
Breast gel based on Boswellia serrata, Betaine and myo-Inositol improves cyclic mastodynia in fertile women: A retrospective clinical study
Abstract
BACKGROUND:
The management of mastodynia plays a central role in improving women quality of life. Despite its high occurrence, specific therapeutic guidelines for mastalgia are still lacking. Available therapies include unspecific anti-inflammatories, even though they may often expose to undesirable effects and low compliance.
OBJECTIVE:
The aim of this study was to highlight the efficacy of the topical application of combined natural molecules including Boswellia serrata, Betaine and myo-Inositol in improving cyclic mastalgia.
METHODS:
In this retrospective pilot clinical study, patients with cyclic mastalgia applied a specific breast gel for three months. The severity of the pain was measured through the Visual Analogue Score (VAS) in the treated group compared to untreated one. Treated patients also filled in a questionnaire evaluating acceptance and safety of the breast gel.
RESULTS:
This pilot clinical study demonstrated for the first time the efficacy of the topical application of a breast gel based on Betaine, Boswellia serrata, and myo-Inositol in improving cyclic mastodynia. The completed questionnaires also revealed high levels of acceptance, as both safety and compliance.
CONCLUSIONS:
Besides confirming the positive effects of these natural molecules in the management of conditions affecting breast physiology – so far evaluated as oral supplementation – the obtained results pave the way for further studies supporting the use of such molecules as a tailored medical device in the management of breast pain, thus also opening toward a combined oral and topical approach.
1.Introduction
Mastodynia is a medical term referring to the common symptom of breast pain, also known as mastalgia. Both women and men can experience such condition, even if it occurs much more frequently in women [1]: approximately 60 to 70% of women experience mastalgia during their lifetime [2].
Breast pain can be categorized in three types: (i) cyclic mastalgia (occurring during the luteal phase of the menstrual cycle), (ii) non-cyclic mastalgia (often related to internal anatomical changes, injuries, surgical procedures, infections, or sometimes with other breast pathologies, i.e., breast cysts or fibroadenoma) and (iii) extramammary pain (as musculoskeletal tenderness or pain associated with breast discomfort that can actually mimic breast pain) [3].
Differences in pain history and the occurrence of specific symptoms may help to differentiate cyclic and non-cyclic breast pain: the former is typically bilateral and diffuse, while the non-cyclic mastalgia may involve continuous or intermittent pain that does not align with the menstrual cycle [4]. In addition, to support a clear differential diagnosis between cyclic and non-cyclic breast pain, physicians recommend using daily diaries. Patients complete the pain diary, such as the pain chart devised at Cardiff Mastalgia clinic [5], in which they can note their experience on a day-to-day basis over a two-month period over two menstrual cycles.
Cyclic mastalgia is very frequent, about 68% of women aged 18–44 years have complained about such condition [6]. Cyclic pain likely arises from a disturbance in hormonal balance between estrogens, progesterone (in terms of reduced production) [7], prolactin (as hyperprolactinemia) [8,9], and the responsiveness of the target tissues to these hormones. Other factors may contribute to cyclic mastalgia such as nutritional and psychological causes, water retention in the body, and body and breast weight gain [10].
The severity of the pain typically varies from mild to severe pain, and it is clinically recorded by using validated scales such as the Visual Analogue Scale (VAS), which is a unidimensional pain rating system [11–14].
The two most common concerns of patients suffering from mastalgia are (i) the fear of having breast cancer and (ii) the presence of a pain that affects daily activities. Indeed, breast pain often influences patients’ mood by provoking anxiety and concerns [15], interfering with social, sexual, and physical activities [16].
Despite the high frequency and lifestyle impairment, specific therapeutic guidelines for mastalgia do not adequately meet patients’ needs. Considering the potential for emotional concern, one of the first-line management strategies for the breast pain is to reassure patients that they do not have a breast cancer [17]. Furthermore, the advice of wearing a good bra-fitting advice [18], as this may be represent a source of mastalgia, should accompany the first-step management. Indeed, recent evidence estimates that up to 70% of women wear improperly fitted bras, especially for women with large mammary glands [19].
