
Outcomes of Patients with Bacillus Calmette-Guérin (BCG)-Unresponsive Non-Muscle Invasive Bladder Cancer as Defined by the U.S. Food and Drug Administration
Abstract
BACKGROUND:
Limited data are available on the outcomes of patients with non-muscle invasive bladder cancer (NMIBC) unresponsive to intravesical bacillus Calmette-Guérin (BCG), as defined by the United States Food and Drug Administration.
OBJECTIVE:
To define the outcomes of patients with BCG-unresponsive NMIBC.
METHODS:
This was a retrospective, single-institution observational cohort study. Records of patients managed at our institution for BCG-unresponsive NMIBC between 2005 and 2020 were reviewed and clinical outcomes evaluated.
RESULTS:
The study included 149 patients. Management was with initial radical cystectomy in 60 patients (40%) and initial bladder-sparing therapy (BST) in 89 patients (60%). Overall survival was greater among patients undergoing RC than BST (HR 1.83, 95% CI 1.04–3.22, p = 0.036), potentially due to patient selection, as no significant difference was noted for metastasis-free or cancer-specific survival. Patients opting for initial BST had high rates of treatment failure, with estimated 5-year cystectomy-free survival of only 42%. Patients who received additional lines of BST after a subsequent failure were at increased risk of having ≥pT3 or pN+ disease at cystectomy (42% for ≥2 lines BST, versus 18% for 1 line BST and 15% for initial cystectomy, p = 0.038).
CONCLUSION:
Among patients who underwent initial BST for BCG-unresponsive NMIBC, rates of treatment failure were very high. Patients who underwent delayed cystectomy after ≥2 lines of BST had elevated rates of extravesical disease. Our observations emphasize the importance of recent and ongoing clinical trials in this clinical space.
INTRODUCTION
The mainstay of treatment in high-risk non-muscle invasive bladder cancer (NMIBC) is complete transurethral resection of bladder tumors (TURBT) followed by intravesical instillation of bacillus Calmette-Guérin (BCG) [1–3]. BCG significantly reduces the risk of recurrence and progression [4–8]. Unfortunately, approximately 30 to 40% of patients experience recurrent disease despite BCG treatment [4–7]; and even the best reported outcomes still place 5-year recurrence rates at over 25% [9]. Patients who have high grade disease recurrence following BCG are faced with a difficult choice. Radical cystectomy with urinary diversion has excellent oncologic outcomes, with 5-year recurrence-free survival rates of approximately 80 to 90% [10–12]. However, cystectomy and urinary diversion carries significant morbidity and may be discouraged by clinicians or refused by patients for numerous reasons such as body image or perceived detriment to quality of life, a process which was explored in the recent BRAVO trial [13]. A number of alternate treatment options have been proposed for patients unwilling or unfit to undergo cystectomy, including continued treatment with BCG or intravesical chemotherapy with various agents including valrubicin, gemcitabine, and gemcitabine plus docetaxel [14].
Development of new treatments for BCG-unresponsive NMIBC has been hampered by the lack of a standard-of-care comparator treatment and the lack of a unified definition of BCG unresponsive disease [15]. These barriers led the United States Food and Drug Administration (FDA) to issue a statement which included a unified definition of BCG-unresponsive NMIBC based on prior research, as well as guidance including approval of single-arm trial design with complete response as a primary endpoint [16, 17]. A number of ongoing clinical trials have arisen from this guidance [18–21]. Despite the importance of this definition of BCG-unresponsive NMIBC for clinical trial design, only limited literature exists on the outcomes of patients with this disease state who do not undergo radical cystectomy [22]. There is also very limited data on patients who pursue multiple lines of therapy rather than undergo cystectomy. We sought to address this limitation in the literature by examining our own institutional experience with such patients. We hypothesized that patients undergoing bladder-sparing treatment would experience high rates of treatment failure and that receipt of additional lines of bladder-sparing treatment after subsequent failures would be associated with adverse pathologic and oncologic outcomes.
PATIENTS AND METHODS
Patients
Following Institutional Review Board (IRB) ap-proval (protocol number STU 2021-0527), we assembled a database of patients undergoing treatment for BCG unresponsive non muscle invasive bladder cancer (NMIBC) at the University of Texas Southwestern Medical Center (UTSW) between March 2005 and December 2020.
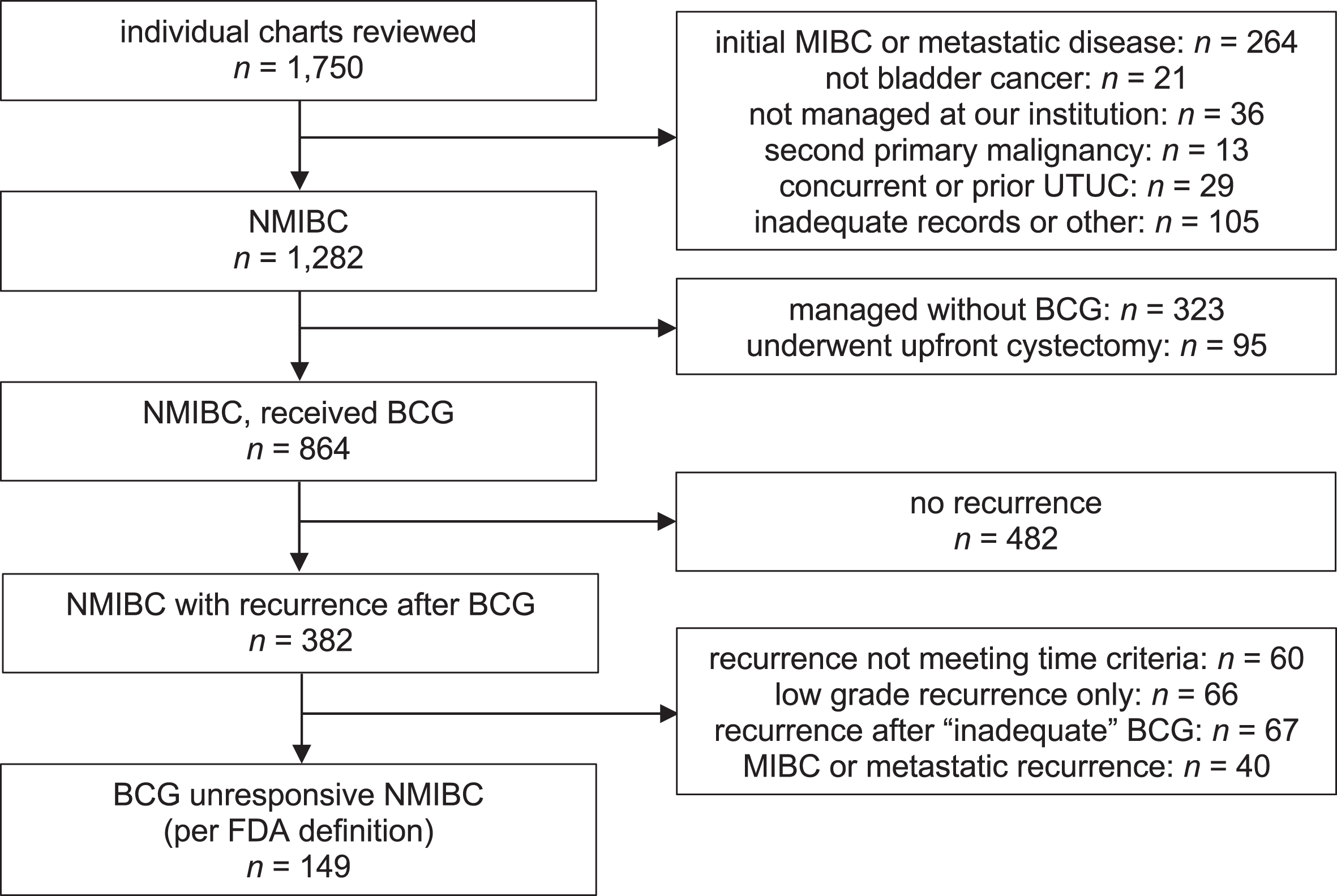
In order to ensure that all eligible patients were captured, we adopted a strategy in which candidate patients were identified by an initial search using very broad criteria (expected to yield many false-positives) and then manually screened to confirm eligibility. Our initial search included a query to billing records to identify all patients receiving a standard-of-care treatment for NMIBC, including those with billing codes for receipt of intravesical treatment (Current Procedural Terminology (CPT) codes 51720 and J9030); those documented as receiving docetaxel with an associated diagnosis of bladder cancer (International Classification of Diseases version 9 (ICD-9) code 188.x or ICD-10 code C67.x); and those receiving pembrolizumab with an associated diagnosis of bladder cancer (ICD-9 188.x or ICD-10 C67.x). We additionally queried the institutional tumor registry for patients with a diagnosis of bladder cancer and a clinical stage of Ta, Tis, or T1. These combined queries yielded a total of 1,750 unique medical records which were then reviewed to determine eligibility, including the stage/grade of disease at initial diagnosis, the timing and dosage of BCG administration, and the timing and stage/grade of BCG failure. Patients were included if they met the criteria established in the 2018 United States Food and Drug Administration (FDA) white paper on drug development in NMIBC [24, 27], which included (1) those with ≥T1 high grade disease at first evaluation following receipt of induction BCG (at least 5/6 doses); (2) those with any high grade or ≥T1 disease within six months of induction plus maintenance (at least 2/3 doses) or reinduction BCG; and (3) those with carcinoma in situ within twelve months of induction plus maintenance or reinduction BCG. These criteria presuppose the use of the Southwest Oncology Group (SWOG) dosing schedule (six weeks’ induction, plus three weeks’ maintenance at 3, 6, 12, 18, 24, 30, and 36 months; with the option for reinduction BCG in the event of recurrent or persistent disease). Thus, patients on atypical/unconventional dosing schedules were excluded. Patients who were managed in any capacity at our institution following development of BCG unresponsive disease were included. In patients with multiple episodes meeting the definition of BCG unresponsive NMIBC, the earliest episode was considered the point of reference for the study. Patients were excluded if they had a concurrent or prior diagnosis of upper tract urothelial carcinoma with a disease-free interval following radical nephroureterectomy of less than 12 months. Patients were also excluded if they had a second primary malignancy (aside from organ-confined low- or intermediate-risk prostate cancer) or if they had a history of prior complex genitourinary reconstruction. Details concerning included/excluded patients are provided in Fig. 1. All data were collected retrospectively and informed consent was waived by the IRB due to the unfeasibility of contacting all patients for consent. