
Functional and Clinicopathologic Outcomes Using a Modified Vescica Ileale Padovana Technique
Abstract
Objective:
To evaluate the clinicopathologic and functional outcomes of a modified Vescica ileale Padovana (VIP) neobladder technique.
Methods:
Data for 160 patients at a single institution who underwent radical cystectomy and orthotopic VIP neobladder creation between 1998 and 2013 were analyzed. Modified VIP technique involved longitudinal opening of the small bowel close to the anterior mesenteric border instead of along the true anti-mesentery. This allowed for creation of a dependent neourethral funnel and a large serosal surface for ureteral anastomosis, distant from any suture lines.
Results:
Mean age for the entire cohort was 59.5, with 9% female and 64% with muscle invasive disease prior to cystectomy. Within 30 days of surgery, 16 patients (10%) developed a Clavien grade 3-4 complication and there were no deaths. Ninety-six percent reported minor or no daytime urinary leakage at 12 months, and 70% reported minor or no nighttime urinary leakage. Two- and five-year overall survival rates were 84.2% and 72.6% , respectively. Seven patients developed a ureteral stricture (4%), three (2%) had bladder neck contractures, two (1%) experienced urethral recurrence, and there were no vesicovaginal fistulas.
Conclusions:
This modified VIP neobladder technique achieves favorable functional, survival, and recurrence outcomes similar to other published orthotopic continent diversions. Its near spheroidal shape lowers internal pressure, allowing for improved continence at physiologic filling capacity, and its offset bowel opening helps prevent unnecessary stretch to the native urethra, even in large individuals. The widened uretero-enteric anastomosis site distant from bowel suture lines contributes to decreased stricture rates and its placement on the dome of the neobladder facilitates endoscopic access should strictures occur. Finally, lack of posterior overlapping suture lines also mitigates the risk of fistulae formation in females should anterior vaginal wall excision or entry be unavoidable.
INTRODUCTION
Radical cystectomy remains the gold standard for management of muscle-invasive bladder cancer [1, 2]. Estimates using data from the Surveillance, Epidemiology, and End Results (SEER) database predict that approximately 18,600 new muscle-invasive bladder cancer cases will be diagnosed in 2014. Analysis of this SEER data reveals that 42% of these patients with muscle-invasive disease ultimately undergo cystectomy [3], necessitating the surgical diversion of urine in the form of an incontinent ileal conduit, a continent orthotopic pouch that empties via urethra, or a catheterizable non-orthotopic cutaneous stoma [4]. Orthotopic neobladders allow voiding through the native urethra and can potentially eliminate the need for stoma appliances or catheters without compromising cancer control [5]. Neobladders created from ileum have been found to be more compliant than those created with large bowel [6], and by detubularizing and refolding into a spherical shape, low pressure filling at physiologic capacity can best be achieved [6]. Specifically, spherical configurations maximize volume for any given surface area, thus decreasing the length of bowel needed for harvest and minimizing the opportunity for electrolyte exchange across the neobladder wall [7]. The specific folding method used varies greatly among institutions and little evidence exists that definitively favors one technique versus another.
Two techniques routinely used at our institution for neobladder creation are the Studer and the vescica ileale Padovana (VIP) techniques. A distinction of the VIP technique is its complete use of bowel segment in the spherical component of the neobladder [8] whereas the Studer neobladder involves the creation of an afferent limb that does not contribute to bladder volume [9]. There are many published studies available that report functional and oncologic outcomes for the Studer neobladder [10–13], but fewer large studies exist that offer data on such outcomes specifically following VIP neobladder creation [8, 14].
Modified creation of the Vescica ileale Padovana (VIP) neobladder has been performed at our institution over a 15-year period. We sought to evaluate the clinicopathologic and functional outcomes of this technique.
METHODS
Patients
After obtaining Institutional Review Board approval for the conduct of this unfunded study, a retrospective review of a single-institution bladder cancer database was performed to identify patients who underwent radical cystectomy with VIP neobladder orthotopic replacement between 1998 and 2013. Only adults (>17 years) were included in the study and all patients had primary urothelial cancer of the bladder.
