
Impact of the COVID-19 pandemic on breast cancer pathological stage at diagnosis in Tunisian patients
Abstract
BACKGROUND:
Breast cancer (BC) patients’ diagnosis and management was affected by a global reorganization after the Coronavirus disease 2019 (COVID-19). Our study aimed to assess the impact of the pandemic on the pathological stage of newly diagnosed patients with BC compared to pre-pandemic and to identify predictive factors of tumor advanced stage.
METHODS:
Pathological records of all consecutive newly operated BC patients between March 2020 and December 2021 were reviewed retrospectively. Clinical and pathological prognostic factors of BC were collected and compared between pre-pandemic and pandemic periods. Then, predictive factors of tumor advanced stage were identified.
RESULTS:
Of the 225 cases included in the analysis, 98.7% were females and 1.3% were males. The median time from first histological diagnosis to first surgical treatment was enlarged by 42 days with a significant difference between the two periods (p = 0.002). Newly diagnosed BC patients during the COVID-19 pandemic were operated at a more advanced stage (54.1% vs 36.2%, p = 0.007), had a greater lymphovascular invasion (p = 0.002), lymph node metastasis (p = 0.015) and are more commonly of IBC NST histological type (p = 0.005). Moreover, multivariate analyses showed that the pandemic period (AOR = 2.28; p = 0.016) and the lympho-vascular invasion (p < 0.001) were independently associated with advanced stage of tumors.
CONCLUSION:
Our findings proved an increase in alarming rates of advanced stage BC associated with the COVID-19 crisis. These findings support recommendations for a quick restoration of BC screening at full capacity, with adequate prioritization strategies to mitigate harm.
1.Introduction
Breast cancer (BC) is the most prevalent cancer and the first leading cause of cancer death in women in the word, with an estimated 3092 new cases and 986 deaths from cancer in 2020 [1]. The incidence of BC in Tunisia is 32.2/100000 women and the mortality is 10.3/100000 women [2]. Screening programs have significantly increased the diagnosis of BC in the early stages with an estimated prognosis improvement of 45% in western countries during the past 10–20 years [3]. Tunisia implemented a national cancer prevention screening program for BC since the early 2000 [2,4]. A study conducted in the north of Tunisia comparing clinical and pathological features of BC issued from a large scale mammography program to those diagnosed in symptomatic patients, found favorable results in terms of clinical and histological tumoral size, number of positive nodes, number of mastectomies and the survival rates [5]. Because early detection plays a crucial role in BC management and outcome, it is imperative to ensure that the screening is uninterrupted due to external factors.
In March 2020, the World Health Organization (WHO) declared the Coronavirus Disease 2019 (COVID-19) a global pandemic [6]. On March 2023, there are 687 million infections and over 6 million deaths in the word. The first case of COVID-19 infection in Tunisia was reported on the 3rd March 2020 [7]. As the number of infected patients and deaths rose, Tunisian authorities imposed a general lockdown in the late March 2020. Since then, COVID-19 infected over one million patients with almost 30 thousand deaths [8]. The pandemic has forced healthcare professionals to tailor their recommendations for treatment and management to ensure that patients can be safely treated without also risking infection [9]. Thus, many national and international associations, cancer centers and research groups published their recommendations, by reorganizing BC management strategies. The majority of these guidelines agreed that population mammographic screening and screening of mutation carriers should be suspended until the pandemic subsides [10].
Unfortunately, measures that aim to control the COVID-19 pandemic do not stop cancer progression and could lead to diagnosis at more advanced stages and thus poor clinical outcomes. Recent studies suggest that pausing BC screening programs during lockdown produced delayed cancer diagnoses associated with significant repercussions on cancer mortality and health economic losses [11,12].
This study aimed to evaluate whether the COVID-19 pandemic was associated with more advanced pathological stage and changes in clinical presentation for patients with BC compared to the pre-pandemic period in Tunisia. We also aimed to identify predictive factors of tumor advanced stage.