Topical nonsteroidal anti-inflammatory drugs and endocrine drugs are effective at providing mastalgia relief [20]; however, they potentially may expose to undesirable effects (menstrual irregularities, hot flashes, vaginal dryness, low libido, mood swings, etc) that may limit their use and impair patients’ compliance [21,22]. Examples of pharmacological approaches include bromocriptine, tamoxifen and danazol, which is the only US FDA approved medication for the treatment of mastalgia. However, a randomized clinical trial on 200 women with mastalgia reported a higher improvement in breast pain symptoms in those women who wore sports brassieres for 12 weeks compared to those treated with danazol. The danazol group had 58% relief of symptoms (with 42% showing adverse drug related side effects), while in the brassiere group, 85% had relief of symptoms with improved lifestyle [19]. Indeed, many patients respond more favourably to non-pharmacologic measures [23] designed to treat symptoms of benign breast pain.
In this scenario, previous works have highlighted the benefits of the oral combination of natural molecules including Boswellia serrata, Betaine, and Myo-inositol (Myo-Ins) in breast physiology. Myo-Ins is a cyclic alcohol, which plays a central role in modulating inflammation, metabolic-endocrine processes, and oxidative damage in several human diseases, including polycystic ovary syndrome (PCOS), metabolic syndrome, and cancer [24–27]. Previous studies also revealed positive effects of the oral administration of myo-Ins in improving mastalgia in women suffering from PCOS or premenstrual dysphoric syndrome [28,29]. In addition, in vitro experiments revealed the anti-inflammatory and anti-fibrotic activity of myo-Ins by reducing levels of Transforming Growth Factor-β (TGF-β), fibronectin and type I collagen [27].
In the same vein, a recent review highlighted the anti-inflammatory properties of Boswellic acid – the active ingredient of Boswellia serrata – acting on several factors and enzymes, including nuclear factor-κB (NF-kB), Cyclooxygenase-2 (COX-2), and 5-lipoxygenese (5-LO) [30]. Accumulating evidence also reported the anti-inflammatory role of Betaine [31]. This latter may inhibit proteins involved in inflammatory and oxidative processes, in particular by counteracting the signalling of NF-kB and pro-inflammatory down-stream genes (TNF-α, IL-1β, IL-23). This property of Betaine, along with its role as osmoprotectant and methyl group donor, may negatively regulate NF-kB, NLRP3 inflammasome and improve oxidative stress [31].
Furthermore, clinical studies have reported the effectiveness of the oral combination of Betaine, Boswellia and Myo-Ins in improving different conditions affecting mammary gland physiology, as high breast density, mastalgia, fibroadenoma [32,33].
Therefore, considering the positive effects of such molecules on breast physiology, taken as an oral dietary supplement, the aim of this study was to evaluate for the first time the efficacy of the topical application of a designed breast gel based on Boswellia, Betaine and Myo-Ins in improving cyclic mastalgia in fertile women.
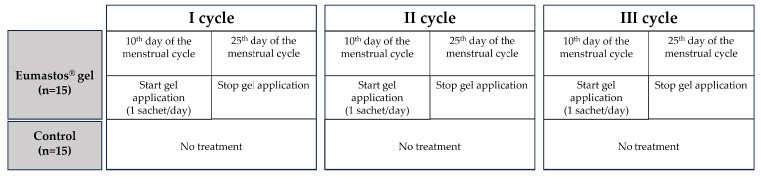
Fig. 1.
Flow chart of the retrospective study. The flow chart represents the two groups of the study and the timing of using the breast gel.
2.Materials and methods
2.1.Study design and patients
This is a retrospective clinical pilot study in which physicians collected data from 30 fertile patients aged between 20 and 45 years old. Informed consent was obtained from all individual participants. Patients were followed privately at Agunco Obstetric and Gynecologic centre (Rome, Italy), following the Ethical Principles of the Helsinki Declaration and the national law. All retrospective data collected were de-identified prior to access by the authors.
All the analysed data included patients affected by cyclic mastodynia. To define the cyclic or non-cyclic nature of the breast pain, during the three months prior to the study, women fulfilled a daily diary according to the Cardiff Breast Score Chart. Only women suffering from severe mastodynia in the last three months were diagnosed as cyclic mastodynia. In addition, physicians excluded from the analysis retrospective data derived from women (i) in pregnancy or breastfeeding, (ii) in menopause, (iii) with previous episodes of breast tumours or familiarity for such pathology, (iv) and from the ones taking hormonal therapies within four months before the beginning of the study.
