
Is There A Benefit of Restaging Transurethral Resection of Bladder Tumor Prior to Radical Cystectomy With or Without Neoadjuvant Chemotherapy?
Abstract
BACKGROUND:
One of the best predictors of positive outcomes in bladder cancer (BC) is pT0 following radical cystectomy (RC). Discordance between clinical and pathologic staging affects decision-making in patients with clinical absence of disease (cT0).
OBJECTIVES:
We sought to determine whether a restaging transurethral resection of bladder tumor (re-TURBT) improves clinical staging accuracy relative to pathologic stage RC in patients treated with neoadjuvant chemotherapy (NAC) versus those who did not receive NAC.
METHODS:
We queried our prospectively maintained IRB approved institutional database to identify 129 patients who underwent RC from 2013 to 2019 with a re-TURBT prior to RC. 53 patients were treated with NAC between their initial and re-TURBT and 76 patients were not treated with NAC.
RESULTS:
The overall upstaging rate from re-TURBT to RC was 34.9%. There was no significant difference in the upstaging rate between the NAC and no-NAC groups - 31.0% vs. 37.0%, respectively. In patients who were cT0 on re-TURBT, the NAC group did not show a significantly greater rate of pathologic clinical CR (pT0) than the no NAC group - 38.5% vs. 37.5%, respectively. Re-TURBT with staging < rT2 as a predictor for absence of MIBC on pathologic staging (<ypT2) did not show a significant difference between the NAC and no NAC group, with a negative predictive value (NPV) of 69.0% and 66.7%, respectively.
CONCLUSIONS:
Re-TURBT after NAC does not show statistically significant improvement in staging accuracy relative to pathologic stage at RC compared to re-TURBT in patients not treated with NAC.
INTRODUCTION
Bladder cancer (BC), the most common neoplasm of the urinary system, is the sixth most common cancer diagnosis and eighth most common cause of cancer mortality in the United States [1, 2]. For muscle-invasive bladder cancer (MIBC), NAC plus Radical Cystectomy (RC) is the gold standard of treatment [3]. NAC is associated with improved survival rates and clinical outcomes in MIBC and cisplatin-based NAC is recommended for all eligible patients prior to RC [4, 5].
One of the best predictors of positive clinical and survival outcomes in BC is pathologic complete response (pCR), or pT0, following RC [6, 7]. The landmark Southwest Oncology Group (SWOG) trial showed increase in pT0 staging in patients treated with NAC prior to RC compared to those who underwent RC alone and this was associated with significant improvement in overall survival compared to patients with residual disease [8].
Identifying the impact of NAC earlier in the clinical course of treatment for MIBC patients, such as prior to RC, remains a topic of interest [9]. Predicting pathologic stage prior to RC, however, is imperfect as transurethral resection of bladder tumor (TURBT), a commonly used procedure in endoscopically evaluating and treating BC prior to possible RC, has shown to be inaccurate [10–14]. Even as other tools including genomic and clinical testing are being utilized, the discordance between clinical to pathologic staging remains high at 20–80% [13, 14]. This limits the confidence with which bladder-sparing options can be recommended in patients with clinical absence of disease (cT0). A recent single-site study found that clinical absence of tumor on re-TURBT did not reliably predict pathologic absence of tumor, as pT0 was found in only 35.7% of patients who were clinically absent of disease (cT0) on re-TURBT [5].
There remains considerable variability regarding re-TURBT following completion of NAC prior to RC and the decision often varies based on institution or surgeon preference [9]. At our institution many of the patients undergo a re-TURBT following NAC administration.
Additionally, determining the role that documenting cT0, or clinical complete response, on re-TURBT following completion of NAC plays in clinical management and decision-making for these patients remains under investigation [15–18]. As research progresses in identifying appropriate candidates for bladder preservation, there has been an increased interest in determining whether a patient with a clinical complete response (cT0) to NAC can confidently opt for organ-preservation in MIBC. More specifically, understanding whether the current clinical staging, including re-TURBT, allow us to accurately determine the likelihood of presence or absence of residual bladder cancer with radical cystectomy.
