
Economic Outcomes of Hexaminolevulinate Blue-Light Cystoscopy in Non-Muscle Invasive Bladder Cancer: A 5-Year, Medicare-Based Model
Abstract
BACKGROUND:
Bladder cancer is the most expensive cancer to treat on a per-patient basis. Blue light cystoscopy with hexaminolevulinate (BLC) has demonstrated improved diagnostic accuracy compared with white light cystoscopy (WLC) in non-muscle invasive bladder cancer (NMIBC). With higher upfront costs, questions remain about long-term BLC cost outcomes.
OBJECTIVE:
This study seeks to investigate the 5-year cost comparison of BLC and WLC from the Medicare payer perspective.
METHODS:
A representative 5-year NMIBC management model was constructed and Medicare reimbursement values were overlaid. The primary outcome was mean year-over-year cumulative cost discounted to present value at a 3% annual percentage rate. The secondary outcome was the rate of clinical events.
RESULTS:
Patients in the BLC cohort experienced fewer recurrences. On a cumulative present value cost basis, BLC was more expensive per patient in years 1, 2, and 3 than WLC, however, in years 4 and 5, BLC was economically favorable. Year 5 BLC mean cumulative cost savings was $1,172 per patient. Overall, 31.6% of all patients in the BLC group generated cumulative cost savings compared to WLC at year 1 compared with 50.9% at the end of year 5.
CONCLUSIONS:
Despite a higher initial annual cost, a slight cumulative economic advantage of BLC is realized after surveillance year 3. Additionally, a greater proportion of patients who received BLC achieved cost savings at the end of year 5. As novel technology emerges, economic models can help health care systems predict associated costs and quality improvements.
INTRODUCTION
Non-muscle invasive bladder cancer (NMIBC) has an annual estimated incidence of nearly 60,000 in the United States [1, 2]. Due to high rates of recurrence and resultant healthcare utilization, bladder cancer is the most expensive cancer to treat on a per-patient basis [3]. Transurethral resection of bladder tumor (TURBT) is the foundation of initial management. Historically, TURBT has been performed with white light cystoscopy (WLC), however, several meta-analyses have since validated early clinical trials, which demonstrated that adding blue light cystoscopy with hexaminolevulinate (BLC) confers improved diagnostic sensitivity and lower recurrence rates compared with WLC [4–9]. The American Urologic Association (AUA)/Society of Urologic Oncology (SUO) guidelines offer a grade B recommendation for TURBT with BLC [10].
The high cost of bladder cancer care and clinical advantages of BLC over WLC have prompted further investigation of the economic outcomes of BLC with results showing cost- superiority, parity, or inferiority using varying costing methodologies [11–15]. Given the promising role of BLC in NMIBC coupled with expanding healthcare costs in the United States, there is a call for additional data on BLC cost outcomes [16]. This study seeks to model the AUA/SUO bladder cancer guidelines by running a Monte Carlo simulation to investigate the 5-year cost comparison of BLC and WLC from the payer perspective. Despite the higher upfront cost, we hypothesized that the clinical advantages of BLC result in cost-parity after 5 years.
MATERIALS AND METHODS
Decision tree and assumptions
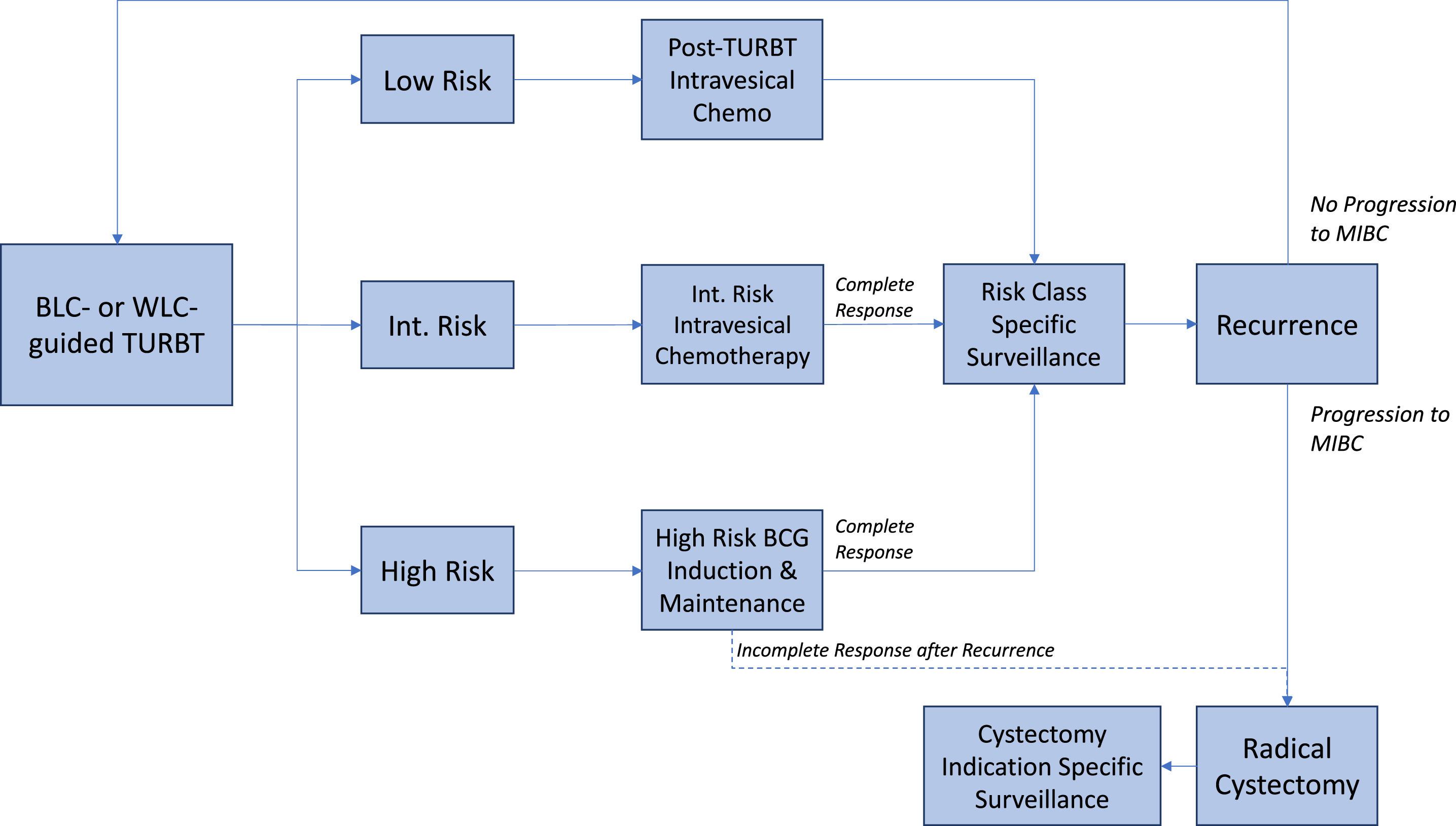
A model was created in Microsoft Excel (Version 16.53, Microsoft; Redmond, WA) with @RISK (Version 8.1, Palisade; Ithaca, NY), a decision analysis software add-in. The clinical decision tree was based on the 2020 AUA/SUO bladder cancer guidelines [10]. Patients were randomized to one of two cohorts—BLC- or WLC-based TURBT—for the duration of the five-year simulation. Following initial TURBT, patients underwent risk-class-specific treatment and surveillance. Immediately following TURBT, low-risk patients underwent perioperative intravesical chemotherapy. Intermediate-risk patients were modeled to receive six instillations of intravesical chemotherapy after TURBT. Patients with high-risk NMBIC underwent induction followed by maintenance BCG. In patients with recurrence, the tumor was removed via TURBT. Based on pathology, patients either remained in the same risk group or advanced to a higher risk group; the model did not allow for downgrading. For the purposes of this model, patients with progression to MIBC or high-risk recurrent NMIBC that is unresponsive to BCG were managed with RC. Following RC, patients underwent indication-specific surveillance per guidelines [17]. Variant histology, re-resection TURBT, salvage intravesical chemotherapy for BCG-unresponsive disease, bladder-preserving trimodality therapy, metastases, palliative care, death, and partial cystectomy were not included in the model. See Fig. 1 for a representative diagram.
