
“Your risk is low, because …”: argument-driven online genetic counselling
Abstract
Advances in genetic research have created the need to inform consumers. Yet, the communication of hereditary risk and of the options for how to deal with it is a difficult task. Due to the abstract nature of genetics, people tend to overestimate or underestimate their risk. This paper addresses the issue of how to communicate risk information on hereditary breast and ovarian cancer through an online application. The core of the paper illustrates the design of OPERA, a risk assessment instrument that applies the UK National Institute of Health and Clinical Excellence's guidelines on the basis of (i) the number of relatives on the same side of the family with the same cancer or cancers that are known to run together; (ii) the ages of these relatives at diagnosis and (iii) the closeness of the family relationship with the person who is doing the assessment. By relying on the argumentation theory, we explain how the communication strategy that OPERA implements is essentially based on Perelman and Olbrechts-Tyteca's deductive argumentation by association. By using as premises “facts” (propositions about reality that can be assumed without further justification) and “truths” (propositions that make connections about facts), OPERA delivers its claims with an ex auctoritate causal link aimed at transferring the audience's acceptance of the cause to the effect. Overall, the design of OPERA rests on its capacity to induce users’ active processing of risk information through an appeal to their reasoning faculty. In the conclusion, we present some results from a pilot evaluation of users’ acceptance of OPERA.
1.Introduction
Cancer-backup is the leading provider of information for cancer patients in the UK. On January 2008, it merged with MacMillian Cancer Support. On 22 April 2008, Cancer-backup launched Online Patient Education and Risk Assessment (OPERA). OPERA is an online interactive software program – designed by the Institute of Communication and Health and the Technology-Enhanced Communication Laboratory of the University of Lugano (Switzerland) – that offers personalised information about the risk of having an inherited genetic link for breast and/or ovarian cancer in one's own family. Indeed, 10% of all breast cancer cases have a strong hereditary component relating to mutations on the genes BRCA1 and BRCA2. In addition, women carrying these mutations are at significant risk to develop ovarian cancer (De Grève, Sermijn, De Brakeleer, Ren, and Teugels 2008). OPERA is currently available at: http://www.cancerbackup.org.uk/Aboutcancer/Genetics/GeneticBreastOvarianCancerRiskAssessmentTool.
The communication of risk information on hereditary breast cancer is fraught with difficulties that people have in understanding and evaluating information on risks (Bennet and Calman 1999). Knowledge regarding risk factors for hereditary breast cancer and the availability of specific options have been shown to be limited or partial (Bottorff, Ratner, Johnson, Lovato, and Joab 1998; Bosompra et al. 2000; Honda and Neugut 2004; Kwate, Thompson, Valdimarsdottir, and Bjovberg 2005; Wold, Byers, Crane, and Ahnen 2005; O'Doherty and Suthers 2007). Also people's general perception of their level of risk can be mistaken. The majority of women who have a relative with breast cancer are not at significantly increased risk. Cancer is, however, an emotive word within the general population. Breast cancer has a particularly high political and media profile, and there appears to be a real, but probably exaggerated fear of developing breast cancer in family members of women who have already developed the disease (Bottorff et al. 1998; Hallowell and Murton 1998; Croyle and Lerman 1999; Rees, Fry, and Cull 2001; Hopwood, Shenton, Lalloo, Evans, and Howell 2001). Part of this might stem from the fact that the real extent of a risk translates into assessments, decisions and actions that strongly depend on people's subjective considerations (O'Doherty and Suthers 2007).
As a matter of fact, the way a person understands his/her risk of carrying a BRCA1 or BRCA2 mutation can negatively impact the actions subsequently undertaken. People who have a significant history of breast and ovarian cancer in the family are offered the genetic test by the National Health Service. Here, it is important that these get to know their breast cancer predisposition and take action accordingly (De Grève et al. 2008). Those who have a negative result for disease-conferring mutations might engage in screening programmes only at a level recommended for the general population. But private genetic testing is available. Considering that genetic testing is an expensive, time-consuming and emotionally demanding procedure, it is crucial that people correctly evaluate whether or not to ask for the private option.
With all this in mind, the central goal of OPERA is to help people reach or shape a realistic understanding of their level of risk and the available options. This paper explains the design of OPERA with a focus on the communication challenges encountered during its development. The material discussed here is the outcome of an initial idea of argumentation-driven online genetic counselling that we presented a few years ago in Mackay, Schulz, Rubinelli, and Pithers (2007). In the concluding section of the paper, we suggest possible strengths in OPERA's interactional strategy by relying on a set of data from a pilot evaluation of the instrument.
2.The theoretical framework: risk explanations as arguments
The choice of the message delivered to users by OPERA was a particularly critical one to make. The way a message is structured highlights some features of an issue and makes them salient (i.e. more meaningful and memorable) to an audience (Entman 1993).
In the last few years, due to an increased availability of genetic tests and a growth in genetic counselling, the study of risk communication in genetics – especially in the field of hereditary breast and ovarian cancer – has produced several important contributions (Lerman et al. 1995; Lipkus, Klein, and Rimer 2001; Huiart et al. 2002; Skinner et al. 2002; Contegiacomo et al. 2004; Lobb et al. 2004, 2006; Phelps, Platt, France, Gray, and Iredale 2004; Fransen, Meertens, and Schrander-Stumpel 2006). So far, however, there is no consensus on the value of specific strategies of communication on users’ cognitive, affective and behavioural outcomes together (Edwards et al. 2006, 2008). What counts as a successful strategy of risk communication is even less clear in dealing with online instruments such as OPERA, which have the potential of reaching vast audience, but can be affected by the limitations of the electronic channel (Souka and Yoshida 2005). Thus, Green et al. (2004), showed that an online system was more effective than traditional counselling for increasing knowledge of breast cancer and genetic testing. Yet, traditional counselling was more effective at reducing women's anxiety.
An important study in this field was conducted by Glasspool, Fox, Coulson, and Emery (2001). As part of the Risk Assessment in Genetics (RAGs) project, they developed a computer-based tool for assisting general practitioners and patients in making decisions about genetic risk of cancer. They constructed the system by adopting an argumentation logic approach that assesses genetic risk during a consultation and provides advice in the form of explanations. Glasspool et al. emphasised the use of argumentation as a way to be more in line with how people naturally think about probability and possibility.
Another important study was conducted by Green (2006). In the perspective of helping lay audiences to understand biomedical arguments, Green illustrated a discourse generator that creates an intentional-level representation of arguments.
