
Nipple-sparing mastectomy and immediate breast reconstruction by prepectoral implant for the management of giant phyllodes tumors: A case series
Abstract
Phyllodes tumor is an uncommon breast neoplasm that is present in variable sizes. Giant phyllodes are those larger than 10 cm in diameter. Clinically, giant phyllodes tumors present as a visible, rapidly growing mass distorting the breast contour. Such tumors with large size and rapid growth rate suggest a phyllode diagnosis of fibroadenoma. Planning a standard treatment strategy for these tumors is quite challenging. While adequate surgical excision with tumor-free resection margins is the standard of care for most giant phyllodes cases, borderline and malignant giant phyllodes tumors might require wider resections given their high recurrence rates. Some authors described total mastectomy as the treatment option for giant borderline and malignant phyllodes to obtain wide, clear margins. Between March 2022 and September 2023, our surgical oncology department presented and operated on three cases of giant phyllodes. They underwent a nipple-sparing mastectomy and immediate breast reconstruction using pre-pectoral silicone implants. We think that with such a procedure, we can benefit from the wide, safe margins of mastectomy that have been proven to decrease local recurrence rates while considering the aesthetic outcome.
1.Introduction
Giant phyllodes tumors constitute about one-fifth of all phyllodes tumors, which is a rare neoplasm with uncertain behavior that accounts for 0.3–1% of all breast neoplasms [1]. Phyllodes tumors are different from breast carcinomas in that they originate from the stroma, or connective tissue, of the breast [2]. Phyllodes tumors are categorized as benign (60–75%), borderline (15–20%), or malignant (10–20%) based on histology [3,4]. Tumor grade determines the local recurrence rate of these cancers; a meta-analysis found that the rates for benign, borderline, and malignant tumors were, respectively, 8%, 13%, and 18% [5].
Wide local excision with negative one-centimeter margin is the surgical treatment in most cases [6]. When wide local excision cannot achieve negative margins, or the tumor is significantly large compared to the breast size, mastectomy becomes necessary [7,8]. In such cases, breast conservation would not yield an acceptable cosmetic outcome.
In this study, we report three cases where we indicated mastectomy as a therapeutic surgery. Pre-pectoral silicone implants offered immediate reconstruction in all three cases.
2.Case presentation
2.1.Case 1
In September 2023, a 43-year-old lady, with no previous medical history presented to the oncology center with a rapidly growing right breast lump over the past four months. By inspection, the breast cup size was B, grade three ptosis., a large subcutaneous lesion was visible, palpating her right breast revealed a hard, lobulated mass that occupied most of the breast. This mass was elastic in consistency, originating from the lower quadrants, stretching the skin over it without direct affection, and distorting the breast’s normal profile (Fig. 1A). The patient never had a screening mammography before. Immediate mammography could not be done for the right side, as it could not be compressed regarding its huge size, so the patient underwent bilateral breast ultrasound that showed the whole right breast occupied by multiple similar well-circumscribed oval-shaped, hypoechoic lesions with macro lobulated and cystic changes inside with faint vascularity, the largest measuring 11.5 × 9.5 cm, with no suspicious axillary LNs. The contralateral breast was imaged and showed benign fibrocystic changes.
Fig. 1.
Preoperative and postoperative photos for Case 1: A. Preoperative photo showing right breast mass. B. Postoperative outcome after reconstruction.
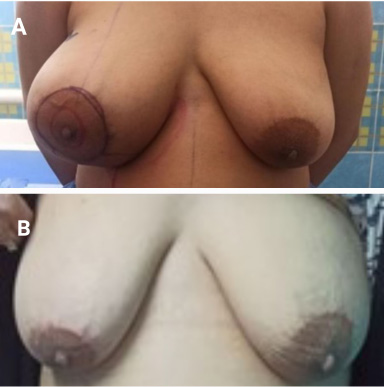
A trucut biopsy revealed low-grade spindle cell proliferation with a myxoid background. Given the huge size of the lesion, a right nipple-sparing mastectomy with reconstruction by implant was planned after the patient’s consent. A right Subcutaneous mastectomy was done through wise pattern incisions. A pre-pectoral implant (370 cc, round, smooth, moderate profile) was placed in the pocket without using a mesh or acellular dermal matrix (ADM); the skin was sutured in layers; and closure was over a suction drain. The patient was discharged after one day. The final histopathologic examination of paraffin sections revealed a borderline phyllodes tumor, with all surgical margins free from tumor tissue. She came on subsequent visits with a well-healed wound and no complications. She presented after three months of follow-up and was satisfied with the cosmetic outcome (Fig. 1B). At the last visit, we performed a right breast ultrasound, which revealed no signs of recurrence.