We compared retrospective data from patients using the breast gel (n = 15) containing Boswellia serrata, Myo-Ins and Betaine (Eumastos® gel, Lo.Li. pharma s.r.l., Rome, Italy and distributed by Farmares, Rome, Italy) with retrospective data from patients who did not receive any treatments for cyclic breast pain (n = 15).
The treatment consisted of 1 sachet (2.5 g) applied on the breast once daily, from the 10th to the 25th day of the menstrual cycle, as this is the period during the which cyclic mastalgia usually occurs. This administration was repeated for three menstrual cycles, so for a total of three months of observation (Fig. 1).
2.2.Evaluation of cyclic mastodynia and intensity of breast pain
The collected retrospective records derived only from those women with a clear diagnosis of cyclic mastalgia, gained through the filling of the Cardiff Breast Score Chart during the three months before the study.
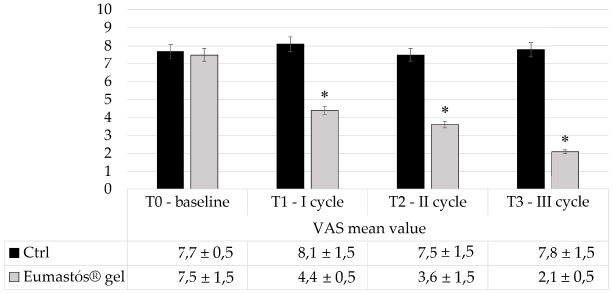
Fig. 2.
VAS records at the baseline and throughout the application of the gel. Records of the Visual Analogue Scale (VAS) evaluation throughout the period of breast gel application. At T1, T2 and T3 patients using Eumastos® gel experienced a significant improvement in breast pain compared to the untreated group (Ctrl) (*p value < 0.01).
Throughout the period of application of the medical device, patients monitored the intensity of the breast pain by using the VAS system. It is a one-dimensional, easy-to-use tool that consists in a pain rating system evaluating the intensity of the pain [34]. Related scores are based on self-reported measures of symptoms in a range between 0 and 10. They are recorded with a single handwritten mark placed at one point along the length of a 10-cm line: “no pain” on the left end (0 cm) of the scale and the “worst pain” on the right end of the scale (10 cm). Most experts on mastalgia consider any pain of ≥3 on a VAS of 0 to 10, to be significantly severe to require therapy [12]. The values are useful to track pain intensity progression and the score is calculated in millimetre – and converted in centimetre (cm) – by measuring the length of the line between the lowest intensity on the left-end and the handwritten mark placed by the patient. A work by Boonstra and colleagues aimed to find the cut-off points on the VAS to distinguish among mild, moderate and severe pain. In particular, they defined VAS scores ≤3.4 cm corresponded to mild pain, scores of 3.5–6.4 cm to moderate interference with functioning, and scores ≥6.5 cm to severe interference [35].
The participants underwent breast clinical examination at the baseline (T0) and each subsequent month, after the first cycle of application (T1), the second (T2) and the third one (T3). At each timepoint, VAS evaluation and possible side effects were recorded. In addition, at the end of the three months of breast gel application, the patients filled another questionnaire on the efficacy of the entire therapy, on potential adverse effects and the related compliance.
2.3.Statistical analysis
Statistical analysis was performed by using unpaired t-test to compare variation in the VAS scores between patients treated with the breast gel and the controls. The level of statistical significance was set for p value below 0.05.
3.Results
Physicians collected retrospective records from VAS evaluation at the baseline and throughout the following three months for all the patients.
At T0 the treated and the untreated groups exhibited no significant differences in breast pain evaluation: both the arms reported a severe grading of the VAS score (7.7 cm ± 0.5 in control group vs 7.5 cm ± 1.5 treated group).
After one month commencement of the breast gel (T1), the patients experienced a significant improvement in cyclic mastodynia compared to the untreated patients. The mean value of the VAS records was 4.4 cm ± 0.5 following the first application, while in the untreated group it remained constant at 8.1 cm ± 1.5 (p value < 0.01 between the groups). Thus, treated patients felt beneficial effects of the gel from the first application and experienced an improvement from severe to moderate intensity of the pain, as indicated by the mean values of the VAS scores (Fig. 2).
