
The Evolution of Nadofaragene Firadenovec: A Review and the Path Forward
Abstract
BACKGROUND:
The intravesical gene therapy nadofaragene firadenovec (rAd-IFNα/Syn3) was FDA approved in 2022 for non-muscle invasive bladder cancer (NMIBC) unresponsive to frontline treatment with BCG, and the first gene therapy developed for bladder cancer. This non-replicating recombinant adenovirus vector delivers a copy of the human interferon alpha-2b gene into urothelial and tumor cells, causing them to express this pleotropic cytokine with potent antitumor effects.
OBJECTIVE:
To provide a historical overview describing how several decades of preclinical and clinical studies investigating the role of interferon in the treatment of bladder cancer ultimately led to the development of gene therapy with nadofaragene for NMIBC.
METHODS:
We conducted a review of the literature using PubMed, Google Scholar, and ClinicalTrials.gov to summarize our knowledge of the evolution of interferon-based therapy in NMIBC.
RESULTS:
The FDA approval of this therapy represents an important landmark in urologic oncology and several decades of research dedicated to the study of interferon’s direct and indirect antitumor properties in NMIBC. The data gathered from the phase 1, 2, and 3 clinical trials continue to provide additional insights into the precise mechanisms underlying both the efficacy of and resistance to nadofaragene.
CONCLUSIONS:
Nadofaragene leverages the cytotoxic, anti-angiogenic, and immune-modulatory roles of interferon to effectively treat NMIBC that is resistant to BCG. Ongoing studies of resistance mechanisms and prognostic biomarkers have been promising; these will ultimately improve patient selection and allow for the modulation of factors in the tumor or immune microenvironment to further increase therapeutic response.
BACKGROUND
The search for effective, bladder-sparing therapies for patients with non-muscle invasive bladder cancer (NMIBC) has occupied this disease space for several decades. Transurethral resection of visible tumor followed by intravesical immunotherapy with Bacillus Calmette-Guérin (BCG)—a weakened strain of the bacterium Mycobacterium bovis—is the current standard of care for patients with high-risk disease (carcinoma in situ (CIS), high-grade Ta or T1 tumors) [1]. The clinical activity of BCG against bladder cancer was described in 1976, and it has remained the frontline treatment for these patients for almost sixty years [2]. However, over 50% of patients will have tumor recurrence despite BCG, and 10% will progress [3–5].
Researchers have extensively studied alternative and second-line treatment options, and until recently only two agents were FDA approved for BCG-unresponsive disease. The cytotoxic anthracycline Valrubicin was approved in 1998, despite a dismal complete response (CR) rate of 10% at one year (and disease-free survival of 4% at two years) [6]. Over a decade later, the single-armed trial KEYNOTE-057 led to the FDA approval of pembrolizumab, a PD-1 inhibitor with a somewhat more durable response that came at the cost of systemic immune-related toxicities [7]. Neither of these treatments have been widely adopted by practicing urologists, partially due to the suboptimal response rates and adverse effect profiles. For patients who are unfit or unwilling to undergo major surgery with radical cystectomy, treatment options have remained extremely limited. In December 2022, the first intravesical gene therapy nadofaragene firadenovec (rAd-IFNα/Syn3) was approved for adult patients with high-risk BCG-unresponsive NMIBC with CIS with or without papillary tumors [8]. This novel interferon alpha (IFNα) therapy demonstrated promising durable responses in the phase 3 trial: 45% of patients with CIS and 60% of those with Ta/T1 who achieved a CR at three months remained recurrence free at 12 months [9]. Most recently, in April 2024 nogapendekin alfa inbakicept-pmln was approved for the same indication of BCG-unresponsive NMIBC. Nogapendekin has similar 3-month CR rates as nadofaragene; however, it relies on BCG availability as it is administered intravesically with BCG weekly for 6 weeks as induction therapy followed by either repeat induction vs. maintenance therapy, pending response [10]. The redosing at 3 months for non-responders in the nogapendekin trial make it difficult to compare overall efficacy and CR rates between this drug and nadofaragene [11].
The purpose of this review is to examine the preclinical and clinical studies elucidating the role of interferon in the treatment of bladder cancer that ultimately led to the development of nadofaragene for BCG-unresponsive NMIBC. The approval of rAd-IFNα/Syn3 represents nearly twenty-five years of studies examining bladder tumor immunology and the role of angiogenesis in NMIBC. We also discuss ongoing evaluations of clinical trial data that are providing new insights into mechanisms of tumor immunobiology. A more in-depth understanding of therapeutic susceptibility and resistance will ultimately improve outcomes for patients with NMIBC.
WHY INTERFERON?
The evolution of IFN-based gene therapy can be traced back to the initial discovery of type 1 IFNs by British virologist Alick Isaacs and his Swiss postdoctoral student, Jean Lindenman in 1957. Their seminal work described a substance produced by virus-infected cells—“interferon”—that was capable of interfering with viral growth [12]. Over a decade later in 1969, American immunologist Ion Gresser began publishing his pioneering work demonstrating that these pleiotropic cytokines could also prolong survival in mice inoculated with tumor cells, providing early evidence for the antitumor properties of IFN [13]. Throughout the 1980s, compelling data emerged suggesting that IFNα inhibited angiogenesis and intravesical IFN may have a role in reducing recurrence in bladder cancers [14].