Fig. 1
A representative clinical decision diagram. BLC = Blue light cystoscopy with hexaminolevulinate; WLC = White light cystoscopy; TURBT = Transurethral resection of bladder tumor; Chemo = Chemotherapy; Int. = Intermediate; BCG = Bacillus Calmette-Guerin; MIBC = Muscle-invasive bladder cancer.
Model inputs and simulation
Inputs for NMIBC incidence and recurrence for BLC and WLC are reported in Table 1 and are based on Burger et al. 2013 and Klaasen et al. 2017 [6, 12]. The proportion of patients in the low, intermediate, and high-risk NMIBC groups were informed by literature at 70%,20%,and 10%,respectively [18, 19]. The relative risk reduction of recurrence between BLC and WLC was individualized to each risk group based on a meta-analysis of raw data [6]. The risk of progression was equal between WLC and BLC and assumed to be cumulative at 4.2% per year [20, 21]. Fifty percent of high-risk NMIBC patients with recurrent disease were modeled as non-responders to intravesical BCG and managed with RC [22–25]. The study relied on inputs sourced from previously published data and did not include individual patient data and thus was IRB exempt.
Table 1
Economic and Clinical Model Inputs
| Economic Model Inputs Medicare 2021 National Average | Code(s) | Professional | Facility | HCPCS | Total Cost |
| White Light Cystoscopy TURBT | 52235 | $ 306 | $ 3,076 | $ 3,383 | |
| Blue Light Cystoscopy TURBT | 52235, A9589 | $ 306 | $ 3,076 | $ 1,205 | $ 4,588 |
| Cystectomy | 51590, DRG655 | $ 2,063 | $ 13,261 | $ 15,324 | |
| Neoadjuvant MVAC×6 cycles | 96413, J9260, J9360, J9000, J9070 | $ 890 | $ 1,865 | $ 345 | $ 3,099 |
| Gemcitabine Instillation (x 1 2000 mg dose)* | 51720, J9201 | $ 97 | $ 40 | $ 137 | |
| Bacillus Calmette-Guerin Instillation (x 1 50 mg dose) | 51720, J9030 | $ 97 | $ 143 | $ 240 | |
| Cystoscopy (surveilance) | 52000 | $ 260 | $ 575 | $ 835 | |
| Upper tract Imaging (CT) | 74176 | $ 152 | $ 230 | $ 382 | |
| Abd/Pelvic Imaging (CT) | 74176 | $ 152 | $ 230 | $ 382 | |
| CT Urogram (CTU) | 74178 | $ 257 | $ 368 | $ 625 | |
| CT Chest (CT) | 72192 | $ 106 | $ 109 | $ 215 | |
| Physician Visit (new) | 99204 | $ 180 | $ 180 | ||
| Physician Visit (established) | 99214 | $ 139 | $ 139 | ||
| Urine Cytology | 88112 | $ 51 | $ 51 | ||
| Basic Metabolic Panel | 80048 | $ 8 | $ 8 | ||
| Liver Function Tests | 80076 | $ 8 | $ 8 | ||
| Complete Blood Count | 85027 | $ 6 | $ 6 | ||
| Serum Vitamin B12 | 82607 | $ 15 | $ 15 | ||
| Clinical Model Inputs | Input | ||||
| Low Risk NMIBC Prevelance | 0.700 | ||||
| Year 1 Low Risk Recurrence Risk | 0.150 | ||||
| Year 2 Low Risk Recurrence Risk | 0.100 | ||||
| Year 3 Low Risk Recurrence Risk | 0.050 | ||||
| Year 4 Low Risk Recurrence Risk | 0.080 | ||||
| Year 5 Low Risk Recurrence Risk | 0.070 | ||||
| Int Risk NMIBC Prevelance | 0.200 | ||||
| Year 1 Int Risk Recurrence Risk | 0.260 | ||||
| Year 2 Int Risk Recurrence Risk | 0.130 | ||||
| Year 3 Int Risk Recurrence Risk | 0.060 | ||||
| Year 4 Int Risk Recurrence Risk | 0.050 | ||||
| Year 5 Int Risk Recurrence Risk | 0.030 | ||||
| High Risk NMIBC Prevelance | 0.100 | ||||
| Year 1 High Risk Recurrence Risk | 0.390 | ||||
| Year 2 High Risk Recurrence Risk | 0.110 | ||||
| Year 3 High Risk Recurrence Risk | 0.060 | ||||
| Year 4 High Risk Recurrence Risk | 0.020 | ||||
| Year 5 High Risk Recurrence Risk | 0.030 | ||||
| BLC Recurrence Relative Risk Reduction Low Risk | 0.561 | ||||
| BLC Recurrence Relative Risk Reduction Int Risk | 0.836 | ||||
| BLC Recurrence Relative Risk Reduction High Risk | 0.752 | ||||
| Annual Risk of Progression All Risk Groups | 0.042 |
HCPCS = Healthcare Common Procedure Coding System; TURBT = Transurethral resection of bladder tumor; MVAC = Methotrexate, Vinblastine sulfate, Doxorubicin hydrochloride (Adriamycin), and Cisplatin; Abd = Abdomen; Int = Intermediate. *Professional bundled if immediately after TURBT.