Outcomes and variables
Functional and clinicopathologic outcomes were the primary outcomes of interest in this study. Variables collected for each patient included age, sex, body mass index (BMI), TURBT and cystectomy stage, pre- and post-operative creatinine, neoadjuvant and adjuvant chemotherapy, case length, estimated blood loss (EBL), length of stay (LOS) in the hospital, 30-day and long term complications including vesicovaginal fistula, presence of hydronephrosis at three weeks and twelve months, and functional outcomes. Functional outcomes included the need to catheterize at twelve months, daytime control at twelve months, and nighttime control at twelve months. Continence and need to catheterize was assessed by physician interview. Other follow-up variables included subsequent development of a ureteral stricture, bladder neck contracture, and urethral recurrence. Overall survival status was assessed using our departmental database and the Social Security Death Index. A Kaplan-Meier overall survival curve was generated using Stata 12.1 (Stata Corp, College Station, TX).
Case length was defined as the time from skin opening to skin closure. 30-day complications were classified using the modified Clavien-Dindo system [15]. Patients receiving perioperative blood transfusion were classified as having a Clavien grade 2 complication. Only the highest-grade complications were reported. Hydronephrosis was assessed by intravenous pyelogram in the immediate post-operative period, and long-term surveillance imaging included renal ultrasound or cross-sectional imaging with CT/MRI. Daytime control was defined by patient report of normal, minor, or major leakage on the majority of days each week. Nighttime control was defined by patient report as no leakage, occasional (1-2 times per week) low volume leakage, occasional high volume leakage, frequent (>2 times per week) low volume leakage, or frequent high volume leakage. Variables were assessed for completeness. BMI was missing for 33% of patients (n = 53/160), preoperative creatinine was missing for 13% (n = 20/160), case time was missing for 33% (n = 53/160), and EBL was missing for 12% (n = 19/160). The majority of patients with missing data were operated upon prior to 2003.
Surgical description
VIP neobladder construction was based on its initial report [8], with minor modifications by the surgeon. Briefly, a 40–50 cm distal ileal segment approximately 15–20 cm from the ileocecal valve is folded into a sideways-“U” configuration. The small bowel is then opened longitudinally, close to the mesenteric border instead of along the true anti-mesentery. The distal segment of bowel, using the minimum length necessary as determined by patient anatomy (∼3-4 cm) is then fashioned into a funnel to form the bladder neck/neourethra. The proximal segment is folded into a spiral configuration with adjacent bowel sutured together in order to approximate the new posterior wall. The pouch is folded onto itself in a cephalad to caudad fashion. Using a non-tunneled anastomosis, both ureters are reimplanted on their respective sides onto the superior portion of the neobladder. The pouch is tested intraoperatively, with an average initial capacity of 200–400 mL. Ureteral stents are brought out through the urethra alongside the indwelling catheter. Among female patients undergoing cystectomy with VIP neobladder creation, the anterior vaginal wall was spared. In those patients with entry into the anterior vaginal wall, primary repair was performed without flap-interposition prior to neobladder creation. All patients received 2 grams of Cefoxitin for 24 hours as antibiotic prophylaxis. Additionally, patients received either 40 mg of enoxaparin daily or 5000 units of heparin three times daily as thromboembolism prophylaxis during hospitalization.
RESULTS
One hundred and sixty patients were identified as undergoing VIP neobladder creation during the study period. Patient characteristics are shown in Table 1. The majority of patients underwent radical cystectomy for muscle invasive bladder cancer (64%). Forty-seven percent of patients had ≤pT1 disease on cystectomy pathology, and 30% of patients were pT3-4.
With regard to early and late complications (Table 2), 16 patients (10%) developed a Clavien grade 3-4 complication within 30 days of surgery, and no patients died within 30 days of surgery (Clavien grade 5). Of the 13 women undergoing modified VIP replacement, all had attempted sparing of the anterior vaginal wall and none were clinically T3 or higher at the time of surgery. Two patients had small inadvertent vaginotomies that were closed primarily. There were no vesicovaginal fistulas. Seven patients (4%) developed ureteral stricture, four of which occurred within one year of surgery. All strictures were managed successfully: five with ureteral reimplantation, one with an ileal ureter, and one with temporary stenting. Three patients (2%) developed a bladder neck contracture, two of which occurred within one year of surgery. Two contractures were managed by incision, one was managed with sequential dilation, and only one patient required intermittent catheterization following contracture. One patient developed a late urethral stricture (1%), which was managed with conversion to ileal conduit.