Cyclic mastodynia further improved in the following months (Fig. 2): the reported mean value of the VAS scores was 3.6 cm ± 1.5 at T2, and 2.1 cm ± 0.5 at T3, signifying a lower intensity of pain. Meanwhile, in the untreated women the reported mean values of the VAS scores were constant throughout the entire period of observation (7.5 cm ± 1.5 at T2, 7.8 cm ± 1.5 at T3).
In addition, retrospective data on patients’ compliance and gel efficacy and safety were collected. After three months of application, patients evaluated the efficacy of such medical device according to a scale ranging from 0 (no effect) to 4 (excellent). As reported in Fig. 3A, 86.7% of patients (13/15) self-evaluated an excellent efficacy of the gel, with no scores of 0 or 1 being reported, thus indicating a good degree of patient satisfaction regarding the application.
Fig. 3.
Patients’ compliance and perception of efficacy and safety of the medical device. At T3 patients expressed their thoughts about efficacy (A) and safety (B) of the medical device and reported their compliance to the treatment (C).
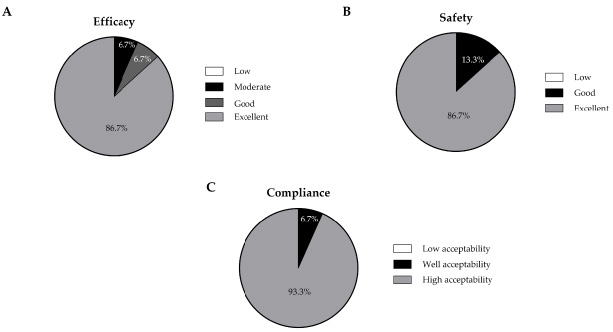
Regarding the safety, at each breast clinical examination, patients recorded the eventual adverse effects that had occurred during treatment. The safety of the gel was ranked using the 0 (low safety) to 3 (excellent safety) scale. As reported in Fig. 3B, the safety of the medical device was considered excellent by 86.7% (13/15) and good by 13.3% patients (2/15), with no patients gave a score of low or sufficient safety.
In line with the other results, compliance was also excellent: each patient evaluated the acceptability of the treatment by using a scale of three points ranging from “low acceptability” to “high acceptability”. As reported in Fig. 3C, none of the patients treated with the breast gel reported a low acceptable compliance, instead 93.3% reported a high compliance and only 6.7% reported a good compliance.
4.Discussion
In this clinical study, physicians found that the topical application of combined natural molecules, including Betaine, Boswellia serrata, and Myo-Ins, is effective in reducing breast pain related to cyclic mastodynia.
Cyclic mastalgia is a common condition referring to a specific type of breast pain usually concurring with the menstrual cycle. Hormonal unbalances between estrogens, progesterone, and prolactin, as well as several other factors such as nutrition, weight gain, water retention, may contribute to its development.
Various studies have already demonstrated that the above mentioned natural molecules have a protective effect in the physiology of mammary gland [32,33,36]. Previous studies have reported the effect of Myo-Ins in modulating inflammatory, metabolic, oxidative and endocrine processes in a wide array of pathological contexts [24–27], as well as both Boswellic acid and Betaine may help counteract inflammation and exert protective effects on breast physiology [30,37,38].
The obtained results are in line with previous clinical studies evaluating the effect of orally taken Betaine, Boswellia and Myo-Ins on breast physiology. A randomized clinical study investigated their effectiveness in the treatment of symptomatic fibroadenomas [36] in young women, thus reporting a reduction in dimensions and a modulation of inflammatory, metabolic, oxidative, and endocrine processes. The oral treatment with Beatine, Boswellia and Myo-Ins restored mammary gland physiology, without the side effects typically associated with pharmacological intervention. These results are in agreement with a previous study in which the oral administration of Betaine, Boswellia and Myo-Ins improved both clinical symptoms and radiological signs of high breast density in those women with extremely dense breasts [32]. Furthermore, another clinical study in premenopausal women demonstrated that orally taken Betaine, Boswellia serrata and Myo-Ins, restored breast physiology by reducing mammary density and also induced an improvement in breast pain [33].
Besides the physical pain, women affected by cyclic mastalgia also experience emotive concerns regarding the fear to have a breast cancer and the affection of their social, sexual and daily activities. For this reason, in the management of breast pain improving quality of daily life plays a crucial role for such patients. Typically, patients are well-disposed to non-pharmacological approaches, because molecules such as danazol, tamoxifen, bromocriptine, or other anti-estrogenic treatments may expose patients to potential adverse effects, limiting their use. In addition, recurrence may occur very often.