It has been proved that inducing active processing – i.e. generation, re-organisation and self- explanation of presented material - improves understanding and recall of the information provided (Cosmides and Tooby 1996; Wadey and Frank 1997; Natter and Berry 2005). The use of argumentation in the delivery of health-related information facilitates this active processing by presenting a contextualisation of the claims at stake, i.e. in our case, the level of risk and the options available (Rubinelli and Schulz 2006; Schulz and Rubinelli 2006, 2008). Argumentation offers motivators to individuals’ internal reasons (factual information and intentional states) and can help them in the appraisal of the relative weights of the whole set of motivators as a way to arrive at a decision. Argumentation stimulates deeper processing and more critical thinking over a piece of information (Voss 1991; Kuhn 1993; Zeidler 1997).
In light of this, we designed OPERA according to a conceptual framework which is argumentative in nature, but more refined than RAGs in the personalisation and format of the information it delivers. RAGs produces final explanations as lists of reasons in support of a claim. OPERA works on the basis of a text-generation matrix that combines data from medical knowledge bases and data on the specific patient (Cawsey, Webber, and Jones 1997), and reorganises them into sentences which are fluent and at a higher level of granularity (Bickmore, Giorgino, Green, and Picard 2006). OPERA combines the personalisation of the information – as done by programmes, such as STOP (Smoking Termination through cOmputerised Personalisation, Reiter, Robertson, and Osman 2003) – with an argumentative framework.
3.The analytical framework
Before entering the discussion of the communication strategy adopted for OPERA, we present a summary explanation of how its engine works (Rubinelli, Bolchini, Paolini, and Schulz 2007). The risk level and the appropriate management options run by OPERA are categorised according to the UK National Institute of Health and Clinical Excellence (NICE) guidelines published in 2004, on the basis of (i) the number of relatives on the same side of the family with the same cancer or cancers that are known to run together; (ii) the ages of these relatives at diagnosis and (iii) the closeness of the family relationship with the person who is doing the assessment.
OPERA invites users to enter details of their personal and family history of breast and/or ovarian cancer. It also gathers information on age, sex, ethnicity and history of other cancers that are relatively rare. The user is led through the process by a series of questions about his/her demographic data and family history situation (e.g. “Have you ever been diagnosed with breast cancer?” and “In your family, how many relatives on the same side of the family have had breast and/or ovarian cancer?”). As the user answers the questions, the engine determines which questions should be asked next and finally computes the level of risk via a decision-tree. The inner working of the engine is determined by a number of rules that have the conjunctive form:
IF (A and B and C and …) IMPLIES a; where a can be:
• a question number (determining if a question should be asked or not);
• the level of risk (i.e. low, medium or high risk) the user is grouped into;
• a piece of information (determining if that piece should be delivered to the user or not).
• the summary: a textual expression of the most relevant data to assure the correctness of users’ answers;
• the risk assessment message.
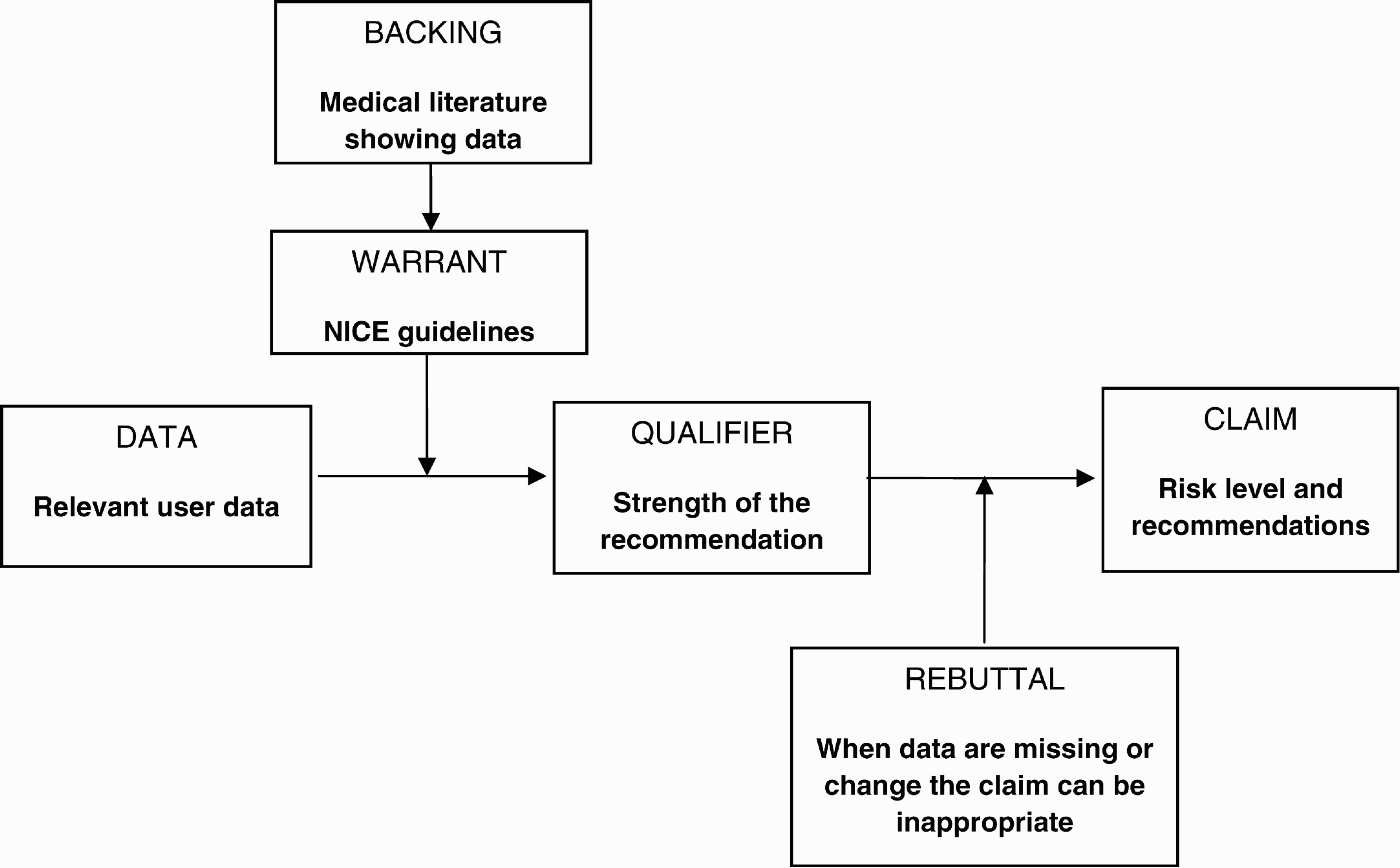
(1) Data: The evidence, facts, background and information on which a claim is made.