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cohort studies. The completed STROBE checklist is provided in Supplementary Materials.
Fig. 1
Patients included in the study. “Inadequate” BCG was defined as less than 5/6 doses of an induction or reinduction course and less than 2/3 doses of a maintenance course. Abbreviations: BCG, bacille Calmette-Guérin; MIBC, muscle-invasive bladder cancer; NMIBC, non-muscle invasive bladder cancer; UTUC, upper tract urothelial carcinoma; XRT, radiation therapy.
Treatments
Patients were managed at the discretion of their treating clinicians with either initial radical cystectomy (RC) or bladder-sparing therapy (BST), taking into consideration the totality of patient- and disease-related factors. At our institution, neoadjuvant chemotherapy (NACT) is only offered to patients with ≥cT2 disease; thus, no patients in the initial RC group received NACT. Some patients in the initial BST group who had subsequent disease progression did receive NACT. Similarly, chemoradiation therapy was also restricted to those with ≥cT2 disease and so was not offered to any patients in the initial BCG unresponsive NMIBC cohort; however, it was offered to select patients in the initial BST group who experienced subsequent disease progression.
Data collection
Survival times were calculated from the point of BCG unresponsive disease (“BCG failure”), which was the date of the TURBT which confirmed the diagnosis. For all purposes, metastasis was defined by the date of a pathologic diagnosis confirming metastatic (≥cM1a) disease or by the date of an imaging study which prompted the patient to be managed as metastatic. Recurrence was defined as pathologically proven high grade recurrent disease on TURBT or by the development of metastatic disease as defined above. Findings on cystoscopy or positive urine cytology alone were not considered sufficient to define recurrence. Progression was defined by pathological ≥T2 or N+ disease on TURBT or radical cystectomy specimens, or by the development of metastatic disease as defined above. Cystectomy-free survival was defined by the interval to the date of radical cystectomy. Bladder-intact metastasis-free survival was defined by the interval to radical cystectomy or development of metastatic disease as defined above, whichever occurred first. Deaths were determined to be cancer-related if they occurred in the context of metastatic urothelial carcinoma and were not definitively unrelated to the underlying malignancy, or if they resulted from a complication of cancer treatment. Cancer stage and grade were classified using the American Joint Commission on Cancer (AJCC) 8th edition TNM system and the 1998 World Health Organization/International Society of Urological Pathology (WHO/ISUP) systems, respectively. Tumor size at TURBT was determined by reference to operative reports or, where not available, by reference to Current Procedural Terminology (CPT) billing codes. Charlson Comorbidity Index (CCI) scores were determined retrospectively by a full-chart text search for each of the component medical conditions, as well as by review of the initial outpatient consult note and any available anesthesia preoperative evaluations. Patients were defined as lost to follow up if they were alive at the point of last contact with >12 months elapsed since that time. Date of final data collection was March 19, 2022.
Statistical methods
Descriptive statistics were reported as number and percentage for categorical variables and as median with interquartile range (IQR) for continuous variables. Comparisons between groups were made using the Pearson χ2 test or the Mann-Whitney U test, as appropriate. Survival outcomes were reported using the Kaplan-Meier method, with comparisons between multiple groups using the log-rank test and association of covariates with survival using the Cox proportional hazards method. Missing values were omitted. Covariates were included in multivariable analyses if they achieved a p value of ≤0.10 on univariable analysis. Median follow-up was estimated by the reverse Kaplan-Meier method [23].
Immortal-time bias was a concern in when comparing outcomes between patients undergoing 1 and ≥2 lines of bladder-sparing treatment. This phenomenon occurs in retrospective comparisons of groups where inclusion in one group requires patients by definition to have survived for a certain period of time. In this case, patients included in the group receiving ≥2 lines of BST, by definition, suffered no clinical event during the period of time prior to starting a second line of BST. This would tend to bias outcomes in favor of this group. Where relevant, this concern was addressed by treating exposure as a time-dependent covariate [24].
For all analyses, the threshold for statistical significance was set at p < 0.05 and all p values were two-sided. Data analysis was performed using SPSS version 27 (IBM, Armonk, New York).
RESULTS
Study population, patient characteristics, and oncologic outcomes
A total of 1,750 charts were reviewed to identify a study population of 149 patients with BCG-unres-ponsive, non-muscle invasive bladder cancer (≤cT1 N0 M0) (Fig. 1). Of note, we excluded 40 patients who otherwise met criteria for BCG unresponsiveness but had muscle-invasive, node-positive, and/or metastatic disease. Characteristics of the study population are provided in Table 1. At the time of developing BCG unresponsive NMIBC, 60 patients (40%) underwent radical cystectomy (RC) and 89 (60%) were treated with different modalities of bladder-sparing treatment (BST) as detailed in Supplementary Table 1. Patients opting for radical cystectomy were more likely to have invasive (cT1) disease than those undergoing initial BST (67% versus 46%, p = 0.013, χ2 test). No other difference be-tween the groups reached statistical significance.