The present study reported for the first time the efficacy of a designed breast gel based on Betaine, Boswellia serrata, and Myo-Ins in improving breast cyclic pain. Indeed, previous studies only demonstrated the effectiveness in preserving or recovering breast physiology as orally taken molecules.
Despite the existence of a wide-range of topical low risk anti-inflammatory drugs for the treatment of breast pain [39], this study takes a step forward highlighting that a topical treatment consisting of the same natural molecules designed for the treatment of mastalgia, is effective at improving breast pain. All the women under treatment in this study experienced reduced breast pain early from the first application, while the untreated controls experienced a constant severe pain during the entire period of observation. In addition, the VAS score improved decreasing to values lower than 3 thus below the threshold in which therapy is typically recommended by physicians.
Patients’ self-report indicated high grade of satisfaction of the breast gel treatment in terms of safety, efficacy, and suitability for prolonged use. Furthermore, daily application of a breast gel facilitated self-examination of the breast, thus allowing for constant monitoring and early evaluation in the event of suspected masses, thus providing emotional reassurance for patients.
Of course, the small number of the evaluated individuals, the short-time duration of the observation and the retrospective nature of the study, represent limitations of the study, along with the lack of a prospective placebo-controlled group. However, the obtained results may be useful for opening to future investigations strengthening the use of such natural molecules for the management of breast pain, as combined oral and topical approach in order to optimize therapeutical effect.
5.Conclusion
This pilot clinical study reported for the first time the efficacy of the topical application of a breast gel based on Betaine, Boswellia serrata and Myo-Ins in improving cyclic mastodynia. Such natural molecules have already exhibited a clear efficacy in recovering breast physiology when orally administered; therefore, the obtained findings aim to expand the use of this combined treatment as both oral and topical approach. Aside from confirming the positive effects of the natural molecules against conditions affecting mammary gland physiology, such as cyclic mastodynia, the results of this study pave the way for further clinical studies, with a large population and a prospective placebo-controlled group, supporting the use of these molecules as a topical combined treatment for the management of breast pain.
Conflict of interest
No competing financial interests exist.
Data availability
The datasets generated and analysed during this study are available from the corresponding author upon reasonable request.
Funding
This study received no external funding. The APC is funded by Lo.Li pharma.
Author contributions
M.B. interpreted the data and wrote the original draft of the manuscript. G.M., C.P., G.D.F. collected and analysed the data. L.C. interpreted the data, wrote and revised the manuscript.
All authors have read and approved the final article.
References
[1] | Grullon S, , Bechmann S, Mastodynia, in: StatPearls. Treasure Island (FL), 2023. |
[2] | Dixon M, , Thomas J, Symptoms, assessment and guidelines for referral, in: Dixon M (ed.), ABC of Breast Diseases. Wiley-Blackwell, 2012. |
[3] | Klimberg VS. Etiology and management of breast pain, in: Harris JR, Lippman M, Morrow M, Hellman S (eds), Diseases of the Breast. Lippincott-Raven (Philadelphia), 99–106, 1996. |
[4] | Hubbard TJ, , Sharma A, , Ferguson DJ, Breast pain: assessment, management, and referral criteria, Br J Gen Pract, 70: : 419–420, (2020) . doi:10.3399/bjgp20X712133. |
