr, A.E. Walts, F. Chung and S. Bose, BD proEx c: A sensitive and specific marker of HPV-associated squamous lesions of the cervix, Am J Surg Pathol 32: ((2008) ), 899–906. |
[12] | A. Boers, R.P. Bosgraaf, van Leeuwen et al., DNA methylation analysis in self-sampled brush material as a triage test in hrHPV-positive women, Br J Cancer 111: ((2014) ), 1095–1101. |
[13] | Q. Tian, Y. Li, F. Wang et al., MicroRNA detection in cervical exfoliated cells as a triage for human papillomavirus-positive women, J Natl Cancer Inst 106. ((2014) ). |
[14] | M. Schmitz, C. Driesch, K. Beer-grondke, L. Jansen, I.B. Runnebaum and M. Durst, Loss of gene function as a consequence of human papillomavirus DNA integration, Int J Cancer 131: ((2012) ), e593–e602. |
[15] | Z. Hu, D. Zhu, W. Wang et al., Genome-wide profiling of HPV integration in cervical cancer identifies clustered genomic hot spots and a potential microhomology-mediated integration mechanism, Nat Genet 47: ((2015) ), 158–163. |
[16] | F. Pichiorri, H. Okumura, T. Nakamura et al., Correlation of fragile histidine triad (Fhit) protein structural features with effector interactions and biological functions, J Biol Chem 284: ((2009) ), 1040–1049. |
[17] | C.M. Shachaf and D.W. Felsher, Tumor dormancy and MYC inactivation: Pushing cancer to the brink of normalcy, Cancer Res 65: ((2005) ), 4471–4474. |
[18] | T.C. Wright, M.H. Stoler, C.M. Behrens, A. Sharma, G. Zhang and T.L. Wright, Primary cervical cancer screening with human papillomavirus: End of study results from the ATHENA study using HPV as the first-line screening test, Gynecol Oncol 136: ((2015) ), 189–197. |
[19] | D.M. von KNEBEL, New markers for cervical dysplasia to visualise the genomic chaos created by aberrant oncogenic papillomavirus infections, EUR J CANCER 38: ((2002) ), 2229–2242. |
[20] | N. Wentzensen, L. Schwartz, R.E. Zuna et al., Performance of p16/Ki-67 immunostaining to detect cervical cancer precursors in a colposcopy referral population, Clin Cancer Res 18: ((2012) ), 4154–4162. |
[21] | R.M. Ebisch, van der Horst, M. Hermsen et al., Evaluation of p16/Ki-67 dual-stained cytology as triage test for high-risk human papillomavirus-positive women, Mod Pathol 30: ((2017) ), 1021–1031. |
[22] | R. Maruyama, K. Sugio, I. Yoshino, Y. Maehara and A.F. Gazdar, Hypermethylation of FHIT as a prognostic marker in nonsmall cell lung carcinoma, Cancer-am Cancer Soc 100: ((2004) ), 1472–1477. |
[23] | T. Noguchi, S. Takeno, Y. Kimura et al., FHIT expression and hypermethylation in esophageal squamous cell carcinoma, INT J MOL MED 11: ((2003) ), 441–447. |
[24] | G. Gao, J.L. Kasperbauer, N.M. Tombers, V. Wang, K. Mayer and D.I. Smith, A selected group of large common fragile site genes have decreased expression in oropharyngeal squamous cell carcinomas, Genes Chromosomes Cancer 53: ((2014) ), 392–401. |
[25] | E. Giarnieri, N. Zanesi, A. Bottoni et al., Oncosuppressor proteins of fragile sites are reduced in cervical cancer, Cancer Lett 289: ((2010) ), 40–45. |
[26] | N. Meyer and L.Z. Penn, Reflecting on 25 years with MYC, NAT REV CANCER 8: ((2008) ), 976–990. |
[27] | Y. Lu, Y. Wu, X. Feng et al., CDK4 deficiency promotes genomic instability and enhances myc-driven lymphomagenesis, J Clin Invest 124: ((2014) ), 1672–1684. |
[28] | M. Dews, J.L. Fox, S. Hultine et al., The myc-miR-17 ∼ 92 axis blunts TGFβ signaling and production of multiple TGFβ-dependent antiangiogenic factors, CANCER RES 70: ((2010) ), 8233–8246. |
[29] | M.T. Gomez-casares, E. Garcia-alegria, C.E. Lopez-jorge et al., MYC antagonizes the differentiation induced by imatinib in chronic myeloid leukemia cells through downregulation of p27 (KIP1)., Oncogene 32: ((2013) ), 2239–2246. |
[30] | F.B. Guijon, K. Greulich-bode, M. Paraskevas, P. Baker and S. Mai, Premalignant cervical lesions are characterized by dihydrofolate reductase gene amplification and c-Myc overexpression: Possible biomarkers, J Low Genit Tract Dis 11: ((2007) ), 265–272. |