Table 1
Demographic and disease characteristics of patients with BCG unresponsive NMIBC (≤cT1 N0 M0), stratified by treatment at time of BCG unresponsive disease
| Characteristic n (%) or median (IQR) | Radical Cystectomy | Bladder-Sparing Treatment | Total | p |
| patient demographics/history | ||||
| total patients | 60 (40%) | 89 (60%) | 149 | |
| age, years | 71 (65–76) | 72 (66–78) | 72 (65–77) | 0.45 |
| < 50 | 3 (5.0%) | 3 (3.4%) | 6 (4.0%) | 0.75 |
| 50–59 | 5 (8.3%) | 9 (10%) | 14 (9.4%) | |
| 60–69 | 16 (27%) | 18 (20%) | 34 (23%) | |
| 70–79 | 29 (48%) | 43 (48%) | 72 (48%) | |
| ≥80 | 7 (12%) | 16 (18%) | 23 (15%) | |
| sex | ||||
| male | 46 (77%) | 78 (88%) | 124 (83%) | 0.079 |
| female | 14 (23%) | 11 (12%) | 25 (17%) | |
| Charlson comorbidity index (exclusive of malignancy) | ||||
| 0–1 | 5 (8.3%) | 8 (9.0%) | 13 (8.7%) | 0.98 |
| 2–3 | 19 (32%) | 28 (32%) | 47 (32%) | |
| 4–5 | 26 (43%) | 36 (40%) | 62 (42%) | |
| ≥6 | 10 (17%) | 17 (19%) | 27 (18%) | |
| body mass index (BMI), kg/m2 | 27 (24–31) | 27 (24–31) | 27 (24–31) | 0.89 |
| obesity (BMI > 30) | 18 (30%) | 27 (30%) | 45 (30%) | 0.97 |
| history of smoking (current or prior) | 40 (67%) | 63 (71%) | 103 (69%) | 0.59 |
| history of NMIBC (prior to reference course of iBCG) | 12 (20%) | 24 (27%) | 36 (24%) | 0.33 |
| prior history of UTUC (≥12 months) | 2 (3.3%) | 3 (3.4%) | 5 (3.4%) | 0.99 |
| time from BCG failure to treatment (weeks) | 8 (5–11) | 5 (4–7) | 6 (4–9) | < 0.001 |
| duration of follow up (months, reverse Kaplan-Meier) | 81 (53–125) | 75 (33–126) | 76 (43–125) | 0.86 |
| lost to follow up | 4 (6.7%) | 5 (5.6%) | 9 (6.0%) | 0.79 |
| initial disease characteristics | ||||
| (prior to induction BCG) | ||||
| tumor stage | ||||
| Ta/Tis (noninvasive) | 27 (46%) | 52 (60%) | 79 (54%) | 0.096 |
| T1 (invasive) | 32 (54%) | 35 (40%) | 67 (46%) | |
| carcinoma in situ (any component) | 23 (41%) | 27 (33%) | 50 (37%) | 0.36 |
| BCG administration details | ||||
| BCG administered at outside facility | 24 (40%) | 25 (28%) | 49 (33%) | 0.13 |
| total BCG instillations (induction + maintenance) | 9 (6–12) | 9 (6–12) | 9 (6–12) | 0.65 |
| BCG unresponsive disease characteristics | ||||
| year of BCG unresponsive diagnosis, median | 2015 | 2017 | 2016 | 0.10 |
| 2005–2008 | 5 (8.3%) | 12 (14%) | 17 (11%) | 0.27 |
| 2009–2012 | 14 (23%) | 17 (19%) | 31 (21%) | |
| 2013–2016 | 24 (40%) | 25 (28%) | 49 (33%) | |
| 2017–2020 | 17 (28%) | 35 (39%) | 52 (35%) | |
| unresponsive disease classification | ||||
| ≥T1 disease after induction | 27 (45%) | 33 (37%) | 60 (40%) | 0.40 |
| HG or ≥T1 ≤6 months after last maintenance | 16 (27%) | 33 (37%) | 49 (33%) | |
| CIS ≤12 months after last maintenance | 17 (28%) | 23 (26%) | 40 (27%) | |
| tumor stage | ||||
| Ta/Tis (noninvasive) | 20 (33%) | 48 (54%) | 68 (46%) | 0.013 |
| T1 (invasive) | 40 (67%) | 41 (46%) | 81 (54%) | |
| tumor grade | ||||
| low grade | 0 | 1 (1.1%) | 1 (0.7%) | 0.41 |
| high grade | 60 (100%) | 87 (99%) | 147 (99%) | |
| not reported | 0 | 1 (1.1%) | 1 (0.7%) | |
| tumor size | ||||
| small (< 2 cm) | 45 (80%) | 68 (86%) | 113 (84%) | 0.39 |
| medium (2–5 cm) | 10 (18%) | 11 (14%) | 21 (16%) | |
| large (≥5 cm) | 1 (1.8%) | 0 | 1 (0.7%) | |
| carcinoma in situ (any component) | 36 (62%) | 53 (62%) | 89 (62%) | 0.96 |
| variant histology (at or before BCG failure) | 8 (13%) | 6 (6.7%) | 14 (9.4%) | 0.18 |
| micropapillary | 3 (5.0%) | 2 (2.2%) | 5 (3.4%) | |
| squamous cell | 1 (1.7%) | 2 (2.2%) | 3 (2.0%) | |
| glandular/adenocarcinoma | 2 (3.3%) | 2 (2.2%) | 4 (2.7%) | |
| nested | 2 (3.3%) | 0 | 2 (1.3%) | |
| variant histology (at any point) | 11 (18%) | 10 (11%) | 21 (14%) | 0.22 |
| micropapillary | 3 (5.0%) | 3 (3.3%) | 6 (4.0%) | |
| squamous cell | 3 (5.0%) | 3 (3.3%) | 6 (4.0%) | |
| glandular/adenocarcinoma | 3 (5.0%) | 3 (3.3%) | 6 (4.0%) | |
| nested | 2 (3.3%) | 0 | 2 (1.3%) | |
| plasmacytoid | 0 | 1 (1.1%) | 1 (0.7%) |
Patients were defined as lost to follow up if they were last reported alive with > 12 months since the time of last contact. Disease was high grade at the time of initial TURBT in all cases. Variant histology is reported if present in any proportion. Column percentages are exclusive of missing values. Abbreviations: BCG, bacille Calmette-Guérin; BMI, body mass index; CIS, carcinoma in situ; iBCG, induction BCG; NMIBC, non-muscle invasive bladder cancer; UTUC, upper tract urothelial carcinoma. Reported p values are per the Mann-Whitney U test for continuous variables and the Pearson χ2 test for categorical variables. Duration of follow up was calculated by the reverse Kaplan-Meier method.