[5] | Gautam S, , Srivastava A, , Kataria K, , Dhar A, , Ranjan P, , Kumar J, New breast pain chart for objective record of mastalgia, Indian J Surg, 78: : 245–248, (2016) . doi:10.1007/s12262-016-1492-z. |
[6] | Ader DN, , South-Paul J, , Adera T, , Deuster PA, Cyclical mastalgia: prevalence and associated health and behavioral factors, J Psychosom Obstet Gynaecol, 22: : 71–76, (2001) . doi:10.3109/01674820109049956. |
[7] | Sitruk-Ware R, , Sterkers N, , Mauvais-Jarvis P, Benign breast disease I: hormonal investigation, Obstet Gynecol, 53: : 457–460, (1979) . |
[8] | Kumar S, , Mansel RE, , Scanlon MF, , Hughes LE, , Edwards CA, , Woodhead JS , Altered responses of prolactin, luteinizing hormone and follicle stimulating hormone secretion to thyrotrophin releasing hormone/gonadotrophin releasing hormone stimulation in cyclical mastalgia, Br J Surg, 71: : 870–873, (1984) . doi:10.1002/bjs.1800711123. |
[9] | Peters F, , Pickardt CR, , Zimmermann G, , Breckwoldt MP, TSH, and thyroid hormones in benign breast diseases, Klin Wochenschr, 59: : 403–407, (1981) . doi:10.1007/BF01698519. |
[10] | Mirzaee F, , Fakari FR, , Babakhanian M, , Roozbeh N, , Ghazanfarpour M, The effectiveness of herbal medicines on cyclic mastalgia: a systematic review on meta-analysis, Rev Bras Ginecol Obstet, 44: : 972–985, (2022) . doi:10.1055/s-0042-1755456. |
[11] | McCormack HM HD, , Sheather S, Clinical applications of visual analogue scales: a critical review, Psychol Med, 18: : 1007–1019, (1988) . doi:10.1017/s0033291700009934. |
[12] | Wewers ME, , Lowe NK, A critical review of visual analogue scales in the measurement of clinical phenomena, Res Nurs Health, 13: : 227–236, (1990) . doi:10.1002/nur.4770130405. |
[13] | Couper MP, , Tourangeau R, , Conrad FG, , Singer E, Evaluating the effectiveness of visual analog scales: a web experiment, Social Science Computer Review, 24: : 227–245, (2006) . doi:10.1177/0894439305281503. |
[14] | Boonstra AM, , Schiphorst Preuper HR, , Reneman MF, , Posthumus JB, , Stewart RE, Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain, Int J Rehabil Res, 31: : 165–169, (2008) . doi:10.1097/MRR.0b013e3282fc0f93. |
[15] | Sharami SH, , Sobhani AR, , Asgharnia M, , Shabaani M, Prevalence of cyclic mastalgia and it’s relation with age, marriage and employment outside the house, J Guil Uni Med Sci, 9: : 111–116, (2000) . |
[16] | Johnson KM, , Bradley KA, , Bush K, , Gardella C, , Dobie DJ, , Laya MB, Frequency of mastalgia among women veterans. Association with psychiatric conditions and unexplained pain syndromes, J Gen Intern Med, 21: (Suppl 3): S70–75, (2006) . doi:10.1111/j.1525-1497.2006.00378.x. |
[17] | Rosolowich V, , Saettler E, , Szuck B, Mastalgia, J Obstet Gynaecol Can, 28: : 49–71, (2006) . |
[18] | Hafiz SP, , Barnes NLP, , Kirwan CC, Clinical management of idiopathic mastalgia: a systematic review, J Prim Health Care, 10: : 312–323, (2018) . doi:10.1071/HC18026. |
[19] | Hadi MS, Sports brassiere: is it a solution for mastalgia? Breast J, 6: : 407–409, (2000) . doi:10.1046/j.1524-4741.2000.20018.x. |
[20] | Gumm R, , Cunnick GH, , Mokbel K, Evidence for the management of mastalgia, Curr Med Res Opin, 20: : 681–684, (2004) . doi:10.1185/030079904125003377. |
[21] | Olawaiye A, , Withiam-Leitch M, , Danakas G, , Kahn K, Mastalgia: a review of management, J Reprod Med, 50: : 933–939, (2005) . |
[22] | Vonkeman HE, , van de Laar MA, Nonsteroidal anti-inflammatory drugs: adverse effects and their prevention, Semin Arthritis Rheum, 39: : 294–312, (2010) . doi:10.1016/j.semarthrit.2008.08.001. |
[23] | Smith RL, , Pruthi S, , Fitzpatrick LA, Evaluation and management of breast pain, Mayo Clin Proc,, 3: : 353–372, (2004) .. |