(2) Warrant: The knowledge that justifies a claim made using the data.
(3) Backing: The knowledge material that validates the warrant.
(4) Qualifier: The verbalisation of the confidence with which the claim is supported to be true.
(5) Rebuttal: An exception of aspects for which the claim presented is not true.
(6) Claim: The assertion or conclusion put forward for general acceptance.
Figure 1 shows the meta-argument structure of OPERA.
Figure 1.
A meta-argument structure for OPERA, based on Toulmin's argument structure. The structure reads: Given Data, therefore Claim, since Warrant, because Backing, unless Rebuttal.
The above scheme results in the information package delivered by OPERA composed of five main parts, namely:
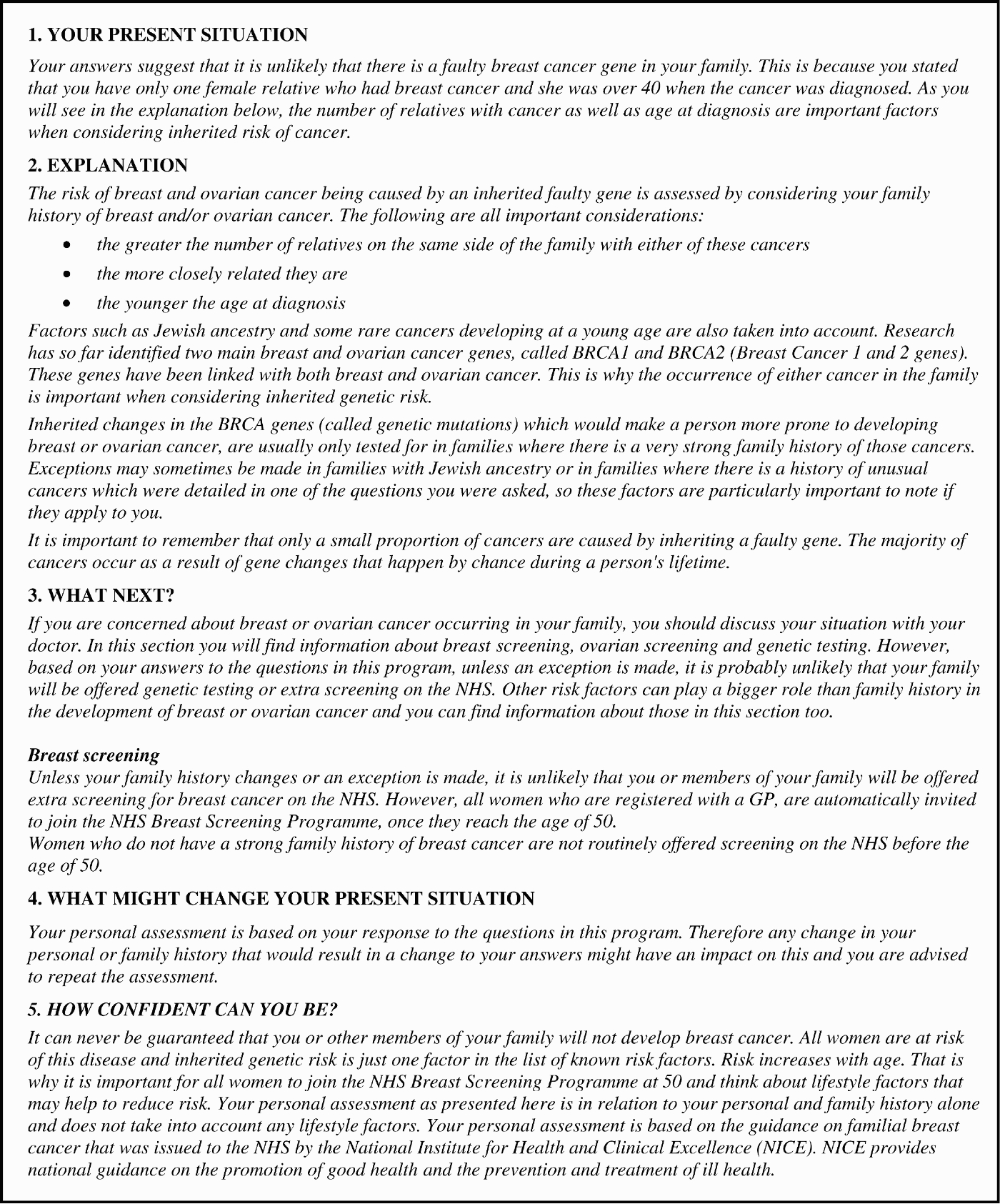
(1) Your present situation (the Claim, part a): an indication of the risk level.
(2) Explanation (the Backing and the Warrant, on the basis of user Data): the justification of “Your present situation” on the basis of the data inserted and the NICE guidelines.
(3) What next? (the Claim, part b): a description of possible options which may be offered and why.
(4) What might change your current situation? (the Rebuttal): a general warning stating that, should users discover new information about their personal or familial history, they have to redo the assessment.
(5) How confident can you be? (the Qualifier): a set of information on the “authority” of Cancer-backup and the NICE guidelines.
Currently aged between 19 and 39, female, not had breast cancer, not had ovarian cancer, no men in the family who have had breast cancer, one female relative diagnosed with breast cancer when she was over 40, no Jewish ancestry, no history of some unusual type(s) of cancer in the family.
Figure 2.
Example of a risk assessment message delivered by OPERA to a low-risk user.
Shifting to the specific contents of the argumentation, we applied a deductive model of argumentation “by association”. The term argumentation by association goes back to the New Rhetoric (Perelman and Olbrecht-Tyteca 1958); it indicates those argumentative moves where two elements that are separate in the mind of an audience are coupled in light of a certain (more or less) explicit relation. Considering that for the New Rhetoric there are different types of argumentation by association, we chose as the main frame for OPERA, an argument by association on “the structure of the reality”. By using as premises “facts” (propositions about reality that can be assumed without further justification, in the context of OPERA information about users’ personal and familial history) and “truths” (propositions that make connections about facts, in our case the NICE guidelines) we designed a message where the main claims (i.e. You are at risk X and You should do Y) are presented as the effects of the premises, with a causal link aimed at transferring the audience's acceptance of the cause to the effect. Overall, the validity of this link is explicitly linked to its source of provenance – the NICE guidelines – that, as such, provides an argumentative input from authority to the factual contents delivered by OPERA.
