
Effect of Bacille Calmette-Guérin for Non–Muscle-Invasive Bladder Cancer After Prostate Radiotherapy
Abstract
BACKGROUND:
Little is known about the impact of prior prostate radiation therapy (RT) on the Bacille Calmette-Guerin (BCG) immunotherapy response in patients with non-muscle invasive bladder cancer (NMIBC).
OBJECTIVE:
We hypothesized that the damaging radiation effects on the bladder could negatively influence BCG efficacy.
METHODS:
Men with a history of high-risk NMIBC were identified within the Surveillance, Epidemiology, and End Results–Medicare database. All patients completed adequate BCG defined as at least 5 plus 2 treatments completed within 12 months. Patients were stratified into 2 groups: with prior RT for prostate cancer and without prior RT before the diagnosis of NMIBC. The primary endpoint was a 5-year composite for progression defined as disease progression requiring systemic chemotherapy, checkpoint inhibitors, radical or partial cystectomy, or cancer-specific death.
RESULTS:
We identified 3,466 patients with NMIBC, including 145 with prior RT for prostate cancer. Five-year progression occurred in 471 patients (13.6%). Patients with prior RT were older than patients without prior RT (77.0 vs 75.0 years; P < .001). The distribution of T stage was significantly different at diagnosis between the RT and non-RT groups (RT: Ta, 44.8%; Tis, 18.6%; T1, 36.6%; without RT: Ta, 40.9%; Tis, 10.8%; T1, 48.3%; P = .002). No difference in the risk of total progression was observed between patients with and without prior RT (P = .67). Similarly, no difference was observed after multivariable adjustment (hazard ratio, 0.99; 95% CI, 0.61-1.58; P = .95).
CONCLUSION:
For patients with NMIBC who undergo adequate BCG treatment, prior RT for prostate cancer was not associated with worse 5-year progression-free survival.
Abbreviations
AJCC | American Joint Committee on Cancer |
BCG | bacille Calmette-Guerin |
HR | hazard ratio |
NMIBC | non–muscle-invasive bladder cancer |
RT | radiation therapy |
SEER | Surveillance, Epidemiology, and End Results |
TURBT | transurethral resections of bladder tumor |
Tis | carcinoma in situ |
INTRODUCTION
Bacille Calmette-Guérin (BCG) therapy is the treatment of choice for high-risk non–muscle-invasive bladder cancer (NMIBC) [1]. Although its mechanism of action is incompletely understood, this mycobacterial-based intravesical treatment is believed to function by activating the cellular inflammatory response, leading to immune stimulation and antitumor effect [2]. Failure rates for BCG intravesical therapy are estimated at 20% to 40% [3, 4]. BCG treatment failure has been associated with biological factors, such as tumor stage and variant histologic characteristics, and treatment factors including inadequate BCG doses [5–7]. Environmental risk factors such as radiation exposure have been associated with bladder cancer development, but little is known about the relationship of radiation therapy (RT) to BCG treatment response [8–15].
Radiation exposure is known to cause perivascular fibrosis and urothelial nuclear irregularity and to disrupt urothelial cellular connections [16, 17]. A systematic review and meta-analysis showed that the risk of bladder cancer among patients who have undergone RT for prostate cancer is 1.7 times that of patients unexposed to RT [8]. These effects have translated to worse oncologic outcomes for some patients with bladder cancer who previously received RT [8–11, 18]. For instance, patients with muscle-invasive bladder cancer with prior radiation exposure are more likely than patients without radiation exposure to have adverse pathologic outcomes at radical cystectomy [9, 18, 19]. For patients with NMIBC, some evidence exists that prior radiation exposure is a risk factor for decreased cancer-specific survival [20]. However, what effect RT has on BCG response is unclear for patients with high-risk NMIBC.
In this study, we evaluated the risk of NMIBC disease progression posed by prior RT and the outcomes at a population level. Because radiation damage may hinder the immune response, we hypothesized that patients with NMIBC and prior RT for prostate cancer would have poorer oncologic outcomes after BCG treatment. Given the national shortages of BCG, identification of factors predisposing patients to a poor response to BCG therapy is critical. Patients deemed at high risk for BCG treatment failure could receive expedited use of potentially more efficacious oncologic treatments, such as radical cystectomy, or participate in clinical trials investigating the role of other intravesical and immune therapies.
PATIENTS AND METHODS
Study cohort and design
This study was approved by the Mayo Clinic Institutional Review Board (protocol #21-011911, approved December 6, 2021). A retrospective study was performed by using the linked Surveillance Epidemiology and End Results (SEER)–Medicare database and by focusing on patients with bladder cancer diagnosed from 2000 through 2013. All relevant, deidentified data supporting the findings of this study are reported in the article and the supplemental materials. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines [21].