Outcomes of the overall patient cohort
Median (IQR) duration of follow up for the overall cohort was 76 (43–125) months (81 [53–125] for patients undergoing initial RC, 75 [33–126] months for patients undergoing initial BST, p = 0.86, all by the reverse Kaplan-Meier method). Comparing patients who underwent initial RC to initial BST, neither metastasis-free survival (MFS) nor cancer-specific survival (CSS) differed significantly between groups (HR for MFS 1.30, 95% CI 0.68–2.52, p = 0.42; HR for CSS 1.58, 95% CI 0.78–3.19, p = 0.20) (Fig. 2A and 2B). The survival curves did diverge, however, suggesting that the study may have been underpowered to detect a difference in these outcomes. Overall survival (OS) was greater among patients undergoing RC than BST (HR 1.83, 95% CI 1.04–3.22, p = 0.036), possibly due in part to selection of healthier patients for RC (Fig. 2C). No clinical or demographic factor, including choice of initial RC versus initial BST, was significantly associated with MFS on univariable or multivariable Cox regression analysis. Greater patient age and higher Charlson comorbidity index (CCI) were associated with poorer CSS (HR for age 1.04 / year, 95% CI 1.01–1.08, p = 0.028; HR for CCI 1.25 / point, 95% CI 1.03–1.50, p = 0.023) on univariable analysis, but these factors did not reach significance on multivariable analysis (Supplementary Table 2).
Fig. 2
Oncologic outcomes of patients with BCG-unresponsive NMIBC. Kaplan-Meier curves showing metastasis-free (A), cancer-specific (B) and overall survival (C) of patients with BCG-unresponsive NMIBC opting for either upfront cystectomy or initial bladder-sparing management at the time of BCG unresponsive disease (“BCG failure”). Metastasis-free and cancer-specific survival did not differ significantly between the two groups (HR for MFS 1.30, 95% CI 0.68–2.52, p = 0.42; HR for CSS 1.58, 95% CI 0.78–3.19, p = 0.20), whereas overall survival was greater among patients undergoing initial RC (HR 1.83, 95% CI 1.04–3.22, p = 0.036). Abbreviations: BCG, bacillus Calmette-Guérin; CI, confidence interval; CSS, cancer-specific survival; HR, hazard ratio; MFS, metastasis-free survival; NMIBC, non-muscle invasive bladder cancer; OS, overall survival.
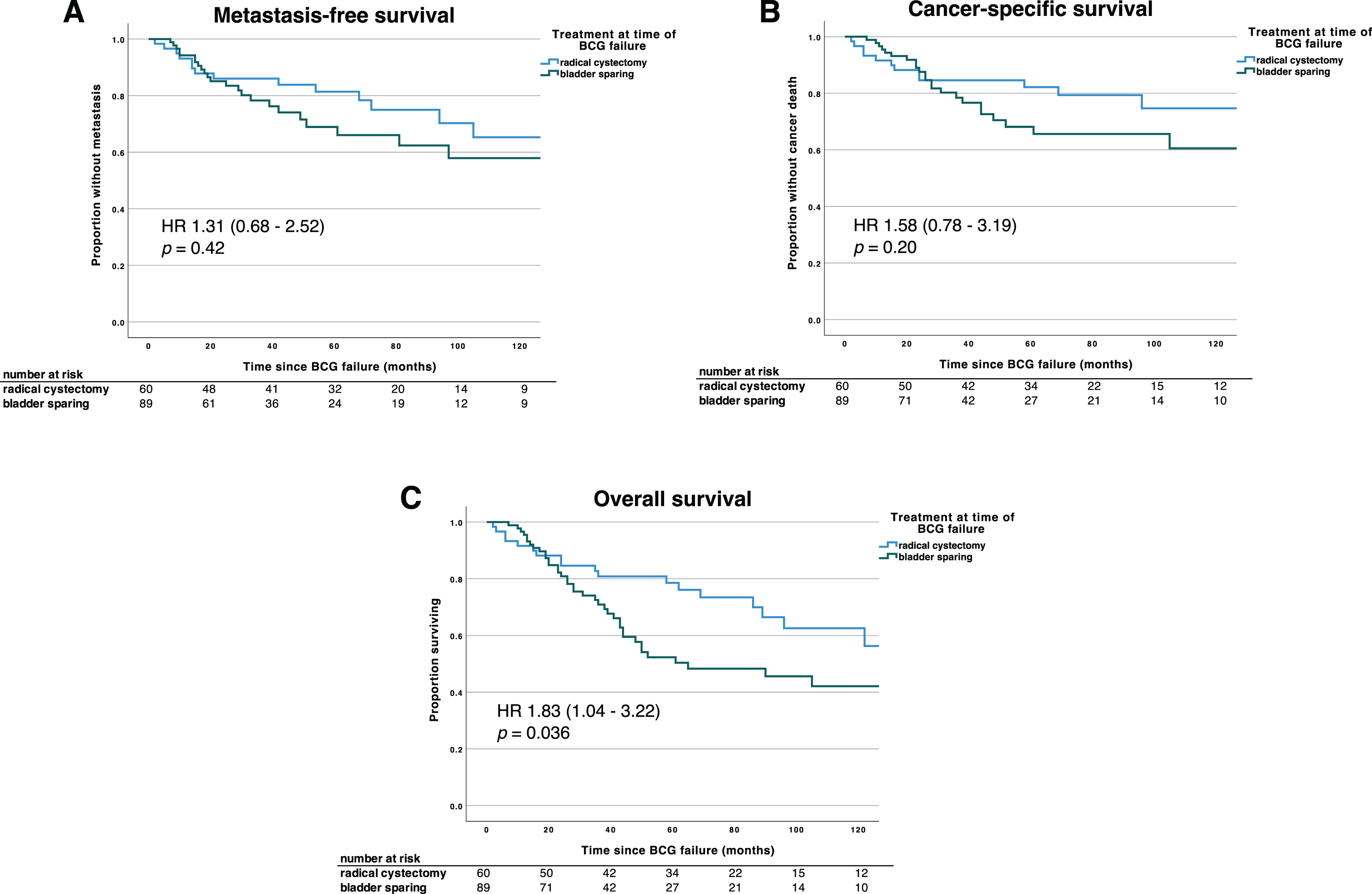
Table 2
Detailed outcomes of patients undergoing initial bladder-sparing treatment for BCG unresponsive NMIBC
| Outcome | 6 months | 12 months | 18 months | 24 months | 48 months | 60 months | ||||||
| recurrence | 34% | 89 | 58% | 58 | 72% | 37 | 75% | 22 | 80% | 10 | 80% | 8 |
| progression | 2% | 89 | 16% | 86 | 25% | 60 | 28% | 50 | 36% | 29 | 39% | 20 |
| rec’d 2nd-line BST | 9% | 89 | 31% | 80 | 38% | 57 | 44% | 45 | 45% | 21 | 49% | 14 |
| rec’d 3rd-line BST | 0% | 89 | 1% | 88 | 8% | 83 | 12% | 67 | 25% | 30 | 25% | 20 |
| rec’d 4th-line BST | 0% | 89 | 0% | 88 | 1% | 84 | 3% | 72 | 14% | 37 | 20% | 22 |
| cystectomy | 5% | 89 | 22% | 84 | 35% | 67 | 38% | 48 | 47% | 22 | 58% | 15 |
| metastasis | 0% | 89 | 6% | 88 | 11% | 81 | 15% | 67 | 26% | 35 | 31% | 25 |
| cystectomy or metastasis | 5% | 89 | 23% | 84 | 39% | 67 | 43% | 46 | 55% | 21 | 64% | 14 |
| bladder cancer death | 0% | 89 | 3% | 89 | 7% | 85 | 11% | 75 | 28% | 40 | 32% | 28 |
Values shown are the Kaplan-Meier estimate of the proportion of patients experiencing an event by each timepoint and the number of patients at risk in each interval. Abbreviations: BST, bladder-sparing treatment.