The model was conducted from the perspective of the health care system and analyzed reimbursement. Economic inputs were sourced from 2021 Medicare reimbursement averages with a 10% of mean standard deviation to simulate geographic variability [26]. The model was simulated to 60,000 iterations to approximate the incidence of NMBIC in the United States.
Sensitivity analysis was performed to investigate the effect of recurrence and progression on cost outcomes. BLC recurrence and progression rates were varied while WLC variables were held constant. The outcome of interest was present value cumulative costs at year 5 for blue-light vs. white-light cystoscopy cohorts. To conduct a sensitivity analysis, additional simulations were performed with BLC recurrence rates that were improved and worsened relative to the baseline expected rate by 20% and BLC progression rates that were improved and worsened relative to the baseline expected rate by 35%. The baseline expected rates for recurrence and progression are reported in Table 1.
Economic and clinical outputs
Economic outcomes included mean year-over-year cost per patient, cumulative cost at years 2, 3, 4, and 5, and the percent of patients with present value cumulative savings comparing WLC and BLC. Cost savings were reported as the absolute difference between treatment modalities. All economic outcomes were reported in USD, discounted at a 3% annual percentage rate (APR).
Clinical outcomes were analyzed by year and included the number of recurrences, the number of patients requiring RC for progression from NMIBC to MIBC or BCG unresponsive patients. In addition, the percent of patients who had at least one recurrence and the percent of patients who underwent RC during the modeled period were reported.
Statistical methods
All data were modeled for 5 years from NMIBC diagnosis. Summary statistics for each cohort are reported as percent of cohort, proportion of cohort, or cohort means, and analyzed per year. Economic data is presented annually and cumulative. For continuouseconomic variables, the difference of cohort means is reported.
RESULTS
Clinical results
The overall cystectomy rate for the BLC group was 13.9% and 13.9% in the WLC group. The percent of patients in each cohort with at least one recurrence during the 5-year model, were as follows: 63.8% BLC; 79.4% WLC. Each patient in the WLC cohort experienced a mean of 1.36 recurrences during the 5-year simulation whereas the BLC cohort experienced 1.07 (Table 2).