Thus, we sought to determine whether there was a significant difference in staging accuracy from re-TURBT to pathologic staging in patients receiving a post-NAC re-TURBT versus those who underwent a re-TURBT prior to RC but did not receive NAC. We also observed clinical outcomes such as upstaging rates, bladder cancer recurrence, median survival, among other factors. We hypothesized that clinical staging post-NAC with re-TURBT may be sufficiently accurate compared to pathologic staging at cystectomy and therefore provide useful information either for planning surgery or for consideration of bladder sparing options. Our goal in comparing accuracy of re-TURBT to pathologic staging in NAC vs no-NAC groups was to determine whether in the post-NAC cohort, including those who are potentially candidates for bladder sparing options, re-TURBT staging exhibits a significantly higher rate of accuracy to pathologic staging.
METHODS
Inclusion Criteria
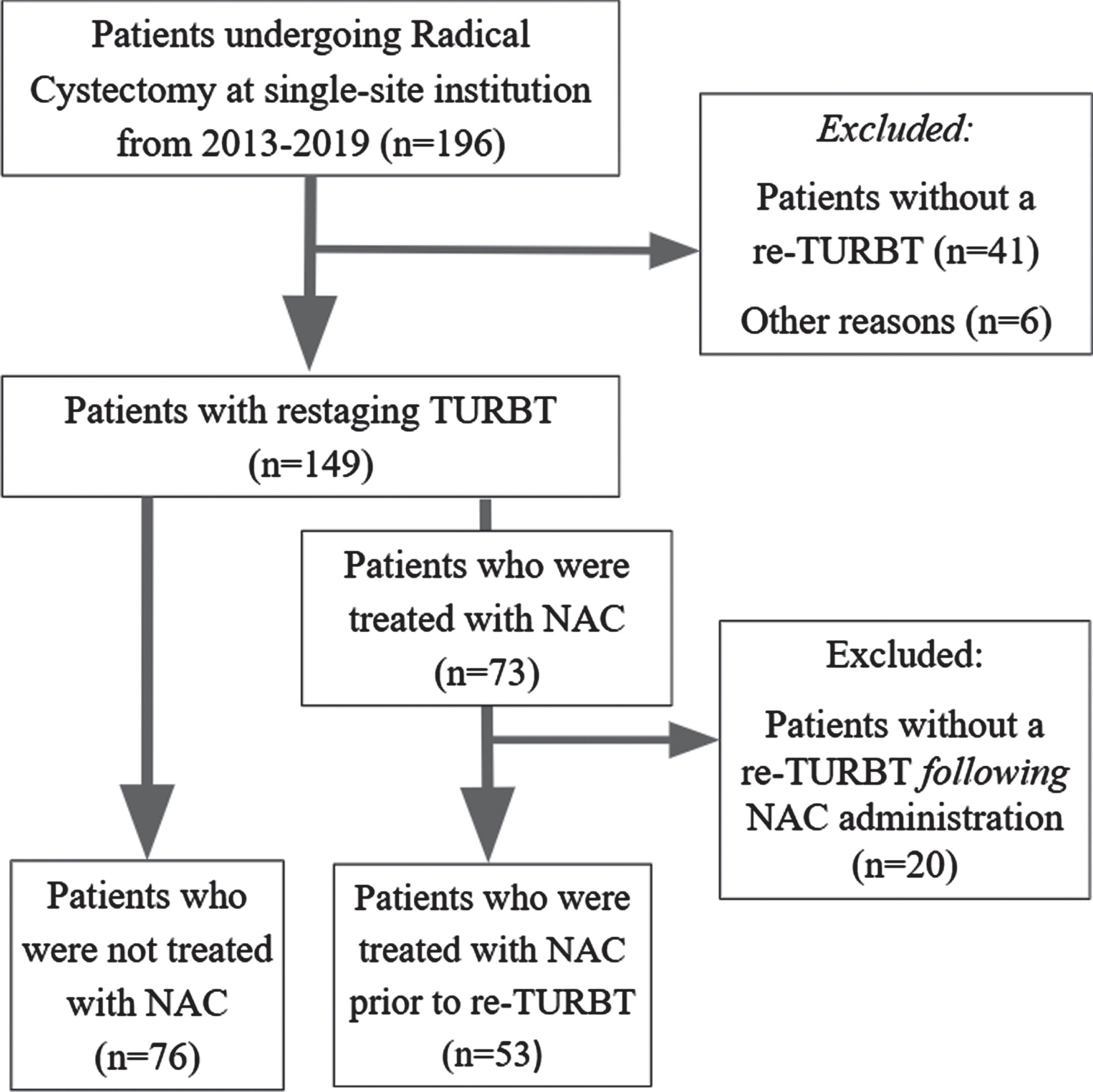
This retrospective cohort was curated from our prospectively maintained IRB approved institutional database (H-22878) to identify 196 patients who underwent a radical cystectomy from 2013 to 2019 at a single center. All patients signed an informed consent prior to enrollment in the database. Patients who had either not undergone a TURBT or only had one TURBT prior to RC were excluded. Patients treated with NAC who did not undergo a re-TURBT following NAC treatment were also excluded. Only those treated with NAC between their initial and re-TURBT were included to ensure uniform timeline of treatment. 53 patients were treated with NAC between their initial and re-TURBT and 76 patients were not treated with NAC. This resulted in 129 patients who underwent RC from 2013 to 2019 with a re-TURBT prior to RC (Fig. 1 Consort diagram). Exam under anesthesia (EUA) was performed routinely during TURBT and re-TURBT and used for clinical staging. If no residual disease was identified on cystoscopy, the prior resection bed was resected on re-TURBT as well as site directed biopsies to determine presence or absence of CIS. For our restaging specimens, 96 of 129 (74%) had explicit mention of presence of muscularis for pathologic evaluation, 16 (12%) did not, and 17 (13%) pathology reports were not able to be accessed on retrospective review for confirmation of presence of muscularis.