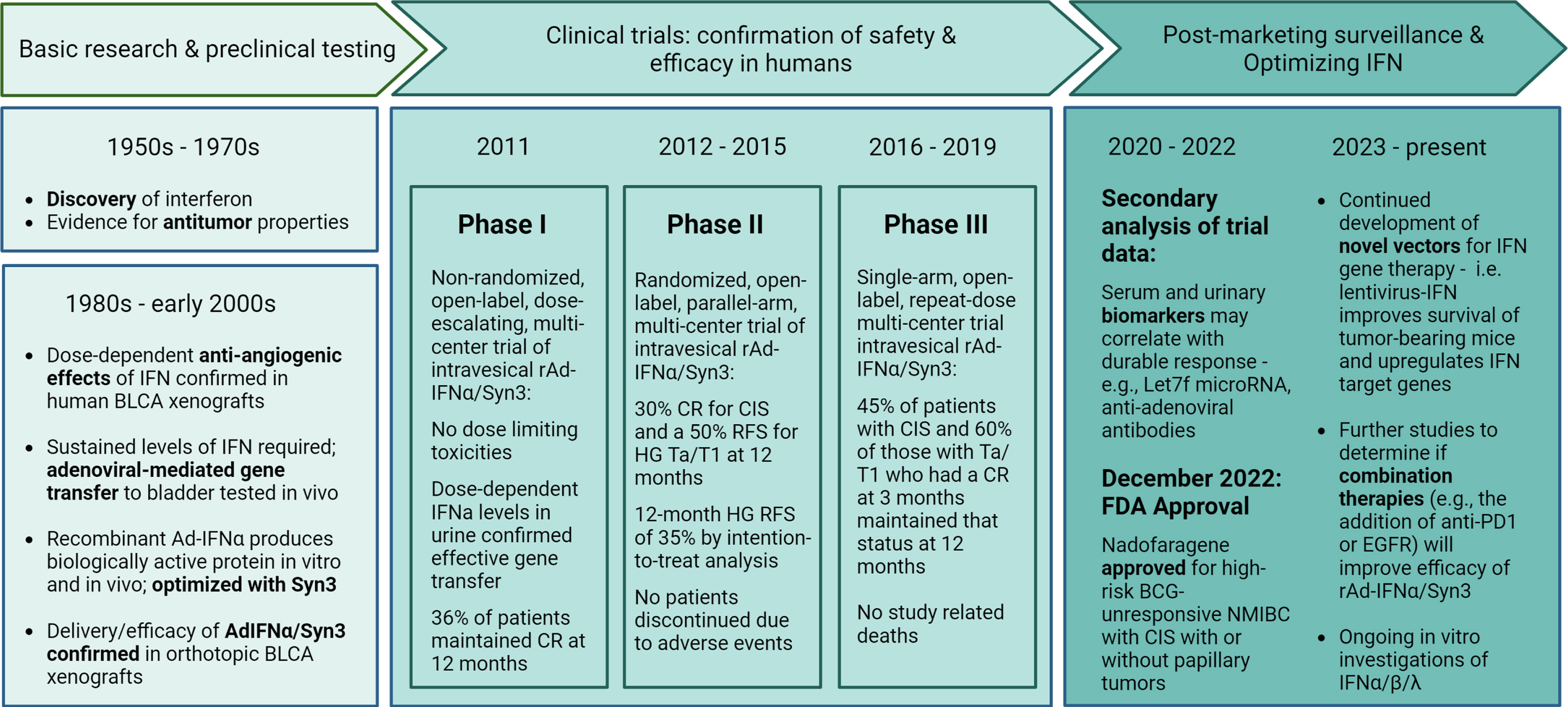
Josh Fidler extensively studied cancer metastasis and tumor biology; work from his lab at the University of Texas MD Anderson Cancer Center (MDACC) demonstrated that IFN had a potent anti-angiogenic effect in colorectal cancer [15]. Fidler was a mentor to urologic oncologist Colin Dinney, who built upon this work and examined IFN’s impact on angiogenesis in bladder cancer [16]. This set the stage for almost 25 years of multi-institutional collaborations dedicated to understanding the immunostimulatory, antiangiogenic, and apoptotic effects of IFN in the setting of bladder malignancy (Fig. 1).
Fig. 1
Key milestones in the evolution of nadofaragene firadenovec-vncg and the path forward. IFN, interferon. BLCA, bladder cancer. Ad, Adenovirus. CR, complete response. CIS, carcinoma in situ. RFS, recurrence free survival. HG, high grade. FDA, Food and Drug Administration. NMIBC, non-muscle invasive bladder cancer. BCG, Bacillus Calmette-Guérin.