Table 2
Clinical Outcomes Through Model Year 5
| Outcomes through Year 5 | WLC | BLC |
| Patients with 1+ Recurrence | 79.4% | 63.8% |
| Mean Recurrence per Patient | 1.36 | 1.07 |
| Patient with all cause Cystectomy | 13.9% | 13.9% |
BLC = Blue light cystoscopy with hexaminolevulinate; WLC = White light cystoscopy.
Economic results
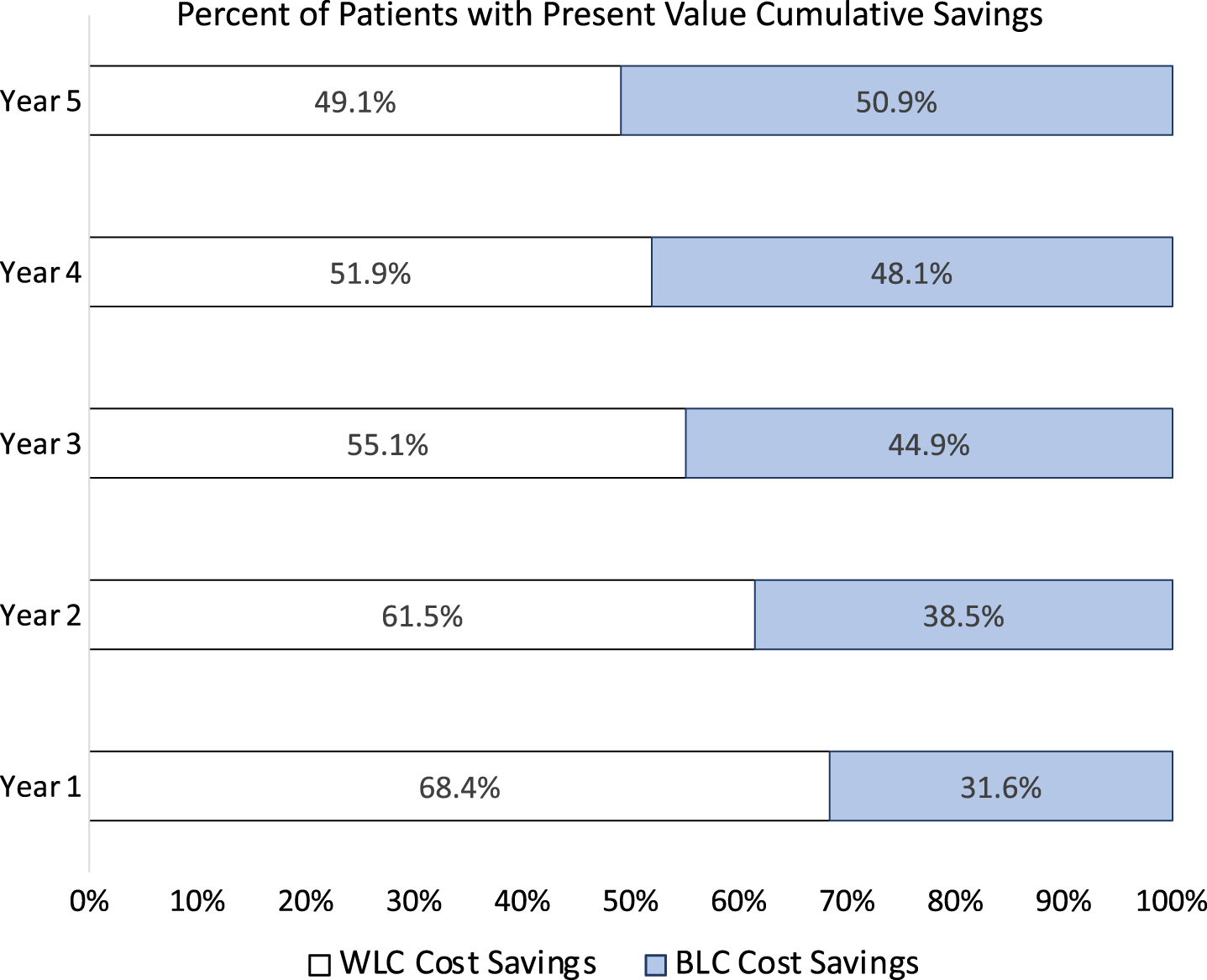
On a year-by-year analysis, costs were front-loaded with year 1 costs of $10,498 for BLC and $9,446 for WLC. BLC had a consistent yearly cost advantage over WLC in years 2 through 5 (Fig. 2A). In terms of cumulative cost, BLC was more expensive than WLC in years 1,2 and 3. In years 4 and 5, BLC was more cost-effective than WLC. For years 1 and 2, the cumulative cost for WLC was $9,446 and $13,891 respectively. This was in comparison to BLC, which had cumulative costs of $10,498 and $14,551, respectively. At year 3, there was relative parity between BLC and WLC cumulative costs at $18,758 and $18,716 respectively. Year 4 cumulative costs for BLC was $23,146 while WLC was $23,675. Finally, Year 5 costs for WLC was $28,788 and for BLC was $27,616 (Fig. 2B). On a descending proportion plot for cumulative costs at year 5, BLC demonstrates a higher proportion of patients with lower costs compared with WLC (Fig. 2C). Overall, 31.6% of all patients in the BLC cohort generated cumulative cost savings compared to WLC at year 1. However, 50.9% had cumulative cost savings compared with BLC at the end of year 5 (Fig. 3).
Fig. 2
Economic Outcomes. A. Year-over-year average cost per patient of blue-light and white-light guided transurethral resection of bladder tumor. B. Cumulative average cost per patient by year. C. Descending proportion plot of cumulative costs at year 5 for blue-light and white-light cystoscopy cohorts. Blue graphics represent the blue-light cystoscopy cohort and light grey graphics represent the white-light cystoscopy cohort. All values in United States Dollars discounted to present value at 3% annual percentage rate. Blue values represent BLC, grey values represent WLC.
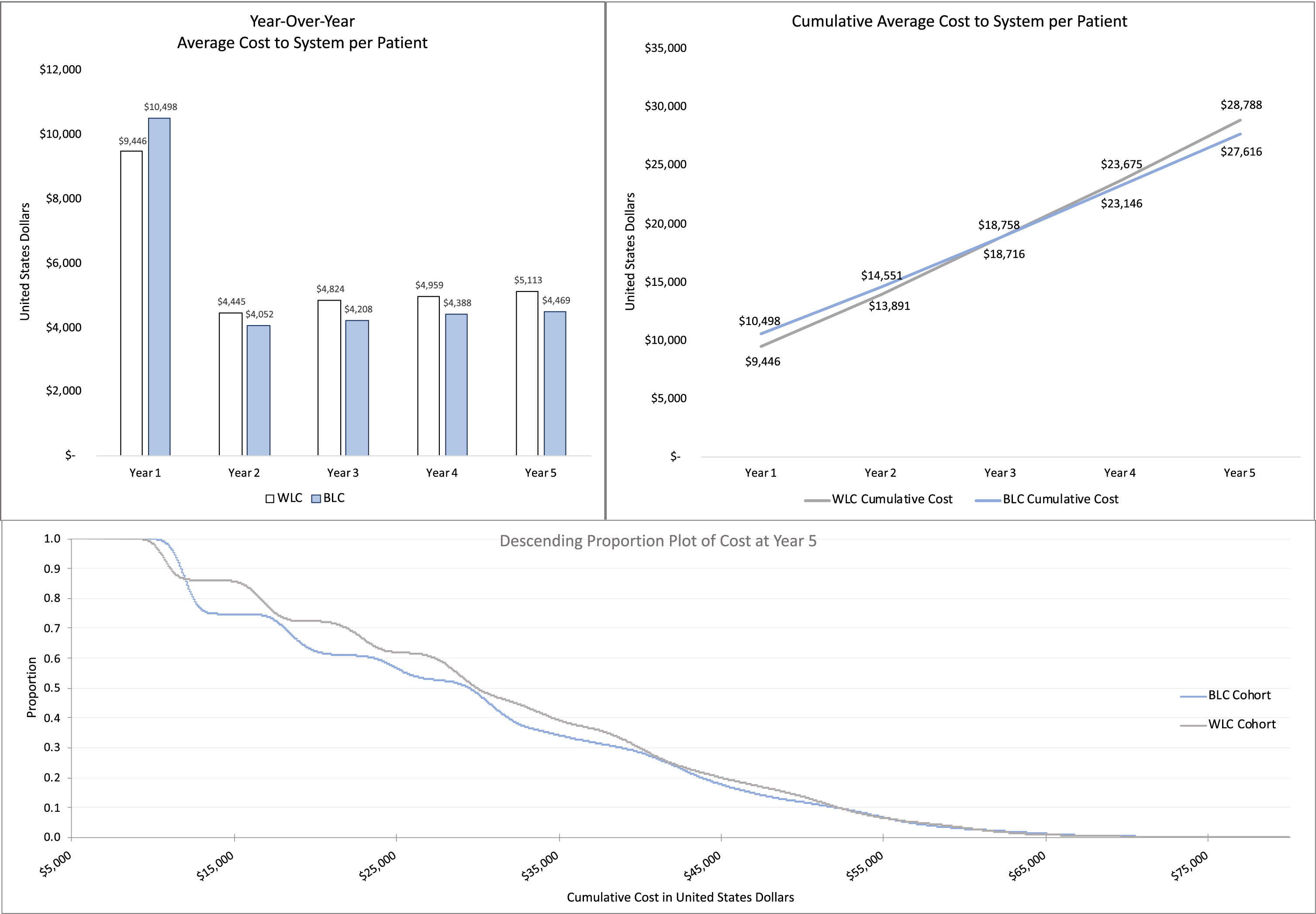
Fig. 3
Percent Patient Savings. The percentage of patients (WLC versus BLC cohorts) with cumulative savings. All value discounted to 2021 present-day United States Dollars at 3% APR. BLC = Blue light cystoscopy with hexaminolevulinate; WLC = White light cystoscopy.