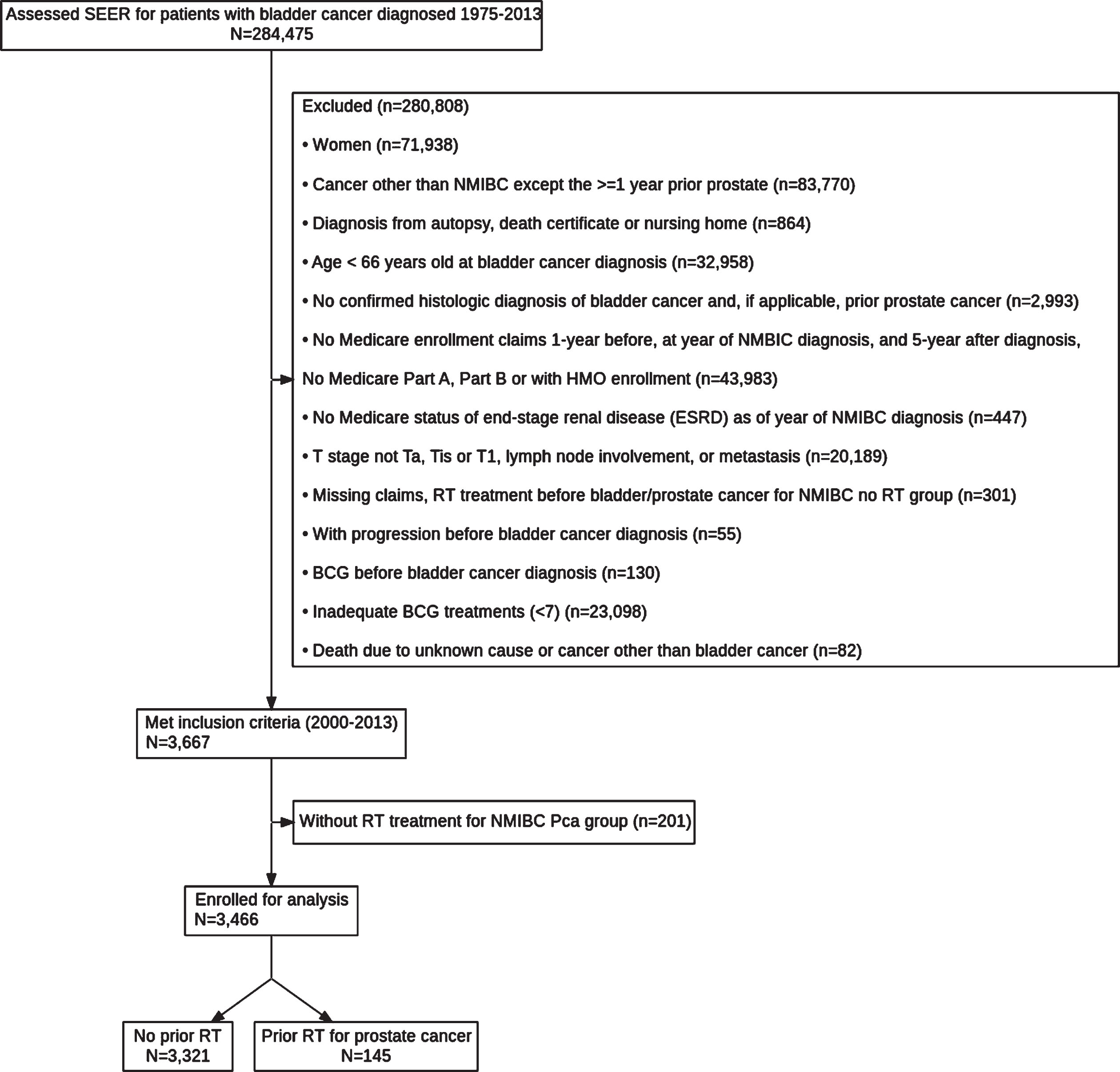
Men 66 years or older at their first bladder cancer diagnosis were selected for the study (Fig. 1). Patients were required to have Medicare Parts A and B and not be enrolled in a health maintenance organization plan for 1 year before and in the year of their bladder cancer diagnosis and for up to 5 years afterward (Fig. 1). A histologic diagnosis of bladder cancer and prior prostate cancer (if applicable) was confirmed on the SEER pathology report. Patients were excluded if the diagnosis of bladder cancer or prior prostate cancer was obtained from an autopsy, death certificate, or nursing home report; if they had an unknown cause of death; or if they died of cancer other than bladder cancer. Patients were required to have an NMIBC diagnosis staged at Ta, Tis, or T1. All patients received adequate BCG, defined as at least 5 initial treatments plus 2 treatments completed within 12 months [22].
Fig. 1
Flowchart for Identifying Patients in SEER Database with NMIBC and Adequate BCG Therapy With and Without a History of RT for Prostate Cancer. BCG indicates bacille Calmette-Guérin; ESRD, end-stage renal disease; HMO, health maintenance organization; NMIBC, non–muscle-invasive bladder cancer; RT, radiation therapy; SEER, Surveillance Epidemiology and End Results.
The cohort was stratified into 2 groups: 1) patients who had a prostate cancer diagnosis and RT at least 1 year before bladder cancer diagnosis (RT group) and 2) patients without prior RT (i.e., bladder cancer was the only primary cancer diagnosis; non-RT group). The presence of prostate cancer was identified by noting documented International Classification of Diseases diagnosis codes for prostate cancer (Ninth and Tenth Revisions and Oncology, Third Edition; Supplementary Table 1). We excluded all other cancer diagnoses except prostate cancer before bladder cancer diagnosis and all cancer diagnoses including prostate cancer after bladder cancer diagnosis. Additionally, a sensitivity analysis was performed comparing outcomes for NMIBC patients with or without a history of RT regardless of BCG treatment.
