
Systematic Review and Meta-Analysis on the Role of Perioperative Blood Transfusion in Patients Undergoing Radical Cystectomy for Urothelial Carcinoma
Abstract
BACKGROUND:
Radical cystectomy (RC) is the standard of care in patients with muscle-invasive bladder cancer. The impact of perioperative red blood cell (RBC) transfusion on oncological outcomes after RC is not clearly established as the existing publications show conflicting results.
OBJECTIVES:
The aim of this systematic review and meta-analysis was to investigate the prognostic role of perioperative RBC transfusion on oncological outcomes after RC.
METHODS:
Systematic online search on PubMed was conducted, based on PRISMA criteria for publications reporting on RBC transfusion during RC. Publications with the following criteria were included: (I) reported data on perioperative blood transfusion; (II) Reported Hazard ratio (HR) and 95% -confidence interval (CI) for the impact of transfusion on survival outcomes. Primary outcome was the impact of perioperative RBC transfusion on recurrence-free survival (RFS), cancer-specific survival (CSS) and overall survival (OS). Risk of bias assessment was performed using Newcastle-Ottawa Scale. Statistical analysis was performed using Revman 5.4 software.
RESULTS:
From 27 primarily identified publications, 19 eligible articles including 22897 patients were selected. Perioperative RBC transfusion showed no impact on RFS (Z = 1.34; p = 0,18) and significant negative impact on CSS (Z = 2.67; p = 0.008) and OS (Z = 3.22; p = 0.001). Intraoperative RBC transfusion showed no impact on RFS (Z = 0.58; p = 0.56) and CSS (Z = 1.06; p = 0.29) and OS (Z = 1.47; p = 0.14).
Postoperative RBC transfusion showed non-significant trend towards improved RFS (Z = 1.89; p = 0.06) and no impact on CSS (Z = 1.56; p = 0.12) and OS (Z = 0.53 p = 0.60).
CONCLUSION:
In this meta-analysis, we found perioperative blood transfusion to be a significant predictor only for worse CSS and OS but not for RFS. This effect may be determined by differences in tumor stages and patient comorbidities for which this meta-analysis cannot control due to lack of respective raw data.
INTRODUCTION
Bladder cancer (BC) is the 11th most common diagnosed cancer worldwide, with approximately 75% of cases accounting for non-muscle invasive disease [1]. Radical cystectomy (RC) is the mainstay of treatment in patients with muscle-invasive bladder cancer (MIBC) and in those with non-muscle invasive bladder cancer (NMIBC) at (very) high risk of recurrence [1, 2]. For patients, unfit for RC or opting for bladder preservation, trimodal therapy is a further therapeutic option [1, 2].
Patient age and performance status (including comorbidities), tumour stage, perioperative chemotherapy, resection margins, extent of lymphadenectomy, surgeon and hospital volume are accepted outcome predictors in patients with urothelial carcinoma undergoing RC [1–5].
A number of previously published studies examined the prognostic role of perioperative blood transfusion (PBT) on outcome after RC [6–25]. Some studies reported a significant negative impact on oncological outcomes [6, 7, 10–12, 21, 23]. In contrast, other studies could not confirm this hypothesis in their populations [9, 13, 14, 16, 18–20, 22, 24]. Some authors demonstrated that the choice of statistical model might significantly influence the results [16]. Other studies postulated that only intraoperative blood transfusion has a significant impact on the oncological outcomes [6, 8, 18]. Thus, the existing evidence remains controversial. Because of the substantial clinical relevance of this issue, we performed a systematic review and meta-analysis of the existing studies on the impact of PBT on oncological outcomes after RC in patients with BC.
METHODS
Search strategy
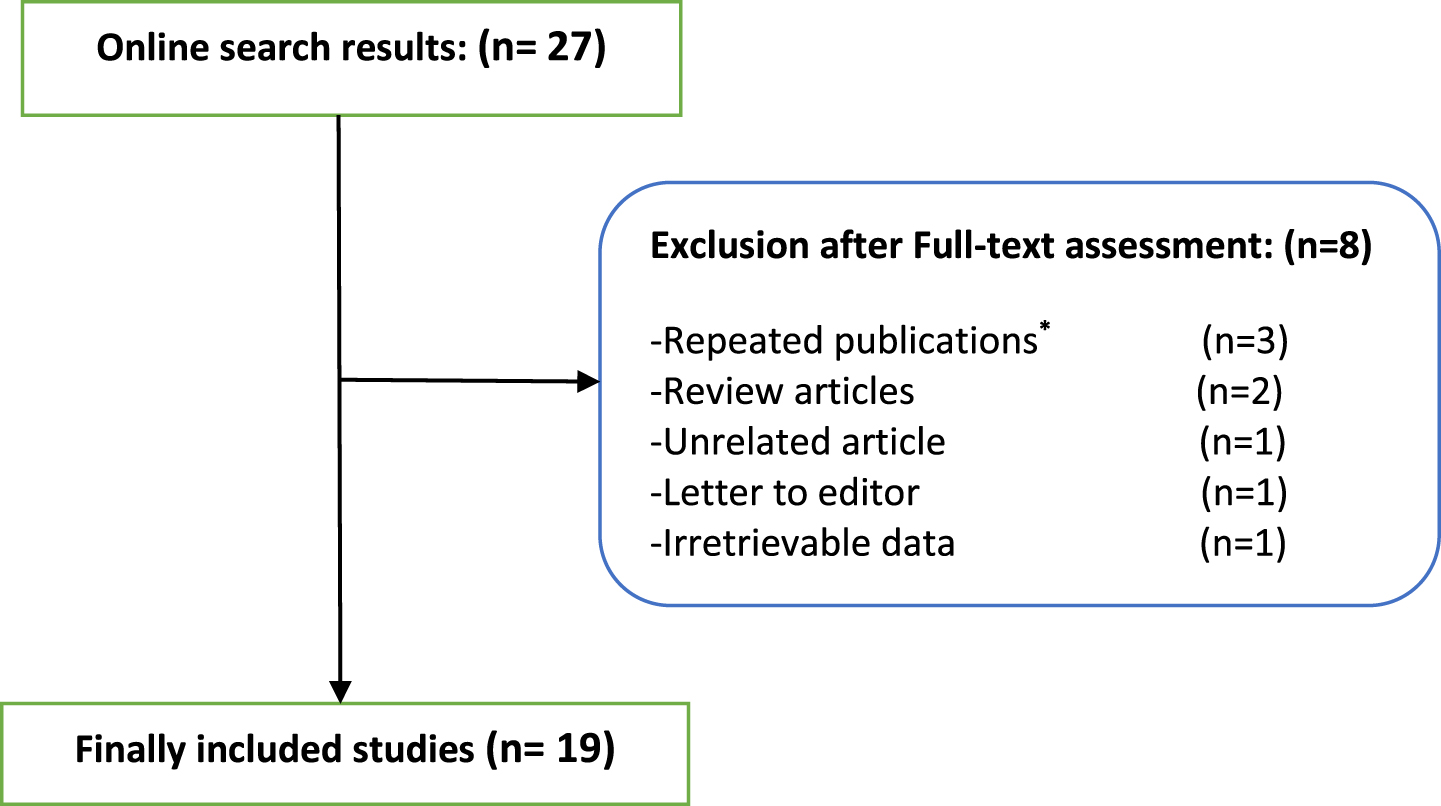
Based on PRISMA statement [26], two authors (MK, LE) conducted independent systematic online search in PubMed database [27]. The following keywords were used for search: radical cystectomy, bladder cancer, urothelial carcinoma, blood transfusion, outcome, perioperative. The retrieved results by the two authors underwent full-text assessment. Suitable publications were subjected to full-text assessment including a manual search in their reference lists. In case of any discrepancies on literature findings between both authors, a third author was consulted (GG). Publications, which met the following criteria, were included: (I) reported data on perioperative blood transfusion, (II) reported Hazard ratio (HR) and 95% -confidence interval (CI) for the impact of PBT on survival outcomes or presence of Kaplan-Meier curve for survival outcome based on the presence or absence of PBT. Publications which met one of the following criteria were excluded: (I) absence of HR and 95% CI, or Kaplan-Mayer curve, (II) review articles, (III) editorial comments or letters to editor, (IV) repeated publications on the same cohort (unless complementary data could be extracted without double counting of the patients in the total number of this study. PBT was defined as transfusion of whole blood, or packed red blood cells 24 hours before, or during surgery or, postoperatively before discharge of the patient. The CONSORT diagram for the selection process is present at Fig. 1.