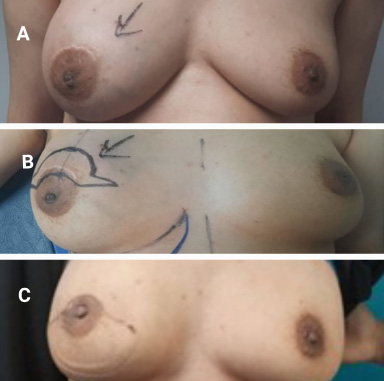
Fig. 2.
Preoperative and postoperative photos for Case 2: A. Preoperative photo showing right breast mass. B. Preoperative incision design (batwing mammoplasty). C. Postoperative outcome after reconstruction.
2.2.Case 2
A 40-year-old female patient, who does not smoke and has no prior medical history, came to our department with a recurrent large right breast lump, previously excised two years ago, and a postoperative pathology examination revealed the diagnosis of fibroadenoma. The patient had a follow-up bilateral breast ultrasound almost one year after that previous excision, which was free from local recurrence. In June 2023, a rapidly growing large mass without skin affection occupied the upper half of her right breast (Fig. 2A). Examination revealed a breast cup size of B, with a grade two ptosis; palpation revealed a lobulated, firm, and non-tender mass, without any palpable axillary LNs. Bilateral mammography reported a large retro areolar hyperdense, ill-defined lesion in the right breast, normal skin and nipple, and free axillary lymph nodes.
A trucut biopsy showed low-grade spindle cell proliferation and a focal residual fibroepithelial lesion, which makes a phyllodes tumor possible. Given the rapid recurrence of a large lesion within 2 years, the possibility of malignant phyllodes was suggested even without a proven histopathology of malignancy. The treatment decision was to perform extensive wide local excision, and since that would not lead to an accepted cosmetic outcome, a nipple-sparing mastectomy with reconstruction by implant was planned for this patient upon her consent. The batwing pattern was chosen for the skin-sparing design (Fig. 2B), with the insertion of a pre-pectoral implant (285 cm, round, smooth, moderate profile) without using a mesh or ADM. The final histopathology examination revealed a malignant phyllodes tumor with free surgical margins. Furthermore, the pathology revision of the previously excised lesion revealed malignant phyllodes, explaining the local recurrence within 2 years. The patient was referred to receive radiotherapy, she then showed up one week after the completion of the radiotherapy sessions with radiation dermatitis, and after 3 months, she was better with accepted cosmesis (Fig. 2C).