Median follow-up of patients was 73 months. Two patients (1%) experienced urethral recurrence. Overall survival is shown in Fig. 2, with median survival not reached. Two-year overall survival was 84.2% and five-year overall survival was 72.6% . Fifteen patients died within one year of surgery, ten of which had progression of disease and five were disease free at last follow-up.
Functional outcomes are shown in Table 3, representing only those patients with twelve-month follow-up (n = 107). Incidence of mild hydronephrosis decreased dramatically from the three-week to twelve-month appointments and no patients had moderate or severe hydronephrosis at either point in time. Seven patients (7%) were catheterization dependent at 12 months due to urinary retention, and an additional nine patients opted to catheterize daily in addition to spontaneous voiding in order to ensure complete emptying.
DISCUSSION
The technique for VIP neobladder creation was first described in 1990, with its authors advocating orthotopic bladder replacement following cystectomy as “the ideal solution to enhance the quality of the patient’s life.” Their new surgical technique promised improved rates in both daytime and nighttime continence [8]. In performing this study we were able to investigate the validity of this claim as well as explore other clinicopathologic outcomes resulting from this particular method of bladder substitution.
In our modified technique for the neobladder there are several distinct advantages. The near pure spherical configuration maximizes the ratio of bladder volume to amount of bowel utilized [16]. Offset opening of the bowel wall results in a wider, well-vascularized bowel segment to use for ureteral reimplantation. This allows for a minimally mobilized ureter and reimplantation distant from any suture lines, which contributes to the very low ureteral stricture rate. This placement also ensures that when ureteral strictures do occur, they are easily accessible surgically. Stricture rates in the literature are reported to be as low as 2.7% following refluxing anastomosis, and we found our own rates to be comparable [12, 17]. Offset opening also facilitates ease in reaching the native urethra (even in obese individuals) when creating the neourethra, a dependent funnel that promotes better bladder emptying. And finally, this modified technique results in intervening mesentery that avoids posterior overlapping suture lines. This mitigates risk of fistulae formation potentially caused by ongoing urinary drainage into areas of injury [11, 18–20] should tumor anatomy necessitate removal of the anterior vaginal wall or if inadvertent entry is unavoidable. In our own experience, with two unplanned vaginotomies, neither resulted in vesicovaginal fistula.
Our rate of reported postoperative complications, while significant, was at the low end of ranges reported previously. Given the extent of disease and scope of this procedure, expected morbidity following radical cystectomy is high, ranging from 20 to 57% during the first 30 days postoperatively as reported in a review by Richards et al. [21] and rising to 64% of patients within the first 90 days as reported by Shabsigh et al. [22]. In the previously discussed studies, as well as within our own cohort, the predominant percentage of complications was minor in nature. Fortunately, despite these high complication rates mortality remains relatively low, with 1.5% deaths in the first 30 days as reported by Shabsigh et al. [22] and no perioperative deaths reported in our own series.
When comparing on the basis of quality of life, available literature does not definitively support the implementation of one type of reconstruction over another [23, 24]. With a funneled bladder outlet, there is some reported concern for kinking requiring catheterization to void [12]. However, the anatomic placement of the neobladder reservoir helps to avoid this concern for retention, with only seven patients requiring intermittent catheterization to void at one year. This is similar to that seen in other large cohorts, for example Studer et al. report 4.6% use of indwelling catheter or intermittent catheterization in their cohort [12]. Continence varies slightly between published cohorts based on the definition used. However, despite this, our rates compare favorably to those seen previously [10, 14, 16] with daytime continence (no leakage or minor leakage) at 96% and nighttime continence (no leak or occasional low leakage) of 70% . Hautmann et al. report ranges of 88–95% daytime and 66–93% nighttime in their review of the literature [16]. Studer et al. too found with their technique that 12 months after surgery, 92% of neobladder patients considered themselves continent (completely dry or minimal loss of a few drops of urine, 1-2 times per month) during the day and 79% reported continence at night [12, 25]. Although there are a number of factors including patient age as well as attempted nerve sparing and native sphincter preservation [16] that contribute to continence, the ability to achieve low pressure filling at physiologic capacity is a major contributor to both daytime and nighttime continence. This highlights the importance of the nearly spheroidal configuration of this neobladder technique.