2.Materials and methods
2.1.Study design and population
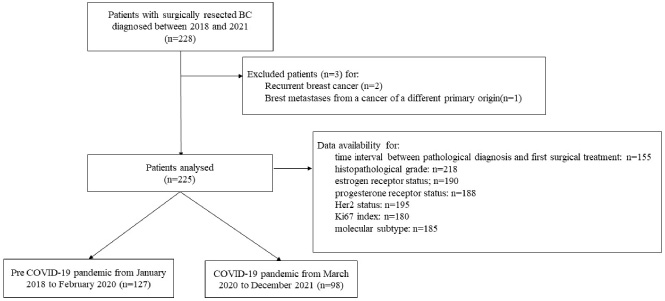
This was a single-center retrospective study that included all consecutive patients undergoing BC surgery and diagnosed in the department of pathology at Habib Bourguiba University Hospital in Sfax, Tunisia between January 2018 and December 2021.
Patients with relapsed BC or with breast metastases from cancer of a different organ were excluded.
This report follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and the national research committee of Habib Bourguiba and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
2.2.Dataset details
Patient’s clinical and pathological data at the time of diagnoses were collected from their pathological records. Clinical data concerned, age at diagnosis, gender, as well as time interval between the first histological diagnosis and the first surgical treatment.
Pathological data concerned, bilateral tumors, histological subtype, lympho-vascular invasion, pathological stage (pT), lymph node involvement (pN), pathological stage group, histopathological grade, molecular subtype, estrogen receptor (ER) status, progesterone receptor (PR) status, human epidermal growth factor receptor 2 (Her2) status and Ki67 index.
The histological type was determined according to the fifth edition of the WHO classification of breast tumors [13].
The pathological classification (pT, pN, Pathological stage group) was determined according to the eighth edition of the Tumor-Node-Metastasis (TNM) staging system adopted by the American Joint Committee on Cancer (AJCC) [14]. The histopathological grade was assessed according to the Nottingham combined histologic grade (Elston-Ellis modification of the Scarff-Bloom-Richardson grading system) [15].
ER, PR and Her2 status were determined by immunohistochemistry either on the biopsy specimen or on the corresponding surgical resection, according to the American Society of Clinical Oncology/College of American Pathologists ASCO/CAP Guideline [16].
Fig. 1.
Selection criteria of study population.
2.3.Outcomes
Patients were divided into two groups according to the surgery date. The COVID-19 pandemic period was defined from March 2020 to December 2021 and the pre COVID-19 pandemic period was defined from January 2018 to February 2020.
The primary outcome was an advanced pathological stage group at diagnosis defined by the stage III. As secondary outcomes, we assessed whether the COVID-19 pandemic impacted on the time interval between histological diagnosis and primary surgical treatment of BC, clinical and pathological prognostic factors.
2.4.Statistical analysis
All statistical analyses were performed using the software package SSPS 20.0. Clinical and pathological characteristics were presented using count and percentage for categorical variables, median, and interquartile range for continuous variables when they are non-normally distributed. To compare BC characteristics between pandemic and pre-pandemic periods, Pearson chi-square or Fisher’s exact tests were used to compare categorical variables. As for continuous variables, Student t-test, or the Mann-Whitney U-test to compare two mean values. To identify factors associated with advanced pathological stage, univariate logistic regression was performed, and crude odds ratio (COR) was calculated accompanied by their 95% confidence interval (95% CI; p). Then, variables with p-value less than 0.05 in the univariate analysis were fitted into a multivariate binary logistic regression model in order to identify independent factors of advanced pathological stage, Adjusted Odds Ratio (AOR) (95% CI; p). Potential risk factors reported in the literature and confounding variables were also systematically put into the final model. To evaluate the validity of the model, calibration was assessed using the Hosmer-Lemeshow test for goodness of fit, which evaluated expected and observed probabilities in population deciles. This test allows to evaluate the difference between values predicted by the model and the observed values. According to the results of this test, we have chosen the model with the best fit and the highest level of significance. Then, the discriminatory power of the prediction model was expressed as the area under the receiver operating characteristic curve (AUROC). The sensitivity and the specificity of the prediction model were calculated. The results were considered statistically significant at p < 0.05.