Outcomes of patients undergoing initial bladder-sparing treatment
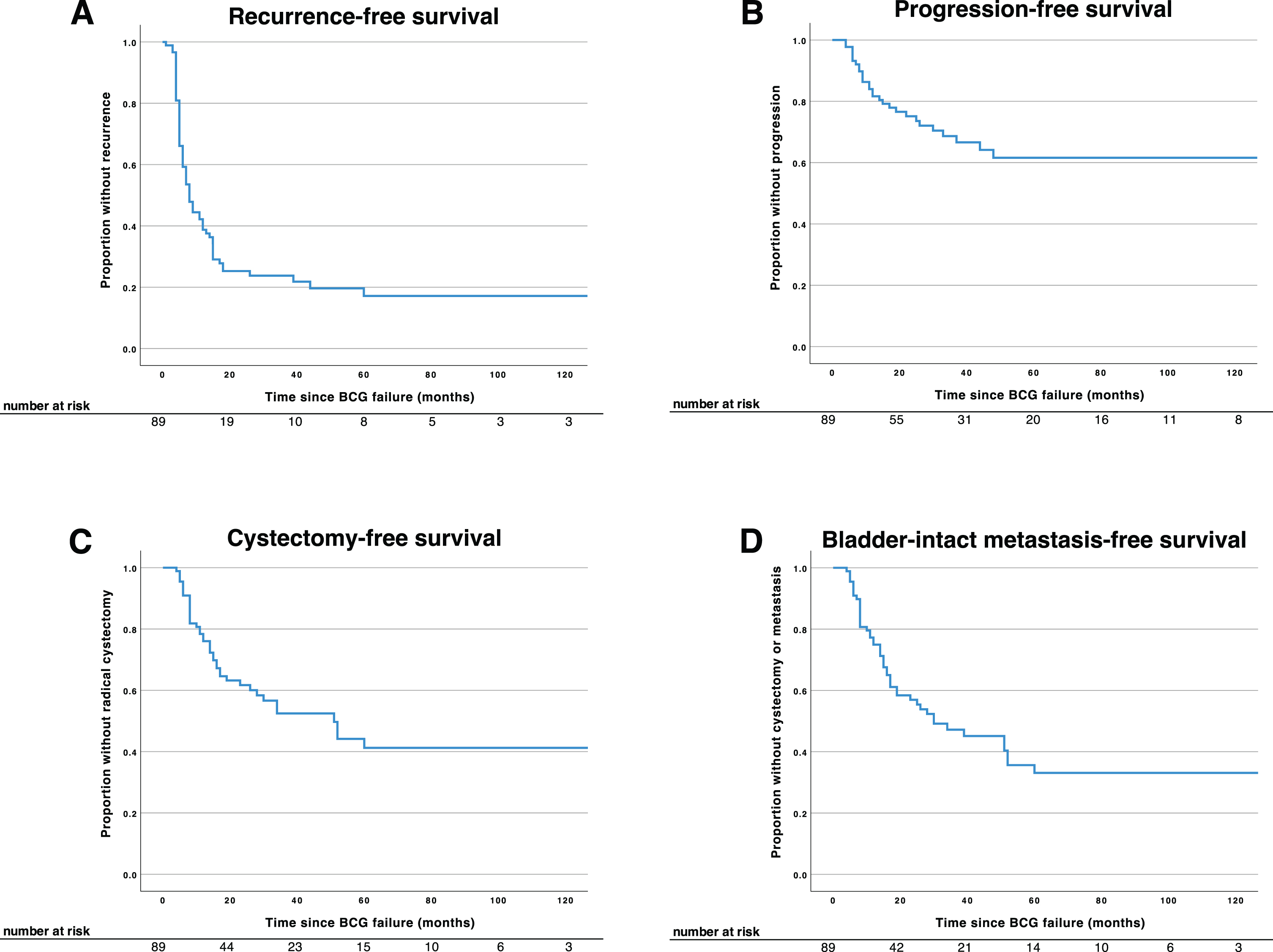
Of the 89 patients who were managed with initial bladder-sparing treatment (BST), 57 patients (64%) received additional BCG, 24 patients (27%) received alternate intravesical agents as detailed in Supplementary Table 1, and 6 patients (6.7%) received re-TURBT or observation only. Patients managed with initial BST had high rates of treatment failure. Three-quarters of patients experienced recurrence within two years of treatment (Fig. 3A), and roughly 25% of patients progressed to muscle invasive or metastatic disease in the same interval (Fig. 3B). Estimated two-year cystectomy-free survival (CFS) and bladder-intact metastasis-free survival (BIMFS) were 62% and 57%, respectively (Fig. 3C, D), and five-year CFS was only 42% (Fig. 3C). Thus, initial BST proved unable to prevent cystectomy in a majority of patients. BCG-unresponsive NMIBC clinical trials are often stratified by the presence or absence of carcinoma in situ (CIS) at the time of BCG failure. In our cohort, the presence of CIS at BCG failure was associated with significantly poorer RFS (HR 1.67, 95% CI 1.03–2.70, p = 0.037), but association with other outcomes did not reach significance (Supplementary Figure 1). Further detail concerning the outcomes of patients opting for initial BST, including receipt and timing of additional lines of BST, is provided in Table 2.
Fig. 3
Oncologic outcomes of patients undergoing bladder-sparing treatment for BCG-unresponsive NMIBC. Kaplan-Meier curves showing recurrence-free (A), progression-free (B), cystectomy-free (C), and bladder-intact metastasis-free survival (D) of patients opting for initial bladder-sparing management of BCG-unresponsive NMIBC. Recurrence-free survival was a composite of high-grade intravesical and systemic recurrence. Progression-free survival was a composite of muscle-invasive (≥T2) and metastatic (nodal/distant) progression. A large majority of patients experienced disease recurrence within the first two years, and over half underwent radical cystectomy within five years of initial BCG failure. Abbreviations: BCG, bacillus Calmette-Guérin; NMIBC, non-muscle invasive bladder cancer.
Outcomes of patients receiving multiple lines of bladder-sparing treatment
Patients who opt for initial BST are often averse to undergoing radical cystectomy and will inquire about additional lines of BST after treatment failures. We sought to examine the outcomes of such patients. Of the 89 patients opting for initial BST, 40 (45%) went on to receive a second line of BST after a failure of the initial course, and some patients received as many as six additional lines of BST (Supplementary Table 3 and data not shown). Among patients who underwent radical cystectomy, those who received two or more lines of BST had a significantly higher risk of extravesical disease (≥pT3 or pN+) than those who underwent initial RC or one line of BST (15% versus 18% versus 42%, p = 0.038), despite greater receipt of neoadjuvant chemotherapy (Table 3). Compared with initial RC, receipt of ≥2 lines of BST was independently associated with non-organ-confined disease at cystectomy on both univariable and multivariable logistic regression analysis (univariable OR 4.12, 95% CI 1.30–13.1, p = 0.016; multivariable OR 4.47, 95% CI 1.33–15.0, p = 0.015) (Supplementary Table 4). This difference in pathologic outcomes was not, however, associated with a significant difference in oncologic outcomes compared with patients undergoing initial RC or only 1 line of BST (log-rank p = 0.68 for MFS, p = 0.39 for CSS) (Supplementary Figure 2). To account for immortal-time bias, we performed a time-varying Cox regression comparing oncologic outcomes of patients undergoing ≥2 lines versus 1 line of BST, which again showed no significant difference in MFS or CSS (HR for MFS 1.91, 95% CI 0.82–4.42, p = 0.13; HR for CSS 1.19, 95% 0.52–2.75, p = 0.68) (Table 4).