Results of this study reveal favorable oncologic outcomes as compared to other published orthotopic diversions. Our five-year overall survival was 72.6% , as compared to the series published by Stein et al. that reported 66% 5-year overall survival in their cohort of 1,054 patients undergoing cystectomy [1]. Madersbacher et al. too reported a 5-year overall survival of 59% in 507 patients undergoing cystectomy for node negative, metastasis negative transitional cell carcinoma [2, 6]. Because neobladder creation necessitates sparing the urethra, it carries with it an inherent risk of urethral recurrence not universally present in other forms of continent diversion where urethrectomy is possible. Despite mitigating this risk with intraoperative urethral frozen section analysis, a small percentage of recurrences are expected. Our personal experience yielded two urethral recurrences (1%), which correlates well with a meta-analysis by Gakis et al. that reports urethral recurrence rates with orthotopic diversion of 1.1–2.5% [6]. These favorable results likely relate to patient selection, whereby patients chosen for neobladder creation are often lower clinical stage with less muscle invasive disease. This is evidenced by the fact that nearly half of our patients had ≤pT1 disease on cystectomy pathology and only ten patients were pT4.
We recognize that there are limitations in this study. Because the study is purely descriptive, without comparison or randomization, there is potential for bias whereby physician selection of patients with a potentially higher preoperative functional status and more favorable tumor features might bias the study results. Indeed our cohort has a predominance of younger patients with low stage disease, however this reflects the reality of patient selection for orthotopic bladder replacement – an option typically reserved by for patients meeting strict criteria that would indicate success. A lack of validated pre- and postoperative quality of life data makes comparison to other studies more challenging. Previously, generic questionnaires set strict standards for a definition of ‘continence’, particularly nighttime continence, that is potentially unreasonable to expect in the post-cystectomy setting. Although disease specific quality of life questionnaires have since been validated [27, 28] to address concerns that are more specific to this population such as need for catheterization, difficulties with stoma care or stoma appliances, and the distinction between daytime and nighttime continence, [23] many institutions (including ours) have only recently begun to incorporate these into practice. Perhaps the most challenging limitation is the retrospective nature of this study and its incomplete data set. Nevertheless, we believe that our cohort represents one of the largest experiences in the literature to assess functional, complication, and clinicopathologic outcomes in this unique population.
CONCLUSION
Modified VIP neobladder technique achieves favorable functional, survival, and recurrence outcomes similar to other published orthotopic continent diversions. Its near spheroidal shape optimizes the bowel surface area to volume ratio, lowering internal pressure and allowing for improved continence at physiologic filling capacity. Its offset bowel opening helps prevent unnecessary stretch to the native urethra, even in large individuals. The widened uretero-enteric anastomosis site distant from bowel suture lines contributes to decreased stricture rates and its placement on the dome of the neobladder facilitates endoscopic access should strictures occur. Finally, lack of posterior overlapping suture lines also mitigates the risk of fistulae formation in females should anterior vaginal wall excision or entry be unavoidable.