Fig. 1
CONSORT diagram for the selection process of the included studies. *Repeated publications were added when complementary data was present in 2 articles, without double counting the cohort in the total number of patients.
Data extraction
The following variables were extracted independently by three authors (MK, OF, LE): number of the patients who underwent RC, gender, age, time interval of the study cohort, duration of follow up, recurrence free survival (RFS), cancer specific survival (CSS), overall survival (OS). Hazard ratio (HR) and 95% -confidence interval (CI) for the following factors based on multivariate analysis. HR and 95% CI for the impact of perioperative transfusion on OS were extracted from Kaplan Meier curves using Tierney’s method [28].
Outcome measures
The primary outcome of this analysis was the impact of perioperative, intraoperative and postoperative blood transfusion on RFS, CSS and OS after RC.
Statistical analysis
This meta-analysis was conducted using Review Manager (RevMan) software version 5.4 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen). Log HR and standard error (SE) of the extracted HR were used in the pooled analysis. Fixed effect model was used when I2 value was less than 50% to minimize the effect of heterogeneity between the included studies.
Risk of bias assessment
Newcastle-Ottawa Scale [29] was used to assess the risk of bias of the included studies. The studies were categorized as having low, moderate or high risk of bias based on the following scores, ≥7–9, 4–6, <4 respectively.
RESULTS
Search results and patient criteria
In this systematic review and meta-analysis, 19 studies were finally included [6–24]. A CONSORT diagram is provided in (Fig. 1) to demonstrate the selection process.
A total number of 22893 patients (17963 men, 78% and 4704 women, 22%) underwent RC and were involved in the pooled analysis. 9690 (42%) patients received perioperative blood transfusion. The summary of the included studies is provided in Table 1.
Table 1
Newcastle-Ottawa Scale for risk of bias assessment of the included studies (scores≥7-9, 4-6, < 4 are considered as low, intermediate, and high risk, respectively)
| Study | Type* | Selection | Comparability | Outcome | Overall | |||||
| Represen-tativeness of exposed cohort | Selection of non-exposed | Ascertain-ment of exposure | Outcome not present at start | Assess-ment of outcome | Adequate follow-up length | Adequacy of follow-up | ||||
| Abel 2014 [6] | R,M | * | * | * | * | * | * | 6/9 | ||
| Buchner 2017 [7] | R,S | * | * | * | * | * | * | * | 7/9 | |
| Chalfin 2016 [8] | R,S | * | * | * | * | ** | * | * | 8/9 | |
| Chipollini 2017 [9] | R,S | * | * | * | * | * | * | * | * | 8/9 |
| Furrer 2018 [10] | R,S | * | * | * | * | ** | * | * | * | 9/9 |
| Gerschman 2016 [11] | R,S | * | * | * | * | ** | * | * | * | 9/9 |
| Gierth 2014 [12] | R,S | * | * | * | * | * | * | * | * | 8/9 |
| Kluth 2014 [13] | R,M | * | * | * | * | * | * | * | 7/9 | |
| Lee 2015 [14] | R,S | * | * | * | * | * | * | * | * | 8/9 |
| Linder 2013 [15] | R,S | * | * | * | * | * | * | * | 7/9 | |
| Morgan 2013 [16] | R,S | * | * | * | * | * | * | * | 7/9 | |
| Moschini 2015 [18] | R,S | * | * | * | * | ** | * | * | * | 9/9 |
| Moschini 2016 [17] | R,S | * | * | * | * | * | * | * | * | 8/9 |
| Rivas 2016 [19] | R,S | * | * | * | * | ** | * | 7/9 | ||
| Sadeghi 2012 [20] | R,S | * | * | * | * | * | * | * | * | 8/9 |
| Siemens 2017 [21] | R,S | * | * | * | * | * | * | * | * | 8/9 |
| Soubra 2015 [22] | R,LDB | * | * | * | * | * | * | 6/9 | ||
| Syan-Bhanvadia 2017 [23] | R,S | * | * | * | * | * | * | * | 7/9 | |
| Vetterlein 2018 [24] | R,M | * | * | * | * | * | * | * | 7/9 | |
*Types of the studies: R = Retrospective, M = Multi-institutional, S = Single-institutional, LDB = Large Data Base based study.
All the included studies were categorized as low risk of bias, but only one, demonstrated intermediate risk [22]. (see Table 2)
Table 2
Overview of studies included in the meta-analysis
| Study | Period | Sample size (PBT/no PBT) | Follow-up | Result | Differences between groups | Other issues |
| Abel, 2014 [6] | 2003–2012 | 360 (241/119) | 18.7 m | Sign. impact on RFS, CSS, OS | Sign. worse tumour stage, ECOG and age in PBT group | Patients with CTx excluded, median V = 2 U |
| Buchner, 2017 [7] | 2004–2014 | 722 (317/405) | 26 m | Sign. impact on CSS | Unclear | Only 13 pts. received CTx, median V = 2 U, sign. dose-dependency |
| Chalfin, 2016 [8] | 2010–2013 | 115 (65/50) | 7.8 m | Sign. impact on CSS and OS only for iop BT | Unclear | Cisplatin-based NAC in all patients, V > 2 U with sign. impact on morbidity |
| no impact for peri- or postoperative BT | ||||||