Fig. 1
Consort diagram of criteria for patient inclusion for both groups.
Outcome measures
The primary outcome of this study was the upstaging rate from re-TURBT to RC. Re-TURBT clinical staging was notated as rT and pathologic staging at RC was notated as ypT and pT, with and without NAC, respectively. We compared stratified upstaging rates from rT0/Ta/TisN0 and from rT1N0. Secondary outcomes included pathologic stage at RC for those with absence of residual disease (cT0N0) on re-TURBT, re-TURBT with staging < rT2 as a predictor for absence of MIBC on pathologic staging, and median time from RC to death from any cause stratified by treatment with or without NAC.
Statistical analysis
Statistical analyses were performed using R 3.6.2 (R Foundation For Statistical Computing, Vienna, Austria) for chi-square test and Fisher’s exact test for categorical variables. Statistical significance was set at p < 0.05.
RESULTS
The median age at RC for all patients was 69.5 years (IQR: 61.1–76.8). There was no significant difference in median age at RC, gender, or race between the two groups stratified by NAC status (Table 1). Complete initial, restaging, and pathologic tumor staging at RC data for the whole cohort is described in Table 2.
Table 1
Demographic data for all patients
| Parameter | All patients (n = 129) | NAC patients (n = 53) | No NAC patients (n = 76) | p-value |
| N, (%) | 129 (100) | 53 (41.1) | 76 (58.9) | – |
| Median age at RC, yr (IQR) | 69.5 (61.1–76.8) | 68.9 (61.1–75.3) | 69.6 (61.0–77.7) | 0.783 |
| Male, n (%) | 107 (82.9) | 43 (81.1) | 64 (84.2) | 0.647 |
| Race | – | – | – | – |
| White, n (%) | 121 (93.8) | 51 (96.2) | 70 (92.1) | 0.340 |
| Black, n (%) | 6 (4.7) | 2 (3.8) | 4 (5.3) | 0.693 |
| Other, n (%) | 2 (1.6) | 0 (0.0) | 2 (2.6) | 0.512 |
NAC = Neoadjuvant chemotherapy; RC = Radical Cystectomy.
Table 2
Staging data for all patients
| First TURBT clinical stage, n (%) | Re-staging TURBT clinical stage, n (%) | Pathologic tumor stage at RC, n (%) | |
| T0 | 0 (0.0) | 21 (16.3) | 14 (10.9) |
| Ta | 18 (14.0) | 18 (14.0) | 7 (5.4) |
| Tis | 8 (6.2) | 12 (9.3) | 24 (18.6) |
| T1 | 33 (25.6) | 32 (24.8) | 14 (10.9) |
| T2 | 49 (38.0) | 29 (22.5) | 18 (14.0) |
| T3 | 21 (16.3) | 15 (11.6) | 44 (34.1) |
| T4 | 0 (0.0) | 2 (1.6) | 8 (6.2) |
| Lymphovascular Invasion | 16 (12.4) | 11 (8.5) | 42 (32.6) |
| Median time from initial TURBT to re-TURBT, d (IQR) | 105 (47–163) | N/A | N/A |
| Median time from re-TURBT to RC, d (IQR) | N/A | 28 (14–55) | N/A |
IQR = interquartile range, TURBT = transurethral resection of bladder tumor.