REFERENCES
1 | Stein JP, Lieskovsky G, Cote R(2001) Radical cystectomyin the treatment of invasive bladder cancer: Long-term results in 1,054 patientsJournal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology19: 3666675 |
2 | Stenzl A, Cowan NC, De Santis M(2009) The updated EAU guidelines on muscle-invasive and metastatic bladder cancerEuropean Urology55: 4815825 |
3 | DeSantis CE, Lin CC, Mariotto AB(2014) Cancer treatment and survivorship statistics, CA: A Cancer Journal for Clinicians n/a-n/a |
4 | Gore JL, Saigal CS, Hanley JM, Schonlau M, Litwin MSand the Urologic Diseases in America P(2006) Variations in reconstruction after radical cystectomyCancer107: 4729737 |
5 | Lee RK, Abol-Enein H, Artibani W(2014) Urinary diversion after radical cystectomy for bladder cancer: Options, patient selection, and outcomesBJU International113: 11123 |
6 | Gakis G, Stenzl A(2010) Ileal neobladder and its variantsEuropean Urology Supplements9: 10745753 |
7 | Chang D, Lawrentschuk N(2015) Orthotopic neobladder reconstructionUrology Annals7: 11 |
8 | Pagano F, Artibani W, Ligato P, Piazza R, Garbeglio A, Passerini G(1990) Vescica Ileale Padovana: A technique for total bladder replacementEuropean Urology17: 2149154 |
9 | Studer UE, Danuser H, Hochreiter W, Springer JP, Turner WH, Zingg EJ(1996) Summary of 10 years’ experience with an ileal low-pressure bladder substitute combined with an afferent tubular isoperistaltic segmentWorld Journal of Urology14: 12939 |
10 | Nieuwenhuijzen JA, de Vries RR, Bex A(2008) Urinary diversions after cystectomy: The association of clinical factors, complications and functional results of four different diversionsEuropean Urology53: 4834844 |
11 | Granberg CF, Boorjian SA, Crispen PL(2008) Functional and oncological outcomes after orthotopic neobladder reconstruction in womenBJU International102: 1115511555 |