DEVELOPMENT OF AN ORTHOPTIC MODEL TO STUDY IFN’S ABILITY TO INHIBIT ANGIOGENESIS
Researchers at MDACC successfully developed an orthotopic model of bladder cancer by implanting a human bladder cancer cell line into the bladders of athymic, nude mice. Through in vivo cycling (where metastases are isolated and cells are reinjected into the bladder wall), aggressive variant cell lines with high tumorigenic and metastatic potential were characterized to better understand the molecular basis of tumor progression [17]. This early work demonstrated that metastatic tumors were highly vascularized and overexpressed pro-angiogenic molecules, such as basic FGF (bFGF).
This in vivo model was then used to determine whether the systemic administration of IFNα could decrease the growth of bladder tumors. Treatment with IFNα led to suppression of bFGF (and to a lesser extent, VEGF), which correlated with reduced microvessel density and decreased tumor growth [16]. This observation was independent of cell lines’ susceptibility to the antiproliferative effects of IFNα, supporting the idea that the inhibition of angiogenesis was a key antitumor mechanism of IFNα [16].
Subsequent experiments confirmed these findings and identified the optimal dosing and schedule of IFNα while further exploring its anti-angiogenic properties [18]. Mice with orthoptic implants were treated with subcutaneous injections of human IFNα, which acted to inhibit the expression of pro-angiogenic factors bFGF, VEGF, and MMP-9; expression inversely correlated with the inhibition of tumor-induced neovascularization and tumor growth [18]. Moreover, researchers found that the optimal schedule of IFNα required daily dosing to downregulate these factors [18]. The need to maintain continuous low levels of IFNα to maximize its effect made this therapy an ideal candidate for viral-mediated gene therapy, where bladder and tumor cells would constantly produce the cytokine without the need for daily re-dosing.
DEVELOPING AND OPTIMIZING GENE THERAPY FOR NMIBC
Intravesical IFN was studied as a therapy for superficial bladder cancer to avoid the significant systemic toxicities associated with IFN. Moreover, intravesical instillation allowed for direct contact with the urothelium and tumor. However, early reports of intravesical IFNα were discouraging, presumably due to the inability to sustain sufficient dwell time and exposure to urothelial cells [19]. Meanwhile, gene therapy had emerged in the 1960s-1970s, and by the 1990s adeno-associated virus-mediated delivery of antiangiogenic factors was emerging as an antitumor strategy [20].
The viral delivery of genes ensures active proteins exist inside transfected cells and are also released into the microenvironment. In the case of bladder cancer therapy, this provides continuous exposure to IFN even with time-limited exposure of the agent to the bladder [19]. Gene therapy also takes advantage of IFN’s ability to directly impede tumor growth, elicit an effective bystander effect, and activate the innate and adaptive immune responses; every tumor cell does not need to take up the vector for it to be efficacious [21]. A series of experiments using human and murine Ad-IFNβ were conducted to study the in vitro and in vivo effects of Ad-IFN and confirm the antiangiogenic effects that had been previously described [22]. Human bladder cancer cells (resistant to the antiproliferative effects of IFN) were infected with Ad-IFNβ, and orthotopically implanted into nude mice. The investigators also directly injected these vectors into human xenografts in nude mice [22]. This study took advantage of the species specificity of Ad-IFNβ to demonstrate that IFN’s effects went well beyond direct toxicity. Murine Ad-IFNβ had no effect on angiogenesis factor expression by the human tumor cells, as it was targeting the microenvironment and not the human tumor cells. Ad-IFNβ effectively inhibited tumor growth and metastasis through antiangiogenic effects (e.g., inhibiting angiogenesis factor production, inducing endothelial cell apoptosis) and neovascularization, and activated host effector cells [22].
The growing interest in Ad-IFN gene therapy for NMIBC led investigators to search for ways to enhance viral transgene expression by removing the glycosaminoglycan (GAG) layer of the bladder surface lining with detergents or chemicals. The GAG layer served as a barrier to cell entry, leading to insufficient gene delivery [23–25]. The solution to this dilemma was discovered by investigators using a rat model to screen compounds that would increase viral transduction and subsequently gene transfer [23]. One detergent tested called BigCHAP showed initial promise, although results were inconsistent when BigCHAP was used from different pharmaceutical producers. Testing different commercially available preparations revealed that the active ingredient in BigCHAP was actually a contaminant of the manufacturing process—an excipient called Syn3 [23].