Re-TURBT clinical staging was compared to pathologic staging for all patients as well as for the NAC and no-NAC groups, respectively (Fig. 2). The overall upstaging rate from re-TURBT to RC was 34.9% (n = 29). There was a significantly higher overall upstaging rate in the rT1N0 group at 53.1% (n = 17) versus the rT0/Ta/TisN0 group at 23.5% (n = 12) (p < 0.006). There was no significant difference found in the upstaging rate from re-TURBT to RC between the NAC and no-NAC groups, with 31.0% (n = 9) upstaged in the NAC group and 37.0% (n = 20) in the no-NAC group, respectively (p = 0.584) (Table 3). There was no significant difference found in upstaging rates between the NAC and no-NAC groups in the rT0/Ta/TisN0 (p = 0.739) and rT1N0 (p = 0.691) stratifications, respectively. Of note, 62.5% of patients who were cT1 on post-NAC re-TURBT were pT2 or greater (Fig. 2). Additionally, all patients who were cN+ on initial TURBT were found to be pT2 or greater following chemotherapy and re-TURBT (n = 7).
Fig. 2
Distribution of final re-TURBT stage (rT) vs final pathologic stage (ypT). (A) all patients undergoing re-TURBT prior to RC; (B) patients treated with NAC prior to RC; (C) patients who were not treated with NAC prior to RC. TURBT = transurethral resection of bladder tumor; RC = radical cystectomy; NAC = neoadjuvant chemotherapy.
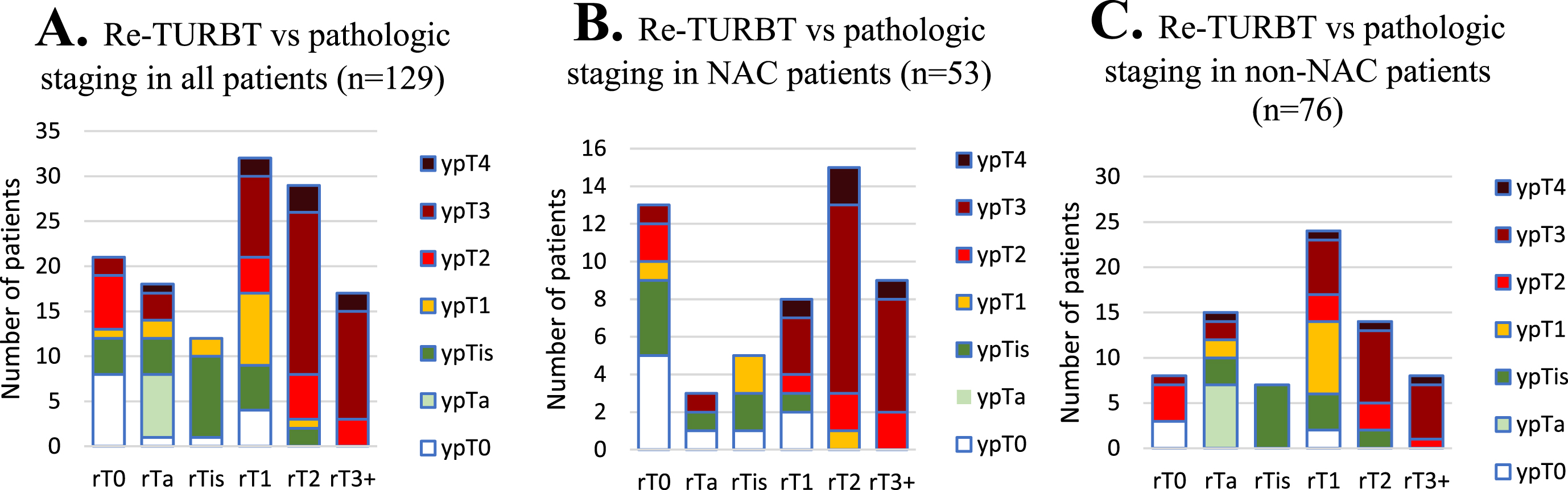
Table 3
Upstaging in total, NAC, and no NAC patients
| All patients n = 83 | NAC n = 29 | No NAC n = 54 | p-value | |
| Upstaged from re-TURBTa, n (%) | 29 (34.9) | 9 (31.0) | 20 (37.0) | 0.584 |
| All patients n = 51 | NAC n = 21 | No NAC n = 30 | ||
| Upstaged from rT0/Ta/TisN0a, n (%) | 12 (23.5) | 4 (19.0) | 8 (26.7) | 0.739 |
| All patients n = 32 | NAC n = 8 | No NAC n = 24 | ||
| Upstaged from rT1N0a, n (%) | 17 (53.1) | 5 (62.5) | 12 (50.0) | 0.691 |
a = Upstaging defined as clinical stage non-muscle invasive bladder cancer (NMIBC) on re-TURBT being pathologically staged as muscle-invasive bladder cancer (MIBC) or pTanyN+. NAC = neoadjuvant chemotherapy; TURBT = transurethral resection of bladder tumor.