12 | Studer UE, Burkhard FC, Schumacher M(2006) Twenty years experience with an ileal orthotopic low pressure bladder substitute— lessons to be learnedThe Journal of Urology176: 1161166 |
13 | Cancrini A, De Carli P, Pompeo V(1996) Lower urinary tract reconstruction following cystectomy: Experience and results in 96 patients using the orthotopic ileal bladder substitution of Studer et alEuropean Urology29: 2204209 |
14 | Novara G, Ficarra V, Minja A, De Marco V, Artibani W(2010) Functional results following vescica ileale Padovana (VIP) neobladder: Midterm follow-up analysis with validated questionnairesEuropean Urology57: 610451051 |
15 | Dindo D, Demartines N, Clavien PA(2004) Classification of surgical complications: A new proposal with evaluation in a cohort of patients and results of a surveyAnnals of Surgery240: 2205213 |
16 | Hautmann RE, Volkmer BG, Schumacher MC, Gschwend JE, Studer UE(2006) Long-term results of standard procedures in urology: The ileal neobladderWorld Journal of Urology24: 3305314 |
17 | Hautmann RE, Abol-Enein H, Davidsson T(2013) ICUD-EAU International Consultation on Bladder Cancer Urinary diversionEuropean Urology63: 16780 |
18 | Rapp DE, O’Connor RC, Katz EE, Steinberg GD(2004) Neobladder-vaginal fistula after cystectomy and orthotopic neobladder constructionBJU International94: 710921095 |
19 | Tunuguntla HS, Manoharan M, Gousse AE(2005) Management of neobladder-vaginal fistula and stress incontinence following radical cystectomy in women: A reviewWorld Journal of Urology23: 4231235 |
20 | Chang SS, Cole E, Cookson MS, Peterson M, Smith JAJr(2002) Preservation of the Anterior Vaginal Wall During Female Radical Cystectomy With Orthotopic Urinary Diversion: Technique and ResultsThe Journal of Urology168: 4,Part 114421445 |
21 | Richards KA, Steinberg GD(2013) Perioperative outcomes in radical cystectomy: How to reduce morbidity? Current Opinion in Urology23: 5456465 |
22 | Shabsigh A, Korets R, Vora KC(2009) Defining Early Morbidity of Radical Cystectomy for Patients with Bladder Cancer Using a Standardized Reporting MethodologyEuropean Urology55: 1164176 |