3.Results
3.1.Patients’ and tumor characteristics
A total of 225 patients was included in the study (Fig. 1). The overall median age at diagnosis was 53 years (IQR = [46, 61]). Male patients accounted for 1.3% of the total included patients. The tumor was bilateral in nine cases (4%). The overall median time interval between the first histological diagnosis and the first surgical treatment was 90.5 days (IQR = [53,192]). Invasive breast carcinoma of no special type (IBC-NST) was the most common histological type (N = 177; 78.7%). The tumor had mainly a histopathological grade 2 (G2) (N = 116; 53.2%). The pathological stage (pT) was high (pT3/pT4) in 50 cases (22.2%). One hundred forty-three cases were associated with nodal metastases (pN+) (63.6%). The main tumor pathological stage group was III (N = 100; 44.4%). The positive rates for ER, PR and Her2 were 76.3% (145 cases), 70.2% (132 cases) and 30.8% (60 cases), respectively. Ki67 index was high (≥14%) in 58.3% of cases (Table 1). The most common molecular subtype was luminal A in 92 cases (49.7%) (Table 1).
Table 1
Comparison of the sample characteristics between pre-pandemic and pandemic periods
| Variables | Overall sample | Prepandemic period | Pandemic period | p value |
| Overall | N = 225 | N = 127 | N = 98 | |
| Median age (years (IQR)) | 53 [46-61] | 53 [46-62] | 53.5 [46-62] | 0.65 |
| Gender N (%) | ||||
| Males N (%) | 3 (1.3) | 0 (0) | 3 (3.1) | 0.08 |
| Females N (%) | 222 (98.7) | 127 (100) | 95 (96.9) | |
| Median time interval between the first histological diagnosis and the first surgical treatment (days (IQR)) | 90.5 [53-192] | 76 [48-120] | 118 [61.5-234] | 0.002 |
| Bilateral tumor, N (%) | 9 (4) | 5 (3.9%) | 4 (4.1) | 0.9 |
| Histological subtype N (%) | ||||
| IBC-NST | 177 (78.7) | 90 (70.9) | 87 (88.8) | 0.005* |
| Invasive lobular carcinoma | 17 (7.6) | 13 (10.2) | 4 (4.1) | |
| Other | 31 (13.8) | 24 (18.9) | 7 (7.1) | |
| Lympho-vascular invasion N (%) | ||||
| Present | 102 (45.3) | 46 (36.2) | 56 (57.1) | 0.002 |
| Absent | 123 (55.7) | 81 (63.8) | 42 (42.9) | |
| Pathological T(pT) N (%) | ||||
| pT1/pT2 | 175 (77.8) | 107 (84.3) | 68 (69.4) | 0.008 |
| pT3/pT4 | 50 (22.2) | 20 (15.7) | 30 (30.6) | |
| Nodal involvement (pN) N (%) | ||||
| pN0 | 82 (36.4) | 55 (43.3) | 27 (27.6) | 0.015 |
| pN+ | 143 (63.6) | 72 (56.7) | 71 (72.4) | |
| Pathological stage group N (%) | ||||
| I | 29 (12.9) | 17 (13.3) | 12 (12.2) | 0.031 |
| II | 96 (42.7) | 63 (49.6) | 33 (33.7) | |
| III | 100 (44.4) | 47 (37) | 53 (54.1) | |
| Pathological Stage class N (%) | ||||
| Early stage (I/II) | 126 (56) | 81 (63.8) | 45 (45.9) | 0.007 |
| Advanced stage (III) | 99 (44) | 46 (36.2) | 53 (54.1) | |
| Histopathological Grade N (%) | ||||
| G1/G2 | 123 (56.4) | 71 (59.2) | 52 (53.1) | 0.36 |
| G3 | 95 (43.6) | 49 (40.8) | 46 (46.9) | |
| Estrogen receptor N (%) | ||||
| Positive | 145 (76.3) | 83 (78.3) | 62 (73.8) | 0.46 |
| Negative | 45 (23.7) | 23 (21.7) | 22 (26.2) | |
| Progesterone receptor N (%) | ||||
| Positive | 132 (70.2) | 77 (72.6) | 55 (67.1) | 0.4 |
| Negative | 56 (29.8) | 29 (27.4) | 27 (32.9) | |
| Her2 N (%) | ||||
| Positive (score 3+) | 60 (30.8) | 32 (29.6) | 28 (38.2) | 0.7 |
| Negative (score 0,1,2) | 135 (69.2) | 76 (70.4) | 59 (67.8) | |
| Ki67 N (%) | ||||
| <14% | 75 (41.7) | 46 (46) | 29 (36.3) | 0.18 |