In patients showing absence of residual disease (cT0) on re-TURBT (n = 21), there was no difference in pathologic absence of disease (pT0) between the NAC group (38.5%, n = 5) and non-NAC group (37.5 %, n = 3) (p = 1.00) (Fig. 2). Re-TURBT with staging < rT2 as a predictor for absence of MIBC on pathologic staging (<ypT2) did not show a significant difference between the NAC (n = 29) and no NAC (n = 54) group, with a negative predictive value (NPV) of 69.0% (n = 20) and 66.7% (n = 36), respectively (p = 0.831) (Table 4).
Table 4
Test performance characteristics of restaging TUR (≥rT2) in patients treated with NAC as a test for residual MIBC at cystectomy (≥ypT2)
| Patients treated with NAC | |||
| <ypT2 | ≥ypT2 | ||
| <rT2 | 20 | 9 | NPV: 20/29 = 69% |
| ≥rT2 | 1 | 23 | PPV: 23/24 = 96% |
| Specificity: 20/21 = 95% | Sensitivity:23/32 = 72% | ||
| Patients not treated with NAC | |||
| <ypT2 | ≥ypT2 | ||
| <rT2 | 36 | 18 | NPV: 36/54 = 67% |
| ≥rT2 | 2 | 20 | PPV: 20/22 = 91% |
| Specificity: 36/38 = 95% | Sensitivity: 20/38 = 53% | ||
MIBC = muscle-invasive bladder cancer; NAC = neoadjuvant chemotherapy; NPV = negative predictive value; PPV = positive predictive value; TUR = transurethral resection.
There was no significant difference found in recurrence of primary bladder cancer tumor at any time between the NAC and no NAC groups, with recurrence rates of 30.2% and 25.0%, respectively (p = 0.575). There was also no significant difference found in secondary primary tumor of the upper urinary tract or urethra (p = 0.143), overall death (p = 0.130), and death from bladder cancer rates (p = 0.602) between the NAC and no NAC groups. A subgroup analysis of pT0 patients showed no significant difference in recurrence rates, overall death, death from bladder cancer between the two groups (Table 5).
Table 5
Recurrence and mortality data for all patients
| Parameter | All patients (n = 129) | NAC patients (n = 53) | No NAC patients (n = 76) | p-value |
| Recurrencea, n (%) | 35 (27.1) | 16 (30.2) | 19 (25.0) | 0.575 |
| Secondary primary tumorb, n (%) | 4 (3.1) | 0 (0.0) | 4 (5.3) | 0.143 |
| Died, n (%) | 36 (27.9) | 11 (20.8) | 25 (32.9) | 0.130 |
| Died from bladder cancer, n (%) | 17 (13.2) | 6 (11.3) | 11 (14.5) | 0.602 |
| Median TTR, mo (IQR) | 8.0 (4.1–14.1) | 7.5 (3.8–9.8) | 8.7 (4.8–16.8) | 0.275 |
| Median follow-up for all patients, mo (IQR) | 19.2 (7.3–39.4) | 16.6 (7.3–31.6) | 23.9 (8.0–44.4) | 0.201 |
| pT0 patients | All patients (n = 14) | NAC patients (n = 9) | No NAC patients (n = 5) | p-value |
| Recurrencea, n (%) | 1 (7.1) | 1 (11.1) | 0 (0.0) | 1.00 |
| Died, n (%) | 1 (7.1) | 1 (11.1) | 0 (0.0 | 1.00 |
| Died from BC, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.00 |
a = Recurrence defined as presence or metastasis of primary bladder cancer tumor following radical cystectomy. b = Secondary primary tumors refer to malignancies of urinary tract following radical cystectomy. TTR = time to recurrence; IQR = interquartile range; NAC = neoadjuvant chemotherapy.