The primary endpoint was total disease progression at 5 years after diagnosis, a composite endpoint that included all the secondary outcomes: definitive surgical treatment (i.e., radical or partial cystectomy) [23], use of systemic chemotherapy, use of checkpoint inhibitors, or cancer-specific death. Chemotherapy billing codes from the Healthcare Common Procedure Coding System were for chemotherapy agents typical for treatment of bladder cancer, including cisplatin, carboplatin, vincristine, methotrexate, doxorubicin, and gemcitabine (Supplementary Table 1). Disease progression to use of checkpoint inhibitors was defined as use of avelumab, atezolizumab, nivolumab, pembrolizumab, or durvalumab (Supplementary Table 1).
Statistical analysis
Patients’ demographic and clinical characteristics were summarized with the median (IQR) for continuous variables and count (percentage) for categorical variables. The Wilcoxon rank sum test was used for comparing continuous variables, and the χ2 test was used for comparing categorical variables. Univariate and multivariable analyses were performed for 5-year progression by using the Fine and Gray subdistribution hazard model [24]. Definitive surgical treatment (i.e., radical or partial cystectomy), use of systemic chemotherapy, use of checkpoint inhibitors, or cancer-specific death was considered the event, and death due to other cause was used as the competing event to evaluate the effect of patient characteristics on 5-year progression. Patient characteristics studied were the NMIBC group (with or without prior PT), the patient’s region of residence, Charlson Comorbidity Index scores and comorbid conditions, the number of transurethral resections of bladder tumor (TURBT) after bladder cancer diagnosis, and American Joint Committee on Cancer (AJCC) T stage adjusted for patients race and age at bladder cancer diagnosis. The cumulative incidence function of 5-year progression was estimated and plotted for 2 NMIBC groups and AJCC T stage with the Gray K-sample test [25]. Statistical analysis was conducted with SAS version 9.4 (SAS Institute Inc). All tests were 2-sided, and P values < .05 were considered significant.
RESULTS
Among 3,466 patients who underwent adequate BCG treatment for NMIBC, 145 had a history of RT for prostate cancer before their bladder cancer diagnosis, and 3,321 had no prior RT. Table 1 shows baseline demographic and pathologic characteristics. Patients with prior RT were significantly older than patients without prior RT, with a median age (IQR) of 77.0 years (73.0-82.0 years) vs 75.0 years (71.0-80.0 years) (P < .001). Median income for zip code was also significantly higher for patients with a history of prior radiation therapy (57,000 vs 52,000, P = .04), but no other significant differences in demographic characteristics were observed between the two groups. Charlson Comorbidity Index scores and rates of comorbid conditions were similar except for moderate to severe kidney disease, which was higher in the RT group than the non-RT group (11.0% vs 6.0%, P = .01).
On review of the initial pathologic diagnosis, a significant difference was observed in the AJCC T stage (P = .002), with carcinoma in situ (Tis) being more common in the RT group (18.6% vs 10.8%). Conversely, T1 disease was more prevalent in the non-RT group (48.3% vs 36.6%). Rates of Ta disease were similar (40.9% vs 44.8%) between the groups. Tumor pathologic grades also were similar between the groups (P = .63). All other comparisons were similar between the groups (Table 1).
Table 1
Demographic and Tumor Characteristics for Patients With NMIBC (N = 3,466)a
| Characteristic | Without prior radiation therapy (n = 3,321) | With prior radiation therapy (n = 145) | P value |
| Age, y | 75.0 (71.0-80.0) | 77.0 (73.0-82.0) | <.001 |
| Race and ethnicity | .16 | ||
| White | 3,128 (94.2) | >123 (>84.8) | |
| Black | 60 (1.8) | <11 (<7.6) | |
| Otherb | 110 (3.3) | <11 (<7.6) | |
| Unknown | 23 (0.7) | 0 (0.0) | |
| Married | 2,424 (77.3) | 103 (76.9) | .91 |
| Median income for zip code (×$10,000) | 5.2 (3.8-6.9) | 5.7 (4.4-7.1) | .04 |
| Region of patient residence | .08 | ||
| Midwest | 345 (10.4) | 15 (10.3) | |
| Northeast | 790 (23.8) | 45 (31.0) | |
| South | 816 (24.6) | 24 (16.6) | |
| West | 1,370 (41.3) | 61 (42.1) | |