Table 3
Pathologic outcomes of patients undergoing radical cystectomy either at the time of BCG unresponsive disease (upfront cystectomy) or after receiving 1 or ≥2 lines of bladder-sparing treatment
| Characteristic n (%) or median (IQR) | Initial cystectomy | 1 line bladder-sparing treatment | ≥2 lines bladder-sparing treatment | p |
| Total patients | 60 | 22 | 19 | |
| received NACT | 0 | 2 (9.1%) | 3 (16%) | |
| TNM pathologic stage | ||||
| pT0 | 13 (22%) | 2 (9.1%) | 1 (5.3%) | 0.15 |
| pTa/Tis | 24 (40%) | 8 (36%) | 5 (26%) | |
| pT1 | 15 (25%) | 5 (23%) | 5 (26%) | |
| pT2 | 2 (3.3%) | 3 (14%) | 1 (5.3%) | |
| pT3 | 5 (8.3%) | 2 (9.1%) | 4 (21%) | |
| pT4 | 1 (1.7%) | 2 (9.1%) | 3 (16%) | |
| pN+ | 4 (6.7%) | 3 (14%) | 3 (16%) | 0.41 |
| ≥pT3 or pN+ | 9 (15%) | 4 (18%) | 8 (42%) | 0.038 |
| carcinoma in situ | 33 (58%) | 14 (67%) | 9 (47%) | 0.47 |
| lymphovascular invasion | 5 (8.9%) | 4 (19%) | 5 (28%) | 0.12 |
Extravesical (≥pT3 or pN+) disease was more prevalent among those undergoing ≥2 lines of bladder-sparing treatment compared with those undergoing upfront cystectomy or cystectomy after 1 line of bladder-sparing treatment (p = 0.038). Tumor grade is not shown, as all tumors were high grade. Reported p values are per the Pearson χ2 test. Abbreviations; IQR, interquartile range (25th–75th percentiles); NACT: neoadjuvant chemotherapy.
Table 4
Oncologic risk associated with receipt of ≥2 lines of bladder-sparing treatment
| Outcome | Hazard ratio | 95% confidence interval | p |
| recurrence-free survival | 2.55 | 0.58–11.2 | 0.22 |
| progression-free survival | 1.99 | 0.89–4.47 | 0.10 |
| cystectomy-free survival | 2.54 | 1.30–4.97 | 0.007 |
| metastasis-free survival | 1.91 | 0.82–4.42 | 0.13 |
| bladder-intact metastasis-free survival | 2.57 | 1.39–4.76 | 0.003 |
| cancer-specific survival | 1.19 | 0.52–2.75 | 0.68 |
Time-varying Cox regression analysis assessing risk of the described oncologic outcomes in patients undergoing ≥2 lines of BST, compared with patients receiving 1 line of BST. Hazard ratios are reported such that a ratio > 1 indicates greater risk among patients receiving ≥2 lines of BST. Time-varying Cox regression was employed due to the presence of immortal-time bias, which would otherwise tend to favor the ≥2 lines BST group.
DISCUSSION
The management of BCG-unresponsive non-muscle invasive bladder cancer has been complicated by clinical heterogeneity, the lack of a consistent definition of BCG unresponsiveness, and a wide variety of treatment options with little data on comparative effectiveness. In one influential early series, patients failing two consecutive courses of BCG treatment faced a 50% risk of developing metastatic cancer and only a 20% chance of treatment success [25]. A randomized trial compared intravesical gemcitabine with continued BCG instillation and achieved a 2-year recurrence-free survival (RFS) rate of 19% for the gemcitabine group and only 3% for continued BCG; the corresponding progression-free survival (PFS) rates were 67% and 63%, respectively [26]. A retrospective, multi-institutional series of 276 patients receiving gemcitabine plus docetaxel for patients with NMIBC who failed BCG noted 2-year RFS and PFS rates of 46% and ∼96% [27]. Notably, these studies were all conducted in patients with “BCG failure” defined more loosely than the FDA definition used here. The recent single-arm trials of pembrolizumab, nadofaragene firadenovec, N-803, and oportuzumab monatox reported complete response (CR) rates of 41%, 53%, 71%, and 40% respectively, with median duration of response of 16.2, 9.7, 19.2, and 13.2 months in varying subgroups of BCG-unresponsive populations [18–21]. Recurrence-free rates at 12 months in these trials ranged from 19% to 57%. A large retrospective series of patients (with both papillary disease and CIS) receiving intravesical gemcitabine/docetaxel reported 24-month recurrence-free and cystectomy-free rates of 46% and 85%, respectively [27].
The ongoing Comparison of Intravesical Therapy and Surgery as Treatment Options for Bladder Cancer (CISTO) trial (NCT03933826) seeks to describe the outcomes of patients with NMIBC but is several years away from completion. Radical cystectomy is considered to be the most definitive therapy for BCG-unresponsive NMIBC, but the optimal timing of RC in this setting has yet to be determined. One study examining the outcomes of patients undergoing RC for NMIBC showed no improvements over a ten-year period, suggesting that patient selection and management has shown little improvement over time [28]. Limitations with available data have led the United States Food and Drug Administration to offer clinical guidance for the design of single-arm clinical trials, intended to serve as the basis for drug approvals [17]. However, real-world data on the outcomes of patients with BCG-unresponsive NMIBC according to this definition are limited, as are data on the outcomes of patients who pursue multiple lines of bladder-sparing therapy. We sought to review the characteristics and outcomes of these patients in our own institutional experience. We were particularly interested in outcomes of patients with multiple recurrences who chose to pursue additional lines of bladder-sparing treatment in order to avoid cystectomy.
In our series of patients with BCG-unresponsive NMIBC as defined by the FDA, only a minority (40%) opted for immediate cystectomy. Overall survival was greater among patients who underwent initial RC than those who underwent initial BST, but metastasis-free and cancer-specific survival did not differ, suggesting that patient selection was a factor in the difference in OS. This likely involved both patient-related (e.g., perceived comorbidity / life expectancy) and disease-related factors (e.g., tumor stage, which did differ significantly between groups; and perceived burden or aggressiveness of disease, which is difficult to quantify). It is also possible that the OS difference reflects an underlying genuine difference in CSS that was masked by retrospective misattribution of deaths to non-cancer causes. In either case, it is important to emphasize that the two populations were highly selected and that the comparison cannot provide evidence as to the relative effectiveness of RC or BST.
Patients who did elect initial BST had high rates of treatment failure, with three-quarters of patients experiencing local or systemic recurrence, most within the first two years. The estimated cystectomy-free survival at five years was only 42%. Thus, the choice to undergo BST often served to delay rather than to prevent the need for cystectomy. It could be argued that delaying cystectomy and preserving an intact bladder, even if temporarily, offers a benefit to quality of life (QoL). However, the benefits of preserving an intact bladder must be weighed against the burden of ongoing intravesical treatments and surveillance, as well as worry about the development of metastatic disease. Interestingly, the recent BRAVO randomized trial showed no difference in a variety of treatment-agnostic QoL measures between patients undergoing cystectomy and receiving intravesical BCG, suggesting that the QoL detriment associated with radical cystectomy may not be significantly worse than that associated with ongoing BST [13]. Our oncologic outcomes in patients undergoing BST are generally poorer than those reported in recent clinical trials, which could be due to less efficacious treatments or differences in the underlying patient populations. This could also be an example of “trial effect”, a phenomenon in which patients enrolled in clinical trials are posited to have better outcomes than patients receiving the same treatments outside of clinical trials. However, the existence of this phenomenon has not been substantiated in the literature [29, 30].