| ≥14% | 105 (58.3) | 54 (54) | 51 (63.7) | |
| Molecular subtype N (%) | ||||
| Luminal (A/B) | 140 (75.7) | 82 (78.1) | 58 (72.5) | 0.48 |
| Her2+ | 17 (9.2) | 10 (9.5) | 7 (8.8) | |
| TN | 28 (15.1) | 13 (12.4) | 15 (18.8) |
[i] Abbreviations: IBC NST: Invasive breast cancer of no special type, Her2: human epidermal growth factor receptor 2, TN: triple negative. *Statistically significant difference between precovid and covid period for IBC NST subtype.
3.2.Comparison of tumor characteristics and timing between pathological diagnosis and surgical treatment between pre-pandemic and pandemic periods
The histological subtype was significantly more frequent between the two periods for the IBC NST type (p = 0.005). A statistically higher frequency was also noted during the pandemic period for the lympho-vascular invasion (57.1% vs 36.2%; p = 0.002), the high pathological stage (pT) (30.6% vs 15.2%, p = 0.008), the lymph node involvement (pN+) (72.4% vs 56.7%, p = 0.015), and pathological stage group (p = 0.031). Specifically, in pandemic period, BC patients were less likely to be diagnosed with early-stage disease (stage I–II) compared to the pre-pandemic period (45.9% vs 63.8%, p = 0.007). On the other hand, no statistical significance between the periods was observed regarding the tumor bilaterality, histopathological grade, ER status, PR status, Her2 status, Ki67 index, and molecular subtype (Table 1).
Looking at BC patients’ management, time interval between the first histological diagnosis and the first surgical treatment was significantly enlarged in the pandemic period (median 118 vs 76 days, p = 0.002) (Table 1).
3.3.Comparison of patient and tumor characteristics according to advanced stage
Univariate analysis showed that tumors at an advanced stage were significantly associated with patients operated during the pandemic period (COR = 2; p = 0.008), positive lympho-vascular invasion (COR = 6.48; p < 0.001), and high histopathological grade (G3) (COR = 1.99; p = 0.013) (Table 2).
Table 2
Comparison of the clinical and the pathological characteristics according to the primary outcome of advanced stage
| Variables | COR (95% CI) | p value | AOR (95% CI) | p value |
| Period | ||||
| Prepandemic | 1 | 0.008 | 1 | 0.016 |
| Pandemic | 2 [1.2-3.5] | 2.28 [1.16-4.59] | ||
| Age class | ||||
| ≤45y | 1 | 0.28 | - | - |
| >45y | 0.71 [0.38-1.32] | |||
| Gender | ||||
| Females | 1 | 0.44 | - | - |
| Males | 2.55 [0.23-28.84] | |||
| Tumors location | ||||
| Unilateral | 1 | 0.97 | - | - |
| Bilateral | 1.01 [0.26-3.89] | |||
| Histological subtype | ||||
| IBC-NST | 1 | 0.23 | - | - |
| Invasive lobular carcinoma | 0.47 [0.16-1.49] | 0.17 | ||
| Other | 0.62 [0.28-1.37] | 0.24 | ||
| Lymphovascular invasion | ||||
| Absent | 1 | <0.001 | 1 | <0.001 |
| Present | 6.48 [3.61-1.62] | 5.85 [2.97-11.50] | ||
| Histopathological grade | ||||
| G1/G2 | 1 | 0.013 | - | - |
| G3 | 1.99 [1.15-3.44] | |||
| Molecular subtype | ||||
| Luminal (A/B) | 1 | 0.46 | 1 | 0.94 |
| Her2+ | 1.84 [0.67-5.08] | 0.23 | 1.13 [0.36-3.57] | 0.82 |
| TN | 1.23 [0.54-2.80] | 0.62 | 1.14 [0.45-2.92] | 0.77 |
[i] Abbreviations: IBC NST: Invasive breast cancer of no special type, Her2: human epidermal growth factor receptor 2, TN: triple negative; COR: Crude Odds Ratio; AOR: Adjusted odds ratio; CI: Confidence interval.