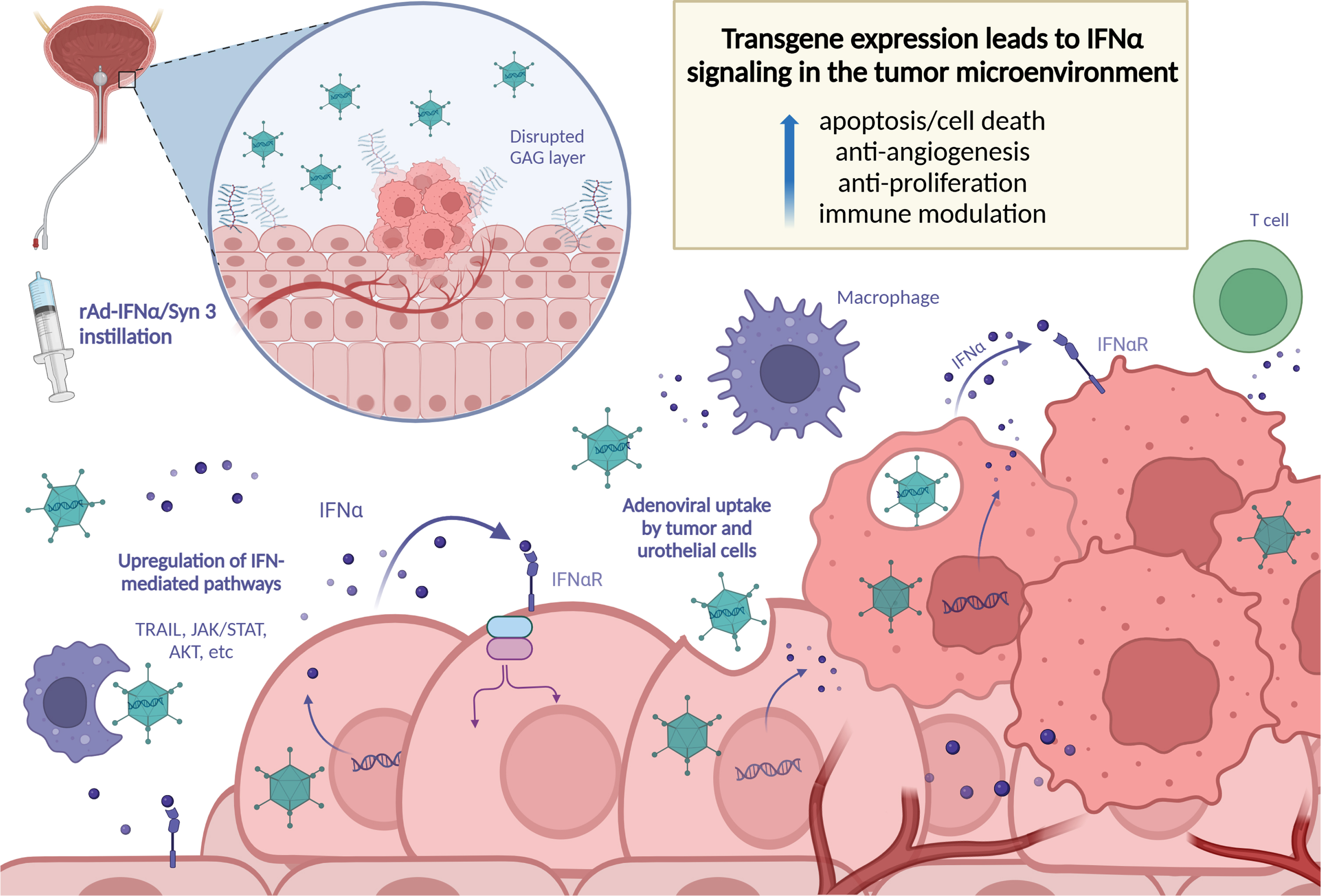
The robust antitumor activity of IFNα (e.g., TRAIL-induced toxicity, caspase-mediated apoptosis, and antiangiogenic effects [18, 26, 27]) was further explored using Ad-IFNα with the addition of Syn3. Important work by Benedict et al. using Ad-IFNα/Syn3 provided additional evidence of the bystander effect induced by Ad-IFNα [28]. Human BLCA cells lines that were resistant to IFN protein underwent apoptosis when exposed to Ad-IFNα; even cells that did not express IFNα underwent apoptosis [28]. The impact of dosing schedule and the ability of Ad-IFNα/Syn3 to provide continuous production and secretion of adequate IFNα levels was assessed in pre-clinical translational studies done in preparation of the phase 2 and 3 clinical trials [29–31]. Intravesical recombinant Ad-IFNα (rAd-IFNα) was administered to rats at varying concentrations, and then re-dosed at both short and long intervals [30]. As hypothesized, the bladder acted as a sort of bioreactor after rAd-IFNα/Syn3 administration, and human IFNα was detectible in the urine for seven days. Longer intervals between doses improved the duration and magnitude of adenoviral gene expression. Importantly, intravesical exposure resulted in only minimal levels of IFNα protein in systemic circulation, and only one intravesical instillation was required [29, 30]. A schematic of the mechanism of intravesical rAd-IFNα/Syn3 is shown in Fig. 2.
Fig. 2
Schematic illustrating the mechanism of intravesical rAd-IFNα/Syn3.
NADOFARAGENE FOR BCG-UNRESPONSIVE NMIBC
The phase 1 dose-escalating clinical trial of 17 patients treated with rAd-IFNα/Syn3 began in April 2011 [32]. Although the study was initiated prior to the formalized FDA definition of BCG failure, it was conducted in patients with NMIBC who had recurred despite standard therapy with BCG. The primary objective was to assess the safety of this therapy, while the secondary endpoints were rAd-IFNα gene expression and evidence of clinical activity at three months. The investigators found that rAd-IFNα/Syn3 was well tolerated, and no dose-limiting toxicities were identified. There were no grade 3 or above adverse events, and the most common adverse events were urgency (88%), headache (59%), and fatigue (47%); urgency was treated effectively using anticholinergic medications. Consistent with preclinical studies, effective gene transfer was demonstrated by elevated IFNα levels in the urine (in a dose-dependent manner for up to 10 days after treatment). 41% of patients achieved a complete response at 3 months [32].