| Chipollini, 2017 [9] | 2008–2015 | 1026 (341/685) | 27.5 m | No sign. impact on RFS, CSS and OS | Sign. worse tumour stage in PBT group | Different NAC, median V = 2 U |
| Furrer, 2018 [10] | 2000–2015 | 885 (267/618) | 39 m | Sign. impact on RFS, CSS and OS | Sign. worse tumour stage and comorbidities in PBT group | 30% of pts. RBC + FFP, NAC and AC, median V = 2 U |
| Gerschmann, 2016 [11] | 1980–2008 | 2086 (1263/823) | 11 y | Sign. impact on CSS and OS, no sign. impact on RFS | Unclear | 14,7 % of pts. with NAC and/or AC, V not provided |
| Gierth, 2014 [12] | 1995–2010 | 350(219/131) | 70.1 m | Sign. impact on RFS and OS | Sign. worse tumour stage in PBT group | No NAC and no data for AC in included pts., sign. dose-dependency (1-2 vs. > 2 U) |
| Kluth, 2014 [13] | 1998–2010 | 2895 (1128/1767) | 36.1 m | No sign. impact on RFS, CSS and OS | Sign. worse tumour stage in PBT group | No NAC and 23% AC in included pts. |
| V not provided | ||||||
| Lee, 2015 [14] | 1991–2012 | 432 (315/117) | 35 m (pts. with PBT) | No sign. impact on CSS and OS; sign. impact on OS (but not CSS), if PBT > 4 U | Comparable | 11% NAC and 25% AC in included pts., median V = 4 U, sign. impact on OS (but not CSS) if PBT > 4 U |
| 44 m (pts. with no PBT) | ||||||
| Lindner, 2013 [15] | 1980–2005 | 2060 (1279/781) | 10.9 y | Sign. impact on RFS, CSS and OS | Sign. worse tumour stage, ECOG, age in PBT group | 6% NAC, 8% AC, median V = 2 U, sign. dose-dependency |
| Morgan, 2013 [16] | 2000–2008 | 777 (323/454) | 25 m | Sign. impact and no sign impact on OS in 2 multivariate models | Sign. worse tumour stage, comorbidities, age in PBT group | 3% NAC, pts. with preop. RT excluded,no data on AC, median V = 2 U, sign. dose-dependency (1-2 vs. 3-4 vs. > =5) |
| Moschini, 2015 [18] | 1990–2013 | 1490 (580/910) | 110 m | Sign. impact on RFS, CSS and OS for iop or iop + pop BT | Comparable | 3% NAC, 26% AC, V not provided |
| no impact for pop BT only | ||||||
| Moschini, 2015 [30] | – | – | – | No sign. impact on CSS and OS for PBT, only sign. impact in pat. without anemia | Comparable | 3% NAC, 26% AC, V not provided |
| Rivas, 2016 [19] | 2005–2012 | 218 (35/183) | No sign. impact on OS | Sign. worse tumour stage in PBT group | 37% “perioperative CT”, V not documented | |
| Sadeghi, 2012 [20] | 1989–2010 | 638 (209/429) | 25.5 m | No sign. impact on CSS and OS in MVA | Sign. worse tumour stage in PBT group | NAC 12%, AC 12%, median V = 2 U, no sign. dose-dependency (1 vs. 2 vs. > = 3) |
| Siemens, 2017 [21] | 2000–2008 | 2593 (1608/985) | Sign. impact on CSS and OS | Sign. worse tumour stage, comorbidity, age in PBT group | AC 17%, pts. with NAC and preop. radiation excluded, V not provided | |
| Soubra, 2015 [22] | 1992–2009 | 5462 (1139/4323) | 21 m | No sign impact on CSS and OS | Comparable, with exception of sign. age difference | Pts. with NAC, AC and postop. radiation included. NAC in 5–18% depending on the year of surgery (1992-2008) |
| V not documented | ||||||
| Syan- Bhanvadia, 2017 [23] | 2010–2014 | 173 (46/127) | 3.1 y | Sign. impact on RFS and OS | Sign. worse comorbidity and tumour stage in PBT group | 34% NAC, 10% AC, median V = 2 |
| Vetterlein, 2018 [24] | 2011 | 611 (315/296) | 26 m | No sign. impact on RFS, CSS and OS | Sign. worse age, comorbidity and tumour stage in PBT group | 2% NAC, 18% AC, median V = 2 U |
Abbreviations: RFS – recurrence-free survival, CSS – cancer-specific survival, OS – overall survival, CT – chemotherapy, NAC – neoadjuvant chemotherapy, AC – adjuvant chemotherapy, V – volume of transfusion, U – unit, PBT – perioperative blood transfusion, MVA – multivariate analysis, iop – i ntraoperative, pop – postoperative, m – months, y – years, and pts. – patients.
Impact of transfusion on RFS
Analysis of the impact of perioperative blood transfusion on RFS was conducted on 6 studies [10, 11, 13, 15, 23, 24], including 8710 patients. It displayed a trend towards higher risk of disease recurrence, however no significant impact (z = 1.34, p = 0.18) was found (Fig. 2 a).
Fig. 2
Impact of RBC transfusion on RFS in peri-, intra- and postoperative setting.
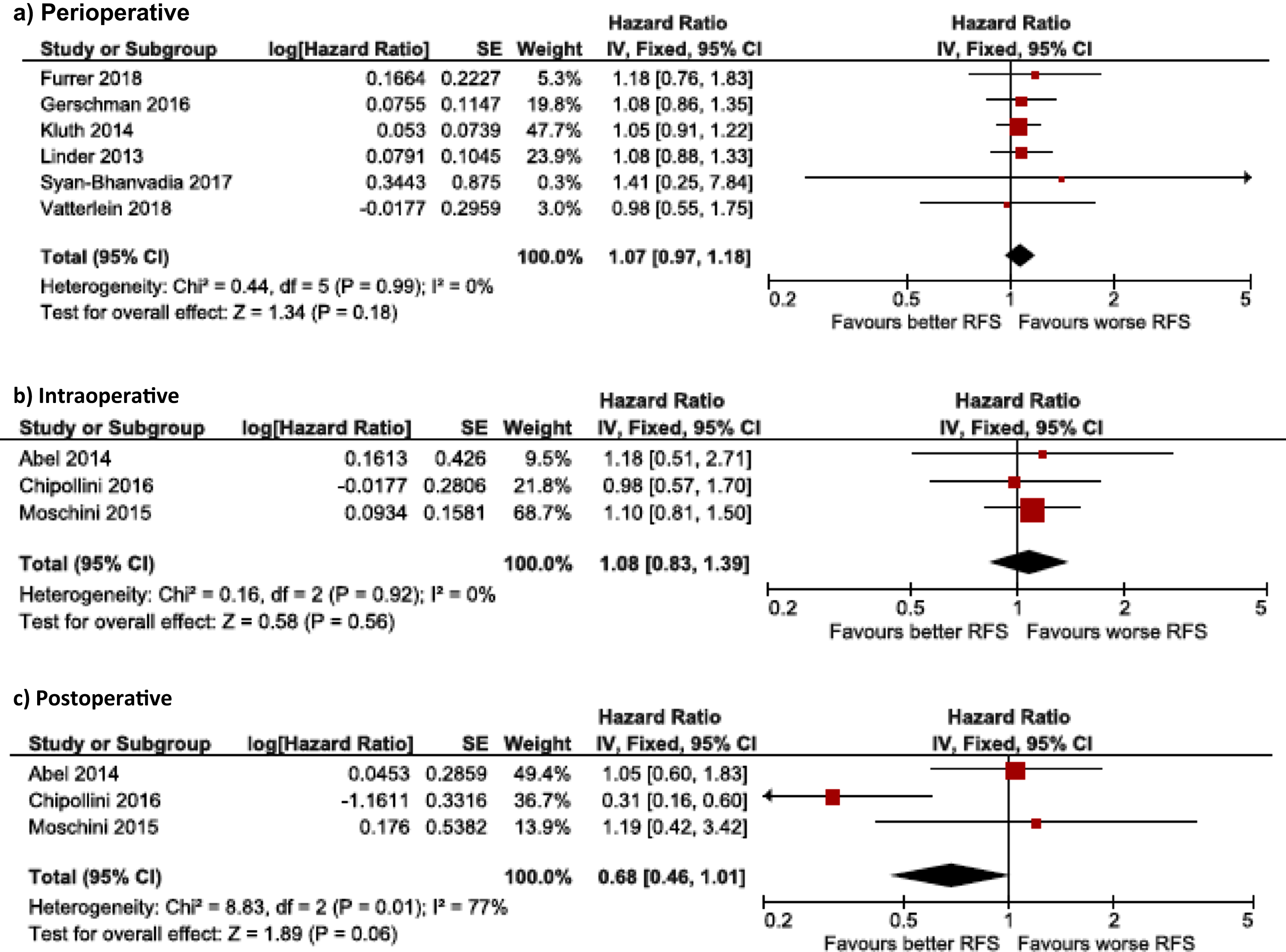
Analysis of the impact of intraoperative and postoperative transfusion, separately, was conducted from 3 studies [6, 9, 17, 30], including 2876 patients. Intraoperative transfusion displayed no significant impact on RFS (z = 0.58, p = 0.56), while postoperative transfusion displayed non-significant trend towards better RFS (z = 1.89, p = 0.06). (Fig. 2, b and c,).
Impact of perioperative transfusion on CSS
11 studies [7, 8, 10, 11, 13, 15, 18, 20–22, 24] were involved in the analysis of PBT impact on CSS including 17851 patients. It significantly displayed worse CSS (z = 2.67, p = 0.008) (Fig. 3 a).
Fig. 3
Impact of RBC transfusion on CSS in peri-, intra- and postoperative setting.