On sensitivity analysis, improved progression rates and recurrence rates of BLC relative to WLC resulted in an increase cumulative cost savings at the end of year 5. Holding BLC recurrence rates constant at the expected value, a 35% improvement in progression rates resulted year 5 cost savings of $1,404 whereas when progression rates were 35% worsened, cost savings were $1,018. With BLC progression rates held constant, a 20% improvement in recurrence rates resulted in year 5 BLC cost savings of $2,892 compared to (-$767) with 20% worsened recurrence rates (Table 3).
Table 3
Sensitivity Analysis
| BLC Recurrence | BLC Progression | ||
| Improved | Expected | Worsened | |
| Improved | $ 3,136 | $ 2,892 | $ 2,709 |
| Expected | $ 1,404 | $ 1,172 | $ 1,018 |
| Worsened | $ (393) | $ (767) | $ (1,071) |
Difference in present value cumulative costs at year 5 for blue-light vs. white-light cystoscopy cohorts. Costs differences are from the perspective of BLC; positive numbers favor BLC, negative numbers favor WLC. BLC= Blue light cystoscopy.
DISCUSSION
This study investigates a potential cost advantage for BLC compared to WLC-guided TURBT in patients with NMIBC. Previous literature has demonstrated an improvement in recurrence rates with BLC compared to WLC, thought to be due to improved tumor detection resulting in more complete resections [4–6]. In this case, we constructed an economic model using the AUA/SUO guidelines that approximates real-world patient outcomes, assigned Medicare reimbursement data, and conducted a Monte-Carlo simulation.
The present simulation demonstrated 79.4% and 63.8% 5-year recurrence rates in the WLC and BLC cohorts, respectively. In a study by Sylvester et al., a prediction model based on analysis of outcomes from 2,596 patients who received a range of post-TUR treatments demonstrated a 5-year recurrence rate ranging from 31% to 78% [19]. Similarly, Daniltchenkio et al. observed a 75% and 59% 5-year recurrence rate with WLC and BLC, respectively [27]. In this model, five-year progression rates were 12.7% and 12.9% in patients treated with WLC versus BLC, respectively. These rates fall within the range of the Sylvester prediction model, in which the progression rate ranged from 1 to 45% [19]. A separate study reporting all-cause cystectomy rates by claims data determined that patients managed with WLC versus BLC had comparable cystectomy rates of 15.3% and 14.1%,respectively [14]. The 5-year modeled relative risk of recurrence for BLC vs WLC was 0.782, similar to a previous meta-analysis [6]. Overall, the resultant absolute recurrence and progression rates of the model are comparable to the upper limit of rates described in the literature. These outcomes may result from perfect surveillance as this model did not account for patients lost to follow-up or incomplete treatment. Importantly, the relative number of recurrences with WLC and BLC closely approximates real-life data [6].
Our analysis showed that, at year 5, BLC mean cumulative present value cost savings compared to WLC was $1,172 per patient. Additionally, on patient-level analysis at year 5, 50.9% of BLC patients demonstrated cumulative cost savings relative to WLC. There is a lack of agreement in the literature as to when, or if, BLC becomes cost-effective resulting from a difference in methods, perspectives, and assumptions [11–15].
Our finding corroborates that BLC has a modest long-term cumulative cost advantage over WLC. Garfield et al. conducted an analysis that compared BLC versus WLC-based TURBT in patients with NMIBC. Using a 5-year, cohort level, probabilistic decision-tree, BLC resulted in lower cumulative costs at year 5 compared with WLC from the Medicare perspective (BLC: $25,921 USD, WLC: $30,581 USD). This study also reported increased patient utility scores, (BLC: 4.9, WLC: 4.4). Higher patient utility and improved cost outcome suggest that BLC is a dominant treatment choice compared to WLC [11]. However, this model used best-case scenarios and clinical inputs based on a single phase III trial which could overestimate the advantage of BLC. Also, it is unclear how BLC fared in years 1 to 4 as year-over-year costs were not reported. Cumulative BLC savings of $4,660 USD are roughly in line with our findings of $1,172 per patient at year 5. However, as this study was conducted in 2013, these outcomes do not account for inflation or changes in reimbursement.
Another analysis has shown that BLC is cost-neutral to WLC. In a 5-year Swedish cost-consequence model from the perspective of the hospital system, year-over-year cost comparisons showed the BLC was more expensive in year 1 versus WLC. BLC was less expensive than WLC in years 2 to 5 [13]. At year 5, BLC was found to be cost-neutral compared to WLC (BLC: 14,033,864 SEK, WLC: 13,815,155 SEK; 10 SEK = $1.28 USD) on a discounted cumulative cost basis [13]. When re-running the model with only low-risk patients, BLC incurred 11.9% higher costs compared with WLC suggesting BLC is best suited for patients in higher risk groups. In separate subanalyses of intermediate and high-risk patients, cost improvement was identified with BLC incurring 1.7% and 1.2% higher costs, respectively [13]. The Dansk et al. model assumed that 15%,45%,and 40% of the cohort were low, intermediate, and high-risk patients which, on the whole, is a higher risk cohort than what is reported in literature [18, 19]. Both this analysis and our study used results from Burger et al. to inform diagnostic test performance [6]. However, in our case, we sub-stratified BLC relative risk reduction of recurrence based on risk-group whereas, in the Dansk et al. model, performance was equal across risk-groups. This study and ours support that costs are front-loaded, and BLC appears to generate cumulative costs savings over time. However, Dansk et al. found that BLC was cost-neutral to WLC, likely because it assumed the perspective of the hospital and capital expenditures wereanalyzed.