The reasons behind the risk-level are, then, offered by means of a tailored explanation based on the selection and combination of those attributes that are particularly relevant for supporting the diagnosis of risk in light of the NICE guidelines. Thus, in our example, the explanation of the above risk is justified by pointing out the small number of relatives who have had a history of breast cancer, as well as the age at which the one family member with cancer was diagnosed.
In a second stage, we decided to include a rhetorical (persuasion-oriented) component in OPERA's argumentation that aims at assessing and addressing low-risk users’ eventual concerns. Indeed, one of the key premises from which argumentation theory proceeds is that influencing real audiences is not simply a matter of presenting facts and premises which are scientifically validated. To enhance persuasiveness, it is important to take into account values, attitudes and opinions that people might have (van Eemeren 2010). As discussed by Bennett et al. (2008), about 25% of people that undertake cancer genetic risk assessment based on family history show high level of distress. The main factors that are likely to influence an emotional response to a risk diagnosis include people's understanding of the nature of the health threat and their expectations of its outcome. A deeper personalisation of the argumentation appears here as a necessary requirement for understanding the type of concerns that users might have and meeting the range of their eventual expectations.
We considered the above assumption to be particularly relevant in dealing with the low-risk group. People in this category of risk do not have a significant personal or family history of cancer. Yet, they must have a reason for utilising the programme, including, as mentioned earlier, the possibility that they perceive themselves in a higher risk category. We decided to address this reason to prevent potential resistance to good news. The phenomenon of risk perception resistance is, indeed, known in the literature (Dillard, McCaul, Kelso, and Klein 2006).
To help the assessment of users’ motivations to access OPERA, we screened possible sources of influence on their risk-perception, considering what could influence the perceived threat of a hereditary cancer link. By moving from a social-interaction perspective, we assumed that individuals’ beliefs and opinions are the product of micro-individual characteristics and of a social construction activity performed within the social networks of the single person. Following the indications by the genetic counsellors who collaborated in this project, and have years of experience with the concerns that people express to Cancer-backup, we decided to consider three main possible categories of influence:
1. from healthcare workers;
2. from relatives and friends;
3. from the media.
In the outcome, we added a question at the end of the test for the low-risk group that enquires about the following sources of concern:
You decided to use Cancer-backup's OPERA because:
• You recently read or heard something in the media about cancer in families.
• One or more relatives have had breast or ovarian cancer and you are worried about yourself and/or other family members developing it.
• You have had breast or ovarian cancer and you are worried about your children or other family members developing cancer.
• A friend has recently been diagnosed with breast or ovarian cancer.
• Someone in the health service suggested that you use this programme to find out about your risk.
• None of the above reasons.
It is nevertheless understandable that having a relative with cancer has caused you concern. The following information will hopefully help you to address your concerns and understand that your family history is not significant enough to indicate a higher risk.
The risk of breast and ovarian cancer being caused by an inherited faulty gene is assessed by considering your family history of breast and/or ovarian cancer. The following are all important considerations:
• The greater the number of relatives on the same side of the family with either of these cancers
• The more closely related they are
• The younger the age at diagnosis
• Factors such as Jewish ancestry and some rare cancers developing at a young age are also taken into account.
Overall, the personalisation of the risk assessment is manoeuvred between an essentially deductive argumentation and, for the low-risk target group, a more dialogical component that has the rhetorical goal to enhance the credibility of the message.
4.Pilot-study
4.1.Study design
In this section, we present some indicators of users’ acceptance of OPERA. Data were collected through two self-administered questionnaires 1 month and 3 months after using OPERA during the period between March and July 2008. A non-stratified convenience sample of 61 enrolees aged ≥18, all women, was recruited through advertisements about OPERA on Cancer-backup's website, two London free newspapers and a national newspaper. Eligible participants had to be able to read and speak English, to use a computer and have internet access. No other inclusion or exclusion criteria were used because the intervention was aimed at the general population. Enrolment took place between January and February 2008. Patients were asked to participate only after hearing a description of the project and providing written consent. They were asked to access OPERA in their own homes via a password. Drop-out rate between the first and the second questionnaire was 22% (N = 13). The study was approved by the London Medical Research Ethical Committee.
4.2.Results
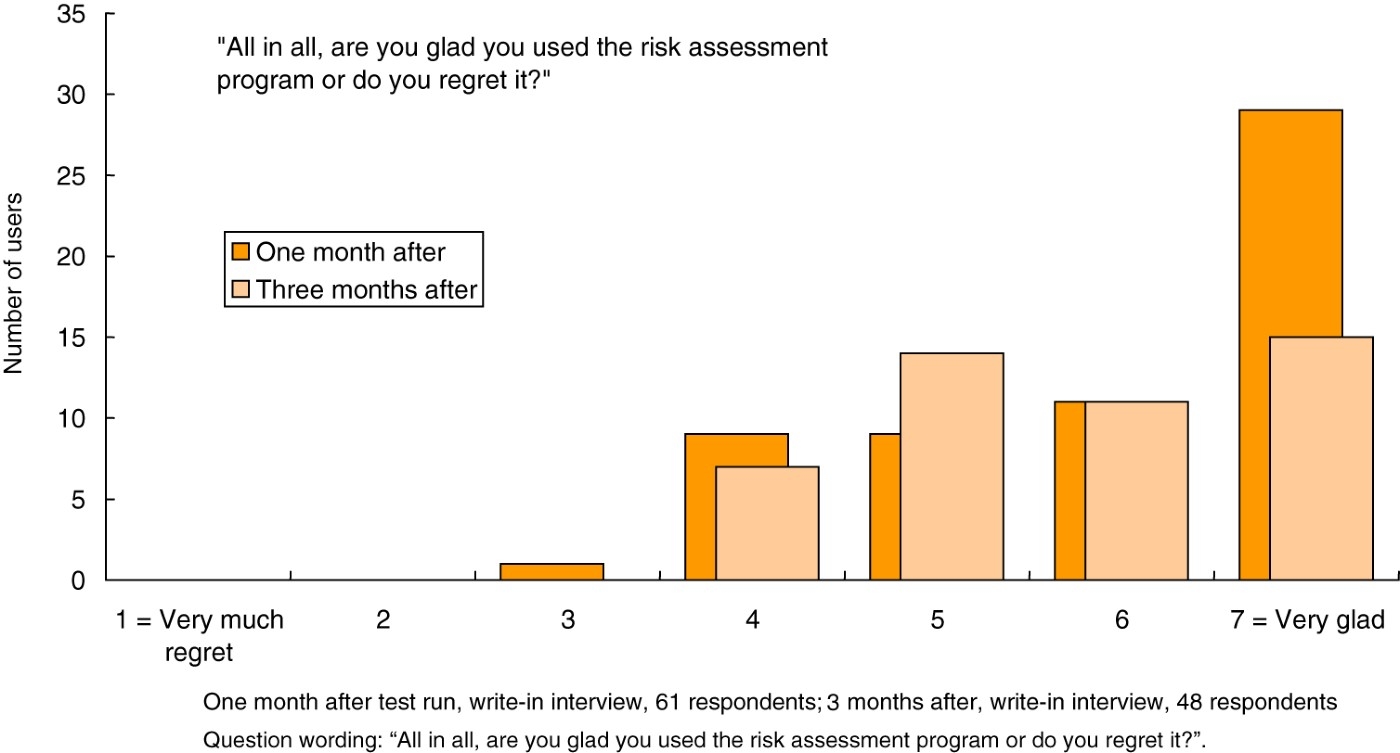
On a general level, users were asked to indicate on a seven-point scale (1=very much regret; 7=very glad) whether they regretted using OPERA or were glad they had done that. Users were more or less all glad they had used OPERA, a month later. That is to say, almost all of them chose scale points on the “glad”-side of the scale. A majority chose even the most extreme point, indicating they were very glad. Some of this enthusiasm wears off after 3 months, but the gladness remains (Figure 3).