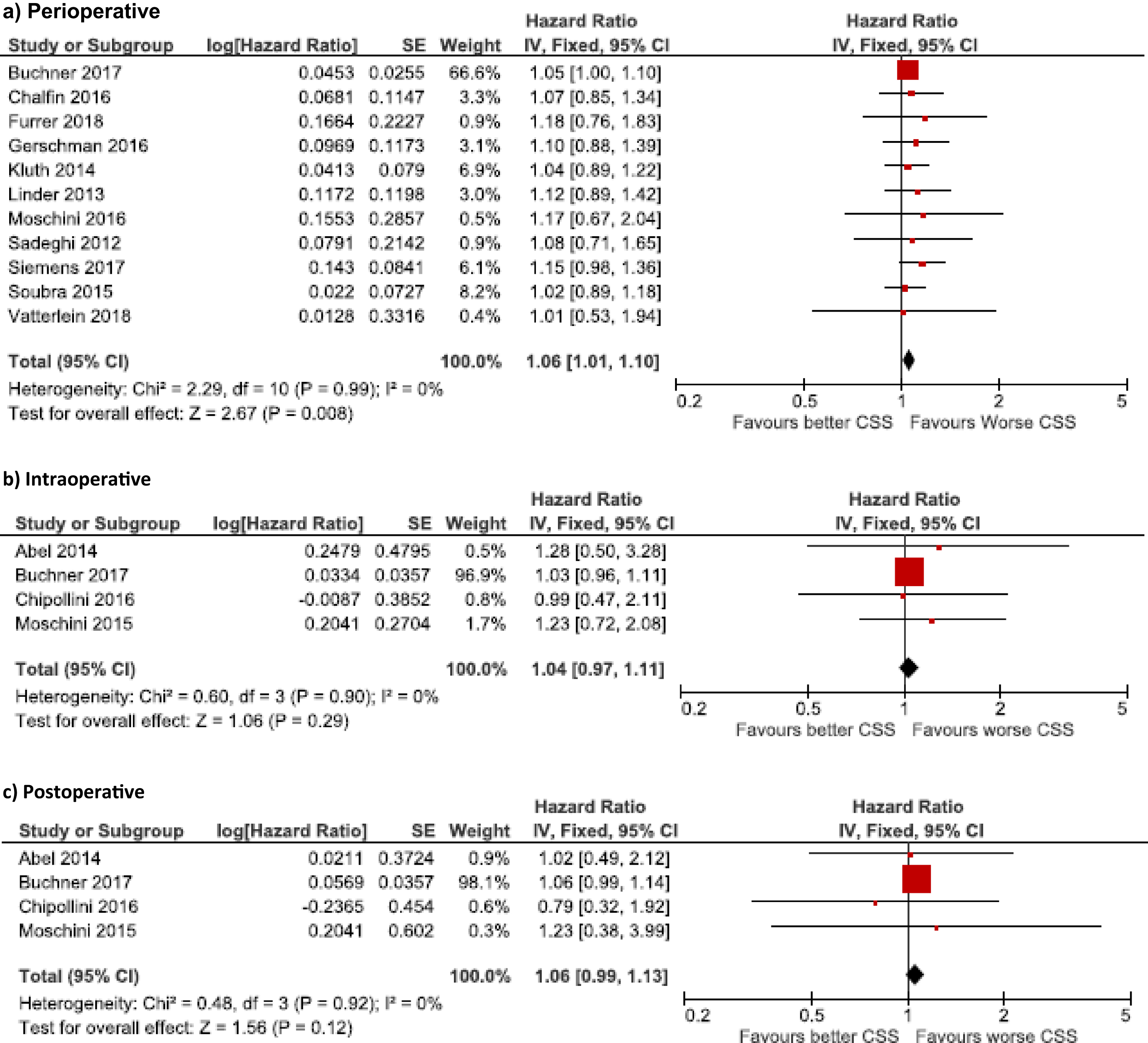
4 studies with 3598 patients were included in the analysis of the impact of intraoperative and postoperative transfusion [6, 7, 9, 17, 30]. Both displayed no significant impact on CSS (z = 1.06, p = 0.29 & z = 1.56, p = 0.12, respectively) (Fig. 3 b and c,).
Impact of transfusion on OS
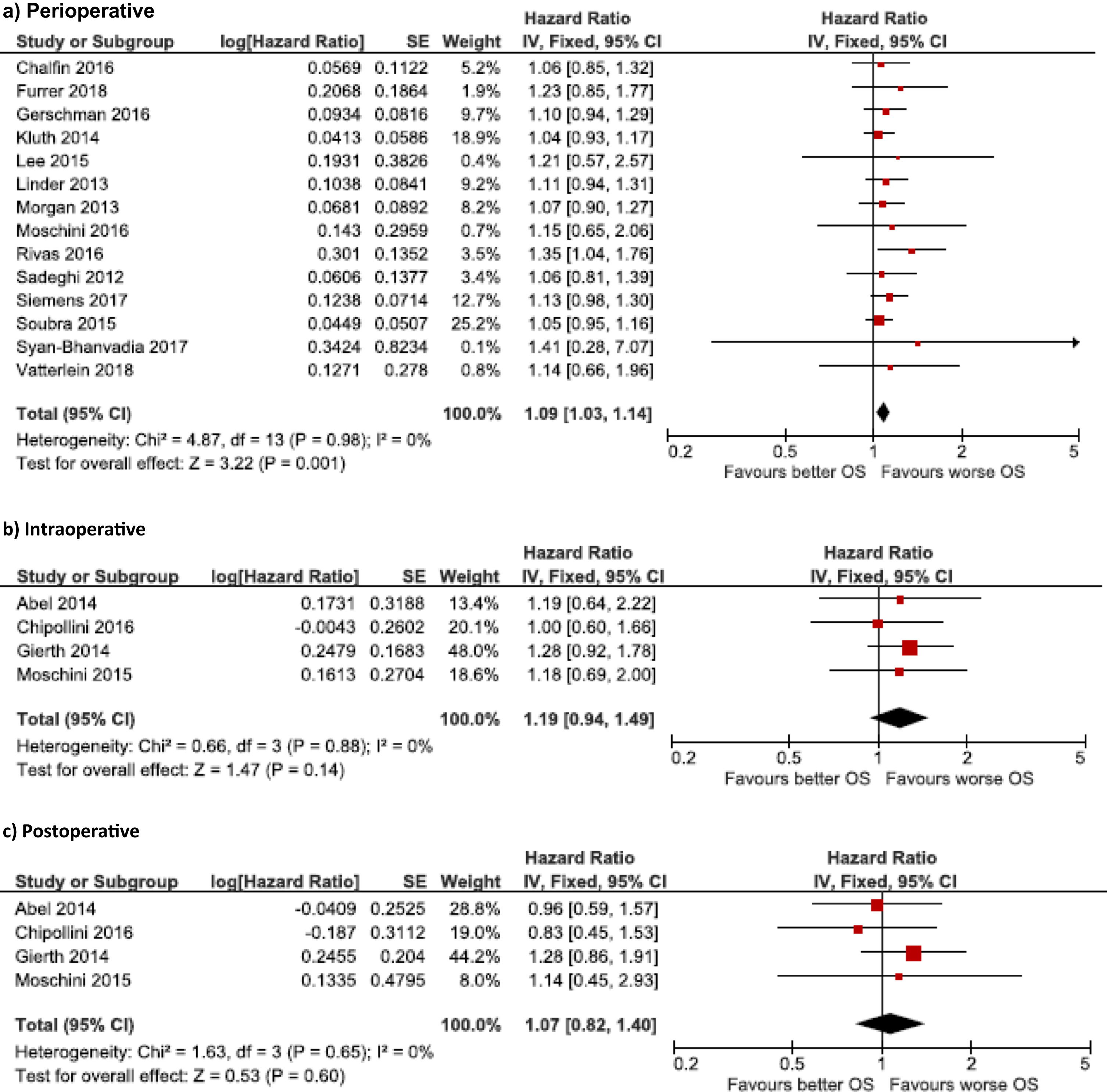
For perioperative transfusion impact on OS, 14 studies including 20439 patients were included in the analysis [8, 10, 11, 13–16, 18–24]. Significant negative impact on OS was detected (z = 3.22, p =0.001), (Fig. 4 a).