2.3.Case 3
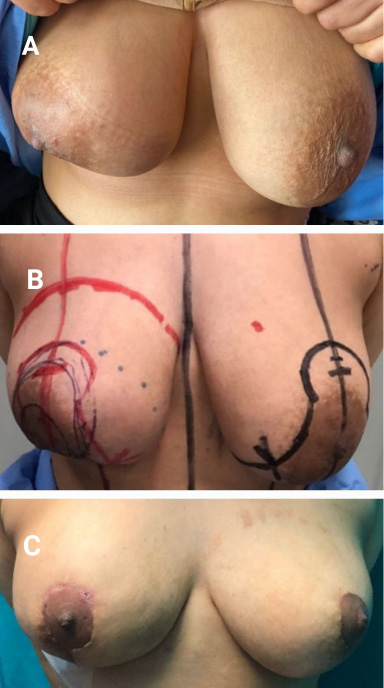
A 33-year-old patient came to our unit in March 2022, presenting with a large recurrent right breast lump that had undergone four previous excisions. The last excision was in October 2021, with the pathology revealing a benign phyllodes tumor, all with free margins. By examination, the breast cup size was B, with grade three ptosis, and the mass occupied most of the right breast (Fig. 3A). A circumareolar scar from the previous operation was detected, On palpation, the mass was firm in consistency and non-tender, and lymph nodes were impalpable. Breast mammography revealed a large lobulated hypoechoic solid mass measuring about 7 × 5 cm, visible at 3–7 o’clock in the right breast. It showed moderate to marked vascularity, with partial parenchymal infiltration visible at 6–7 o’clock, suggesting sarcomatous changes. The mass showed subcutaneous infiltration. A trucut biopsy revealed a fibroepithelial lesion consistent with benign phyllodes. Following patient counseling, we planned a right nipple-sparing skin-reducing mastectomy with contralateral symmetrization surgery (Fig. 3B). A right subcutaneous mastectomy was performed. The frozen section examination from the base of the nipple was free from tumor tissue, and a pre-pectoral implant (285 cc) (round, smooth, high profile) with ULTRAPROTM mesh was sutured around the implant. After two days, the patient was discharged. The final histopathology of the paraffin sections revealed a borderline phyllodes tumor. The physician referred the patient for radiotherapy, administering a 60 Gy/30 fraction over 1.5 months. Subsequent visits revealed a good cosmesis (Fig. 3C) for MRI follow-up, and the final imaging in July 2023 revealed a bilateral normal breast study.
Fig. 3.
Preoperative and postoperative photos for Case 3: A. Preoperative photo showing right breast mass. B. Preoperative incision design (right skin-reducing mastectomy with left reduction mammoplasty). C. Postoperative outcome after reconstruction.
3.Discussion
Phyllodes tumors are lesions derived from periductal and specialized lobular stroma [9], accounting for less than 1% of all breast neoplasms [1,4]. About one-fifth of phyllodes tumors are giant phyllodes [10,11]. They are classified as benign, borderline, and malignant [3]. As reported in our three cases of giant phyllodes tumor, two were borderline phyllodes, and one was malignant.
Depending on a number of variables, including age, tumor size, mitotic activity, stromal expansion, surgical margin, and surgical technique, phyllodes tumors can recur locally [12]. Benign, borderline, and malignant phyllodes tumors had recurrence rates of 10–15%, 14–25%, and 23–30%, respectively [5]. These recurrences usually happen within two years of the initial surgery [13]. Some recurrences may be associated with upgrading from a benign to a borderline or malignant nature [14]. That is exactly what happened with our second case which had a recurrent phyllodes tumor that upgraded from benign to borderline.
Phyllodes tumors mostly affect middle-aged women between 35 and 45 years old [10,15]. Phyllodes are most frequently found in the right breast, where they are multicentric in one-third of instances [16]. Giant phyllodes tumors present as a painless, rapidly growing mass [17] that disfigures the breast contour, stretching the skin over it up to pressure necrosis [2]. Even with the overlapping clinical features between phyllodes and fibroadenoma, the rapid growth rate and large size favor phyllodes diagnosis [10]. The typical clinical presentation of a giant phyllodes was clear in our case study.
The mammographic features of the phyllodes tumor is a smooth, multilobulated mass mimicking fibroadenoma [5,18]. The preoperative distinction between giant fibroadenoma and giant phyllodes though hard, is crucial [10], regarding their different treatment options, either surgery versus observation or even the type of surgery, as fibroadenoma is mainly for excision. In contrast, phyllodes require wide local excision with wide free margins [19] to avoid the burden of the wrong choice of surgery, as encountered in the previous excisions in our second case.
Histopathology by core tissue biopsy remains the only preoperative reliable investigation to differentiate between giant phyllodes and fibroadenoma [5]. As grossly, the two lesions are usually indistinguishable. While under a microscope, phyllodes tumors have a unique leaf-like shape with papillary projections of epithelial stroma [20]. These elements are of paramount importance to differentiate between fibroadenoma and phyllodes and distinguish benign tumors from malignant ones [4]. Yet core biopsies might not be enough to diagnose phyllodes, due to the lack of tissue in the examined specimen, therefore, adequate excision of the lesion is required to obtain a sure diagnosis [5]. None of our patients had a sure pathological diagnosis of phyllodes tumor before the time of surgery.