| Rural-Urban Continuum Code | (n = 3,320) | .26 | |
| Metropolitan counties | 2,768 (83.4) | 126 (86.9) | |
| Nonmetropolitan counties | 552 (16.6) | 19 (13.1) | |
| Comorbid conditions | |||
| History of myocardial infarction | 129 (3.9) | <11 (<7.6) | .88 |
| Peripheral vascular disease | 407 (12.3) | 22 (15.2) | .30 |
| Diabetes | 882 (26.6) | 40 (27.6) | .78 |
| Moderate to severe kidney disease | 200 (6.0) | 16 (11.0) | .01 |
| Charlson Comorbidity Index score | .13 | ||
| 0-1 | 2,469 (74.3) | 97 (66.9) | |
| 2-3 | 645 (19.4) | 36 (24.8) | |
| ≥4 | 207 (6.2) | 12 (8.3) | |
| AJCC T stage | .002 | ||
| Ta | 1,359 (40.9) | 65 (44.8) | |
| Tis | 359 (10.8) | 27 (18.6) | |
| T1 | 1,603 (48.3) | 53 (36.6) | |
| Grade | .63 | ||
| Low Grade | 836 (30.5) | 30 (28.3) | |
| High Grade | 1908 (69.5) | 76 (71.7) | |
| Tumor histologic findings | .75 | ||
| Unspecified neoplasms | <11 (<0.3) | 0 (0.0) | |
| Epithelial neoplasms | 34 (1.0) | <11 (<7.6) | |
| Squamous cell neoplasms | 14 (0.4) | 0 (0.0) | |
| Transitional cell carcinomas | >3,240 (>97.6) | >134 (>92.4) | |
| Adenomas and adenocarcinomas | <11 (<0.3) | 0 (0.0) | |
| Cystic, mucinous, and serous neoplasms | <11 (<0.3) | 0 (0.0) | |
| BCG treatments within 1 y after bladder cancer diagnosis, No. | 9.0 (8.0-12.0) | 10.0 (9.0-12.0) | .42 |
| BCG treatments > 1 y after bladder cancer diagnosis, No. | 6.0 (3.0-10.0) | 6.0 (3.0-10.5) | .70 |
| Time from bladder cancer diagnosis to earliest BCG treatment within 1 y after bladder cancer diagnosis, d | 59.0 (42.0-90.0) | 58.0 (39.0-89.0) | .80 |
| TURBT after bladder cancer diagnosis at 5-y follow-up visit, No. | 3.0 (2.0-4.0) | 3.0 (2.0-5.0) | .14 |
Abbreviations: AJCC, American Joint Committee on Cancer; BCG, bacille Calmette-Guérin; NMIBC, non–muscle-invasive bladder cancer; TURBT, transurethral resections of bladder tumor. aData are number (%) or median (IQR). Specific numbers fewer than 11 cannot be reported according to requirements from Surveillance, Epidemiology, and End Results. bOther race includes American Indian/Alaska Native and Asian/Pacific Islander.
In the RT group, the median time elapsed from RT to bladder cancer diagnosis was 1,432.5 days (IQR, 767.5-2,492.5 days). Most patients had an unspecified modality of RT. However, 52 patients (35.9%) were confirmed to have brachytherapy; fewer than 11 patients (<7.6%) underwent proton beam RT, and fewer than 11 patients (<7.6%) had intensity-modulated RT.
At 5-year follow-up, 471 patients (13.6%) experienced disease progression (Table 2). When 5-year total progression was analyzed, no significant difference was observed between the 2 groups (P = .67). Progression to systemic chemotherapy and progression to checkpoint inhibitor therapy were similar between the RT and non-RT groups (P = .82 and P = .13, respectively). Rates of progression to radical or partial cystectomy also did not significantly differ (P = .29 and P = .62, respectively). The number of cancer-specific deaths at 5-year follow-up was found to be comparable regardless of RT history (P = .05). The median days to progression or last follow up between the 2 groups, excluding cancer-specific death, were similar (P = .93), with the median number of days to earliest progression being 60 months for both the irradiated and nonirradiated cohorts.
Table 2
Five-year disease progression outcomes for patients with non–muscle invasive bladder cancera
| Outcome | Without prior radiation therapy (n = 3,321) | With prior radiation therapy (n = 145) | P value |
| Systemic chemotherapy | 191 (5.8) | <11 (<7.6) | .82 |
| Checkpoint inhibitors | <11 (<0.3) | <11 (<7.6) | .13 |
| Radical cystectomy | 145 (4.4) | <11 (<7.6) | .29 |
| Partial cystectomy | 32 (1.0) | <11 (<7.6) | .62 |
| Cancer-specific death | 233 (7.0) | <11 (<7.6) | .05 |
| 5-year total progressionb | 453 (13.6) | 18 (12.4) | .67 |
| Time from bladder cancer diagnosis to earliest progression, median (IQR), mo | 60.0 (48.0-60.0) | 60.0 (51.0-60.0) | .93 |
aData are number (%) unless otherwise indicated. Specific numbers fewer than 11 cannot be reported according to requirements from Surveillance, Epidemiology, and End Results. bFive-year total progression included progression to requiring systemic chemotherapy, checkpoint inhibitors, radical or partial cystectomy, or cancer-specific death.