23 | Porter MP, Wei JT, Penson DF(2005) Quality of life issues in bladder cancer patients following cystectomy and urinary diversionThe Urologic Clinics of North America32: 2207216 |
24 | Hautmann RE, Abol-Enein H, Hafez K(2007) Urinary DiversionUrology69: 1, Supplement1749 |
25 | Kessler TM, Burkhard FC, Perimenis P(1323) Attempted nerve sparing surgery and age have a significant effect on urinary continence and erectile function after radical cystoprostatectomy and ileal orthotopic bladder substitutionThe Journal of Urology172: 4, Part 113231327 |
26 | Madersbacher S, Hochreiter W, Burkhard F(2003) Radical Cystectomy for Bladder Cancer Today— A Homogeneous Series Without Neoadjuvant TherapyJournal of Clinical Oncology21: 4690696 |
27 | Gilbert SM, Wood DP, Dunn RL(2007) Measuring health-related quality of life outcomes in bladder cancer patients using the Bladder Cancer Index (BCI)Cancer109: 917561762 |
28 | Cookson MS, Dutta SC, Chang SS, Clark T, Smith JA, Wells N(2003) Health related quality of life in patients treated with radical cystectomy and urinary diversion for urothelial carcinoma of the bladder: Development and validation of a new disease specific questionnaireThe Journal of urology 170: 519261930 |
Figures and Tables
Fig.1
Modified VIP neobladder construction. (A) A 40–50 cm distal ileal segment is chosen approximately 15–20 cm from the ileocecal valve and (B) is folded into a sideways “U” configuration. The small bowel is opened longitudinally, close to the mesenteric border instead of along the true anti-mesentery. (C) The distal segment of bowel is tubularized into the neourethra and (D) the proximal segment is folded into a spiral configuration with adjacent bowel sutured together to approximate the new posterior wall. (E) The pouch is folded onto itself in a cephalad to caudad fashion and both ureters are reimplanted anteriorly on their respective sides.