In patients who died from any cause, median time from RC to death was 8.4 months (IQR, 6.0–17.3) for the NAC group and 10.1 months for the no NAC group (IQR, 4.4–27.4). For the patients who died from bladder cancer, median time from RC to death was 8.1 months (IQR, 7.6–9.5) for the NAC group and 10.1 (IQR, 8.0–17.8) for the no NAC group.
DISCUSSION
We found that re-TURBT prior to RC with or without NAC is associated with similar rates of pathologic upstaging. Even when stratifying among patients clinically staged with NMIBC on re-TURBT, specifically rT0/rTis/rTaN0 and rT1N0, there was no significant difference found in upstaging rates between the NAC and no NAC groups. Additionally, clinical absence of disease (cT0) on re-TURBT was not an accurate predictor of pathologic absence of disease (pT0), with no significant difference found between the NAC and no NAC groups. We also found that a high percentage of patients who were cT1 on post-NAC re-TURBT possessed > pT2. All cN+ patients on initial TURBT were pT2 or greater at time of RC.
Our overall upstaging rate in our study sample was 34.9% (31.0% and 37.0% when stratified by NAC and no NAC, respectively), which falls within the reported rates in the literature on discordance from clinical to pathological staging in bladder cancer, reported as ranging from 20% to 80% [12–14].
Absence of disease on re-TURBT was a poor predictor of pathologic absence of disease. This finding is in line with the recent work of Kukreja et al. who found only 35.7% of patients who were cT0 on re-TURBT were pT0 on RC [5].
Re-TURBT clinical staging was a poor predictor of the presence of residual MIBC on RC in both patients who did and did not receive NAC. Becker et al. found a NPV of 62.7% in their post-NAC re-TURBT population [10], which is similar to our NPV of 69.0% in our post-NAC re-TURBT group. We also applied this model to our no NAC group and found a similar NPV of 67.0%.
Inaccuracy between clinical and pathological staging has long been one of the primary difficulties in bladder cancer treatment, with the utility of the post-NAC re-TURBT frequently debated. SWOG 0219 remains a cautionary tale in utilizing clinical staging as an indicator for absence of disease in a post-NAC population with 60% of patients presumed to be pT0 at time of cystectomy based on cT0 status post-NAC found to have persistent cancer [19].
Similarly, Becker and colleagues looked at whether re-TURBT after NAC reliably predicts response. In this population, 32% of patients were falsely downstaged when compared with pathological staging and 38% of patients < cT2 were > pT2, leading them to conclude that re-TURBT may indeed be a sub-optimal predictor of clinical response to NAC [10].
Most recently, Zibelman et al. studied whether NAC can affect TURBT versus pathologic stage accuracy utilizing prospective endoscopic tissue sampling immediately before cystectomy [11]. In the overall group, 51.6% of patients with no tumor on endoscopic sampling harbored residual invasive or non-muscle invasive disease at time of cystectomy. In a post-hoc subgroup analysis, the rate in the NAC patients was 43%. This study is particularly of note as it utilizes prospective analysis of endoscopic sampling to address the limits of retrospective analysis of discordance in clinical vs pathologic staging.
Important considerations in utilizing the information obtained from a post-NAC re-TURBT and clinical stage is determining the confidence with which active surveillance can be suggested to a post-NAC cT0 patient vs RC. More specifically, is there an added risk of mortality by deciding against RC due to a cT0 response that may not in fact be truly disease free? In a recent retrospective study of 148 patients who were cT0 following NAC for MIBC who elected active surveillance, 48% experienced a recurrence in the bladder, with 11 of the 15 bladder cancer deaths having local recurrence followed by metastasis [17]. Our findings that only a minority of patients found to be cT0 were found to be pT0 at time of radical cystectomy highlights the risk of electing for active surveillance in patients without residual disease on re-TURBT.
Another important recent study highlighting the challenge in utilizing post-NAC clinical staging as a driver of outcomes and response to NAC followed 32 patients with complete clinical response on a post-NAC TURBT, all of whom opted for active surveillance [18]. At 5-year follow-up, 17/32 had no recurrence of BC, thus they may have been overtreated had they proceeded with RC. However, with 7/15 undergoing salvage RC and 4/15 dying from bladder cancer and 3/15 alive but with metastatic disease, this may have been a missed opportunity for immediate RC. More investigation is needed to stratify those patients who are cT0 who can be safely monitored on active surveillance and those that require RC.