The Society of Urologic Oncology Clinical trials consortium oversaw the randomized, open-label, parallel-arm phase 2 trial of rAd-IFNα/Syn3 which enrolled 43 patients with high grade BCG refractory or relapsed NMIBC [33]. Lack of high-grade disease recurrence at 12 months was the primary end point. Treatment response, incidence and time to cystectomy, and concentration of IFNα in the urine were secondary endpoints. Trial investigators reported a 30% CR for CIS and a 50% HG RFS for HG Ta/T1 at 12 months. Of the 9 patients with a 12-month CR who were also alive and had available follow up data at the end of the study, 8 remained disease-free for 15 to more than 36 months. Again, treatment with Ad-IFNα/Syn3 was well-tolerated; while drug-related adverse events were reported by 85% of patients, no patients discontinued treatment for this reason. Similar to the phase 1 study, urgency was most commonly reported (40% of patients), along with dysuria and fatigue (40% and 32.5%, respectively). In this phase 2 trial, 22% of patients reported grade 3 events such as diarrhea, sepsis, and renal failure, and there were no grade 4 of 5 events [33].
This promising data from the phase 1 and 2 trials supported the registration of a multi-institutional phase 3 study in 2016, which would lay the groundwork for the FDA approval of nadofaragene as the first gene therapy for bladder cancer [9]. Ultimately 151 patients were included in the efficacy analysis. Participants received a single intravesical dose followed by repeat dosing at 3, 6, and 9 months in the absence of high-grade recurrence. 45% of patients with CIS and 60% of those with Ta/T1 who had a CR at 3 months maintained that response at 12 months. Late recurrences beyond 12 months were rare, and only 5% of patients progressed to muscle invasion (eight patients in the entire study population, including five with CIS and three with Ta/T1). In the phase 3 trial, 70% of patients had study drug-related adverse events: 66% had grade 1-2 events and 4% had grade 3. Grade 3 events related to nadofaragene included urgency, bladder spasms, urinary incontinence, syncope, and hypertension; as with the other trials, these reflect a combination of local irritative symptoms and the systemic effects of interferon. Only three patients discontinued therapy due to adverse effects, and there were no treatment related deaths. Overall, treatment with nadofaragene was safe, well-tolerated, and efficacious [9].
BIOMARKERS TO PREDICT RESPONSE AND FURTHER ELUCIDATE UNDERLYING MECHANISMS
The identification of clinical characteristics or biomarkers that accurately predict complete and durable responses can improve patient selection and provide additional information about the mechanistic properties of Ad-IFNα/Syn3, particularly in understanding its ability to decrease angiogenesis and induce cell death and immune pathways. Analysis of urine samples from patients in the phase 2 clinical trial demonstrated that Ad-IFNα/Syn3 induced a sustained IFN phenotypic response in the bladder; there was increased expression of T cell and checkpoint markers, and no single immune cell was responsible for the effect of the therapy [21]. Four days after intravesical instillation, levels of IFNα2 as well as CXL10 (a desirable chemokine attractant of CD8 + T cells) had increased significantly and remained elevated [21]. Other studies have shown that BCG does not induce CXL10 expression, which has been hypothesized to contribute to suboptimal therapeutic responses to BCG [34]. The levels of other urinary cytokines—TRAIL, CCL2, IL-6 and G-CSF—were also trending upwards after exposure to Ad-IFNα/Syn3. Notably, patients who were considered complete responders had a significant correlation of increased urinary IFNα2 and IL-6 levels from day 4 compared to pre-treatment—this was not significant in non-responders [21].
Let7f is another potential urinary biomarker currently under investigation in patients with BCG-unresponsive NMIBC treated with Ad-IFNα/Syn3. Let7f is a non-coding microRNA capable of post-transcriptional gene regulation that has been identified as a possible tumor suppressor in multiple human malignancies, including NMIBC [35]. Loss of let7 leads to overexpression of oncogenic targets, making it a promising therapeutic target and potential biomarker. Detectable Let7f levels in the urine from trial patients correlated with response to Ad-IFNα/Syn3 and were prognostic of treatment response at 12 months [36].
Further exploration of phase 3 data demonstrated that anti-adenoviral antibodies are predictive of a durable response [37]. Patients with a peak antibody titer greater than 800 or a peak fold change greater than 8 were more likely to experience a durable response. Baseline antibody titers were not associated with treatment response. Now that nadofaragene is commercially available, it will be increasingly possible to validate these findings in larger cohorts. Lastly, alterations in urinary tumor DNA may predict response to nadofaragene, and further studies validating the clinical performance of such mutational profiles are underway [48].