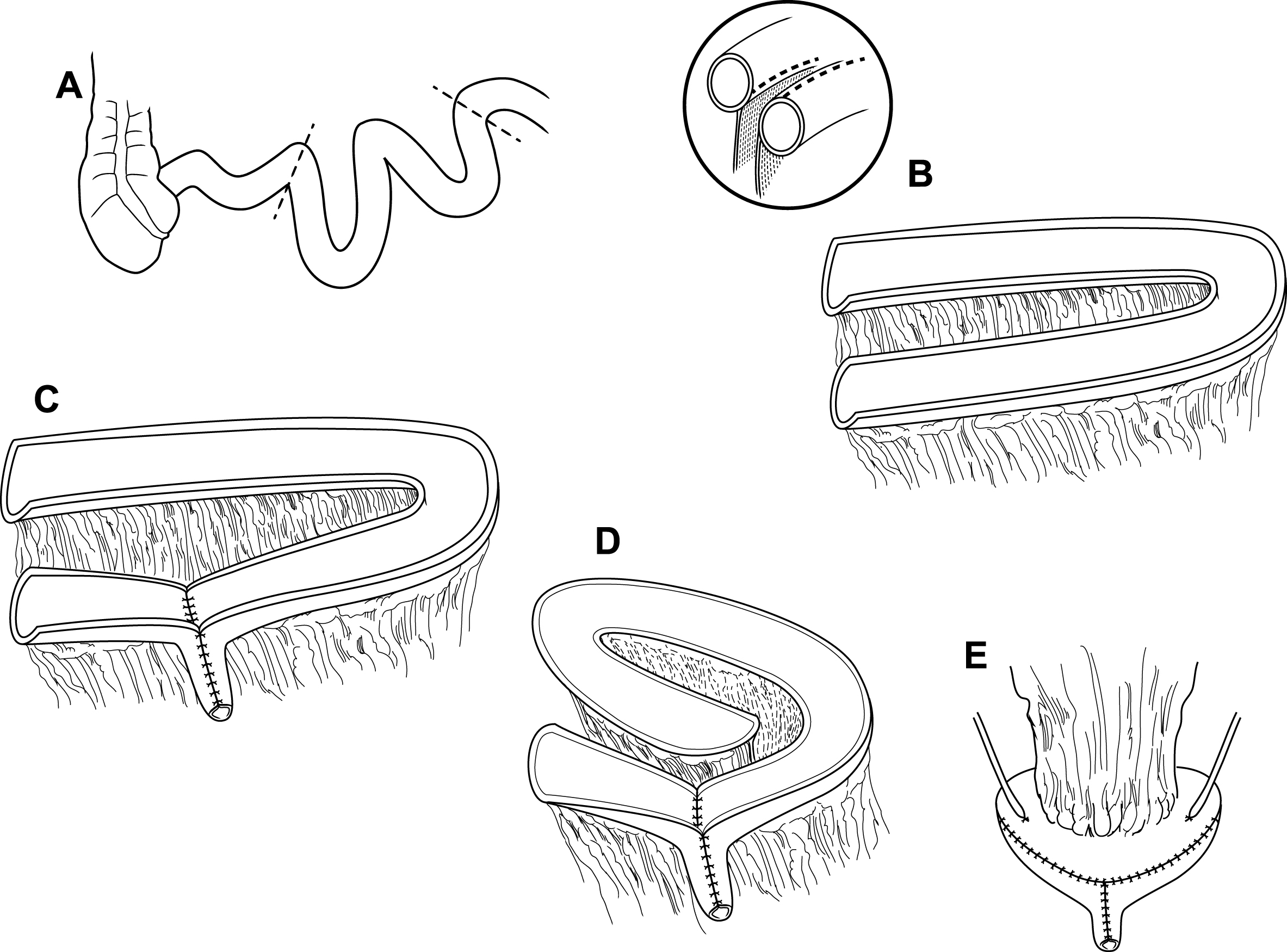
Fig.2
Overall survival for VIP neobladder patients.
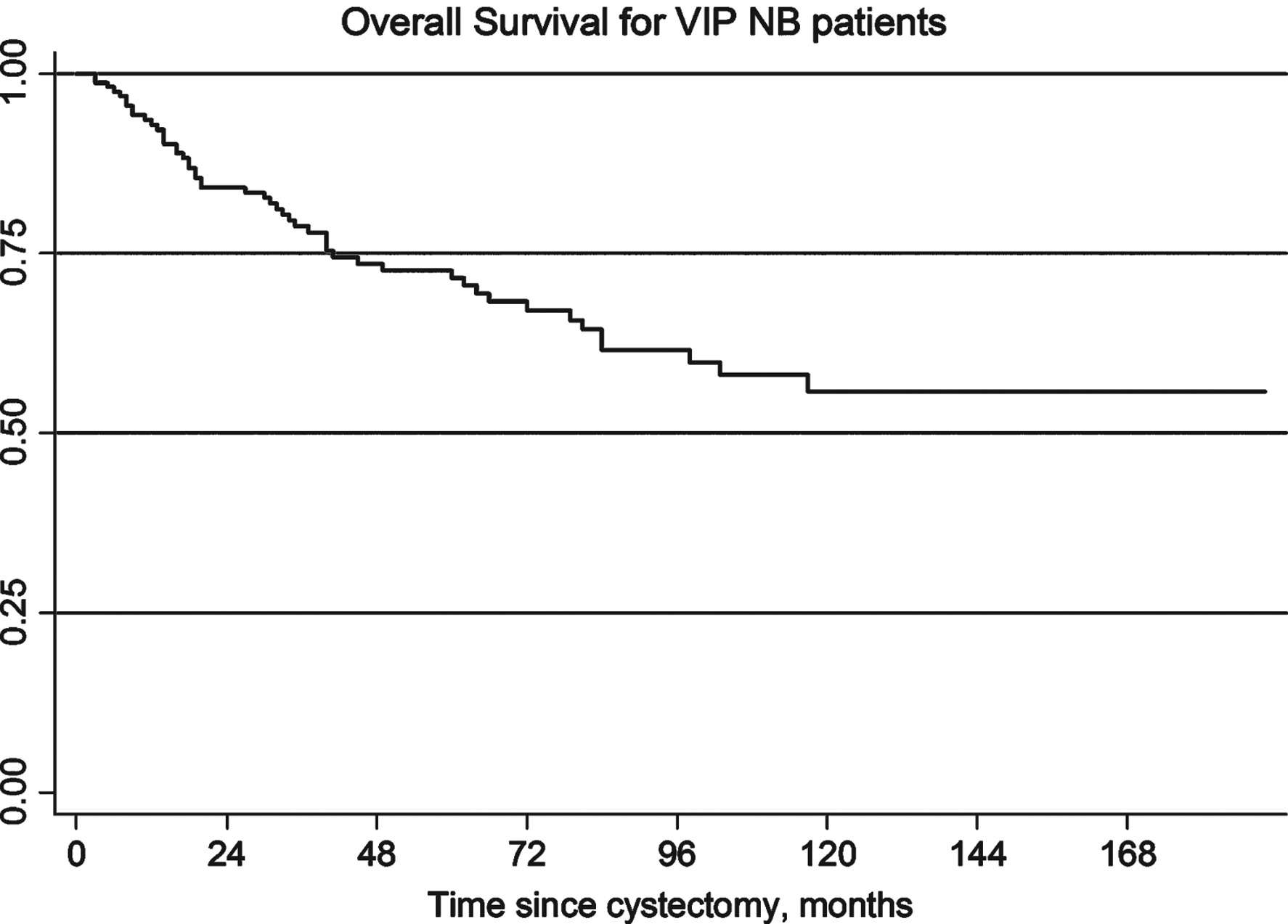
Table 1
VIP neobladder patient characteristics
| Variable | n (%) = 160 |
| Age, mean (SD) | 59.5 (10.4) |
| Sex | |
| Female | 14 (9) |
| Male | 146 (91) |
| BMI, mean (SD) | 28.2 (4.9) |
| TURBT stage | |
| ≤T1 | 58 (36) |
| ≥T2 | 102 (64) |
| Neoadjuvant chemotherapy | 20 (13) |
| Preoperative creatinine, mean (SD) | 1.11 (0.3) |
| Postoperative creatinine, mean (SD) | 1.10 (0.3) |
| Pathologic stage | |
| pT0, pTis, pTa | 55 (34) |
| pT1 | 21 (13) |
| pT2 | 36 (23) |
| pT3 | 38 (24) |
| pT4 | 10 (6) |
| Lymph nodes positive | 36 (23) |
| Adjuvant chemotherapy | 50 (31) |
| Length of case, mean (SD) | 239 (38) min. |
| EBL, mean (SD) | 564 (435) mL |
| LOS, mean (SD) | 7.3 (2.8) days |
*BMI missing for 53/160, pre-operative creatinine missing 20/160, case time missing for 53/160, EBL missing for 19/160.
Table 2
Post-operative complications in patients undergoing VIP neobladder replacement
| Complication | n (%) = 160 |
| 30 day Clavien grade | |
| Clavien 1 | 25 (16%) |
| Clavien 2 | 30 (19%) |
| Clavien 3 | 6 (4%) |
| Clavien 4 | 10 (6%) |
| Clavien 5 | 0 (0%) |
| Vesicovaginal fistula | 0 (0%) |
| Ureteral stricture | 7 (4%) |
| Urethral stricture | 1 (1%) |
| Bladder neck contracture | 3 (2%) |
Table 3
Functional outcomes at twelve-month follow-up appointment (n = 107)
| Mild hydronephrosis at 3 weeks | 35 (33) |
| Mild hydronephrosis at 12 months | 12 (11) |
| Catheterize 1/day at 12 months | 16 (15) |
| Catheterization dependent at 12 months | 7 (7) |
| Daytime control at 12 months | |
| No leakage | 82 (76) |
| Minor leakage | 21 (20) |
| Major leakage | 4 (4) |
| Nighttime control at 12 months | |
| No leak | 28 (26) |
| Occasional low leakage | 47 (44) |
| Occasional high leakage | 0 |
| Frequent low leakage | 18 (17) |
| Frequent high leakage | 14 (13) |


