
Use of axillary ultrasound to guide breast cancer management in the genomic assay era
Abstract
INTRODUCTION:
Chemotherapy is conventionally offered to non-stage IV breast cancer patients with metastatic nodes. However, the RxPONDER trial showed that chemotherapy can be omitted in selected patients with 1–3 metastatic nodes if the 21-gene assay recurrence score is ≤25. We aimed to investigate if axillary ultrasound can identify this group of patients with limited nodal burden so that they can undergo upfront surgery followed by gene assay testing, to potentially avoid chemotherapy.
METHODS:
T1-3, node positive, hormone receptor-positive and HER2-negative breast cancer patients ≥50 years old with axillary lymph node dissection (ALND) were reviewed from 2 centres. Patients with neoadjuvant chemotherapy and bilateral cancers were excluded. Number of ultrasound-detected abnormal axillary nodes, demographic and histological parameters were correlated with the number of metastatic nodes found on ALND.
RESULTS:
138 patients were included, 59 (42.8%) and 79 (57.2%) patients had 1–3 and >3 metastatic nodes on ALND respectively. On logistic regression and ROC analysis, the number of ultrasound-detected abnormal nodes was significant (p < 0.001) for predicting limited nodal burden (ROC AUC = 0.7135). Probabilities of <4 metastatic nodes with ultrasound cut-offs of 5, 6 and 8 abnormal nodes were 0.057, 0.026 and 0.005 respectively, with 100% specificity.
CONCLUSION:
A cut-off of ≤5 ultrasound-detected abnormal nodes can distinguish between patients with limited versus high nodal burden, with high specificity. Hence, incorporating the number of abnormal ultrasound-detected nodes into clinical practice may prove useful in guiding between upfront surgery and gene assay testing or neoadjuvant chemotherapy in this group of patients.
1.Introduction
In non-stage IV breast cancer patients with metastatic axillary nodes, chemotherapy is conventionally offered. However, the recent RxPONDER (A Clinical Trial RX for Positive Node, Endocrine Responsive Breast Cancer) trial [1] showed that chemotherapy can be omitted in selected patients with limited nodal burden of 1–3 metastatic nodes if the 21-gene assay recurrence score is ≤ 25. These patients also had invasive non-inflammatory breast cancer of hormone-receptor (HR) positivity, human epidermal growth factor receptor 2 (HER2) negativity and were postmenopausal. Omission of chemotherapy, in this group of patients, did not statistically affect the invasive disease–free survival, at a median follow-up of 5.3 years, when compared to patients who received endocrine-only therapy.
With this recent finding, it is crucial that clinicians can identify upfront those patients likely to have limited nodal burden, to allow them to benefit from 21 gene assay recurrence score testing. For those with high nodal burden of >3 metastatic lymph nodes, chemotherapy would still be needed, and in such cases, it would be beneficial to give chemotherapy in the neoadjuvant setting, since this has certain advantages such as shrinkage of the tumour to allow breast conservation, etc.
We aimed to investigate if axillary ultrasound can reliably distinguish between patients with limited or high nodal burden, so that the patients with limited nodal burden can potentially avoid chemotherapy and instead receive upfront surgery followed by gene assay testing.
2.Methods
Patients treated at KK Women’s and Children’s Hospital (KKH) and Singapore General Hospital (SGH), Republic of Singapore, from January 2007–December 2016 were retrospectively reviewed. We included breast cancer patients with T1-3, HR-positive and HER2-negative disease. All patients had an axilla ultrasound, biopsy proven metastatic lymph node and axillary lymph node dissection (ALND). All patients did not have palpable axillary lymph nodes. As the menopausal status was not recorded in all cases, we used a cut-off age of ≥50 years old to define patients who were postmenopausal in this study. This same age cut-off was also used in the RxPONDER trial to define patients who were postmenopausal if the definition of postmenopausal status did not apply. In the RxPONDER trial, postmenopausal status was defined as having bilateral oophorectomy or >12 months since the last menstrual period and no previous hysterectomy.
Patients with neoadjuvant chemotherapy and bilateral cancers were excluded. Generally, in our practice during the specified time period of this study, neoadjuvant chemotherapy was reserved for patients with locally advanced cancer which was inoperable.
In this study, breast cancer patients received mammogram and ultrasound of the breast and ipsilateral axilla as routine work-up. The axillary nodes were defined as abnormal sonographically if they showed any of the following characteristics: (1) cortical thickness more than 3 mm (2) eccentric cortical thickening of more than 2 mm, and (3) marked fatty hilar effacement. Only the most suspicious looking node was needle biopsied to confirm nodal metastatic status, while the remaining nodes were assessed using ultrasound criteria. The radiological data were retrieved from the radiological reports. Patients with no data on the number of abnormal axillary nodes on ultrasound were excluded.