NADOFARAGENE ALTERNATIVES IN BCG-UNRESPONSIVE NMIBC
Numerous other therapies are actively being evaluated for patients with BCG-unresponsive NMIBC. Data from a phase 2/3 multicenter trial demonstrated that nogapendekin alfa inbakicept, an IL-15 superagonist, has a significant synergistic effect when given with BCG for this indication; this therapy received FDA approval in April 2024. Unlike in the phase 3 nadofaragene trial, patients who did not respond at 3 months were re-dosed, resulting in a higher CR [10, 11]. A phase 3, single-arm trial of cretostimogene grenadenorepvec—a recombinant oncolytic adenovirus encoding GM-CSF—has completed accrual and is awaiting data maturation (NCT04452591) [38]. Other promising therapies also under investigation in early-stage trials include intravesical enfortumab vedotin, EG-70 (non-viral gene therapy), TAR-200 (sustained release gemcitabine), TARA-002 (cell therapy), and TLD-1433 (photodynamic therapy), among others (NCT05014139, NCT04752722, NCT04640623, NCT05951179, NCT03945162) [39–43].
Finally, repurposing therapies already used in NMIBC may have promise as second- or third-line options for BCG-unresponsive disease and await further prospective validation. Several studies have been published on single-agent intravesical gemcitabine in this population, though larger, well-designed studies are needed [44]. Intravesical chemotherapy with gemcitabine and docetaxel has gained traction as a BCG alternative, and retrospective series of this treatment following BCG failure have demonstrated encouraging results [45, 46]. Hyperthermic intravesical chemotherapy (HIVEC) is currently FDA approved as a BCG alternative, and a recent multicenter retrospective series suggest confirmatory prospective studies in BCG-unresponsive disease may be warranted [47].
CONCLUSION
Although BCG became one of the most successful cancer immunotherapies on the market, even with adequate treatment most patients will eventually recur—and many will progress to incurable disease. For this reason, the addition of this adenoviral vector-mediated gene therapy to the BCG-unresponsive armamentarium has been an important advancement in the management of this challenging disease. Currently, studies are underway investigating methods to modulate factors inherent to nadofaragene sensitivity. Other treatments are also being tested, and innovative combination strategies may ultimately help overcome single-agent resistance mechanisms. While the response rates to nadofaragene are better than other FDA approved treatments, additional work is needed to improve patient selection and provide durable oncologic outcomes for patients with BCG-unresponsive NMIBC.
FUNDING
The authors report no funding.
AUTHOR CONTRIBUTIONS
AS: conception, interpretation of data, writing the article; SM: conception, performance of work, interpretation of data, writing the article; DM: conception, performance of work, interpretation of data; CD: conception, performance of work, interpretation of data, writing the article. All authors have reviewed the paper prior to submission.
CONFLICT OF INTEREST
Alexis Steinmetz: No COI to disclose.
Sharada Mokkapati: No COI to disclose.
David McConkey: Grants or funding: AstraZeneca. Honoraria: Janssen. Editorial Board member of this journal, but was not involved in the peer-review process nor had access to any information regarding its peer-review.
Colin Dinney: Consulting for AstraZeneca. Consulting and stock options for CG Oncology. Research support: shared resources covered by the Cancer Center Support Grant funding from NIH/NCI (award number P30CA016672). Creator of intellectual property owned by UT/MDACC related to the use of genetic alterations as a predictive biomarker for response to Nadofaragene firadenovec. Editorial Board member of this journal, but was not involved in the peer-review process nor had access to any information regarding its peer-review.
REFERENCES
[1] | Chang SS et al.,Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J Urol. (2016) ;196: (4):1021–9. |
[2] | Morales A , Eidinger D , Bruce AW . Intracavitary Bacillus Calmette-Guerin in the treatment of superficial bladder tumors. J Urol. (1976) ;116: (2):180–3. |
[3] | Oddens J et al.,Final Results of an EORTC-GU Cancers Group Randomized Study of Maintenance Bacillus Calmette-Guérin in Intermediate- and High-risk Ta, T1 Papillary Carcinoma of the Urinary Bladder: One-third Dose Versus Full Dose and 1YearVersus 3Years of Maintenance. European Urology. (2013) ;63: (3):462–472. |
[4] | Sylvester RJ , van der MA , Lamm DL . Intravesical bacillus Calmette-Guerin reduces the risk of progression in patients with superficial bladder cancer: a meta-analysis of the published results of randomized clinical trials. J Urol. (2002) ;168: (5):1964–70. |