At multivariate analysis, the pandemic period (AOR = 2.28; p = 0.016) and the lympho-vascular invasion (AOR = 5.85; p < 0.001) were independently associated with advanced stage of tumors (Table 2).
3.4.Validity of the model
A good calibration of the depressive symptom model (Hosmer-Lemeshow test p = 0.06) was noted. The AUROC of the predictive logistic regression model was 0.75 (95%CI = [0.68-0.83]; p < 0.001), indicating a good predictive power in discriminating depressive symptoms, with a sensitivity of 73% and a specificity of 75%.
4.Discussion
To the best of our knowledge, this is the first study to evaluate whether the COVID-19 pandemic has affected the stage of BC in Tunisia.
The dreadful consequences of COVID-19 put an unprecedented pressure on health-care services across the globe. Consequently, there was a complete reorganization of the National Health System, including reallocation of crucial human and economic health resources. This inevitably impacted on hospital admissions for non-communicable diseases hampering both inpatients and outpatients care. In particular, all elective activities were paused or postponed in order to preserve the health care system capacity for COVID-19 patients [17].
Diagnostic procedures and screening programs were deprioritized, routine clinical practices (such as follow up visits and multidisciplinary tumor meetings) reoriented to virtual care, to reduce risk exposure and ease the pressure on hospital facilities [18]. Cancer patients, as a highly vulnerable population to better manage at a safe distance [19]. Telehealth visits were encouraged for non-emergent cases and follow-up appointments [20]. On these grounds, the American Society of Breast Surgeons, the National Accreditation Program for Breast Centers, the National Comprehensive Cancer Network, the Commission on Cancer, the American College of Radiology as well as the Italian Association of Medical Oncology provided preliminary guidance on the prioritization and treatment of BC during this particular period [10,21].
BC screening in the asymptomatic population leads to early diagnosis and treatment. This prospect results in improved survival and may avert BC deaths [22]. It is noteworthy that screen-detected BC shows some peculiarities. In particular, women diagnosed through the mammographic screening programs usually present with tumors with luminal-like subtype, more frequently of low grade, small size and node-negative [23].
As the most common diagnosed tumor globally, mainly benefitting in the early stage disease from screening detection, it is of utmost importance to consider the potential effect of BC delayed diagnoses on patients’ outcome, ultimately resulting in divergent therapeutic intents (curative vs palliative) [24]. Numerous associations have issued serious warnings about the disastrous impact of reducing cancer screening programs [25].
The real impact of temporary mammographic screening suspension on BC outcomes remains uncertain. Yong et al. [26] have recently estimated the long-term clinical impact of BC screening interruptions in Canada using a validated mathematical model. The authors found that a 3-month interruption in BC screening could increase cases diagnosed at advanced stages and cancer deaths in 2020–2029. Moreover, longer interruptions and reduced volumes when screening resumes would further increase excess cancer deaths. Similarly, Sharpless [27] reported the results of a comparable analysis in the USA, using the CISNET cancer simulation model. This analysis predicted approximately 5300 additional BC deaths in the USA over the next decade.