Figure 3.
Respondents are and remain glad they used OPERA.
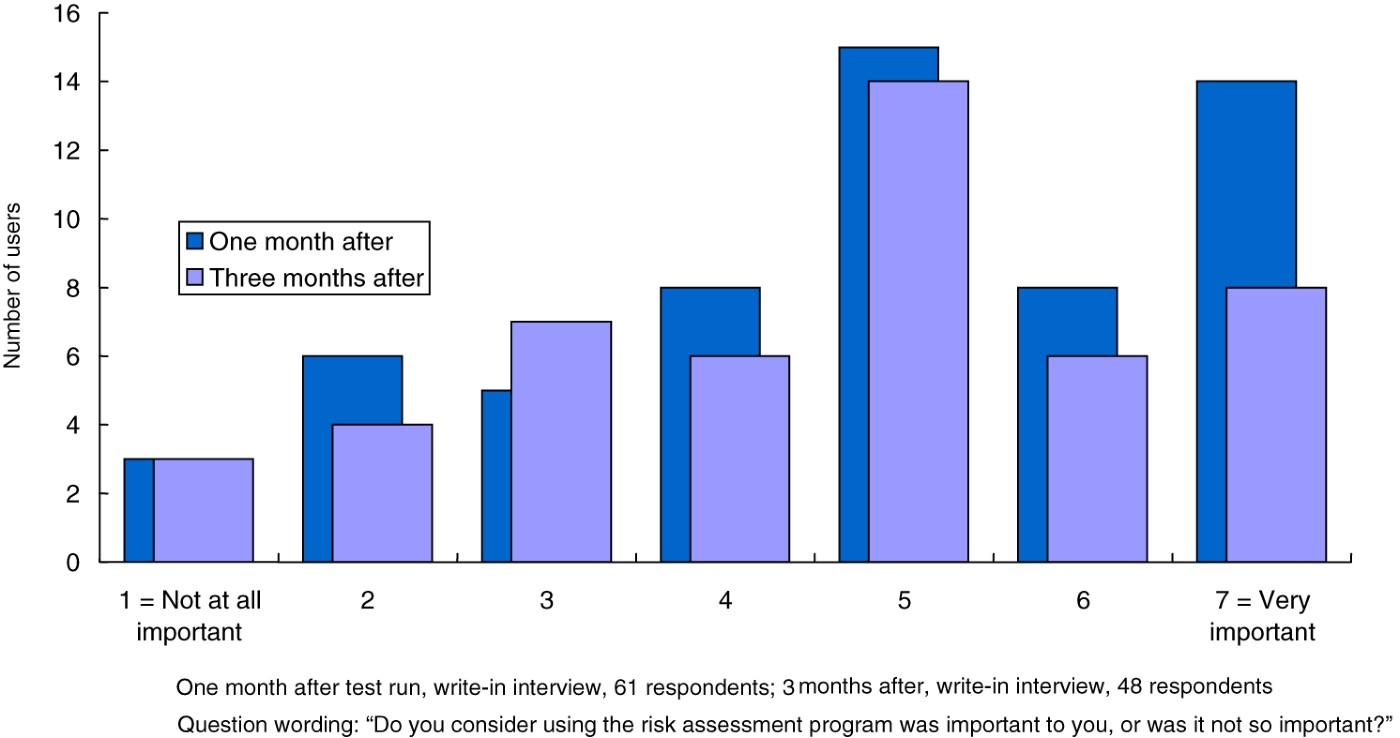
Another indicator of general evaluation is the importance ascribed to using the instrument. For many users, running through OPERA was an important thing to do (Figure 4).
Figure 4.
Using OPERA was an important thing to do.