Patients who opt for BST are often averse to undergoing radical cystectomy and inquire about further bladder-conserving options after an initial treatment failure. In our cohort, receipt of ≥2 lines of BST following BCG unresponsive disease was associated with much higher rates of ≥pT3 or pN+ disease than reported in other series of patients undergoing RC after BCG failure [28, 31]. Metastasis-free and cancer-specific survival were not significantly worse among patients undergoing ≥2 lines of BST compared with 1 line of BST or initial RC, but our power to detect differences was limited by a small sample size and a high degree of patient selection. Clinical trial participation was low, with only six out of 89 patients enrolling in a clinical trial at the time of initial BCG failure. Interestingly, a further nine patients enrolled in clinical trials after subsequent treatment failures, suggesting that patients may be more amenable to trial enrollment after multiple intravesical treatment failures.
Limitations
Our study carries the usual limitations of a retrospective, single-institution study. The sample size was comparatively small and reduced our ability to detect differences between clinical groups. The quality of the retrospective data, particularly those derived from external sources, is potentially inconsistent and may contain hidden bias or confounders, particularly with regard to the assignment of comorbidity, metastatic status, and cancer-specific mortality. Furthermore, our study population may be subject to hidden or unaccounted confounders, including selection bias at the time of referral (e.g., referral of more complex or higher-risk patients to our academic center). A shortcoming of this publication, and one shared with much of the literature concerning NMIBC, is the heterogeneity of the underlying patient cohort. The study spans a broad period of time and patients were managed by many different clinicians (including those both within and outside of our institution), who may have had different treatment philosophies or varying access to different treatment options. The initial RC and initial BST cohorts were highly selected both with regard to patient and disease characteristics, and the study should therefore not be interpreted as providing evidence as to the comparative effectiveness of RC and BST.
CONCLUSIONS
Here, we reviewed the outcomes of patients managed at our institution with BCG unresponsive NMIBC according to the US Food and Drug Administration’s 2018 definition, which has served as the basis for the design of numerous clinical trials. A majority of patients opted for initial bladder-sparing treatment (BST), but these patients had high rates of treatment failure. Those who received two or more lines of BST after a subsequent failure had increased risk of adverse pathology should they go on to require cystectomy. Our findings emphasize the degree of patient interest in bladder-sparing options for management of BCG-unresponsive NMIBC and a historic lack of consensus as to optimal management, highlighting the importance of recent and ongoing clinical trials. Ongoing support for and patient enrollment in such trials remains critical for continued progress in this important clinical space.
ACKNOWLEDGMENTS
The authors have no acknowledgements.
FUNDING
The study was funded internally by the University of Texas Southwestern Department of Urology. No external funding source was used.
AUTHOR CONTRIBUTIONS
Conception–J.M.H., V.M., S.L.W., Y.L.
Performance of work–J.M.H., G.C., A.T.
Interpretation of data–J.M.H., Y.L., K.N.
Writing the article–J.M.H., Y.L.
All authors had access to the full data set used in the study.
CONFLICT OF INTEREST
Y.L. is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding its peer-review. Y.L. reports relationships with the following entities: Abbott, Abbvie, Ambu, AstraZeneca, BioCanCell, CAPs Medical, Cepheid, Cleveland Diagnostics, C2I Genomics, Fergene, Ferring Research, FKD, GenomeDx Biosciences, Hitachi, Karl Storz, MDxHealth, Merck, Nanorobotics, Nucleix, Pacific Edge, Photocure, Seattle Genetics, Stimit, Verity Pharmaceuticals, Vessi Medical, Virtuoso Surgical. J.M.H., G.S.C., A.T., K.N., V.M. and S.L.W. report no conflicts.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/BLC-211657.
REFERENCES
[1] | Chang SS , Boorjian SA , Chou R , Clark PE , Daneshmand S , Konety BR , Pruthi R , Quale DZ , Ritch CR , Seigne JD , Skinner EC , Smith ND , McKiernan JM . Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline. J Urol. (2016) ;196: :1021–9. doi:10.1016/j.juro.201606.049. |
[2] | Woldu SL , Bagrodia A , Lotan Y . Guideline of guidelines: Non-muscle-invasive bladder cancer. BJU Int. (2017) ;119: :371–80. doi:10.1111/bju.13760. |
[3] | Babjuk M , Burger M , Compérat EM , Gontero P , Mostafid AH , Palou J , van Rhijn BWG , Rouprêt M , Shariat SF , Sylvester R , Zigeuner R , Capoun O , Cohen D , Escrig JLD , Hernández V , Peyronnet B , Seisen T , Soukup V . European association of urology guidelines on non-muscle-invasive bladder cancer (TaT1 and carcinoma in situ) - 2019 update. Eur Urol. (2019) ;76: :639–57. doi:10.1016/j.eururo.2019.08.016. |
[4] | Böhle A , Jocham D , Bock PR . Intravesical bacillus Calmette-Guerin versus mitomycin C for superficial bladder cancer: A formal meta-analysis of comparative studies on recurrence and toxicity. J Urol. (2003) ;169: :90–5. doi:10.1016/S0022-5347(05)64043-8. |
[5] | Han RF , Pan JG . Can intravesical bacillus Calmette-Guérin reduce recurrence in patients with superficial bladder cancer? A meta-analysis of randomized trials. Urology. (2006) ;67: :1216–23. doi:10.1016/j.urology.2005.12.014. |
[6] | Shelley MD , Kynaston H , Court J , Wilt TJ , Coles B , Burgon K , Mason MD . A systematic review of intravesical bacillus Calmette-Guérin plus transurethral resection vs transurethral resection alone in Ta and T1 bladder cancer. BJU Int. (2001) ;88: :209–16. doi:10.1046/j.1464-410X.2001.02306.x. |
[7] | Shelley MD , Wilt TJ , Court J , Coles B , Kynaston H , Mason MD . Intravesical bacillus Calmette-Guérin is superior to mitomycin C in reducing tumour recurrence in high-risk superficial bladder cancer: A meta-analysis of randomized trials. BJU Int. (2004) ;93: :485–90. doi:10.1111/j.1464-410X.2003.04655.x. |
[8] | Sylvester RJ , Van der Meijden APM , Lamm DL . Intravesical bacillus Calmette-Guerin reduces the risk of progression in patients with superficial bladder cancer: A meta-analysis of the published results of randomized clinical trials. J Urol. (2002) ;168: :1964–70. doi:10.1016/S0022-5347(05)64273-5. |