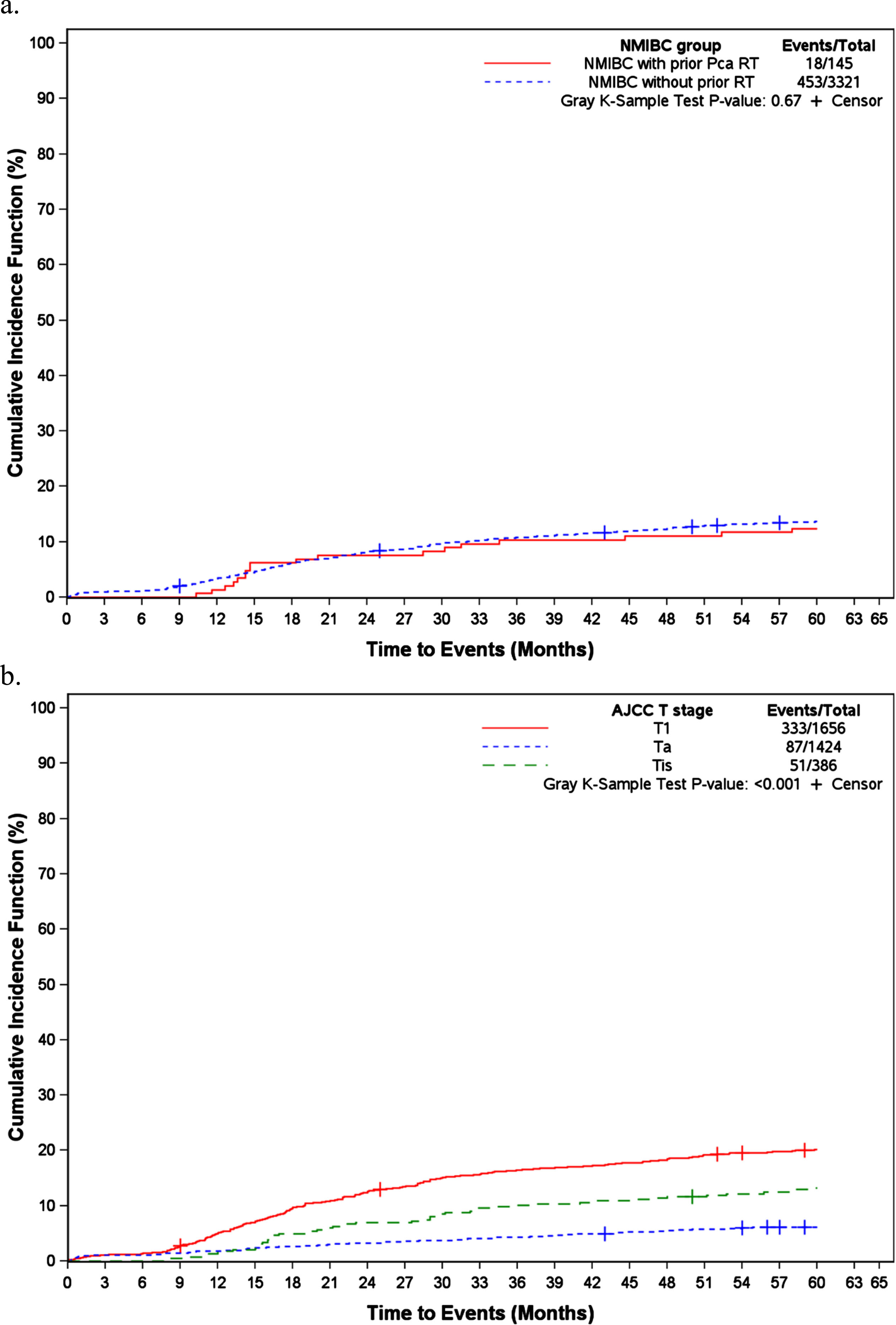
On multivariable analysis for variables affecting 5-year progression, those with more TURBT performed after bladder cancer diagnosis had a higher risk of progression (hazard ratio [HR], 1.14; 95% CI, 1.11-1.17; P < .001) (Table 3). Patients with Tis disease were 2.1 times more likely to have progression as patients with Ta disease (HR, 2.14; 95% CI, 1.51-3.03; P < .001), and patients with T1 disease were 3.4 times as likely to have progression (HR, 3.36; 95% CI, 2.65-4.26; P < .001). A history of RT was not associated with 5-year progression (P = .95). The cumulative incidence function also showed that radiation exposure history (P = .67) was not significantly associated with progression, unlike AJCC T stage (P < .001) (Fig. 2).
Table 3
Multivariable fine and gray subdistribution hazards model with month from bladder cancer diagnosis to 5-year total progression as the outcome
| Variable | Comparison | HR (95% CI) | P value |
| NMIBC group | With prior prostate cancer RT vs without prior RT | 0.99 (0.61-1.58) | .95 |
| Age at Bladder Cancer Diagnosis | 1-unit Increase (per 10 years) | 1.03 (0.89, 1.19) | .68 |
| White | No vs Yes | 1.03 (0.66, 1.60) | .90 |
| Rural-Urban SEER Status | Nonmetropolitan vs Metropolitan Counties | 1.33 (1.06, 1.67) | 0.01 |
| Categorical Charlson Comorbidity Index score | 2-3 vs 0-1 | 0.92 (0.72-1.16) | .47 |
| ≥4 vs 0-1 | 1.00 (0.68-1.46) | >0.99 | |
| No. of TURBT after bladder cancer diagnosis | 1-unit Increase | 1.14 (1.11-1.17) | <.001 |
| AJCC T stage | T1 vs Ta | 3.36 (2.65-4.26) | <.001 |
| Tis vs Ta | 2.14 (1.51-3.03) | <.001 |
Abbreviations: AJCC, American Joint Committee on Cancer; HR, hazard ratio; NMIBC, non–muscle-invasive bladder cancer; RT, radiation therapy; TURBT, transurethral resections of bladder tumor.
Fig. 2
Cumulative Incidence Function of 5-Year Progression of NMIBC With Corresponding Plots at Each Time Point. A, NMIBC group. B, AJCC T stage. AJCC indicates American Joint Committee on Cancer; NMIBC, non–muscle-invasive bladder cancer; PCa, prostate cancer; RT, radiation therapy.