According to the NCCN guidelines, the management of borderline and non-metastatic malignant phyllodes tumors is surgical excision with one-centimeter clear margins [6,21], and does not require surgical axillary staging due to the low incidence of lymph node metastasis [21]. Some authors describe total mastectomy for giant borderline or malignant phyllodes to get wide clear margins [8]. Hence, it was difficult to achieve wide clear margins in our three cases of giant phyllodes. While attaining an accepted cosmetic outcome, they were offered A nipple-sparing mastectomy with reconstruction. Through such a procedure, we can achieve the desired wider margins, and we can offer a good aesthetic outcome, as most of those patients are middle-aged women.
Whether or not the patient would undergo adjuvant radiation therapy depends on the final histology. Adjuvant radiotherapy (RT) decreases the incidence of local recurrence in malignant phyllodes tumors, but it does not affect overall or disease-free survival [22]. As reviewed in our second case of malignant phyllodes, she received radiotherapy, and as for our first and third cases of borderline phyllodes, only the third case received radiotherapy given the history of multiple local recurrences compared to her young age (33 years old), while the first case was for close follow up.
The study’s limitations include the small number of included patients and the short follow-up period. Also, there is heterogeneity in mesh usage. The strengths included showcasing the successful management of a unique disease and demonstrating the feasibility of such a technique in managing large phyllodes tumors.
4.Conclusion
Though rare in the literature, nipple-sparing mastectomy with reconstruction by pre-pectoral implants should be considered a suitable surgical approach for giant phyllodes tumors, given the association between giant phyllodes and malignancy, thus the higher tendency of their local recurrence, and also considering the most affected age group, which is middle-aged women who can benefit from the possibility of achieving wide clear margins, that are proven to reduce the local recurrence without the psychological burden of mastectomy.
Acknowledgements
The authors have no acknowledgments.
Ethics approval and consent to participate
All procedures in the study involving human participants adhered to the ethical standards set by the institutional research committee, the 1964 Helsinki Declaration, its subsequent amendments, or comparable ethical standards. We can waive specific ethical approval in this case series.
Consent for publication
The patient signed a written consent for the surgical maneuvers for resection and reconstruction. There is consent for publication.
Conflict of interest
The authors declare that they have no conflict of interest.
Data and material availability
All of the clinical, radiological, and pathological data used in this manuscript are available on the Mansoura University medical system (Ibn Sina Hospital management system) https://srv137.mans.edu.eg/mus/newSystem/.
Author contributions
All authors have read and approved the manuscript. KMA, MMS, and AH are responsible for the data collection and editing, SE and KMA: writing and revision OH: preparation and revision.
References
[1] | Testori A., , Meroni S, , Errico V, , Travaglini R, , Voulaz E, , Alloisio M, Huge malignant phyllodes breast tumor: A real entity in a new era of early breast cancer, World J Surg Oncol, 13: : 81, (2015) . doi:10.1186/s12957-015-0508-7. |
[2] | Faridi SH, , Siddiqui B, , Ahmad SS, , Aslam M, Progression of fibroadenoma to malignant phyllodes tumour in a 14-year female, J Coll Physicians Surg Pak, 28: (1): 69–71, (2018) . doi:10.29271/jcpsp.2018.01.69. |
[3] | Ye JS, Statistical analysis on the behavior and recurrence of breast phyllodes tumors, J Clin Oncol, 34: (3_suppl): e294, (2016) . doi:10.1200/jco.2016.34.3_suppl.e294. |