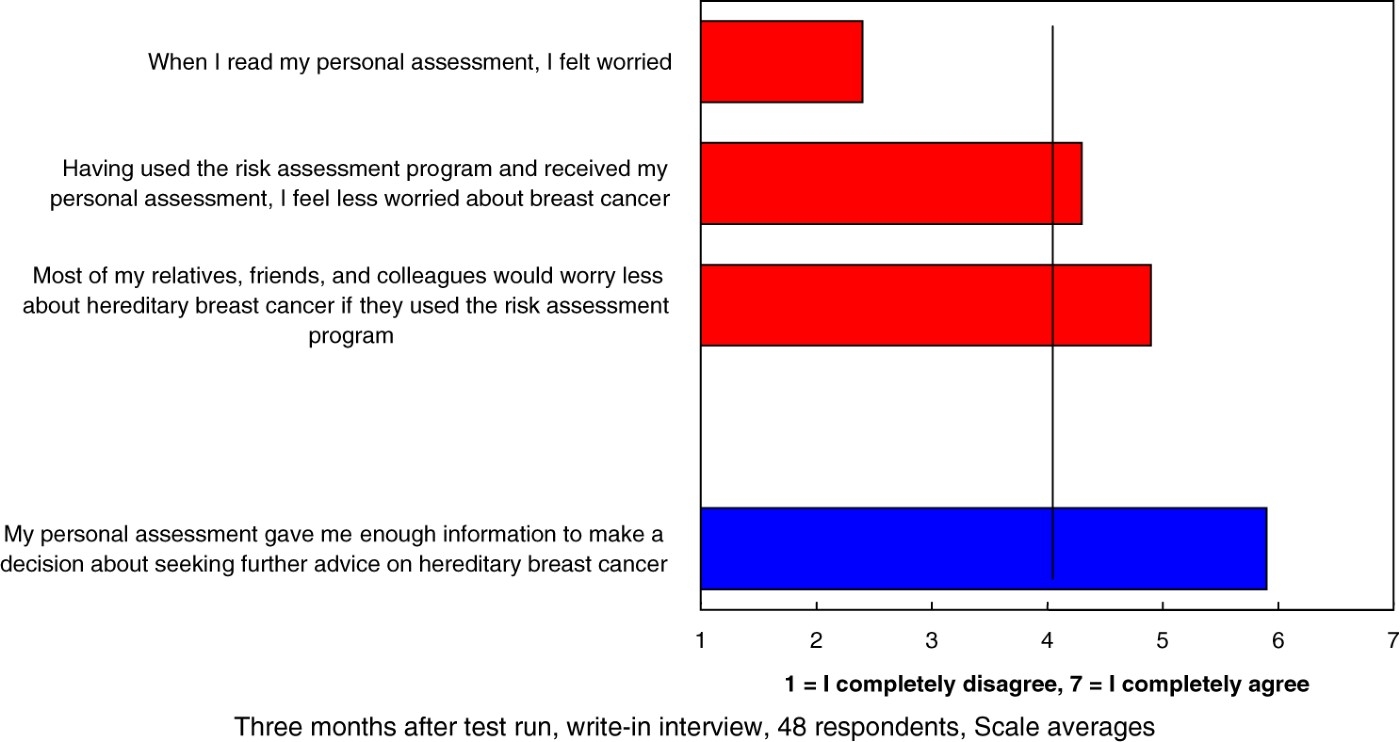
Some effects of using the tool were measured by a question: “Here are some statements about the personal assessment. Please indicate on the scales underneath how much you agree or disagree with each statement”. Scales ran from 1=I completely disagree to 7=I completely agree. There was strong disagreement to a statement that one felt worried after reading the personal assessment. In contrast, respondents significantly agreed on that they felt less worried after using OPERA and that others would also worry less after doing that (Figure 5). There is also strong agreement that OPERA is a good basis for making decisions to seek further advice on breast cancer (Figure 5).
Figure 5.
Assessment of OPERA after three months – worry and relevance.
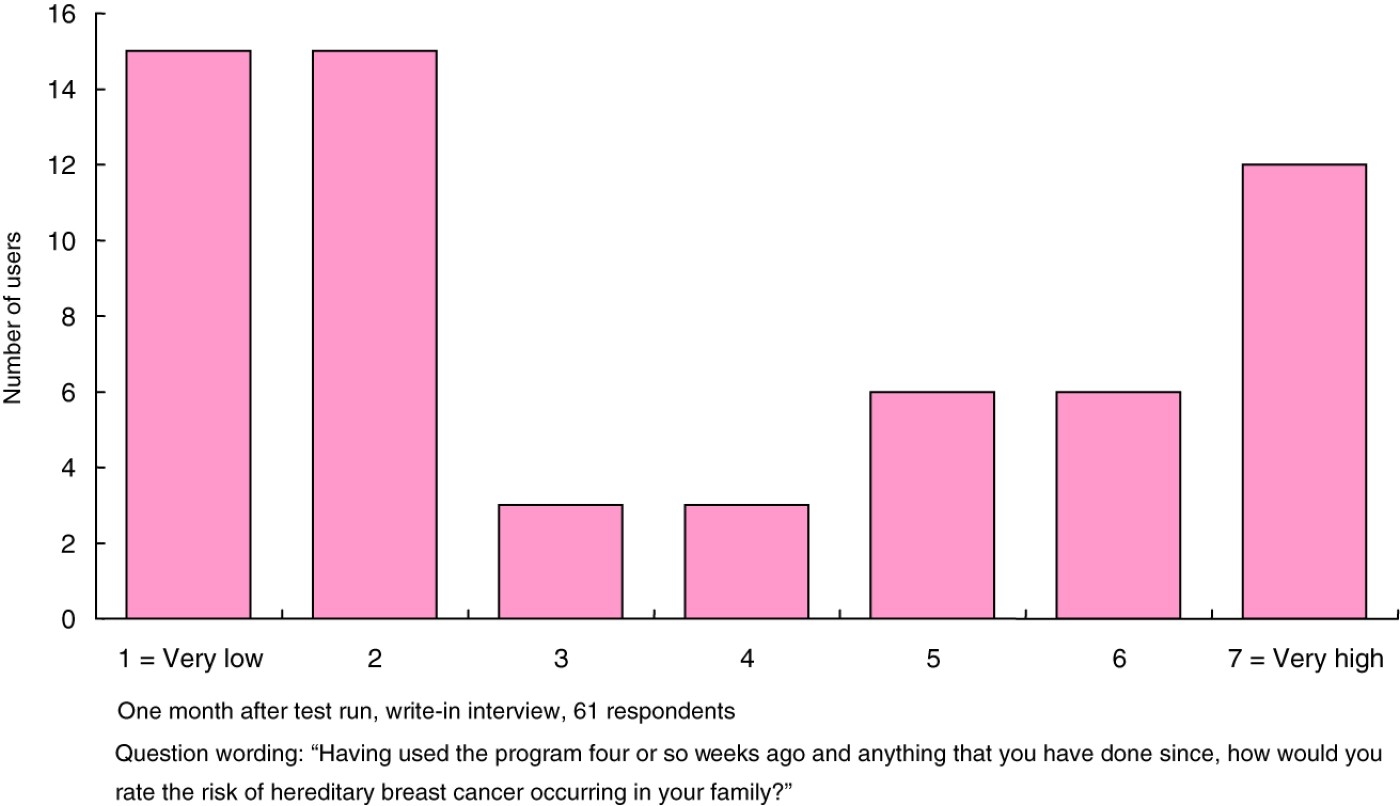
Most respondents judged their family risk for breast cancer either as very low or very high. Respondents clearly tended to choose either one of the extreme scale points on this question, suggesting that the message sent by OPERA is rather clear and does not create confusion (Figure 6).