Klassen et al. conducted a 5-year cost-consequence model comparing BLC and WLC in NMIBC patients through the lens of payers in three Canadian provinces (British Columbia, Ontario, and Quebec). This study showed that BLC is more expensive on a cumulative, five-year basis. The analysis was unique as it included net differences in estimated staffing, medication, and capital expenditures. Clinical model inputs were sourced from a meta-analysis conducted by the authors and from Burger et al. [6, 12]. The authors analyzed Ontario in greater detail and found that BLC was more expensive than WLC at 5 years with a cost-difference per case of $1,181 CAD ($1.00 CAD = $0.77 USD). The cost per one recurrence prevented ranged from $19,354 to $28,463 CAD depending on the provincial payer [12]. However, these results were derived from a universal healthcare system and may not be generalizable to the United States.
On sensitivity analysis, recurrence rate was found to be a stronger driver of cost than rate of progression. In contrast, Klassen et al. found that recurrence was a moderate driver of cost while progression was a stronger cost-driver. This most likely resulted from a difference in model inputs. For Klassen et al the largest expense was palliative care which all patients with metastases received ($55,215 CAD), however, costs related to palliative care were not included in the present economic analysis. In patients who are post-cystectomy, metastasis is reported in up to 50% of patients, in which case altering progression rates would significantly influence economic outcomes when considering palliative care costs [28].
Despite AUA/SUO guideline support, blue light cystoscopy remains underutilized in the United States and its widespread adoption has stagnated [29]. This trend is exaggerated in community practice, where the majority of urology care occurs, compared with academic medical centers [29]. Upfront equipment costs are thought to represent a significant barrier to adoption of blue light cystoscopy with the cost of a blue light cystoscopy compatible endoscopy system reported at approximately $150,000, although BLC implementation costs can vary based on several factors including existing equipment, existing staff experience, vendor relationships, differing cost structures (outright equipment purchase vs lease), and purchasing power [30]. Given our analysis, the cost savings of BLC would break even the above-mentioned equipment expenditure after treating 128 patients for 5 years. However, in a fee-for-service reimbursement system, these cost-savings could actually dissuade medical centers from investing in blue light capable endoscopy equipment, further stymieing adoption of guideline-based care. While there is internal data from industry suggesting a halo effect of new patients seeking care at centers who adopt blue light cystoscopy, this effect is apropos to an individual center rather than the healthcare system as a whole [31].
The strength of the present study is its complexity and detail. This is the first study to report the percent of a cohort with cumulative cost-savings comparing BLC and WLC. This study also stratified relative risk reduction of recurrence from BLC compared to WLC by NMIBC risk group rather than applying the same model inputs to low, intermediate, and high-risk groups. While previous studies have modeled cystectomies in patients with progression to MIBC, this model also accounts for NMIBC in patients with BCG unresponsive disease which is informed by contemporary trials [24, 25]. The costs that were included in this analysis were also a source of strength. Professional, facility, and HCPCS fees were included in the analysis to more fully account for costs associated with NMIBC.
This study should also be considered in the context of its limitations. Costs were analyzed from the perspective of Medicare, thus capital expenditures, staffing differences, and implementation costs were not analyzed. This study did not include hospice or patient death as a potential outcome, but because BLC does not confer improved survival relative to WLC, this omission is unlikely to affect the conclusions and follows the with-without economic valuation principle [32]. This model assumes optimal intravesical treatment, however, data for recurrence and progression was sourced from Burger et al. which did not report intravesical treatment rates in aggregate. This model therefore assumes the benefits of BLC are maintained in patients who underwent intravesical treatment which may bias the economic outcomes. Furthermore, the source data used to construct this model such as Klaasen et al. and several randomized trials included in the Burger et al. meta-analysis used BCG for intermediate and high-risk NMBIC [6, 12]. However, the current treatment landscape recommends intravesical chemotherapy for intermediate risk disease and thus we modeled the cost of intravesical therapy for intermediate-risk patients based on intravesical chemotherapy rather than BCG. This model also does not allow for a patient to cross over from BLC and WLC. Other forms of enhanced cystoscopy such as narrow-band imaging, flexible BLC, and alternative treatment scenarios (i.e. trimodality therapy for MIBC patients, salvage intravesical chemotherapy for BCG-unresponsive patients, in-office fulgurations etc.) were not included as this would have further complicated the model, but could certainly play a role in overall outcomes and treatment costs. Finally, this study did not model patient-centric outcomes such as quality-adjusted life years (QALYs). Although, a reduction in disease recurrence has been previously modeled to correlate with improved patient-reported utility outcomes [11].
High-value care is an increasingly critical component in the management of patients with urologic diseases. This study is timely as the last Medicare-based model was conducted nearly a decade ago [11]. The number of Medicare beneficiaries is increasing relative to other insurance payer segments and yet Medicare reimbursements for urologists are declining when compared to inflation-adjusted values [33]. Further, with the passage of Medicare Access and CHIP Reauthorization Action (MACRA) into law in 2016, the adoption of alternative payment models (APMs) and merit-based incentive payment system (MIPS) will lead to payment adjustments to incentivize value-based, cost-conscious care [34]. In this study, BLC was shown to offer lower cumulative cost and lower overall recurrences at year 5. Future studies should seek real-world data to confirm concordance between modeled and practice data. With continued analysis of economic outcomes, we can inform more cost-effective care for our patients, healthcare systems, and payers alike.
In this Medicare-based model, BLC is associated with a cumulative $1,172 cost savings per patient over WLC for management of NMIBC at year 5. Despite the higher initial annual cost, the cumulative economic advantage of BLC is realized after year 3. Additionally, compared with WLC, a greater proportion of patients who received BLC achieved cost savings at year 5. Economic simulations represent an important framework through which clinical practice can be evaluated to inform cost-effective care. Targeted analysis and investment into cost-effective care are needed to improve clinical and economic outcomes for patients and the healthcare system as a whole.
ACKNOWLEDGMENTS
The authors have no acknowledgments.
FUNDING
The authors report no funding.