The number of ultrasound-detected abnormal axillary nodes, demographic and histological parameters were then correlated with the number of metastatic nodes found on surgical histology.
2.1.Statistical analysis
Fisher’s exact test was used to compare proportions between the high (>3 metastatic nodes) and limited axillary nodal burden (1–3 metastatic nodes) groups in patients’ demographical, radiological and histological features. From a set of specified candidates, stepwise multiple logistic regression (SLE = 0.20, SLS = 0.25) was used to select variables and develop a model predictive of observed tumor burden, defined as the number of metastatic lymph nodes per surgical histology. Candidate variables investigated were the following: number of ultrasound abnormal lymph nodes, patient age, size of cancer (mm), tumor grade, and histology type. ROC analysis was used to obtain area under the receiver operating characteristic curve (ROC AUC) associated with the fitted model, calculated as an overall measure of predictive capability.
This study obtained exemption from SingHealth Centralised Institutional Review Board (CIRB Ref: 2022/2514) as this study used de-identified data which was collected from previous study (CIRB Ref: 2017/2077). There was waiver of patients’ consent.
3.Results
138 patients were included in this multicentre study. 108 and 30 patients were from KK Women’s and Children’s Hospital and Singapore General Hospital respectively. The mean age of the cohort was 62.5 years (range: 50–85). The average tumour size was 34.5 mm (6–130 mm) (Table 1). 59 (42.8%) and 79 (57.2%) patients had ≤3 and >3 pathologically metastatic nodes on ALND respectively.
Table 1
Characteristics of patients ≥50 years old with estrogen receptor positive, HER2 negative breast cancer
| Patients with 1–3 metastatic nodesN = 59∕% | Patients with >3 metastatic nodesN = 79∕% | P value∗ | |
| Age | 0.7770 | ||
| 50–59 | 28 (47.5) | 33 (41.7) | |
| 60–69 | 17 (28.8) | 27 (34.2) | |
| ≥70 | 14 (23.7) | 19 (24.1) | |
| Number of US abnormal lymph nodes | 0.0004 | ||
| 1 | 38 (64.4) | 23 (29.1) | |
| 2 | 13 (22.0) | 21 (26.6) | |
| 3 | 6 (10.2) | 21 (26.6) | |
| 4 | 2 (3.4) | 6 (7.6) | |
| 5 | 0 (0) | 4 (5.1) | |
| >5 | 0 (0) | 4 (5.1) | |
| Surgical histology | 0.1627 | ||
| Invasive ductal carcinoma | 54 (91.5) | 65 (82.3) | |
| Invasive lobular carcinoma | 2 (3.4) | 10 (12.7) | |
| Others | 3 (5.1) | 4 (5.1) | |
| Grade | 0.8792 | ||
| I | 3 (5.1) | 4 (5.1) | |
| II | 29 (49.2) | 35 (44.3) | |
| III | 27 (45.8) | 40 (50.6) | |
| Progesterone receptor | 0.1695 | ||
| Positive | 46 (78.0) | 69 (87.3) | |
| Negative | 13 (22.0) | 10 (12.7) | |
| Tumour size/mm | 0.3709 | ||
| < ∕ =20 | 13 (22.0) | 13 (16.5) | |
| >20–50 | 40 (67.8) | 52 (65.8) | |
| >50 | 6 (10.2) | 14 (17.7) | |
| Number of metastatic nodes on axillary clearance | NA | ||
| 1–3 | 59 (100) | 0 (0) | |
| 4–9 | 0 (0) | 52 (65.8) | |
| >9 | 0 (0) | 27 (34.2) |
[i] ∗P value using Fisher’s exact test.
86.2% had invasive ductal carcinoma. 7 (5.1%), 64 (46.4%) and 67 (48.5%) patients had grade I, II and III disease respectively. 83.3% had progesterone receptor (PR) positivity.
On Fisher’s exact test, only the number of abnormal lymph nodes seen on ultrasound was statistically significant (p = 0.0004) in distinguishing between patients with limited nodal burden of ≤3 versus high nodal burden of >3 metastatic nodes.