Analysis from 4 studies with 3226 patients [6, 9, 12, 17, 30] for the effect of intraoperative transfusion displayed no significant impact on OS (z = 1.47, p = 0.14). From the same former 4 studies, postoperative transfusion displayed almost no impact on OS (z = 0.53, p = 0.60), (Fig. 4, b and c).
Fig. 4
Impact of RBC transfusion on OS in peri-, intra- and postoperative setting.
DISCUSSION
The impact of PBT on outcomes has been initially investigated many years ago. In 1973, Opelz et al observed the beneficial effect of allogenic blood transfusion (BT) on kidney transplants, and suggested immunomodulatory effects [31]. This beneficial effect (preventive effect on disease recurrence) was also observed in patients with Crohn‘ s disease [32–34], although later studies could not confirm it [35, 36]. Other studies postulated a possible unfavorable effect of perioperative BT on the course of oncological diseases [37–39]. Various study groups showed that PBT exerts a negative effect on patients with some cancer entities. The negative effect of PBT on oncological outcome has been observed for oesophageal [40], gastric [41], primary and metastatic colorectal [42–44], hepatocellular [45], pancreatic [46] and lung [47] cancer, as well. Yet, this effect could not be observed for other cancer types like breast cancer [48], cervical cancer [49] or prostate cancer [50]. For BC conflicting results have been published over the last twenty years. We tried to identify all the relevant publications on this issue and performed our systematic search without time frame. Among 27 publications which met our inclusion criteria, 8 were excluded for above mentioned reasons and 19 were finally included in the analysis.
The study of Jahnson et al. [25] seems to be the first one which addressed the impact of PBT on oncological outcomes after RC for BC. The authors did not observe an adverse impact of the number of units (< 6 vs. ≤6) of packed red blood cells (RBC) on oncological outcomes. This study was excluded for three reasons. First, there was no group without BT as comparator. Second, the definition of perioperative transfusion included the time frame of two weeks preoperatively to 4 weeks postoperatively and third, the majority of patients received neoadjuvant radiation therapy, which is not supported by international guidelines for many years [1].
Wang et al. [51] published 2015 the first systematic review and meta-analysis concerning impact of BT on oncological outcome after RC. The analysis included 7080 patients from 6 retrospective studies (all but one multicenter) with intermediate to high methodological quality (NOS≥6) of the period from 2012 to 2014. The authors could demonstrate a significant negative impact of PBT on RFS (based on 3 studies), CSS (based on 4 studies) and OS (based on 6 studies).
Cata et al. [52] published 2016 the second systematic review and meta-analysis to this topic with 8 retrospective studies (3 additional studies compared to above mentioned review of Wang et al.), that included a total of 15 655 patients and were published between 2012 and 2015. All the included studies were retrospective with moderate to good methodological quality (NOS≥7) including also one multicenter study. A significant negative impact of PBT on RFS (based on 5 studies), CSS (based on 7 studies) and OS (based on 8 studies) could be demonstrated.
In our review, we included 19 studies published between 2012 and 2018. All the studies from both previous reviews were included and the additional 11 studies were identified. To our knowledge, we included all the studies of the PubMed database, suitable for meta-analysis and dealing with perioperative BT in RC patients, with a total of 22897 patients.
All the included publications were retrospective, 16 as single-center [7–12, 14–23, 30] and three as multi-center [6, 13, 24] studies. Of note, no prospective studies were identified. The included studies showed relevant heterogeneity. Most studies defined perioperative blood transfusion as administration of blood cells either intra- and/or postoperatively. Sadeghi et al included also patients with preoperative blood transfusion [20]. The definition of “postoperative” was in the majority of studies between surgery and discharge. Furrer et al included patients with blood transfusion within 24 h after surgery only [10].
Ten of 19 selected studies found a significant negative impact of BT on CSS and/or OS (Table 1) [6, 7, 10–12, 15, 16, 18, 21, 23]. Two of these studies found this effect only in intraoperative (or intraoperative + postoperative) setting [6, 18], and not for perioperative or only postoperative blood transfusion. One of these studies [16] that used two different models of multivariate analysis found a significant impact of PBT on outcome in one model but could not confirm it in another model. In 7 of 10 studies the blood transfusion group had significantly worse tumor stage and/or age and comorbidities [6, 10, 12, 15, 16, 21, 23]. In 2 studies the difference in age, comorbidities and tumor stage between two groups was not clear [7, 11] and in only one study the groups were similar [18].
Eight of 19 studies found no significant impact of PBT on oncological outcomes in patients with RC [9, 13, 14, 18–20, 22, 24]. The study of Moschini et al found a significant impact of perioperative blood transfusion only for patients without preoperative anemia [18].
In the pooled analysis on a relevant amount of patients for perioperative blood transfusion we could not confirm a significant negative effect on RFS, which is new and deviates from the results of two prior meta-analyses [51, 52]. We also observed a significant negative impact on CSS and OS for the transfusion in perioperative setting. We tried to identify the impact of timing of the blood transfusion. Based on 4 eligible studies [6, 7, 9, 17, 30] we could not confirm a significant negative impact of intraoperative (with or without postoperative) or postoperative only BT on RFS, CSS and OS. A possible explanation of the significant effect of PBT (which is per definition intra and/or postoperative, as the proportion of patients with preoperative BT in the included studies was negligible) on oncological outcomes and no significant effect of intraoperative only or postoperative only is that the number of studies included in the latter analysis was much lower. The interpretation of the significant impact of PBT might be related to the significantly advanced tumor stage and higher comorbidities that were observed in the majority of included studies, despite the independent outcome effect of PBT in multivariate analyses. Due to lacking of raw data, the propensity matching and/or adjustment for this variables was unfortunately not possible. Other possible previously postulated factors influencing the outcome might be the volume of blood transfusion and the perioperative chemotherapy.
The data concerning the number of RBC units were very heterogeneous among included studies. Many publications provided no data on volume of transfused RBC [11, 13, 17–22]. Some publications reported the average transfused volume of 2 units [6, 9, 10, 15, 23, 24] but did not evaluate the effect of transfusion volume on outcome. Several studies found a volume-associated effect of transfusion but had different cut-offs of 2 [7, 8, 12, 15] and 4 units of RBC [14]. Sadeghi et al. [20] found no influence of transfusion volume on oncological outcome. Thus, due to limited and heterogeneous data on impact of transfusion volume and presence of other confounding factors, it is difficult to make a definitive conclusion on confounding factors.
Perioperative chemotherapy is another issue, influencing oncological outcome and a possible source of bias. The data on neoadjuvant (NAC) and adjuvant (AC) chemotherapy in included studies are summarized in the Table 2. Here we are able to see a substantial variability, with (I) studies, that completely excluded patients with chemotherapy [6], (II) studies, that excluded patients with NAC [12, 13, 21] and (III) studies, in which all the patients received NAC [8]. Other studies included patients with NAC and/or AC in different proportion of patients (s. Table 2), which might also have biased the results.
Furthermore, the regimen of perioperative chemotherapy, preoperative hemoglobin level, complexity of surgery, surgeons experience, intraoperative blood loss, different management and care pathways for administration of RBC in different clinical centers with resulting lack of standardization and evidence-based guidelines may also play an additional role (the indication for perioperative blood transfusion was often based on individual clinicians decision).
Altogether, due to retrospective design and relevant heterogeneity of included studies, our systematic review has significant limitations as outlined above.
Nonetheless, we consider this review to represent the most updated evidence available on the association (but not the causation) between perioperative blood transfusion and oncological outcome of patients undergoing RC.