In the sensitivity analysis cohort, non-RT and RT NMIBC patients were compared regardless of BCG history. Similar to the primary cohort, NMIBC patients with a history of RT were significantly older, with a median age (IQR) of 78.0 years (74.0-83.0 years) vs 77.0 years (72.0-82.0 years) (P < .001) (Supplementary Table 3). Again, higher rates of Tis and Ta were present in the RT group (Tis 9.3% vs 7.0%, Ta 66.4% vs 61.6%, P < .001). There was no significant difference in patients who received BCG treatments within 1-year post bladder cancer diagnosis when comparing the RT and non-RT groups (32.9% v 34.0%, P = 0.46). Evaluation of 5-year disease progression outcomes revealed no significant difference in progression to checkpoint inhibitors, partial or radical cystectomy or cancer-specific death (Supplementary Table 3). Progression to systemic chemotherapy was slightly higher in the RT group (5.2%) compared to the non-RT group (4.0%, P = 0.04). However, the 5-year disease progression rates were comparable between the two groups (RT 12.5% v non-RT 12.7%, P = 0.83) (Supplementary Table 3). On multivariable analysis, RT was not associated with higher rates of progression (hazard ration, 1.06; 95% CI, 0.90-1.24, P = 0.52) (Table 4).
Table 4
Multivariable fine and gray subdistribution hazards model for sensitivity analysis with month from bladder cancer diagnosis to 5-year total progression as the outcome
| Variable | Comparison | HR (95% CI) | P value |
| NMIBC group | NMIBC with prior Pca RT vs NMIBC without prior RT | 1.06 (0.90, 1.24) | 0.52 |
| Age (per 10 years) at Bladder cancer Diagnosis | 1 Unit increase | 1.19 (1.13, 1.26) | <.001 |
| White | No vs Yes | 1.26 (1.09, 1.46) | .002 |
| Rural-Urban SEER Status | Nonmetropolitan vs Metropolitan Counties | 1.07 (0.97, 1.18) | 0.16 |
| Categorical Charlson Comorbidity Index score | 2-3 vs 0-1 | 0.96 (0.88, 1.05) | 0.37 |
| 4 + vs 0-1 | 1.07 (0.95, 1.21) | 0.27 | |
| Number of TURBT post bladder cancer DX for 5-year follow up | 1 Unit increase | 1.07 (1.06, 1.08) | <.001 |
| AJCC T Stage | T1 vs Ta | 5.13 (4.70, 5.61) | <.001 |
| Tis vs Ta | 2.31 (1.98, 2.69) | <.001 | |
| With BCG 1-year post DX treatment or not | Yes vs No | 0.85 (0.78, 0.92) | <.001 |
Abbreviations: AJCC, American Joint Committee on Cancer; HR, hazard ratio; NMIBC, non–muscle-invasive bladder cancer; RT, radiation therapy; TURBT, transurethral resections of bladder tumor.
DISCUSSION
We reviewed 3,466 patients with NMIBC in the SEER-Medicare database with or without a history of RT for prostate cancer and observed that prior RT was not associated with NMIBC disease progression after BCG therapy at 5-year follow-up. This observation remained true on the multivariable model evaluating 5-year disease progression. These results suggest that BCG response in patients with a history of prostate cancer RT is not impacted, and a history of RT does not predict NMIBC response, progression or survival.
Pelvic radiation exposure is a known risk factor for development of secondary cancers [8–15]. Studies have found poorer clinical characteristics associated with radiation-induced bladder cancer. A study assessing patients after cystectomy to treat bladder cancer found increased risks of locally advanced tumors and poorer survival for patients with prior RT for prostate cancer than those without prior RT [18]. Another retrospective study of bladder cancer cases found similar results comparing 83 previously irradiated patients with 61 nonirradiated patients, with evidence of significantly higher tumor grade and higher stage progression of disease [27].
The aforementioned studies evaluated radiation-related bladder tumors, but little evidence exists on the effectiveness of intravesical therapies in an irradiated population. In 2013, Rao et al. [28] published an analysis of 26 previously irradiated patients with subsequent high-risk NMIBC who completed at least 1 induction BCG course. The study found a 50% response rate to BCG therapy at a median of 5 years’ follow-up, which is comparable to the known mean BCG response rates. We also have evaluated in a single-institution retrospective setting the effect of previous RT on NMIBC outcomes after at least 1 induction BCG course. Twenty-three patients with a history of prostate cancer RT were compared with 159 patients who did not receive RT. Although limited by the study design and small sample size, the analysis did not show a significant effect on recurrence or progression at 1-year follow-up for previously irradiated patients compared with nonirradiated patients [29].
To our knowledge, the current study is the first to evaluate the effectiveness of adequate BCG therapy for previously irradiated patients at a population level. Our data provide reassuring evidence of the effectiveness of BCG, the standard-of-care intravesical treatment, in this specific patient population. The primary cohort data showed similar cancer-specific mortality and 5-year disease progression outcomes for both the RT and non-RT groups. The sensitivity analysis further confirmed that a history of RT did not significantly affect cancer-specific death and progression of disease to extirpative therapy regardless of BCG treatment.