[24] | Giordano D, , Corrado F, , Santamaria A, , Quattrone S, , Pintaudi B, , Di Benedetto A , Effects of myo-inositol supplementation in postmenopausal women with metabolic syndrome: a perspective, randomized, placebo-controlled study, Menopause, 18: : 102–104, (2011) . doi:10.1097/gme.0b013e3181e8e1b1. |
[25] | Dona G, , Sabbadin C, , Fiore C, , Bragadin M, , Giorgino FL, , Ragazzi E , Inositol administration reduces oxidative stress in erythrocytes of patients with polycystic ovary syndrome, Eur J Endocrinol, 166: : 703–710, (2012) . doi:10.1530/EJE-11-0840. |
[26] | Shamsuddin A, Anticancer function of phytic acid, International Journal of Food Science and Technology,, 7: : 769–782, (2002) . |
[27] | Monti N, , Dinicola S, , Querqui A, , Fabrizi G, , Fedeli V, , Gesualdi L , Myo-inositol reverses TGF-beta1-induced EMT in MCF-10A non-tumorigenic breast cells, Cancers (Basel), 15: (2023) . doi:10.3390/cancers15082317. |
[28] | Dinicola S, , Chiu TT, , Unfer V, , Carlomagno G, , Bizzarri M, The rationale of the myo-inositol and D-chiro-inositol combined treatment for polycystic ovary syndrome, J Clin Pharmacol, 54: : 1079–1092, (2014) . doi:10.1002/jcph.362. |
[29] | Carlomagno G, , Unfer V, , Silvia B, , Francesco D, Myo-inositol in the treatment of premenstrual dysphoric disorder, Hum Psychopharmacol, 26: : 526–530, (2011) . doi:10.1002/hup.1241. |
[30] | Roy NK, , Parama D, , Banik K, , Bordoloi D, , Devi AK, , Thakur KK , An update on pharmacological potential of boswellic acids against chronic diseases, Int J Mol Sci, 20:: : 4101–4101, (2019) . doi:10.3390/ijms20174101. |
[31] | Zhao G, , He F, , Wu C, , Li P, , Li N, , Deng J , Betaine in inflammation: mechanistic aspects and applications, Front Immunol, 9: : 1070, (2018) . doi:10.3389/fimmu.2018.01070. |
[32] | Pasta V, , Gullo G, , Giuliani A, , Harrath AH, , Alwasel SH, , Tartaglia F , An association of boswellia, betaine and myo-inositol (Eumastos) in the treatment of mammographic breast density: a randomized, double-blind study, Eur Rev Med Pharmacol Sci, 19: : 4419–4426, (2015) . |
[33] | Pasta V, , Dinicola S, , Giuliani A, , Harrath AH, , Alwasel SH, , Tartaglia F , A randomized pilot study of inositol in association with Betaine and Boswellia in the management of mastalgia and benign breast lump in premenopausal women, Breast Cancer (Auckl), 10: : 37–43, (2016) . doi:10.4137/BCBCR.S38408. |
[34] | Alexander I, Electronic medical records for the orthopaedic practice, Clin Orthop Relat Res Nurs Health, 114–119, (2007) . |
[35] | Boonstra AM, , Schiphorst Preuper HR, , Balk GA, , Stewart RE, Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain, Pain, 155: : 2545–2550, (2014) . doi:10.1016/j.pain.2014.09.014. |
[36] | Pasta V, , Dinicola S, , Giuliani A, , Harrath AH, , Alwasel SH, , Tartaglia F , A randomized trial of Boswellia in association with betaine and myo-inositol in the management of breast fibroadenomas, Eur Rev Med Pharmacol Sci, 20: : 1860–1865, (2016) . |
[37] | Go EK, , Jung KJ, , Kim JY, , Yu BP, , Chung HY, Betaine suppresses proinflammatory signaling during aging: the involvement of nuclear factor-kappaB via nuclear factor-inducing kinase/IkappaB kinase and mitogen-activated protein kinases, J Gerontol A Biol Sci Med Sci, 60: : 1252–1264, (2005) . doi:10.1093/gerona/60.10.1252. |
[38] | Detopoulou P, , Panagiotakos DB, , Antonopoulou S, , Pitsavos C, , Stefanadis C, Dietary choline and betaine intakes in relation to concentrations of inflammatory markers in healthy adults: the ATTICA study, Am J Clin Nutr, 87: : 424–430, (2008) . doi:10.1093/ajcn/87.2.424. |
[39] | Colak T, , Ipek T, , Kanik A, , Ogetman Z, , Aydin S, Efficacy of topical nonsteroidal antiinflammatory drugs in mastalgia treatment, J Am Coll Surg, 196: : 525–530, (2003) . doi:10.1016/S1072-7515(02)01893-8. |