In this regard, our study has proved that new diagnosed BC during COVID-19 pandemic were operated at a more advanced stage (54.1% vs 36.2%, p = 0.007). Our univariate and multivariate analyses showed also, that the advanced stage of BC was significantly associated with the pandemic period as an independent factor.
These results confirm the estimates obtained through the mathematical models of Yong et al. [26] and Harpless [27], Toss et al. [28] and Mentrasti et al. [17] in terms of increased advanced stages at diagnosis. These results can be explained by the chronic stress due to COVID-19 which caused delayed referring and health resources reallocation.
In particular, analysis of the secondary outcomes showed that patients who underwent surgery during the COVID-19 pandemic period had a greater lymphovascular invasion (p = 0.002), lymph node metastasis (p = 0.015) and are more commonly of IBC NST histological type (p = 0.005). These are worrisome finding, because they are related with a poor prognosis and a poor overall survival in patients with BC [13,29,30].
Additionally, since treatment of more advanced cancers generally involves more widespread use of systemic therapy and invasive surgery, we may also conclude that these delays in cancer diagnosis could be associated with increased morbidity and higher costs for our national health system.
Our study failed to find any significant difference between the two periods in ER, PR, Her2 status, Ki67 index and molecular subtype. There was also no difference in the median age, the sex, although males were seen only in the pandemic period, bilateral tumors, and histopathological grade. These findings were consistent with the studies of Toss et al. [28] and Mentratsi et al. [17].
Previous concerning findings worldwide demonstrated the greater diagnostic backlog after the shutdown of screening programs and also patient reluctance to visit hospital outpatient clinics amid concerns regarding the transmission of COVID-19 [31,32].
Our analysis showed that the procedures to obtain a definitive diagnosis and start surgical treatment were subsequently carried out with a longer delay in the pandemic period. The median time from first histological diagnosis to first surgical treatment was enlarged by 42 days with a significant difference between the two periods (p = 0.002). This is essentially due to the absence of a dedicated COVID-free hospital and the reorganization of all national resources to COVID-19 patients. Giuliani et al. [33] evaluated the effect of COVID-19 crisis in cancer diagnosis and showed a drop of 15.4% of the newly diagnosed solid tumors, including BC. Despite this, the diagnosis care was not affected during COVID-19 lockdown and the median time of pathological diagnosis has no statistically significant differences between pre-lockdown and after lockdown period.
Our work has potential limitations. The present study is limited by the single-center retrospective design relying on pathological reports. Although very important in establishing the pathological stage group especially the stage IV, metastatic status of patients was unavailable in the pathological reports. Moreover, patients with recurrent disease were excluded in order to analyze a homogeneous sample of new BC diagnoses and to avoid potential biases related to the oncological management during the follow up period for patients with previous BC. This decision could be considered a potential limitation of the work, taken into account that COVID-19 might have also and equally impacted on diagnosis and treatment of BC relapses. Since the COVID-19 vaccination campaign started in April 2021 in Tunisia, this prevention plan could have a potential effect on cancer care in the study period [34]. Finally, the sample size of 225 patients may not have enough power for all types of statistical analyses.
5.Conclusion
Ultimately, from our analysis we can conclude that, while COVID-19 has left its trail on cancer care, the impact of the advanced stage BC diagnoses might clearly unfold in the years to come. Pandemic’s challenges considered, our study offers a valuable picture of the Tunisian oncology and pathology departments’ performances to ensure diagnosis, and staging for BC patients during the first pandemic year. In this setting, the quick restoration of BC screening at its full capacity and adequate prioritization strategies to mitigate harm and comply with infection prevention are required. Further multicentric and larger prospective studies with longer follow-up are needed to evaluate the outcomes of these patients (mostly disease-free survival and overall survival).
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and the national research committee of Habib Bourguiba and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
General consent was obtained from all individual participants included in the study, upon admission to the hospital.
Conflict of interest
The authors have no conflicts of interest to disclose.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding declaration
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Credit authorship contribution statement
Meriam Triki: Conceptualization, Methodology, Writing – original draft. Mouna Zghal: Writing Resources. Houda Ben Ayed: statistical analysis. Saadia Makni: Validation. Marouwa Bouhamed: validation, Slim Charfi: Visualization and Conceptualization, Tahya Boudawara: Supervision, Manel Mellouli: Supervision and validation.