With regards to prior outcome analyses, the SEER study by Alam et al. [20] found that patients with radiation-related bladder tumors actually had an increased risk of bladder cancer–specific death compared to non-irradiated patients. The greatest increase in risk of bladder cancer–specific deaths occurred in irradiated patients with initial Tis. Patients with prior RT had lower rates of T1 disease and higher rates of Tis at the initial bladder cancer diagnosis, findings that align with our results. On the basis of these data, prior RT may be associated with increased risk of Tis which is acknowledged as a particularly high-risk subtype of NMIBC. However, the effect of RT on cancer-specific survival remains unclear.
As mentioned, this study has limitations. It is inherently limited by its retrospective nature. Additionally, not all variables of interest were included in the analysis due to a lack of SEER data. Ideally, smoking history, family history, body mass index, and tumor size would have been evaluated but were excluded because data were incompletely recorded or had mostly unknown values in the SEER database. Knowledge of BCG intolerance or adverse events (i.e. irritative urinary symptoms) were also unable to be compared between the RT and non-RT groups given the limitations of the SEER data. Lack of billing or coding data limited our evaluation because most irradiated patients did not have a specific RT modality recorded. In theory, the unknown modality could affect outcomes because some authors have postulated that brachytherapy may be less likely than other targeted therapies to induce secondary cancers [30]. Furthermore, although this study used a large population database, the cohort of interest— patients with NMIBC and prior RT for prostate cancer— was small (n = 145). We acknowledge that the study’s power may be low given the sample size. Finally, progression to metastasis was excluded as a marker for disease progression due to concern for potential unreliability per SEER Medicare reports.
Conclusion
Overall, among patients with NMIBC who completed adequate BCG, those who received prior RT for prostate cancer did not have a higher risk of 5-year bladder cancer progression, including progression to systemic therapy, checkpoint inhibitors, definitive surgery, or cancer-specific death, compared with nonirradiated patients. Although possessing some limitations, our data suggest that patients with a history of RT are appropriately allocated BCG therapy. During BCG shortages, the current study provides evidence that BCG remains effective for previously irradiated patients with NMIBC.
ACKNOWLEDGMENTS
The authors acknowledge the efforts of the National Cancer Institute; Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database.
FUNDING
This study was supported by Grant Number P30 CA015083 from the National Cancer Institute. This research also received funding from the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery (M.D.T.), the Christian Haub Family Career Development Award for Cancer Research Honoring Dr. Richard Emslander (M.D.T.), the Eric and Gail Blodgett Foundation (M.D.T.), and Chris and Jasmine Endras. The funding sources had no involvement in writing the manuscript or submitting it for publication.
AUTHOR CONTRIBUTIONS
Dr(s) Mark Tyson, Adri Durant, [2-author limit for full access] had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Mark Tyson, Adri Durant, Lanyu Mi. Analysis and interpretation of data: Mark Tyson, Adri Durant, Lanyu Mi. Drafting of the manuscript: Durant, Yeonsoo Lee. Critical revision of the manuscript for important intellectual content: Kassem Faraj, Timothy Lyon, Parminder Singh, Lanyu Mi. Statistical analysis: (list the last name of the author or, if reviewed by a statistician who is not an author, provide the name plus affiliation of the statistician in an acknowledgment). Obtained funding: Mark Tyson. Administrative, technical, or material support: N/A. Study supervision: Mark Tyson.
ETHICAL CONSIDERATIONS
This study used the linked SEER-Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors. The authors acknowledge the efforts of the National Cancer Institute; Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database.
The collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention’s National Program of Cancer Registries, under cooperative agreement 1NU58DP007156; the National Cancer Institute’s SEER Program under contract HHSN261201800032I awarded to the University of California, San Francisco, contract HHSN261201800015I awarded to the University of Southern California, and contract HHSN261201800009I awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the authors and do not necessarily reflect the opinions of the State of California, Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors.
Kathleen Louden, ELS, senior scientific/medical editor, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff, Mayo Clinic, provided proofreading, administrative, and clerical support.
CONFLICTS OF INTEREST
Adri M. Durant, Yeonsoo S. Lee, Lanyu Mi, Kassem Faraj, Timothy D. Lyon, Parminder Singh and Mark D. Tyson II have no known conflicts of interest.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions of the SEER Medicare database.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/BLC-230073.