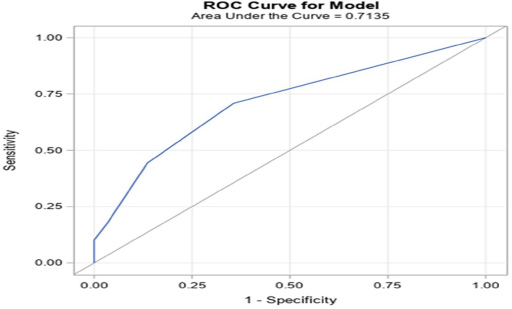
On stepwise logistic regression analysis, the only variable found to be statistically significant (p< 0.001) for predicting limited nodal burden was number of ultrasound-detected abnormal nodes with ROC AUC = 0.7135 (Fig. 1). Ultrasound cut-offs of 5, 6 and 8 abnormal nodes had respective probabilities of 0.057, 0.026 and 0.005 for <4 metastatic nodes with zero false predictions and 100% specificity.
Fig. 1.
ROC AUC using number of sonographically abnormal nodes = 0.7135.
4.Discussion
Our study showed that a cut-off of ≤5 abnormal nodes on axillary ultrasound can reliably predict patients with limited nodal burden of ≤3 metastatic lymph nodes with zero false prediction. This finding can allow upfront identification of those patients with >3 metastatic nodes who will need chemotherapy regardless to proceed with neoadjuvant chemotherapy. At the same time, clinicians could identify patients who would be suitable for gene assay testing. While there have been many studies on the use of ultrasound for the prediction of axillary burden, this is the first study, to the best of our knowledge, which examined the use of axillary ultrasound, in the RxPONDER trial eligible cohort, to guide neoadjuvant chemotherapy versus upfront surgery and gene assay in patients.
For patients needing chemotherapy, neoadjuvant chemotherapy has advantages such as achieving nodal pathological complete response (pCR) in about 40% of patients [2], avoiding ALND and its complications, allowing shrinkage of the tumour to allow breast conservation, assessing tumour response to chemotherapy and hence providing prognostic information, and buying time for genetic test outcomes to be known [3]. As a result, if chemotherapy was deemed necessary for patients, it was best to be given in the neoadjuvant setting. In HER2 negative and HR positive patients however, the benefits of chemotherapy would be less significant with breast and nodal pCR rates of about 7% and 15% reported in literature respectively [4].
Some have argued that with a lower rate of pCR in these tumour subtypes, these patients can be, instead, subjected to upfront surgery followed by gene assay testing based on the metastatic nodal burden on surgical histology. However, this one size fit all approach would deny some patients, who have high nodal burden and needed chemotherapy, albeit a low but not insignificant chance to achieve nodal pCR with neoadjuvant chemotherapy, hence avoiding ALND and its associated complications [5]. In fact, in this group of patients with Her2 negative/HR positive cancer, PR negativity and high tumour grade can result in a higher nodal pCR rate of 35% and 62% of the patients eligible for breast conserving surgery after neoadjuvant chemotherapy [4]. As a result, it is beneficial that patients with limited or high nodal burden be identified upfront so that they can obtain the maximal benefits from their appropriate individualised treatment.
To date, it is still unclear how much the patients with high nodal burden in this study who would have needed chemotherapy would benefit from neoadjuvant chemotherapy. In a study by Ng S et al, there was no difference in the nodal pCR rates of HR positive/HER2 negative patients with high or low nodal burden [6]. However, that study defined low nodal burden as 1–2 abnormal sonographically nodes and there was no restriction of patients to ≥50 years of age which was done in our study. In another study involving patients with locally advanced breast cancer, there was again no difference in the nodal pCR between patients with initially N1/N2/N3 disease [7]. This was demonstrated again in another study which showed that nodal pCR was independent of the initial nodal burden on ultrasound [8]. However, both studies included patients of all biologic subtypes and not of the Her2 negative and HR positive tumour subset as in our study.
Although various imaging modalities such as MRI, PET etc exist for the axilla [9,10], axillary ultrasound remained the most reliable tool for axillary imaging [11]. In addition, it has additional advantages, such as being radiation-free, portable, relatively quick to perform and widely available [12]. The number of abnormal nodes on axillary ultrasound has also been described in other settings [13–15] to affect clinical decisions. For example, in early breast cancer patients (cT1-2N0) with biopsy-proven metastatic nodes, <3 sonographically abnormal nodes would predict a high likelihood of axillary preservation in the Z11 trial era [14]. As a result, counting the number of abnormal lymph nodes on axillary ultrasound of up to 5 in number would have clinical implications.