References
[1] | Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries, CA Cancer J Clin, 71: (3): 209–249, (2021) . |
[2] | INEAS [Internet]. [cited 2023 Apr 30]. Available from: https://www.ineas.tn/. |
[3] | Berry DA, , Cronin KA, , Plevritis SK, , Fryback DG, , Clarke L, , Zelen M , Effect of screening and adjuvant therapy on mortality from breast cancer, N Engl J Med, 353: (17): 1784–1792, (2005) . |
[4] | Khrouf S, , Letaief Ksontini F, , Ayadi M, , Belhaj Ali Rais H, , Mezlini A, Breast cancer screening: a dividing controversy, Tunis Med, 98: (1): 22–34, (2020) . |
[5] | Zeghal D, , Mahjoub S, , Zakraoui MA, , Zouari F, Comparison of breast cancers diagnosed in and outside of the large scale mammography program of the Ariana area of Tunisia, Tunis Med, 87: (7): 450–453, (2009) . |
[6] | WHO Director-General’s opening remarks at the media briefing on COVID-19 - 11 March 2020 [Internet]. [cited 2023 Apr 30]. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020. |
[7] | Chakroun H, , Ben Lasfar N, , Fall S, , Maha A, , El Moussi A, , Abid S , First case of imported and confirmed COVID-19 in Tunisia, Tunis Med, 98: (4): 258–260, (2020) . |
[8] | COVID - Coronavirus Statistics - Worldometer [Internet]. [cited 2023 Apr 30]. Available from: https://www.worldometers.info/coronavirus/. |
[9] | Oncology TL. COVID-19: Global consequences for oncology, Lancet Oncol, 21: (4): 467, (2020) . |
[10] | Toss A, , Isca C, , Venturelli M, , Nasso C, , Ficarra G, , Bellelli V , Two-month stop in mammographic screening significantly impacts on breast cancer stage at diagnosis and upfront treatment in the COVID era, ESMO Open, 6: (2): 100055, (2021) . |
[11] | Gheorghe A, , Maringe C, , Spice J, , Purushotham A, , Chalkidou K, , Rachet B , Economic impact of avoidable cancer deaths caused by diagnostic delay during the COVID-19 pandemic: A national population-based modelling study in England, UK, Eur J Cancer, 152: : 233–242, (2021) . |
[12] | Oldani C, , Vanni G, , Buonomo OC, COVID-19 unintended effects on breast cancer in Italy after the great lockdown, Front Public Health, 8: : 601748, (2020) . |
[13] | Cserni G, Histological type and typing of breast carcinomas and the WHO classification changes over time, Pathol - J Ital Soc Anat Pathol Diagn Cytopathol, 112: (1): 25–41, (2020) . |
[14] | Kim JY, , Lim JE, , Jung HH, , Cho SY, , Cho EY, , Lee SK , Validation of the new AJCC eighth edition of the TNM classification for breast cancer with a single-center breast cancer cohort, Breast Cancer Res Treat, 171: (3): 737–745, (2018) . |
[15] | Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long term follow up, Histopathology, 19: (5): 403–410, (1991) . |
[16] | Allison KH, , Hammond MEH, , Dowsett M, , McKernin SE, , Carey LA, , Fitzgibbons PL , Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP Guideline update, J Clin Oncol, 38: (12): 1346–1366, (2020) . |
[17] | Mentrasti G, , Cantini L, , Vici P, , D’Ostilio N, , La Verde N, , Chiari R , Rising incidence of late stage breast cancer after COVID-19 outbreak. Real-world data from the Italian COVID-DELAY study, Breast Off J Eur Soc Mastology, 65: : 164–171, (2022) . |
[18] | Riera R, , Bagattini ÂM, , Pacheco RL, , Pachito DV, , Roitberg F, , Ilbawi A, Delays and disruptions in cancer health care due to COVID-19 pandemic: Systematic review, JCO Glob Oncol, 7: : 311–323, (2021) . |