On the other hand, it is without any doubt that, in case of planed major surgery, the condition of every patient should be optimized (diet improvement, correction of anemia, cardiorespiratory functions, etc.). The preoperative autologous blood preparation should be considered, if possible. Surgery must be performed in experienced centers and the intraoperative blood loss must be minimized as much as possible [53, 54]. Additionally some established perioperative practices, traditionally used in patients, generally refusing blood transfusions, might also be helpful [55, 56].
Importantly, the indication for blood transfusion has changed over the investigated period with increasingly restricted usage of blood transfusions under consideration of individual risks [57–59]. This development was observed in many medical fields. The non-inferiority of restrictive vs. liberal strategy was demonstrated for non-cardiac [58] surgery, hip replacement [64], ICU-patients [66, 67] and patient with gastrointestinal bleeding [68]. In cardiac surgery, the TITRe2 (Transfusion Indication Threshold Reduction) trial raised concerns about the non-inferiority of restrictive transfusion due to statistically significant increase in mortality rates (4.2% in restrictive vs. 2.6% in liberal transfusion arm) [65]. In 2017, Mazer et al. [72]. demonstrated in the TRICS-III (Transfusion Requirements in Cardiac Surgery) trial that enrolled 5,243 adults who underwent cardiac surgery in 19 countries the non-inferiority of restrictive vs. liberal transfusion (composite outcome in 11.4% vs. 12.5% in restrictive and liberal groups respectively). Transfusion thresholds were < 7,5 mg/dL for restrictive group in both above mentioned studies and < 9 or < 9,5 mg/dL for liberal group in the TITRe2 and TRICS-III trial respectively. But despite the relatively high level of evidence, the assessment of transfusion thresholds in patients with acute coronary syndromes is still ongoing (NCT02981407 Trial on Myocardial Ischemia and Transfusion [MINT] trial is still recruiting).
In case of bleeding modern algorithms of bleeding management should be used. The rising popularity achieve today patient blood management programs [60], that may change common practice patterns and reduce the necessity of allogenic perioperative blood transfusion [61–63].
Assuming all these aspects, it is definitely important to perform a new evaluation of practical relevance of this topic, taking modern treatment guidelines of bladder cancer [53], and state-of-the art clinical practice of perioperative transfusion into consideration.
CONCLUSION
This meta-analysis found perioperative blood transfusion to exert an adverse impact on CSS and OS but not for RFS. This effect may be determined by differences in tumor stages and patient comorbidities for which this meta-analysis cannot control due to lack of respective raw data. Further studies, ideally with randomized controlled prospective design are required to address this issue.
ACKNOWLEDGMENTS
None.
FUNDING
The authors report no funding.
AUTHOR CONTRIBUTIONS
M.K. acquisition of data, analysis and interpretation of data, drafting of the manuscript
O.F. analysis and interpretation of data, statistical analysis, drafting of the manuscript,
L.E. acquisition of data, analysis and interpretation of data
T. G. critical revision for important intellectual content
E.X. critical revision for important intellectual content
C.G.S critical revision for important intellectual content
G.G. critical revision for important intellectual content, supervision
ETHICAL CONSIDERATIONS
This study, as a literature review is exempt from any requirement for Institutional Review Board approval. No human or animal research was involved in the elaboration of this manuscript.
CONFLICT OF INTEREST
G.G. is an Editorial Board member of this journal, but was not involved in the peer-review process nor had access to any information regarding its peer-review. M.K., O.F., L.E., T.G., E.X. and C.G.S. have no conflicts of interest concerning the manuscript.
G.G. reports advisory board activities for MSD, Astellas, Ipsen, Bayer, Leo Pharma and receipt of speaker’s honoraria from MSD, Ipsen, Erbe, Pierre Fabre, Roche.
REFERENCES
[1] | Professionals S-O. EAU Guidelines: Muscle-invasive and Metastatic Bladder Cancer [Internet]. c27.10.2020 [updated 2020 Oct 27; cited 2020 Oct 27]. Available from: https://uroweb.org/guideline/bladder-cancer-muscle-invasiveand-metastatic/#11. |
[2] | Professionals S-O. EAU Guidelines: Non-muscle-invasive Bladder Cancer | Uroweb [Internet]. c27.10.2020 [updated 2020 Oct 27; cited 2020 Oct 27]. Available from: https://uroweb.org/guideline/non-muscle-invasive-bladdercancer/. |
[3] | Venkatramani V , Reis IM , Castle EP , Gonzalgo ML , Woods ME , Svatek RS ,et al. Predictors of Recurrence, and Progression-Free and Overall Survival following Open versus Robotic Radical Cystectomy: Analysis from the RAZOR Trial with a 3-Year Followup. The Journal of Urology (2020) ; 203: :522–29. |
[4] | Madersbacher S , Hochreiter W , Burkhard F , Thalmann GN , Danuser H , Markwalder R , et al. Radical cystectomy for bladder cancer today–a homogeneous series without neoadjuvant therapy, Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology (2003) ; 21: :690–96. |
[5] | Stein JP , Lieskovsky G , Cote R , Groshen S , Feng AC , Boyd S , et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients, Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology (2001) ; 19: :666–75. |
[6] | Abel EJ , Linder BJ , Bauman TM , Bauer RM , Thompson RH , Thapa P , et al. Perioperative blood transfusion and radical cystectomy: does timing of transfusion affect bladder cancer mortality? European Urology (2014) ; 66: :1139–47. |
[7] | Buchner A , Grimm T , Schneevoigt B-S , Wittmann G , Kretschmer A , Jokisch F , et al. Dramatic impact of blood transfusion on cancer-specific survival after radical cystectomy irrespective of tumor stage. Scandinavian Journal of Urology (2017) ;51: :130–36. Available from: https://pubmed.ncbi.nlm.nih.gov/28332428/. |
[8] | Chalfin HJ , Liu J-J , Gandhi N , Feng Z , Johnson D , Netto GJ , et al. Blood Transfusion is Associated with Increased Perioperative Morbidity and Adverse Oncologic Outcomes in Bladder Cancer Patients Receiving Neoadjuvant Chemotherapy and Radical Cystectomy, Annals of Surgical Oncology (2016) ; 23: :2715–22. |
[9] | Chipollini JJ , Tang DH , Patel SY , Garcia-Getting RE , Gilbert SM , Pow-Sang JM , et al. Perioperative Transfusion of Leukocyte-depleted Blood Products in Contemporary Radical Cystectomy Cohort Does Not Adversely Impact Short-term Survival, Urology (2017) ; 103: :142–48. |
[10] | Furrer MA , Fellmann A , Schneider MP , Thalmann GN , Burkhard FC , Wuethrich PY . Impact of Packed Red Blood Cells and Fresh Frozen Plasma Given During Radical Cystectomy and Urinary Diversion on Cancer-related Outcome and Survival: An Observational Cohort Study, European Urology Focus. Available from (2018) ; 4: :916–23https://www.eu-focus.europeanurology.com/article/S2405-4569(17)30214-6/fulltext |
[11] | Gershman B , Moreira DM , Tollefson MK , Frank I , Cheville JC , Thapa P , et al. The association of ABO blood type with disease recurrence and mortality among patients with urothelial carcinoma of the bladder undergoing radical cystectomy, Urologic Oncology (2016) ;34: :4.e1–9. |