REFERENCES
[1] | Chang SS , Boorjian SA , Chou R , et al., Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO Guideline. J Urol. (2016) ;196: :1021–9. |
[2] | Redelman-Sidi G , Glickman MS , Bochner BH . The mechanism of action of BCG therapy for bladder cancer: a current perspective. Nat Rev Urol. (2014) ;11: :153–62. |
[3] | Witjes JA . Management of BCG failures in superficial bladder cancer: a review. Eur Urol. (2006) ;49: :790–7. |
[4] | Gual Frau J , Palou J , Rodriguez O , Parada R , Breda A , Villavicencio H . Failure of Bacillus Calmette-Guerin therapy in non-muscle-invasive bladder cancer: definition and treatment options. Arch Esp Urol. (2016) ;69: :423–33. |
[5] | Sylvester RJ , van der Meijden AP , Oosterlinck W , et al., Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. (2006) ;49: :466–5; discussion 75–7. |
[6] | Solsona E , Iborra I , Dumont R , Rubio-Briones J , Casanova J , Almenar S . The 3-month clinical response to intravesical therapy as a predictive factor for progression in patients with high risk superficial bladder cancer. J Urol. (2000) ;164: :685–9. |
[7] | Zlotta AR , Fleshner NE , Jewett MA . The management of BCG failure in non-muscle-invasive bladder cancer: an update. Can Urol Assoc J. (2009) ;3: :S199–205. |
[8] | Wallis CJ , Mahar AL , Choo R , et al . Second malignancies after radiotherapy for prostate cancer: systematic review and meta-analysis. BMJ. (2016) ;352: :i851. |
[9] | Abern MR , Dude AM , Tsivian M , Coogan CL . The characteristics of bladder cancer after radiotherapy for prostate cancer. Urol Oncol. (2013) ;31: :1628–34. |
[10] | Moschini M , Zaffuto E , Karakiewicz PI ,et al., External beam radiotherapy increases the risk of bladder cancer when compared with radical prostatectomy in patients affected by prostate cancer: a population-based analysis. Eur Urol. (2019) ;75: :319–28. |
[11] | Jin T , Song T , Deng S , Wang K . Radiation-induced secondary malignancy in prostate cancer: a systematic review and meta-analysis. Urol Int. (2014) ;93: :279–88. |
[12] | Dracham CB , Shankar A , Madan R . Radiation induced secondary malignancies: a review article. Radiat Oncol J. (2018) ;36: :85–94. |
[13] | Kamran SC , Berrington de Gonzalez A , Ng A , Haas-Kogan D , Viswanathan AN . Therapeutic radiation and the potential risk of second malignancies. Cancer. (2016) ;122: :1809–21. |
[14] | Brenner DJ , Curtis RE , Hall EJ , Ron E . Second malignancies in prostate carcinoma patients after radiotherapy compared with surgery. Cancer. (2000) ;88: :398–406. |
[15] | Berrington de Gonzalez A , Curtis RE , Kry SF ,et al., Proportion of second cancers attributable to radiotherapy treatment in adults: a cohort study in the US SEER cancer registries. Lancet Oncol. (2011) ;12: :353–60. |
[16] | Browne C , Davis NF , Mac Craith E , et al., A Narrative review on the pathophysiology and management for radiation cystitis. Adv Urol. (2015) ;2015: :346812. |
[17] | Brossard C , Lefranc AC , Simon JM , Benderitter M , Milliat F , Chapel A . Understanding molecular mechanisms and identifying key processes in chronic radiation cystitis. Int J Mol Sci. (2022) ;6: :23. |
[18] | Bostrom PJ , Soloway MS , Manoharan M , Ayyathurai R , Samavedi S . Bladder cancer after radiotherapy for prostate cancer: detailed analysis of pathological features and outcome after radical cystectomy. J Urol. (2008) ;179: :91–5; discussion 5. |
[19] | Krughoff K , Lhungay TP , Barqawi Z , O’Donnell C , Kamat A , Wilson S . The prognostic value of previous irradiation on survival of bladder cancer patients. Bladder Cancer. (2015) ;1: :171–9. |
[20] | Alam SM , Chollet-Hinton L , Thompson J , Holzbeierlein JM . Effect of prior radiation on stage, differentiation, and survival in bladder cancer. World J Urol. (2022) ;40: :719–25. |
[21] | von Elm E , Altman DG , Egger M , et al., The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) ;370: :1453–7. |
[22] | Kamat AM , Sylvester RJ , Bohle A , et al., Definitions, end points, and clinical trial designs for non-muscle-invasive bladder cancer: recommendations from the International Bladder Cancer Group. J Clin Oncol. (2016) ;34: :1935–44. |
[23] | Lyon TD , Faraj KS , Brennan E , Tyson MD 2nd , Boorjian SA , Spaulding AC . Defining radical cystectomy using the ICD-10 procedure coding system. Urol Oncol. (2022) ;165: :e17–e22. |
[24] | Fine JP , Gray RJ . A Proportional Hazards Model for the Subdistribution of a Competing Risk. J Am Stat Assoc. (1999) ;94: :496–509. |
[25] | Gray RJ . A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. Ann Stat. (1988) ;1141-54: :14. |
[26] | National Cancer Institute. Measures that are Limited or not Available in the Data. Div Cancer Control Popul Sci Healthc Deliv Res Progr n.d. https://healthcaredelivery.cancer.gov/seermedicare/considerations/measures.html#13. |
[27] | Yee DS , Shariat SF , Lowrance WT , et al., Impact of previous radiotherapy for prostate cancer on clinical outcomes of patients with bladder cancer. J Urol. (2010) ;183: :1751–6. |
[28] | Rao MV , Ellimoottil C , Sondej T , Flanigan RC , Quek ML . Intravesical Bacillus Calmette-Guerin immunotherapy after previous prostate radiotherapy for high-grade non-muscle-invasive bladder cancer. Urol Oncol. (2013) ;31: :857–61. |
[29] | Durant AM , Chang YH , Faraj KS , Tyson MD . BCG administration after prior radiation treatment for prostate cancer. Clin Genitourin Cancer. (2022) ;20: :591–7. |
[30] | Takam R , Bezak E , Yeoh EE . Risk of second primary cancer following prostate cancer radiotherapy: DVH analysis using the competitive risk model. Phys Med Biol. (2009) ;54: :611–25. |