[5] | Lamm DL et al.,Maintenance bacillus Calmette-Guerin immunotherapy for recurrent TA, T1 and carcinoma in situ transitional cell carcinoma of the bladder: a randomized Southwest Oncology Group Study. J Urol. (2000) ;163: (4):1124–9. |
[6] | Dinney CP , Greenberg RE , Steinberg GD . Intravesical valrubicin in patients with bladder carcinoma in situ and contraindication to or failure after bacillus Calmette-Guérin. Urol Oncol. (2013) ;31: (8):1635–42. |
[7] | Balar AV et al.,Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): an open-label, single-arm, multicentre, phase 2 study. The Lancet Oncology. (2021) ;22: (7):919–930. |
[8] | D.I.S.C.O., F. Burst Edition: FDA approval of Adstiladrin (nadofaragene firadenovec-vncg) for patients with highrisk Bacillus Calmette-Guérin unresponsive non-muscle invasive bladder cancer with carcinoma in situ with or without papillary tumors. January 2023 September 2, 2023]; Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-disco-burst-edition-fda-approval-adstiladrin-nadofaragene-firadenovec-vncg-patients-high-risk#:∼:text=On%20December%%2C%22%2C%20the,with%20or%20without%20papillary%20tumors |
[9] | Boorjian SA et al.,Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: a single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. (2021) ;22: (1):107–117. |
[10] | FDA approves nogapendekin alfa inbakicept-pmln for BCG-unresponsive non-muscle invasive bladder cancer. 2024 [cited 2024 April 24]. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-nogapendekin-alfa-inbakicept-pmln-bcg-unresponsive-non-muscle-invasive-bladder-cancer |
[11] | Chamie K et al.,IL-15 Superagonist NAI in BCGUnresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid. (2023) ;2: (1):EVIDoa2200167. |
[12] | Isaacs A , Lindenmann J , Isaacs A , Virus interference. I. The interferon. Proc R Soc Lond B Biol Sci. (1957) ;147: (927):258–67. |
[13] | Gresser I et al.,Prolongation of the survival time of mice inoculated with tumor cells and treated with preparations of interferon. Comptes rendus hebdomadaires des seances de l’Academie des sciences. Serie D: Sciences Naturelles. (1969) ;268: (6):994–997. |
[14] | Torti FM , Lum BL . Superficial bladder cancer. Risk of recurrence and potential role for interferon therapy. Cancer. (1987) ;59: (3 Suppl):613–6. |
[15] | Fidler IJ , Ellis LM . The implications of angiogenesis for the biology and therapy of cancer metastasis. Cell. (1994) ;79: (2):185–8. |
[16] | Dinney CP et al.,Inhibition of basic fibroblast growth factor expression, angiogenesis, and growth of human bladder carcinoma in mice by systemic interferon-alpha administration. Cancer Res. (1998) ;58: (4):808–14. |
[17] | Dinney CP et al.,Isolation and characterization of metastatic variants from human transitional cell carcinoma passaged by orthotopic implantation in athymic nude mice. J Urol. (1995) ;154: (4):1532–8. |
[18] | Slaton JW et al.,Interferon-alpha-mediated downregulation of angiogenesis-related genes and therapy of bladder cancer are dependent on optimization of biological dose and schedule. Clin Cancer Res. (1999) ;5: (10):2726–34. |
[19] | Narayan VM , Dinney CPN . Intravesical Gene Therapy. Urol Clin North Am. (2020) ;47: (1):93–101. |
[20] | Wirth T , Parker N , Ylä-Herttuala S . History of gene therapy. Gene. (2013) ;525: (2):162–169. |
[21] | Plote D et al.,Inhibition of urothelial carcinoma through targeted type I interferon-mediated immune activation. Oncoimmunology. (2019) ;8: (5):e1577125. |
[22] | Izawa JI et al.,Inhibition of tumorigenicity and metastasis of human bladder cancer growing in athymic mice by interferon-beta gene therapy results partially from various antiangiogenic effects including endothelial cell apoptosis. Clin Cancer Res. (2002) ;8: (4):1258–70. |
[23] | Connor RJ et al.,Identification of polyamides that enhance adenovirus-mediated gene expression in the urothelium. Gene Ther. (2001) ;8: (1):41–8. |
[24] | Yamashita M et al.,Syn3 provides high levels of intravesical adenoviral-mediated gene transfer for gene therapy of genetically altered urothelium and superficial bladder cancer. Cancer Gene Ther. (2002) ;9: (8):687–91. |
[25] | Nagabhushan TL et al.,Enhancement of intravesical delivery with Syn3 potentiates interferon-alpha2b gene therapy for superficial bladder cancer. Cytokine Growth Factor Rev. (2007) ;18: (5-6):389–94. |
[26] | Papageorgiou A , Dinney CP , McConkey DJ . Interferon-alpha induces TRAIL expression and cell death via an IRF-1-dependent mechanism in human bladder cancer cells. Cancer Biol Ther. (2007) ;6: (6):872–9. |
[27] | Yang Z et al.,Direct cytotoxicity produced by adenoviral-mediatedinterferon α gene transfer in interferon-resistant cancercells involves ER stress and caspase 4 activationl. Cancer Gene Ther. (2011) ;18: (9):609–16. |