[9] | Matulay JT , Li R , Hensley PJ , Brooks NA , Narayan VM , Grossman HB , Navai N , Dinney CPN , Kamat AM . Contemporary outcomes of patients with nonmuscle-invasive bladder cancer treated with bacillus calmette-Guérin: Implications for clinical trial design. J Urol. (2021) ;205: :1612–21. doi:10.1097/ju.0000000000001633. |
[10] | Ghoneim MA , Abdel-Latif M , El-Mekresh M , Abol-Enein H , Mosbah A , Ashamallah A , El-Baz MA . Radical cystectomy for carcinoma of the bladder: 2,720 consecutive cases 5 years later. J Urol. (2008) ;180: :121–7. doi:10.1016/j.juro.2008.03.024. |
[11] | Madersbacher S , Hochreiter W , Burkhard F , Thalmann GN , Danuser H , Markwalder R , Studer UE . Radical cystectomy for bladder cancer today - A homogeneous series without neoadjuvant therapy. J Clin Oncol. (2003) ;21: :690–6. doi:10.1200/JCO.2003.05.101. |
[12] | Stein JP , Lieskovsky G , Cote R , Groshen S , Feng AC , Boyd S , Skinner E , Bochner B , Thangathurai D , Mikhail M , Raghavan D , Skinner DG . Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1,054 patients. J Clin Oncol. (2001) ;19: :666–75. doi:10.1200/JCO.2001.19.3.666. |
[13] | Catto JWF , Gordon K , Collinson M , Poad H , Twiddy M , Johnson M , Jain S , Chahal R , Simms M , Dooldeniya M , Bell R , Koenig P , Conroy S , Goodwin L , Noon AP , Croft J , Brown JM . Radical cystectomy against intravesical BCG for high-risk high-grade nonmuscle invasive bladder cancer: Results from the randomized controlled BRAVO-feasibility study. J Clin Oncol. (2021) ;39: :202–14. doi:10.1200/JCO.20.01665. |
[14] | Hassler MR , Shariat SF , Soria F . Salvage therapeutic strategies for bacillus Calmette-Guerin failure. Curr Opin Urol. (2019) ;29: :239–46. doi:10.1097/MOU.0000000000000593. |
[15] | Steinberg RL , Thomas LJ , O’Donnell MA . Bacillus calmette-guérin (BCG) treatment failures in non-muscle invasive bladder cancer: What truly constitutes unresponsive disease. Bladder Cancer. (2015) ;1: :105–16. doi:10.3233/BLC-150015. |
[16] | Steinberg RL , Thomas LJ , Mott SL , O’Donnell MA . Bacillus calmette-Guérin (BCG) treatment failures with non-muscle invasive bladder cancer: A data-driven definition for BCG unresponsive disease. Bladder Cancer. (2016) ;2: :215–24. doi:10.3233/BLC-150039. |
[17] | U.S Food and Drug Administration, BCG-Unresponsive Nonmuscle Invasive Blader Cancer: Developing Drugs and Biologics for Treatment Guidance for Industry. (2018) . https://www.fda.gov/media/101468/download (accessed March 2, 2021). |
[18] | Balar AV , Kamat AM , Kulkarni GS , Uchio EM , Boormans JL , Roumiguié M , Krieger LEM , Singer EA , Bajorin DF , Grivas P , Seo HK , Nishiyama H , Konety BR , Li H , Nam K , Kapadia E , Frenkl T , de Wit R . Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. (2021) ;22: :919–30. doi:10.1016/S1470-2045(21)00147-9. |
[19] | Boorjian SA , Alemozaffar M , Konety BR , Shore ND , Gomella LG , Kamat AM , Bivalacqua TJ , Montgomery JS , Lerner SP , Busby JE , Poch M , Crispen PL , Steinberg GD , Schuckman AK , Downs TM , Svatek RS , Mashni JJ , Lane BR , Guzzo TJ , Bratslavsky G , Karsh LI , Woods ME , Brown G , Canter D , Luchey A , Lotan Y , Krupski T , Inman BA , Williams MB , Cookson MS , Keegan KA , Andriole GLJ , Sankin AI , Boyd A , O’Donnell MA , Sawutz D , Philipson R , Coll R , Narayan VM , Treasure FP , Yla-Herttuala S , Parker NR , Dinney CPN . Intravesical nadofaragene firadenovec gene therapy forBCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. (2020) ;22: :107–17. doi:10.1016/S1470-2045(20)30540-4. |
[20] | Chang S , Chamie K , Hidalgo M , Kramolowsky E , Sexton W , Reddy S , -Shiong Patrick Soon. PLLBA-01 Final clinical results of pivotal trial of il-15rαfc superagonist n-803 with bcg in bcg-unresponsive non-muscle invasive bladder cancer (nmibc) cis and papillary cohorts. J Urol. (2022) ;207: :e1047. doi:10.1097/JU.0000000000002671.01. |
[21] | Shore N , O’Donnell M , Keane T , Jewett MAS , Kulkarni GS , Dickstein R , Wolk F , Dunshee C , Belkoff L , Dillon RL , Cizeau J , Kassouf W . Phase 3 results of Vicinium in BCG-unresponsive non-muscle invasive bladder cancer. J Urol. (2020) ;203: :e72. doi:10.1097/JU.0000000000000823.02. |
[22] | Zlotta AR , Fleshner NE , Jewett MA . The management of BCG failure in non-muscle-invasive bladder cancer: An update. Can Urol Assoc J. (2009) ;3: :199–205. doi:10.5489/cuaj.1196. |
[23] | Schemper M , Smith TL . A note on quantifying follow-up in studies of failure time. Control Clin Trials. (1996) ;17: :343–6. doi:10.1016/0197-2456(96)00075-X. |
[24] | Zhou Z , Rahme E , Abrahamowicz M , Pilote L . Survival bias associated with time-to-treatment initiation in drug effectiveness evaluation: A comparison of methods. Am J Epidemiol. (2005) ;162: :1016–23. doi:10.1093/aje/kwi307. |
[25] | Catalona WJ , Hudson MA , Gillen DP , Andriole GL , Ratliff TL . Risks and benefits of repeated courses of intravesical bacillus Calmette-Gurerin therapy for superficial bladder cancer. J Urol. (1987) ;137: :220–4. doi:10.1016/S00225347(17)43959-0. |
[26] | Di Lorenzo G , Perdonà S , Damiano R , Faiella A , Cantiello F , Pignata S , Ascierto P , Simeone E , De Sio M , Autorino R . Gemcitabine versus bacille Calmette-Guérin after initial bacille Calmette-Guérin failure in non-muscle-invasive bladder cancer: A multicenter prospective randomized trial. Cancer. (2010) ;116: :1893–900. doi:10.1002/cncr.24914. |
[27] | Steinberg RL , Thomas LJ , Brooks N , Mott SL , Vitale A , Crump T , Rao MYA , Daniels MJ , Wang J , Nagaraju S , DeWolf WC , Lamm DL , Kates M , Hyndman ME , Kamat AM , Bivalacqua TJ , Nepple KG , O’Donnell MA , O’Donnell MA . Multi-institution evaluation of sequential gemcitabine and docetaxel as rescue therapy for nonmuscle invasive bladder cancer. J Urol. (2019) ;203: :902–9. doi:10.1097/ju.0000000000000688. |
[28] | Soloway MS , Hepps D , Katkoori D , Ayyathurai R , Manoharan M . Radical cystectomy for BCG failure: Has the timing improved in recent years? BJU Int. (2011) ;108: :182–5. doi:10.1111/j.1464-410X.2010.09830.x. |
[29] | Vist GE , Hagen KB , Devereaux PJ , Bryant D , Kristoffersen DT , Oxman AD . Systematic review to determine whether participation in a trial influences outcome. BMJ. (2005) ;330: :1175. doi:10.1136/bmj.330.7501.1175. |
[30] | Peppercorn JM , Weeks JC , Cook EF , Joffe S . Comparison of outcomes in cancer patients treated within and outside clinical trials: Conceptual framework and structured review. The Lancet. (2004) ;363: :263–70. doi:10.1016/S0140-6736(03)15383-4. |
[31] | Nieder AM , Simon MA , Kim SS , Manoharan M , Soloway MS . Radical cystectomy after bacillus Calmette-Guérin for high-risk Ta, T1, and carcinoma in situ: Defining the risk of initial bladder preservation. Urology. (2006) ;67: :737–41. doi:10.1016/j.urology.2005.10.012. |