[12] | Gierth M , Aziz A , Fritsche HM , Burger M , Otto W , Zeman F , et al. The effect of intra- and postoperative allogenic blood transfusion on patients’ survival undergoing radical cystectomy for urothelial carcinoma of the bladder, World Journal of Urology (2014) ;32: :1447–53. |
[13] | Kluth LA , Xylinas E , Rieken M , El Ghouayel M , Sun M , Karakiewicz PI , et al. Impact of peri-operative blood transfusion on the outcomes of patients undergoing radical cystectomy for urothelial carcinoma of the bladder, BJU International (2014) ;113: :393–98. |
[14] | Lee JS , Kim HS , Jeong CW , Kwak C , Kim HH , Ku JH . The prognostic impact of perioperative blood transfusion on survival in patients with bladder urothelial carcinoma treated with radical cystectomy, Korean Journal of Urology (2015) ;56: :295–304. |
[15] | Linder BJ , Frank I , Cheville JC , Tollefson MK , Thompson RH , Tarrell RF , et al. The impact of perioperative blood transfusion on cancer recurrence and survival following radical cystectomy, European Urology (2013) ;63: :839–45. |
[16] | Morgan TM , Barocas DA , Chang SS , Phillips SE , Salem S , Clark PE , et al. The relationship between perioperative blood transfusion and overall mortality in patients undergoing radical cystectomy for bladder cancer, Urologic Oncology (2013) ;31: :871–77. |
[17] | Moschini M , Bianchi M , Rossi MS , Dell’Oglio P , Gandaglia G , Fossati N , et al. Timing of blood transfusion and not ABO blood type is associated with survival in patients treated with radical cystectomy for nonmetastatic bladder cancer: Results from a single high-volume institution, Urologic Oncology256 (2016) ; 34: :e7–256.e13. |
[18] | Moschini M , Dell’Oglio P , Capogrosso P , Cucchiara V , Luzzago S , Gandaglia G , et al. Effect of Allogeneic Intraoperative Blood Transfusion on Survival in Patients Treated With Radical Cystectomy for Nonmetastatic Bladder Cancer: Results From a Single High-Volume Institution, Clinical Genitourinary Cancer (2015) ;13: :562–67. |
[19] | Rivas JG , Gregorio SAY , Ledo JC , Gómez ÀT , Sebastián JD , La Peña Barthel de JJ . The role of perioperative blood transfusion on postoperative outcomes and overall survival in patients after laparoscopic radical cystectomy, Journal of Cancer Research and Therapeutics (2016) ; 12: :146–49. |
[20] | Sadeghi. The impact of perioperative blood transfusion on survival following radical cystectomy for urothelial carcinoma. Can J Urol (2012) ; 19: :6443. |
[21] | Siemens DR , Jaeger MT , Wei X , Vera-Badillo F , Booth CM . Peri-operative allogeneic blood transfusion and outcomes after radical cystectomy: a population-based study, World Journal of Urology (2017) ;35: :1435–42. |
[22] | Soubra A , Zabell JR , Adejoro O , Konety BR . Effect of perioperative blood transfusion on mortality for major urologic malignancies, Clinical Genitourinary Cancer e (2015) ;13: :173–81. |
[23] | Syan-Bhanvadia S , Drangsholt S , Shah S , Cai J , Miranda G , Djaladat H , et al. Restrictive transfusion in radical cystectomy is safe, Urologic Oncology (2017) ; 35: :528.e15–528.e21. |
[24] | Vetterlein MW , Gild P , Kluth LA , Seisen T , Gierth M , Fritsche H-M , et al. Peri-operative allogeneic blood transfusion does not adversely affect oncological outcomes after radical cystectomy for urinary bladder cancer: a propensity score-weighted European multicentre study, BJU International (2018) ;121: :101–10. |
[25] | Jahnson S , Bergström R , Pedersen J . Extent of blood transfusion and cancer-related mortality after cystectomy and urinary diversion for bladder cancer, British Journal of Urology (1994) ;74: :779–84. |
[26] | Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ (Clinical 578 research ed.) (2016) ; 354: :i4086. |
[27] | National Center for Biotechnology Information [Internet] [updated 2020 Oct 27; cited 2020 Oct 27]. Available from: https://www.ncbi.nlm.nih.gov/. |
[28] | Tierney JF , Stewart LA , Ghersi D , Burdett S , Sydes MR . Practical methods for incorporating summary time-to-event data into meta-analysis, Trials (2007) ;8: :16. |
[29] | Luchini C , Stubbs B , Solmi M , Veronese N . Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale, WJMA (2017) ;5: :80. |
[30] | Moschini M , Bianchi M , Gandaglia G , Cucchiara V , Luzzago S , Pellucchi F , et al. The Impact of Perioperative Blood Transfusion on Survival of Bladder Cancer Patients Submitted to Radical Cystectomy: Role of Anemia Status, European Urology Focus. (2016) ;2: : 86–91Available from https://pubmed.ncbi.nlm.nih.gov/28723456/. |
[31] | Opelz G , Sengar DP , Mickey MR , Terasaki PI . Effect of blood transfusions on subsequent kidney transplants, Transplantation Proceedings (1973) ;5: :253–59. |
[32] | Williams JG , Hughes LE EFFECT OF PERIOPERATIVE BLOOD TRANSFUSION ON RECURRENCE OF CROHN’S DISEASE. Lancet (London, England) (1989) ; 334: :131–33. Available from: https://pubmed.ncbi.nlm.nih.gov/2567897/. |
[33] | Peters WR , Fry RD , Fleshman JW , Kodner IJ . Multiple blood transfusions reduce the recurrence rate of Crohn’s disease, Diseases of the Colon and Rectum (1989) ;32: :749–53. |
[34] | Silvis R , Steup WH , Brand A , Zwinderman KA , Lamers CB , Griffioen G , et al. Protective effect of blood transfusions on postoperative recurrence of Crohn’s disease in parous women, Transfusion (1994) ;34: :242–47. |
[35] | Li Y , Stocchi L , Rui Y , Liu G , Gorgun E , Remzi FH , et al. Perioperative Blood Transfusion and Postoperative Outcome in Patients with Crohn’s Disease Undergoing Primary Ileocolonic Resection in the “Biological Era". Journal of Gastrointestinal Surgery: Official Journal of the Society for Surgery of the Alimentary Tract (2015) ;19: :1842–51. Available from: https://pubmed.ncbi.nlm.nih.gov/26286365/. |
[36] | Steup WH , Brand A , Weterman IT , Zwinderman KH , Lamers CB , Gooszen HG . The effect of perioperative blood transfusion on recurrence after primary operation for Crohn’s disease. Scandinavian journal of gastroenterol ogy. Supplement (1991) ; 188: :81–86. Available from: https://pubmed.ncbi.nlm.nih.gov/1775945/. |
[37] | GANTT C . RED BLOOD CELLS FOR CANCER PATIENTS, The Lancet (1981) ;318: :363. |
[38] | Tzounakas VL , Seghatchian J , Grouzi E , Kokoris S , Antonelou MH . Red blood cell transfusion in surgical cancer patients: Targets, risks, mechanistic understanding and further therapeutic opportunities, Transfusion and apheresis science: official journal of the World Apheresis Association: official journal of the European Society for Haemapheresis (2017) ;56: :291–304. |
[39] | Iqbal N , Haider K , Sundaram V , Radosevic J , Burnouf T , Seghatchian J , et al. Red blood cell transfusion and outcome in cancer, Transfusion and apheresis science: official journal of the World Apheresis Association: official journal of the European Society for Haemapheresis (2017) ;56: :287–90. |
[40] | Boshier PR , Ziff C , Adam ME , Fehervari M , Markar SR , Hanna GB . Effect of perioperative blood transfusion on the long-term survival of patients undergoing esophagectomy for esophageal cancer: a systematic review and meta-analysis, Diseases of the esophagus: official journal of the International Society for Diseases of the Esophagus. 2018;31. |
[41] | Nakanishi K , Kanda M , Kodera Y . Long-lasting discussion: Adverse effects of intraoperative blood loss and allogeneic transfusion on prognosis of patients with gastric cancer, World Journal of Gastroenterology (2019) ;25: :2743–51. |