The limitations of clinical staging both pre- and post-NAC are well documented in the literature [5, 10, 11]. A large percentage of our patients who were cT1 or cT2 were upstaged at cystectomy to pT3 or greater. Cross sectional imaging with MRI may improve clinical staging. A recent study by Nechi et al utilized multiparametric MRI to assess response to neoadjuvant immunotherapy in patients with MIBC [20]. Using a three-step post-therapy MRI assessment sequence, radiologic complete response was found in 37 patients via internal assessment, of which 23 (62%) were found to be pT0. The Vesical-Imaging Reporting And Data System (VI-RADS) is a standardized MRI reporting system for bladder cancer [21]. Recent studies have validated the VI-RADS system for detection of muscle invasion and non-organ confined disease making it a useful tool for staging MIBC [22–25].
The limitations to our study include our retrospective design and single-site patient population, especially as clinical decision-making regarding whether to conduct a post-NAC re-TURBT may vary from institution to institution as well as patient selection for this treatment. As a single institution study, we are also limited by a small dataset which may be under-powered to detect differences between the NAC and no NAC groups. Furthermore, our dataset only dates back to 2013 which precludes any long-term follow-up greater than 9 years.
Another limitation of our study includes potential bias for patients that are selected for re-TURBT. Patients who undergo re-TURBT, versus those who do not, may have higher stage or multifocal disease, which may influence upstaging rates. For our NAC group, re-TURBT is done post-NAC as a result of an institutional workflow that involves a re-TURBT for all patients, including referrals from outside our institution, following NAC and prior to RC. For our patients that have not received NAC but go on to RC, we utilize a similar workflow in order to optimize clinical staging that informs treatment decision making. There may be a risk of bias if not all patients undergo re-TURBT. These limitations should be kept in mind and considered when interpreting our findings.
Additionally, further investigation into whether predictive factors exist predisposing to pT0 status and increased overall and disease-free survival should be undertaken.
CONCLUSION
Re-TURBT prior to RC with or without NAC was associated with similar rates of pathologic upstaging. While we have consistently found that one of the best predictors of positive clinical and survival outcomes is pT0 following RC, challenges remain regarding the accuracy of clinical staging with re-TURBT. All patients who were cN+ on initial TURBT had muscle invasive disease at time of cystectomy, which was independent of intensity/number of treatment cycles. A high rate of patients who were cT1 on post-NAC re-TURBT were found to have MIBC on pathologic staging. Clinical trials that are testing bladder preservation in such patients will require careful follow up in order to determine outcomes relative to the potential for residual bladder cancer and occult metastatic disease.
ACKNOWLEDGMENTS
The authors have no acknowledgments.
FUNDING
Partnership For Bladder Cancer, Scott Department of Urology, Baylor College of Medicine.
AUTHOR CONTRIBUTIONS
Conception (SPL); performance of work (JPM); or interpretation of data (JPM, JNB, SPL); writing the article (JPM, JNB, SPL).
All authors had access to the data.
CONFLICT OF INTEREST
SP Lerner –Clinical trials: Endo, FKD, JBL (SWOG), Genentech (SWOG), QED Therapeutics, UroGen, Vaxiion, Viventia. Consultant/Advisory Board: Aura Bioscience, BMS, C2iGenomics, Pfizer/EMD Serono, Protara, Stimit, UroGen, Vaxiion, Verity. Patent: TCGA classifier. Honoraria: Grand Rounds Urology, UroToday. SPL is co-Editor of this journal, but was not involved in the peer-review process nor had access to any information regarding its peer-review.
J Mehr and J Bates report no COI.