[4] | Tan PH, The 2019 World Health Organization classification of tumours of the breast, Histopathology, 77: (2): 181–185, (2020) . doi:10.1111/his.14091. |
[5] | Lu Y, Local recurrence of benign, borderline, and malignant phyllodes tumors of the breast: A systematic review and meta-analysis, Ann Surg Oncol, 26: (5): 1263–1275, (2019) . doi:10.1245/s10434-018-07134-5. |
[6] | Lohmeyer JA, , Huster N, , Lühr C, , Lindner C, , Wittig KS, , Keck MK, [Treatment of phyllodes tumours of the breast: Evaluation of 66 cases and literature review], Handchir Mikrochir Plast Chir, 53: (2): 159–167, (2021) . doi:10.1055/a-1164-6791. |
[7] | Breastcancer.org; Cancerous Phyllodes Tumors of the Breast. Breastcancer.org, Depolo Jamie, 2023. |
[8] | Lim RS, , Cordeiro E, , Lau J, , Lim A, , Roberts A, , Seely J, Phyllodes tumors-the predictors and detection of recurrence, Can Assoc Radiol J, 72: (2): 251–257, (2021) . doi:10.1177/0846537119899553. |
[9] | Ng CCY, MED12 is frequently mutated in breast phyllodes tumours: A study of 112 cases, J Clin Pathol, 68: (9): 685–691, (2015) . doi:10.1136/jclinpath-2015-202896. |
[10] | Amir RA, , Rabah RS, , Sheikh SS, Malignant phyllodes tumor of the breast with metastasis to the pancreas: A case report and review of literature, Case Rep Oncol Med, 2018: : 6491675, (2018) . doi:10.1155/2018/6491675. |
[11] | Fernández-Ferreira R, , Arroyave-Ramírez A, , Motola-Kuba D, , Alvarado-Luna G, , Mackinney-Novelo I, , Segura-Rivera R, Giant benign mammary phyllodes tumor: Report of a case and review of the literature, Case Rep Oncol, 14: (1): 123–133, (2021) . doi:10.1159/000510741. |
[12] | Ferreira MA, , Leite M, , Ferreira S, , Midões A, , Gonçalves A, A rare case of a large breast phyllodes tumor, Int J Case Rep Imag, 9: : 100951–100956, (2018) . |
[13] | Pornchai S, Malignant transformation of phyllodes tumor: A case report and review of literature, Clin Case Rep, 6: (4): 678–685, (2018) . doi:10.1002/ccr3.1428. |
[14] | Borhani-Khomani K, , Talman M-LM, , Kroman N, , Tvedskov TF, Risk of local recurrence of benign and borderline phyllodes tumors: A Danish population-based retrospective study, Ann Surg Oncol, 23: (5): 1543–1548, (2016) . doi:10.1245/s10434-015-5041-y. |
[15] | Khanal S, , Singh YP, , Bhandari A, , Sharma R, Malignant phyllodes tumor with metastases to lung, adrenal and brain: A rare case report, Ann Med Surg (Lond), 36: : 113–117, (2018) . doi:10.1016/j.amsu.2018.10.030. |
[16] | Jing P, , Wei B, , Yang X, Phyllodes tumor of the breast with nipple discharge: A case report, Medicine, 97: (52): e13767, (2018) . doi:10.1097/MD.0000000000013767. |
[17] | Athamnah MN, , Abuelaish OM, , Rabai NA, Multifocal intra-parenchymal and sub-pectoral malignant phyllodes tumor in young female, rare and unusual presentation: A case report, Int J Surg Case Rep, 71: : 280–284, (2020) . doi:10.1016/j.ijscr.2020.05.014. |
[18] | Calhoun K, , Allison KH, , Kim JN , Phyllodes tumors, in: Harris J, Lippman ME, Morrow M et al. (eds), Diseases of the Breast. 2014 [Google Scholar]. |
[19] | Krings G, , Bean GR, , Chen Y-Y, Fibroepithelial lesions; The WHO spectrum, Semin Diagn Pathol, 34: (5): 438–452, (2017) . doi:10.1053/j.semdp.2017.05.006. |
[20] | Nguyen NT, , Maciolek LM, , Qiu S, , Sadruddin S, , Nguyen QD, Malignant phyllodes tumor of the breast in a 26-year-old woman, Cureus, 12: (1): e6590, (2020) . doi:10.7759/cureus.6590. |
[21] | NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Breast Cancer. Version 2.2024 — March 11, 2024. |
[22] | Gnerlich JL, , Williams RT, , Yao K, , Jaskowiak N, , Kulkarni SA, Utilization of radiotherapy for malignant phyllodes tumors: Analysis of the National Cancer Data Base, 1998–2009, Ann Surg Oncol, 21: (4): 1222–1230, (2014) . doi:10.1245/s10434-013-3395-6. |