[42] | Acheson AG , Brookes MJ , Spahn DR . Effects of allogeneic red blood cell transfusions on clinical outcomes in patients undergoing colorectal cancer surgery: a systematic review and meta-analysis, Annals of Surgery (2012) ;256: :235–44. |
[43] | Busch OR , Hop WC , van Hoynck Papendrecht MA , Marquet RL , Jeekel J . Blood transfusions and prognosis in colorectal cancer, The New England Journal of Medicine (1993) ;328: :1372–76. |
[44] | Lyu X , Qiao W , Li D , Leng Y . Impact of perioperative blood transfusion on clinical outcomes in patients with colorectal liver metastasis after hepatectomy: a meta-analysis, Oncotarget (2017) ;8: :41740–48. |
[45] | Xun Y , Tian H , Hu L , Yan P , Yang K , Guo T . The impact of perioperative allogeneic blood transfusion on prognosis of hepatocellular carcinoma after radical hepatectomy: A systematic review and meta-analysis of cohort studies, Medicinee (2018) ;97: :12911. |
[46] | Mavros MN , Li Xu , Maqsood H , Gani F , Ejaz A , Spolverato G , et al. Perioperative Blood Transfusion and the Prognosis of Pancreatic Cancer Surgery: Systematic Review and Meta-analysis. Annals of Surgical Oncology (2015) ;22: :4382–91.Available from: https://pubmed.ncbi.nlm.nih.gov/26293837/. |
[47] | Wang T , Luo L , Huang H , Yu J , Pan C , Cai X , et al. Perioperative blood transfusion is associated with worse clinical outcomes in resected lung cancer, The Annals of Thoracic Surgery (2014) ;97: :1827–37. |
[48] | Eickhoff JH , Andersen J , Laybourn C . Perioperative blood transfusion does not promote recurrence and death after mastectomy for breast cancer, The Danish Breast Cancer Cooperative GrouThe British Journal of Surgery (1991) ;78: :1358–61. |
[49] | Lentz SS , Shelton BJ , Toy NJ . Effects of perioperative blood transfusion on prognosis in early-stage cervical cancer, Annals of Surgical Oncology (1998) ;5: :216–19. |
[50] | Boehm K , Beyer B , Tennstedt P , Schiffmann J , Budaeus L , Haese A , et al. No impact of blood transfusion on oncological outcome after radical prostatectomy in patients with prostate cancer, World Journal of Urology (2015) ;33: :801–06. |
[51] | Wang Y-L , Jiang B , Yin F-F , Shi H-Q , Xu X-D , Zheng S-S , et al. Perioperative Blood Transfusion Promotes Worse Outcomes of Bladder Cancer after Radical Cystectomy: A Systematic Review and Meta-Analysis, PloS One (2015) ;10: :e0130122. |
[52] | Cata JP , Lasala J , Pratt G , Feng L , Shah JB . Association between Perioperative BloodTransfusions and Clinical Outcomes in Patients Undergoing Bladder Cancer Surgery: A Systematic Review and Meta-Analysis Study. Journal of Blood Transfusion (2016) ;2016: :9876394. |
[53] | Mottet N , Ribal MJ , Boyle H , Santis M de , Caillet P , Choudhury A , et al. Management of bladder cancer in older patients: Position paper of a SIOG Task Force, Journal of Geriatric Oncology (2020) ;11: :1043–53. |
[54] | Bruins HM , Veskimäe E , Hernández V , Neuzillet Y , Cathomas R , Compérat EM , et al. The Importance of Hospital and Surgeon Volume as Major Determinants of Morbidity and Mortality After Radical Cystectomy for Bladder Cancer: A Systematic Review and Recommendations by the European Association of Urology Muscle-invasive and Metastatic Bladder Cancer Guideline Panel, European Urology Oncology (2020) ;3: :131–44. |
[55] | Wujtewicz M . Perioperative strategies in patients who refuse blood product transfusion, Polski Przeglad Chirurgiczny (2020) ;92: :1–5. |
[56] | Habler O , Voss B . Perioperatives Management bei Zeugen Jehovas, Spezielle Berücksichtigung der religiös motivierten Ablehnung von Fremdblut. Der Anaesthesist (2010) ;59: :297–311. |
[57] | Trentino KM , Farmer SL , Leahy MF , Sanfilippo FM , Isbister JP , Mayberry R , et al. Systematic reviews and meta-analyses comparing mortality in restrictive and liberal haemoglobin thresholds for red cell transfusion: an overview of systematic reviews, BMC Medicine (2020) ;18: :154. |
[58] | Holst LB , Petersen MW , Haase N , Perner A , Wetterslev J . Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis, BMJ (Clinical research ed.) (2015) ;350: :h1354. |
[59] | Carson JL , Carless PA , Hebert PC . Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion, The Cochrane Database of Systematic Reviews 2012: :CD002042. |
[60] | Meybohm P. , Richards T. , Isbister J. , Hofmann A. , Shander A. , Goodnough L. T. , Mu& Ntilde oz M. , Gombotz H. , Weber C.F. , Choorapoikayil S. , Spahn D. R. , Zacharowski K. , Patient Blood Management Maßnahmenbündel- A&I Online - Anästhesiologie & Intensivmedizin [Internet]. c29.10.2020 [updated 2020 Oct 29; cited 2020 Oct 29]. Available from: https://www.ai-online.info/archiv/2017/01-2017/patient-blood-managementmassnahmenbuendel.html. |
[61] | Abeysiri S , Chau M , Highton D , Richards T . Management of the patient presenting with anaemia in the preoperative setting, Transfusion and apheresis science: official journal of the World Apheresis Association: official journal of the European Society for Haemapheresis (2019) ;58: :392–96. |
[62] | Merolle L , Marraccini C , Di Bartolomeo E , Montella MT , Pertinhez TA , Baricchi R , et al. Postoperative patient blood management: transfusion appropriateness in cancer patients, Blood transfusion=Trasfusione del sangue (2020) ;18: :359–65. |
[63] | Meybohm P , Fischer D , Schnitzbauer A , Zierer A , Schmitz-Rixen T , Bartsch G , et al. Patient-blood-Management : Stand der aktuellen Literatur. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen (2016) ;87: :40–46. |
[64] | Carson JL , Terrin ML , Noveck H , et al. Liberal or restrictive transfusion in highrisk patients after hip surgery, N Engl J Med (2011) ;365: :2453–62. |
[65] | Murphy GJ , Pike K , Rogers CA , et al. Liberal or restrictive transfusion after cardiac surgery, N Engl J Med (2015) ;372: :997–1008. |
[66] | Marik PE , Corwin HL . Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature, Crit Care Med (2008) ;36: :2667–74. |
[67] | Hébert PC , Wells G , Blajchman MA , et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care, N Engl J Med (1999) ;340: :409–17. |
[68] | Jairath V , Kahan BC , Gray A , et al. Restrictive versus liberal blood transfusion for acute upper gastrointestinal bleeding (TRIGGER): a pragmatic, open-label, cluster randomised feasibility trial, Lancet (2015) ;386: :137–44. |
[69] | Docherty AB , Walsh TS . Anemia and blood transfusion in the critically ill patient with cardiovascular disease, Crit Care (2017) ;21: :61. |
[70] | Hajjar LA , Vincent JL , Galas FR , et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial, JAMA (2010) ;304: :1559–67. |
[71] | Koch CG , Sessler DI , Mascha EJ , et al. A randomized clinical trial of red blood cell transfusion triggers in cardiac surgery, Ann Thorac Surg (2017) ;104: :1243–50. Copyright © Massachusetts Medical Society. |
[72] | Mazer CD , Whitlock RP , Fergusson DA , Hall J , Belley-Cote E , Connolly K , Khanykin B , Gregory AJ , de Médicis É , McGuinness S , Royse A , Carrier FM , Young PJ , Villar JC , Grocott HP , Seeberger MD , Fremes S , Lellouche F , Syed S , Byrne K , Bagshaw SM , Hwang NC , Mehta C , Painter TW , Royse C , Verma S , Hare GMT , Cohen A , Thorpe KE , Jüni P , Shehata N ; TRICS Investigators and Perioperative Anesthesia Clinical Trials GrouRestrictive or Liberal Red-Cell Transfusion for Cardiac Surgery, N Engl J Med (2017) ; 377: (22):2133–2144 doi: 10.1056/NEJMoa1711818. Epub 2017 Nov 12. PMID: 29130845. |