[19] | Liang W, , Guan W, , Chen R, , Wang W, , Li J, , Xu K , Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China, Lancet Oncol, 21: (3): 335–337, (2020) . |
[20] | Kripalani S, , Kulshreshta S, , Saracco B, , Meterissian S, The effect of COVID-19 on breast cancer care and treatment in North America: A scoping review, Am J Surg, 224: (5): 1222–1228, (2022) . |
[21] | Dietz JR, , Moran MS, , Isakoff SJ , Recommendations for prioritization, treatment, and triage of breast cancer patients during the COVID-19 pandemic. The COVID-19 pandemic breast cancer consortium, Breast Cancer Res Treat, 181: (3): 487–497, (2020) . |
[22] | Breast-cancer screening — Viewpoint of the IARC Working Group, N Engl J Med, 372: : 2353–2358, (2015) . |
[23] | Kobayashi N, , Hikichi M, , Ushimado K, , Sugioka A, , Kiriyama Y, , Kuroda M , Differences in subtype distribution between screen-detected and symptomatic invasive breast cancer and their impact on survival, Clin Transl Oncol, 19: (10): 1232–1240, (2017) . |
[24] | Vanni G, , Pellicciaro M, , Materazzo M, , Palombi L, , Buonomo OC, Breast cancer diagnosis in coronavirus-era: Alert from Italy, Front Oncol, 10: : 938, (2020) . |
[25] | Codacci-Pisanelli G, , Giuliani J, , Bonetti A, The effect of COVID-19 pandemic on daily oncology clinical practice, Crit Rev Oncol Hematol, 167: : 103272, (2021) . |
[26] | Yong JH, , Mainprize JG, , Yaffe MJ, , Ruan Y, , Poirier AE, , Coldman A , The impact of episodic screening interruption: COVID-19 and population-based cancer screening in Canada, J Med Screen, 0: (0): 1–8, (2020) . |
[27] | Sharpless NE, COVID-19 and cancer, Science, 368: (6497): 1290–1290, (2020) . |
[28] | Toss A, , Isca C, , Venturelli M, , Nasso C, , Ficarra G, , Bellelli V , Two-month stop in mammographic screening significantly impacts on breast cancer stage at diagnosis and upfront treatment in the COVID era, ESMO Open, 6: (2): 100055, (2021) . |
[29] | Wang G, , Zhang S, , Wang M, , Liu L, , Liu Y, , Tang L , Prognostic significance of occult lymph node metastases in breast cancer: A meta-analysis, BMC Cancer, 21: (1): 875, (2021) . |
[30] | Zhang S, , Zhang D, , Gong M, , Wen L, , Liao C, , Zou L, High lymphatic vessel density and presence of lymphovascular invasion both predict poor prognosis in breast cancer, BMC Cancer, 17: (1): 335, (2017) . |
[31] | Patt D, , Gordan L, , Diaz M, , Okon T, , Grady L, , Harmison M , Impact of COVID-19 on cancer care: How the pandemic is delaying cancer diagnosis and treatment for American seniors, JCO Clin Cancer Inform 1059–1071, (2020) .. |
[32] | Dinmohamed AG, , Visser O, , Verhoeven RHA, , Louwman MWJ, , van Nederveen FH, , Willems SM , Fewer cancer diagnoses during the COVID-19 epidemic in the Netherlands, Lancet Oncol, 21: (6): 750–751, (2020) . |
[33] | Giuliani J, , Bonetti A, Cancer prevales on COVID-19: To maintain high quality standard concerning diagnosis and oncological care even during a pandemic, J Med Virol, 93: (1): 118, (2021) . |
[34] | Chtiba N, , Cherif D, , Mersni I, , Kadri M, , Jemei A, , Lassoued I , COVID-19 vaccines and roles of the health regulatory authority in Tunisia, Disaster Med Public Health Prep 1–3. |