Figure 6.
Respondents’ assessment of hereditary breast cancer risk in family after having used OPERA.
Forty-nine of the 61 users in this analysis could be classified according to the risk of being afflicted with hereditary breast cancer. Twenty-four respondents ran a low risk, five a moderate risk and 20 a high risk. Leaving aside, for sample size reasons, the moderate risk users, how did high-risk users and low-risk users react to the instrument?
As much as they remember what the personal assessment said, users recalled the gist of the message correctly. However, two users in the low-risk group indicated they were told there may be a faulty gene in the family (Table 1).
Table 1.
Recall of OPERA's assessment of users’ risk.
| Risk of hereditary breast cancer | ||
| Low (%) | High (%) | |
| It is unlikely that there is a faulty breast/ovarian cancer gene in family | 80 | – |
| There is a slightly increased chance that there is a faulty breast/ovarian cancer gene in family | – | – |
| There may be a faulty breast/ovarian cancer gene in family | 8 | 77 |
| Do not recall | 4 | 15 |
| No answer | 8 | 8 |
| 100 (n=24) | 100 (n=20) | |
Note: Question wording: “Please tick which of the statements below was used in your personal assessment. If you do not recall reading any of the statements or would not prefer to answer this, please tick (d) or (e)”.
High-risk users mostly estimated their families’ risk of carrying the faulty gene as high or very high, and low-risk users as low or very low. That is to say: the messages sent by OPERA to the two risk groups reach their destinations. Generally, the assessment received is equally well understood and rated by high- and low-risk users. This conclusion holds true despite the fact that high-risk users tended to indicate in a clearly larger share that they did not learn anything from the personal assessment. The difference is not significant, though (Table 2). As most respondents who did not learn anything said they knew already, it can be assumed that knowledge of hereditary breast cancer and of their personal risk was not new to many of our high-risk users.
Table 2.
Learning from the personal assessment.
| Risk of hereditary breast cancer | ||
| Low (%) | High (%) | |
| Yes, I learned something from the personal assessment | 71 | 47 |
| No, have not learned anything | 29 | 53 |
| 100 (n=24) | 100 (n=19) | |
Notes:
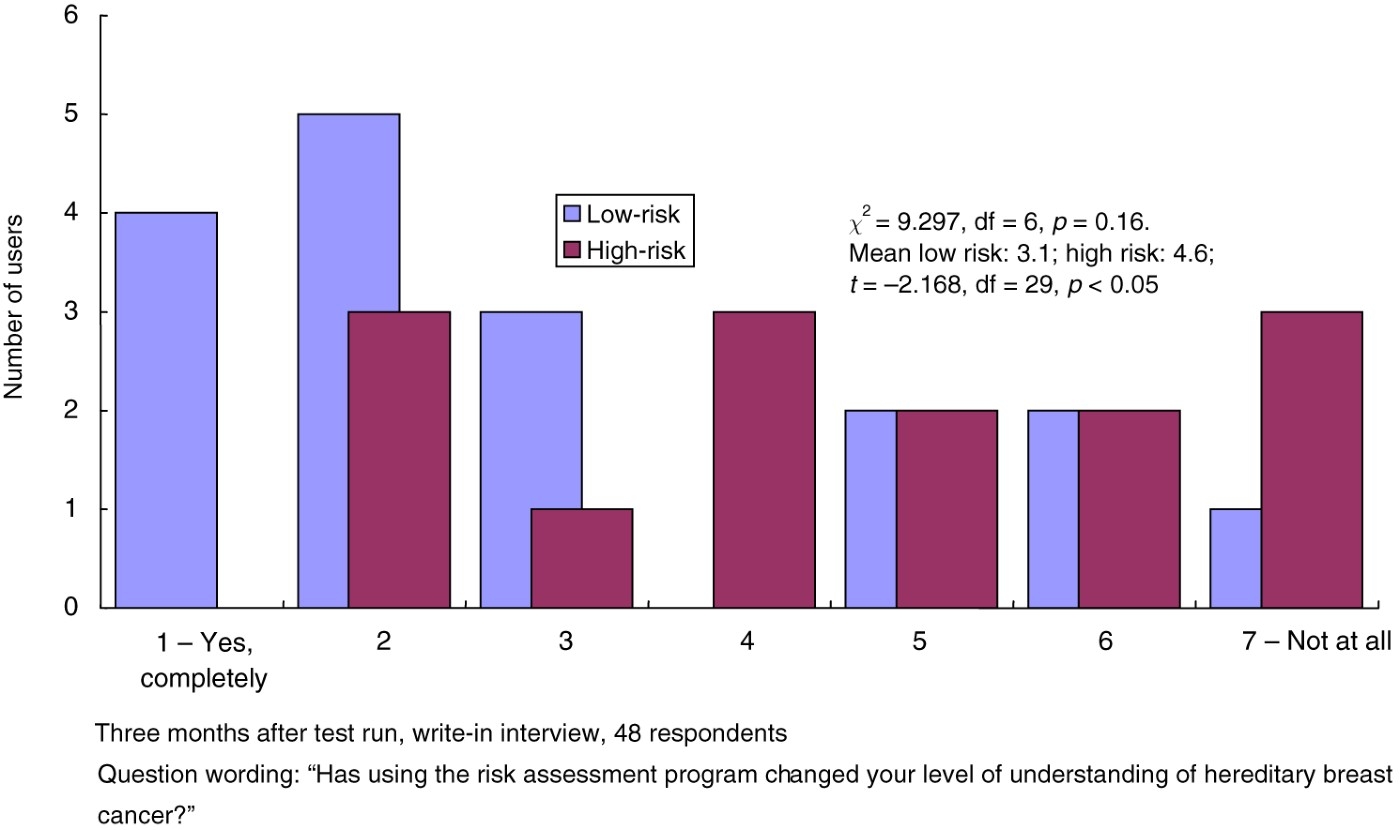
That high-risk users learned less is also evident from a question inquiring whether OPERA has changed a user's level of understanding of hereditary breast cancer (Figure 7).
Figure 7.
Change in level of understanding hereditary breast cancer.