REFERENCES
[1] | Kaseb H , Aeddula NR Bladder Cancer, in StatPearls. 2022, StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.: Treasure Island (FL). |
[2] | Saginala K , et al., Epidemiology of Bladder Cancer.Med Sci (Basel). (2020) ;8: (1). |
[3] | Tyson MD , 2nd, Barocas DA , Quality of Life After Radical Cystectomy, Urol Clin North Am (2018) ;45: (2):249–56. |
[4] | Hamid A , et al., Meta-analysis of neoadjuvant chemotherapy compared to radical cystectomy alone in improving overall survival of muscle-invasive bladder cancer patients, BMC Urol (2020) ;20: (1):158. |
[5] | Kukreja JB , et al., Absence of Tumor on Repeat Transurethral Resection of Bladder Tumor Does Not Predict Final Pathologic T0 Stage in Bladder Cancer Treated with Radical Cystectomy, Eur Urol Focus (2018) ;4: (5):720–4. |
[6] | Kassouf W , et al., P0 stage at radical cystectomy for bladder cancer is associated with improved outcome independent of traditional clinical risk factors, Eur Urol (2007) ;52: (3):769–74. |
[7] | Tilki D , et al., Stage pT0 at radical cystectomy confers improved survival: an international study of 4,430 patients, J Urol (2010) ;184: (3):888–94. |
[8] | Grossman HB , et al., Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer, N Engl J Med (2003) ;349: (9):859–66. |
[9] | Chang E , et al., Refining neoadjuvant therapy clinical trial design for muscle-invasive bladder cancer before cystectomy: a joint US Food and Drug Administration and Bladder Cancer Advocacy Network workshoNature Reviews Urology (2022) ;19: (1):37–46. |
[10] | Becker REN , et al., Clinical Restaging and Tumor Sequencing are Inaccurate Indicators of Response to Neoadjuvant Chemotherapy for Muscle-invasive Bladder Cancer, Eur Urol (2021) ;79: (3):364–71. |
[11] | Zibelman M , et al., Cystoscopy and Systematic Bladder Tissue Sampling in Predicting pT0 Bladder Cancer: A Prospective Trial, J Urol (2021) ;205: (6):1605–11. |
[12] | Bayraktar Z , et al., Staging error in the bladder tumor: the correlation between stage of TUR and cystectomy, Int Urol Nephrol (2001) ;33: (4):627–9. |
[13] | Turker P , et al., Upstaging of urothelial cancer at the time of radical cystectomy: factors associated with upstaging and its effect on outcome, BJU Int (2012) ;110: (6):804–11. |
[14] | Ficarra V , et al., Correlation between clinical and pathological staging in a series of radical cystectomies for bladder carcinoma, BJU Int (2005) ;95: (6):786–90. |
[15] | Sternberg CN ,et al., Can patient selection for bladder preservation be based on response to chemotherapy? Cancer (2003) ;97: (7):1644–52. |
[16] | Robins D , et al., Outcomes Following Clinical Complete Response to Neoadjuvant Chemotherapy for Muscle-invasive Urothelial Carcinoma of the Bladder in Patients Refusing Radical Cystectomy, Urology (2018) ;111: :116–21. |
[17] | Mazza P , et al., Conservative Management Following Complete Clinical Response to Neoadjuvant Chemotherapy of Muscle Invasive Bladder Cancer: Contemporary Outcomes of a Multi-Institutional Cohort Study, J Urol (2018) ;200: (5):1005–13. |
[18] | Yap SA , et al., The Promise and Disappointment of Neoadjuvant Chemotherapy and Transurethral Resection for Muscle Invasive Bladder Cancer: Updated Results and Long-Term FollowuUrology Practice (2018) ;5: (4):6. |
[19] | deVere White RW , sequential treatment approach to myoinvasive urothelial cancer: a phase II Southwest Oncology Group trial (S0219). J Urol. (2009) ;181: (6):2476–80discussion 2480-1. |
[20] | Necchi A , et al., Multiparametric Magnetic Resonance Imaging as a Noninvasive Assessment of Tumor Response to Neoadjuvant Pembrolizumab in Muscle-invasive Bladder Cancer: Preliminary Findings from the PURE-01 Study, Eur Urol (2020) ;77: (5):636–43. |
[21] | Panebianco V , et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System), Eur Urol (2018) ;74: (3):294–306. |
[22] | Luo C , et al., Use of Vesical Imaging-Reporting and Data System (VI-RADS) for detecting the muscle invasion of bladder cancer: a diagnostic meta-analysis, Eur Radiol (2020) ;30: (8):4606–14. |
[23] | Panebianco V , et al., VI-RADS for Bladder Cancer: Current Applications and Future Developments, Journal of Magnetic Resonance Imaging (2022) ;55: (1):23–36. |
[24] | Wang H , et al., Multiparametric MRI for Bladder Cancer: Validation of VI-RADS for the Detection of Detrusor Muscle Invasion, Radiology (2019) ;291: (3):668–74. |
[25] | Kim SH , Validation of vesical imaging reporting and data system for assessing muscle invasion in bladder tumor, Abdom Radiol (NY) (2020) ;45: (2):491–8. |