AUTHOR CONTRIBUTIONS
MLC: conceptualization, methodology, software, formal analysis, writing-original draft, writing-review & editing, visualization, project administration, TNS: formal analysis, writing-original draft, writing-review & editing, MJM: writing-original draft, writing-review & editing, JBM: writing-review & editing, MAP: conceptualization, writing-review & editing CPD: writing-review & editing, CU: methodology, software, writing-review & editing, LS: writing-review & editing, supervision.
All authors had access to the data.
CONFLICT OF INTEREST
Michael L. Creswell has no conflict of interest to report. Tamir N. Sholklapper has no conflict of interest to report. Michael J. Markel has no conflict of interest to report. James B. Mason has no conflict of interest to report. Mark A. Pianka has no conflict of interest to report. Christopher P. Dall has no conflict of interest to report. Canan Ulu has no conflict of interest to report. Lambros Stamatakis has no conflict of interest to report.
REFERENCES
[1] | National Cancer Institute. SEER Cancer Stat Facts: BladderCancer [Internet]. 2021 [cited 2021 Oct 9]. Available from: https://seer.cancer.gov/statfacts/html/urinb.html. |
[2] | Cookson MS , Herr HW , Zhang ZF , Soloway S , Sogani PC , Fair WR The treated natural history of high risk superficial bladder cancer: 15-year outcome, J Urol [Internet]. Available from: (1997) ;158: (1):62–7 http://www.ncbi.nlm.nih.gov/pubmed/9186324 |
[3] | Botteman MF , Pashos CL , Redaelli A , Laskin B , Hauser R The health economics of bladder cancer: a comprehensive review of the published literature, Pharmacoeconomics [Internet]. Available from: (2003) ;21: (18):1315–30 http://www.ncbi.nlm.nih.gov/pubmed/14750899. |
[4] | Russo GI , Sholklapper TN , Cocci A , Broggi G , Caltabiano R , Smith AB , et al. Performance of Narrow Band Imaging (NBI) and Photodynamic Diagnosis (PDD) Fluorescence Imaging Compared to White Light Cystoscopy (WLC) in Detecting Non-Muscle Invasive Bladder Cancer: A Systematic Review and Lesion-Level Diagnostic Meta-Analysis, Cancers (Basel) [Internet] (2021) ;13: (17):4378. Available from: https://www.mdpi.com/2072-6694/13/17/4378. |
[5] | Sari Motlagh R , Mori K , Laukhtina E , Aydh A , Katayama S , Grossmann NC , et al. Impact of enhanced optical techniques at time oftransurethral resection of bladder tumour, with or without singleimmediate intravesical chemotherapy, on recurrence rate ofnon-muscle-invasive bladder cancer: a systematic review and networkmeta-analysis, BJU Int [Internet] (2021) ;128: (3): 280–9. Availablefrom: https://www.ncbi.nlm.nih.gov/pubmed/33683778. |
[6] | Burger M , Grossman HB , Droller M , Schmidbauer J , Hermann G , Dru agoescu O , et al. Photodynamic diagnosis ofnon-muscle-invasive bladder cancer with hexaminolevulinatecystoscopy: a meta-analysis of detection and recurrence based on rawdata, Eur Urol [Internet].. Available from: (2406) ;64: (5):846–54.https://www.ncbi.nlm.nih.gov/pubmed/23602406. |
[7] | Jocham D , Witjes F , Wagner S , Zeylemaker B , van Moorselaar J , Grimm M-O , et al. Improved detection and treatmentof bladder cancer using hexaminolevulinate imaging: a prospective, phase III multicenter study., J Urol [Inter-net] (2005) ;174: (3):862–6. discussion 866. Available from: https://www.ncbi.nlm.nih.gov/pubmed/16093971. |
[8] | Grossman HB , Gomella L , Fradet Y , Morales A , Presti J , Ritenour C , et al. A phase III, multicenter comparison of hexaminolevulinate fluorescence cystoscopy and white light cystoscopy for the detection of superficial papillary lesions in patients with bladder cancer, J Urol [Internet]. (2007) ;178: (1):62–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17499283 |
[9] | Stenzl A , Burger M , Fradet Y , Mynderse LA , Soloway MS , Witjes JA , et al. Hexaminolevulinate guided fluorescence cystoscopy reduces recurrence in patients with nonmuscle invasive bladder cancer, J Urol [Internet]. (2010) ;184: (5):1907–13. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20850152. |
[10] | Chang SS , Boorjian SA , Chou R , Clark PE , Daneshmand S , Konety BR , et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer:AUA/SUO Guideline, J Urol [Internet]. (2016) ;196: (4):1021–9. Available from: https://www.jurology.com/doi/10.1016/j.juro.2016.06.049. |
[11] | Garfield SS , Gavaghan MB , Armstrong SO , Jones JS Thecost-effectiveness of blue light cystoscopy in bladder cancerdetection: United States projections based on clinical data showing4.5 years of follow up after a single hexaminolevulinatehydrochloride instillation.Can J Urol [Internet] (2013) ;20: (2):6682–9. Available from: https://www.ncbi.nlm.nih.gov/pubmed/23587507. |
[12] | Klaassen Z , Li K , Kassouf W , Black PC , Dragomir A , Kulkarni GS Contemporary cost-consequence analysis of blue light cystoscopy withhexaminolevulinate in non-muscle-invasive bladder cancer, Can UrolAssoc J [Internet].(2017) ;11: (6):173. Available from: https://dx.doi.org/10.5489/cuaj.4568. |
[13] | Dansk V , Malmström P-U , Bläckberg M , Malmenäs M Hexaminolevulinate hydrochloride blue-light flexible cystoscopy inthe detection and follow-up of nonmuscle-invasive bladder cancer:cost consequences during outpatient surveillance in Sweden, FutureOncol[Internet]. (2016) ;12: (8):1025–38. Available from: https://www.ncbi.nlm.nih.gov/pubmed/26975197. |