[28] | Benedict WF et al.,Intravesical Ad-IFNalpha causes marked regression of human bladder cancer growing orthotopically in nude mice and overcomes resistance to IFN-alpha protein. Mol Ther. (2004) ;10: (3):525–32. |
[29] | Tao Z et al.,Efficacy of a single intravesical treatment with Ad-IFN/Syn 3 is dependent on dose and urine IFN concentration obtained: implications for clinical investigation. Cancer Gene Therapy. (2006) ;13: (2):125–130. |
[30] | Connor RJ . Sustained intravesical interferon protein exposure is achieved using an adenoviral-mediated gene delivery system: a study in rats evaluating dosing regimens. Urology. (2005) ;66: (1):224–9. |
[31] | Dinney CP et al.,Focus on bladder cancer. Cancer Cell. (2004) ;6: (2):111–6. |
[32] | Dinney CP et al.,Phase I trial of intravesical recombinantadenovirus ediated interferon-α2b formulated in Syn3 forBacillus Calmette-Guérin failures in nonmuscle invasive bladder cancer. J Urol. (2013) ;190: (3):850–6. |
[33] | Shore ND et al.,Intravesical rAd-IFNα/Syn3 for PatientsWith High-Grade, Bacillus Calmette-Guerin-Refractory or Relapsed Non-Muscle-Invasive Bladder Cancer: A Phase II Randomized Study. J Clin Oncol. (2017) ;35: (30):3410–3416. |
[34] | Muthuswamy R et al.,Combination of α and poly-I:C reprograms bladder cancer microenvironment for enhanced CTL attraction. Journal for ImmunoTherapy of Cancer. (2015) ;3: (1):6. |
[35] | Li Y et al.,The Lin28/let-7a/c-Myc pathway plays a role in non-muscle invasive bladder cancer. Cell Tissue Res. (2013) ;354: (2):533–41. |
[36] | Narayan VM et al.,Let-7f microRNA expression within established bladder cancer subtypes and upregulation with recombinant interferon-alpha. Journal of Clinical Oncology. (2019) ;37: (7_suppl):462–462. |
[37] | Mitra AP , et al.,Antiadenovirus Antibodies Predict Response Durability to Nadofaragene Firadenovec Therapy in BCG-unresponsive Non-muscle-invasive Bladder Cancer: Secondary Analysis of a Phase 3 Clinical Trial. Eur Urol. (2022) ;81: (3):223–228. |
[38] | ClinicalTrials.gov. Identifier NCT04452591, Study of CG0070 Given in Patients With Non-Muscle Invasive Bladder Cancer, Unresponsive to Bacillus-Calmette-Guerin (BOND-003). 2023 [cited 2024 February 20]; Available from:https://clinicaltrials.gov/study/NCT04452591. |
[39] | ClinicalTrials.gov. Identifier: NCT05014139, A Study of Intravesical Enfortumab Vedotin For Treatment of Patients With Non-muscle Invasive Bladder Cancer (NMIBC). 2023 [cited 2024 February 20]; Available from: https://classic.clinicaltrials.gov/ct2/show/NCT05014139. |
[40] | ClinicalTrials.gov. Identifier NCT04640623, A Study of TAR-200 in Combination With Cetrelimab, TAR-200 Alone, or Cetrelimab Alone in Participants With Non-Muscle Invasive Bladder Cancer NMIBC) Unresponsive to Intravesical Bacillus Calmette-GuéWho Are Ineligible for or Elected Not to Undergo Radical Cystectomy (SunRISe-1). 2024 [cited 2024 February 20]; Available from:https://classic.clinicaltrials.gov/ct2/show/NCT04640623. |
[41] | ClinicalTrials.gov. Identifier NCT05951179, Dose Expansion, Safety and Efficacy Study of Intravesical Instillation of TARA-002 in Adults With High-grade Non-muscle Invasive Bladder Cancer (ADVANCED-2). 2023 [cited 2024 February 20]; Available from:https://classic.clinicaltrials.gov/ct2/show/NCT05951179. |
[42] | ClinicalTrials.gov. Identifier NCT03945162, Intravesical Photodynamic Therapy (‘PDT’) in BCG-Unresponsive/Intolerant Non-Muscle Invasive Bladder Cancer (‘NMIBC’) Patients. 2023 [cited 2024 February 20]; Available from:https://classic.clinicaltrials.gov/ct2/show/NCT03945162. |
[43] | ClinicalTrials.gov. Identifier NCT04752722, LEGEND Study: EG-70 in NMIBC Patients BCG-Unresponsive and High-Risk NMIBC Incompletely Treated With BCG or BCG-Naïve. 2024 [cited 2024 February 20];Available from:https://classic.clinicaltrials.gov/ct2/show/NCT04752722. |
[44] | Hurle R et al., Intravesical gemcitabine as bladderpreserving treatment for BCG unresponsive non-muscleinvasive bladder cancer. Results from a single-arm, open-label study. BJUI Compass. (2020) ;1: (4):126–132. |
[45] | Garneau CA et al.,Salvage therapy for BCG failure with intravesical sequential gemcitabine and docetaxel in patients with recurrent NMIBC. Can Urol Assoc J. (2024) ;18: (2):33–40. |
[46] | Steinberg RL , et al.,Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. (2020) ;203: (5):902–909. |
[47] | Pignot G . Efficacy of hyperthermic intravesical chemotherapy (HIVEC) in patients with non-muscle invasive bladder cancer after BCG failure. World J Urol. (2023) ;41: (11):3195–3203. |
[48] | Rac G , Patel HD , James C , Desai S , Caruso VM , Fischer DS , Lentz PS , Ward CT , Mazzarella BC , Phillips KG , Doshi C , Bicocca VT , Levin TG , Wolfe AJ , Gupta GN . Urinary comprehensive genomic profiling predicts urothelial carcinoma recurrence and identifies responders to intravesical therapy. Mol Oncol. (2024) )Feb;18: (2)291–304. doi: 10.1002/1878-0261.13530. |