The strengths of this study were that all patients underwent ALND so that the true nodal status could be correlated to the axillary ultrasound findings. Being a multicentre study also eliminated intra-institutional selection bias and allowed the results to be extrapolated more widely. This is the first study, to the best of our knowledge, which explored the use of axillary ultrasound to guide breast cancer management in the genomic assay era.
A limitation of this study was that being retrospective, not all the abnormal lymph nodes may have been purposefully identified during some of the axillary ultrasounds.
In conclusion, a cut-off of ≤5 ultrasound detected abnormal nodes is a beneficial clinical guide to predict limited nodal burden, so that this group of patients can undergo a trial of upfront surgery and gene assay testing to potentially avoid chemotherapy. Documenting the number of abnormal nodes of up to 5 on ultrasound during loco-regional staging will be a useful practice to adopt.
Data sharing statement
The data are available from the corresponding author upon request.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
There was no funding for this study.
References
[1] | Kalinsky K, , Barlow WE, , Gralow JR , 21-gene assay to inform chemotherapy benefit in node-positive breast cancer, N Engl J Med, 385: : 2336–2347, (2021) . |
[2] | Lim GH, , Teo SY, , Gudi M , Initial results of a novel technique of clipped node localization in breast cancer patients postneoadjuvant chemotherapy: Skin Mark clipped Axillary nodes Removal Technique (SMART trial), Cancer Med, 9: : 1978–1985, (2020) . |
[3] | Read RL, , Flitcroft K, , Snook KL , Utility of neoadjuvant chemotherapy in the treatment of operable breast cancer, ANZ J Surg, 85: : 315–320, (2015) . |
[4] | Petruolo OA, , Pilewskie M, , Patil S , Standard pathologic features can be used to identify a subset of estrogen receptor-positive, Her2 negative patients likely to benefit from neoadjuvant chemotherapy, Ann Surg Oncol, 24: : 2556–2562, (2017) . |
[5] | Johnson AR, , Kimball S, , Epstein S , Lymphedema incidence after axillary lymph node dissection: Quantifying the impact of radiation and the lymphatic microsurgical preventive healing approach, Ann Plast Surg, 82: (4S Suppl 3): S234–S241, (2019) . |
[6] | Ng S, , Sabel MS, , Hughes TM , Impact of breast cancer pretreatment nodal burden and disease subtype on axillary surgical management, J Surg Res, 261: : 67–73, (2021) . |
[7] | Gentile LF, , Plitas G, , Zabor EC , Tumor biology predicts pathologic complete response to neoadjuvant chemotherapy in patients presenting with locally advanced breast cancer, Ann Surg Oncol, 24: : 3896–3902, (2017) . |
[8] | Yan Z, , Wong A, , Ng RP , Association of the initial number of sonographically abnormal nodes with nodal pathological response and its implication, Clin Imaging, 78: : 19–21, (2021) . |
[9] | Lee IH, , Lee SJ, , Lee J , Utility of 18F-FDG PET/CT for predicting pathologic complete response in hormone receptor-positive, HER2-negative breast cancer patients receiving neoadjuvant chemotherapy, BMC Cancer, 20: : 1106, (2020) . |
[10] | Chang JM, , Leung JWT, , Moy L , Axillary nodal evaluation in breast cancer: State of the art, Radiology, 295: : 500–515, (2020) . |
[11] | Marino MA, , Avendano D, , Zapata P , Lymph node imaging in patients with primary breast cancer: Concurrent diagnostic tools, Oncologist, 25: : e231–e242, (2020) . |
[12] | Upadhyaya VS, , Lim GH, , Chan EYK , Evaluating the preoperative breast cancer characteristics affecting the accuracy of axillary ultrasound staging, Breast J, 26: : 162–167, (2020) . |
[13] | Lim GH, , Teo SY, , Allen Jr JC , Determining whether high nodal burden in early breast cancer patients can be predicted preoperatively to avoid sentinel lymph node biopsy, J Breast Cancer, 22: : 67–76, (2019) . |
[14] | Lim GH, , Upadhyaya VS, , Acosta HA , Preoperative predictors of high and low axillary nodal burden in Z0011 eligible breast cancer patients with a positive lymph node needle biopsy result, Eur J Surg Oncol, 44: : 945–950, (2018) . |
[15] | Lim GH, , Gudi M, , Teo SY , Would removal of all ultrasound abnormal metastatic lymph nodes without sentinel lymph node biopsy be accurate in patients with breast cancer with neoadjuvant chemotherapy? Oncologist, 25: : e1621–e1627, (2020) . |