[14] | Todenhöfer T , Maas M , Ketz M , Kossack N , Colling C , Qvick B , et al. Retrospective German claims data study on initial treatment of bladder carcinoma (BCa) by transurethral bladder resection (TURB): a comparative analysis of costs using standard white light- (WL-) vsblue light- (BL-) TURB, World J Urol [Internet] (2021) ;39: (8):2953–60. Available from: http://www.ncbi.nlm.nih.gov/pubmed/33569642. |
[15] | Dindyal S , Nitkunan T , Bunce CJ The economic benefit of photodynamic diagnosis in non-muscle invasive bladder cancer, Photodiagnosis Photodyn Ther (2008) ;5: (2):153–8. |
[16] | Lotan Y , Bivalacqua TJ , Downs T , Huang W , Jones J , Kamat AM , et al. Blue light flexible cystoscopy with hexaminolevulinate innon-muscle-invasive bladder cancer: review of the clinical evidenceand consensus statement on optimal use in the USA - update 2018 NatRev Urol[Internet] (2019) ;16: (6):377–86. Available from: https://www.ncbi.nlm.nih.gov/pubmed/31019310. |
[17] | National Comprehensive Cancer Network Bladder Cancer (V6.2020) [Internet]. 2020. p. 1–118. Available from: https://www.nccn.org/professionals/physiciangls/pdf/bladder.pdf. |
[18] | Fernandez-Gomez J , Madero R , Solsona E , Unda M , Martinez-Piñeiro L , Gonzalez M , et al. Predicting Nonmuscle Invasive Bladder Cancer Recurrence and Progression in Patients Treated With Bacillus Calmette-Guerin: The CUETO Scoring Model J Urol [Internet].(2195) ;182: (5):2195–203. Available from: https://dx.doi.org/10.1016/j.juro.2009.07.016. |
[19] | Sylvester RJ , Van Der Meijden APM , Oosterlinck W , Witjes JA , Bouffioux C , Denis L , et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: A combined analysis of 2596 patients from seven EORTC trials, Eur Urol (2006) ;49: (3); 466–77. |
[20] | Kamat AM , Cookson M , Witjes JA , Stenzl A , Grossman HB The Impact ofBlue Light Cystoscopy with Hexaminolevulinate (HAL) on Progressionof Bladder Cancer - A New Analysis, Bl cancer (Amsterdam,Netherlands) [Internet]. (2016) ;2: (2):273–8. Available from: https://www.ncbi.nlm.nih.gov/pubmed/27376146. |
[21] | Gakis G , Fahmy O Systematic Review and Meta-Analysis on the Impactof Hexaminolevulinate- Versus White-Light Guided TransurethralBladder Tumor Resection on Progression in Non-Muscle InvasiveBladder Cancer, Bl cancer (Amsterdam, Netherlands) [Internet] (2016) ;2: (3):293–300. Available from: https://www.ncbi.nlm.nih.gov/pubmed/27500197. |
[22] | Barmoshe S , Zlotta AR Prognosis of T1G3 tumors: Clinical factors, Eur Urol Suppl (2004) ;3: (3): 73–8. |
[23] | Witjes JA Management of BCG Failures in Superficial Bladder Cancer: A Review, Eur Urol (2006) ;49: (5):790–7. |
[24] | Balar AV , Kamat AM , Kulkarni GS , Uchio EM , Boormans JL , Roumiguié M , et al. Pembrolizumab monotherapy for the treatmentof high-risk non-muscle-invasive bladder cancer unresponsive to BCG(KEYNOTE-057): an open-label, single-arm, multicentre, phase 2study, Lancet Oncol [Internet]. (2021) 22: (7):919–30. Available from: https://www.ncbi.nlm.nih.gov/pubmed/34051177. |
[25] | Black PC , Tangen C , Singh P , McConkey DJ , Lucia S , Lowrance WT , et al. Phase II trial of atezolizumab in BCG-unresponsive non-muscle invasive bladder cancer: SWOG S1605 (NCT #02844816)J Clin Oncol [Inter-net] (2020) ;38: (15suppl):5022–5022. Available from: https://ascopubs.org/doi/10.1200/JCO.2020.38.15suppl.5022. |
[26] | Centers for Medicare & Medicaid Services. Medicare Fee-for-Service Payment [Internet]. 2021 [cited 2021 Feb 8].Available from: https://www.cms.gov/Medicare/Medicare |
[27] | Daniltchenko DI , Riedl CR , Sachs MD , Koenig F , Daha KL , Pflueger H , et al. Long-term benefit of aminolevulinic acid fluorescence assisted transurethral resection of superficial bladder cancer: 5-year results of a prospective randomized study, J Urol [Internet]. (2005) ;174: (6):2129–33. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16280742. |
[28] | Mari A , Campi R , Tellini R , Gandaglia G , Albisinni S , Abufaraj M , et al. Patterns and predictors of recurrence after open radical cystectomy for bladder cancer: a comprehensive review of the literature, World J Urol (2018) ;36: (2):157–70. |
[29] | Lewicki P , Arenas-Gallo C , Qiu Y , Venkat S , Basourakos SP , Scherr D , et al. Underutilization of Blue Light Cystoscopy for Bladder Cancer in the United States. Eur Urol Focus [Internet]. 2021;(xxxx). Available from: https://doi.org/10.1016/j.euf.2021.09.025. |
[30] | KARL-STORZ-, Endoscopy-America Value Analysis Brief: Karl Storz Blue Light Cystoscopy with Cysview System [Internet]. 2017. p. 1–17. Available from: https://s3images.coroflot.com/user_files/individual_files/original_pdf_521266_jrgkol7r2tgcy9rq8prs3g6kj.pdf. |
[31] | Photocure KARL STORZ Blue Light ystoscopy with ysview System Photodynamic Diagnosis (PDD) [Internet].2018. p. 1–5. Available from: https://www.cysview.com/wp- content/uploads/2019/01/5c2fd52c98a2b6807e6d53d2KARL-STORZ-Blue-Light-Cystoscopy-with-Cysview-2-Part-System-Brochure.pdf. |
[32] | Regan MM , Weitzell EC Economic Evaluation of Soil and Water Conservation Measures and Programs, J Farm Econ (1947) ;29: (4): 1275. |
[33] | Edmonds VS , Haglin JM , Tyson MD Declining Medicare Reimbursement for Urologists: An Opportunity for Informed Advocacy, J Urol (2021) ;206: (1):10–2. |
[34] | Kaye DR , Miller DC , Ellimoottil C Alternative payment models and urology, Curr Opin Urol (2017) ;27: (4): 360–5. |