As we pointed out in the introduction of this article, OPERA should help users shape a realistic understanding of the risk. It should stimulate high-risk users to go for further tests, while reducing eventual worries of low-risk users. In this respect, 14 in 17 low-risk users completely disagreed (Point 7 on a 1–7 agree/disagree scale) to the statement “When I read my personal assessment, I felt worried”. In the high-risk group, responses distribute more or less equally across points 2–7 of the scale. Only one person in the low-risk group chose a scale value on the agree side, this is to say one in 17 low-risk users was worried.
Three months after using the tool, 11 in 17 low-risk users agreed (Points 1–3 on a 1–7 agree/disagree scale) to the statement “Having used the risk assessment program, I feel less worried about breast cancer”. Only three low-risk users disagree to that. Among high-risk users, most chose the middle point on the scale, two agreed and three disagreed.
The value of OPERA as an instrument for decision-making, claimed by the majority of users 3 months after the test, finds some specific highlights in the observation of some communication behaviours. A considerable share of high-risk users sought their doctor's advice on hereditary breast cancer, or intended to do that, while low-risk users did not report having seen their doctor or intending to do so (Table 3 and Figure 8). This can indicate that low-risk users were satisfied with their personal assessment and not in need of further medical advice.
Figure 8.
Likelihood of seeking doctor's advice in future.
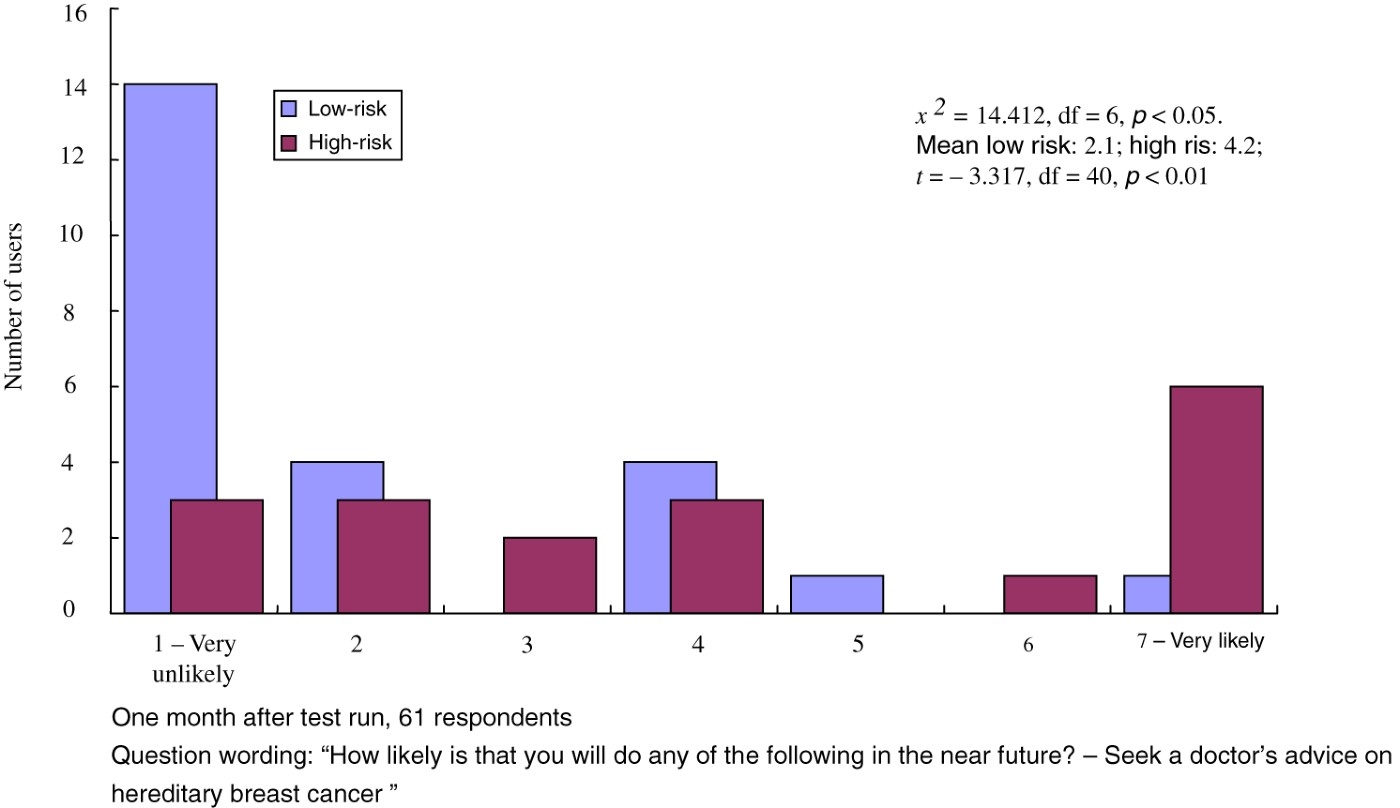
Table 3.
Interpersonal communication behaviour after using OPERA.
| Risk of hereditary breast cancer | ||
| Low (%) | High (%) | |
| Have (once or more often) talked to a doctor or a healthcare professional about hereditary breast cancer risk | ||
| One month after using the tool | 4 (n=24) | 16 (n=19) |
| Three months after using the tool | −(n=17) | 36 (n=14) |
Note: Question wording: “Since using this assessment program, have you talked to a doctor/healthcare professional about hereditary breast cancer risk?”.
5.Discussion and conclusion
In this study, we have created a personalised risk-assessment message that presents an argumentative structure.
The promising evaluation by users in our pilot study points to some value in the communication model applied. At this stage, we can hypothesise the positive impacts on individuals’ risk-communication processing of two inter-related factors:
1. the addition of information content on risks;
2. the appeal to the reasoning faculty of users.
Previous studies have suggested that adding information to help people better understand the real extent of a risk positively impacts people's cognitive outcomes (Hoopwood et al. 2001; Bowen, Burke, McTiernan, Yasui, and Andersen 2004; Edwards et al. 2008). With OPERA, we have focused on the impact of specific contents, i.e. the premises in support of the classification into a risk group and the available options. These premises provide a contextualisation of the risk in a way that can invite users to reflect on the objective (medically based) reasons behind it.
The appeal to reasoning is the second main factor on which OPERA rests. Considering the role of NICEs’ guidelines in the orchestration of OPERA's explanation, we can say that the tool instantiates a deductive argumentation that is, ultimately, based on authority. Indeed, we expect users to recognise two main premises.
The focal premise is that the source of the message (i.e. Cancer-backup) is a genuine expert in cancer information. The second premise is that this source asserts propositions that address the clinical genetic history and the eventual concerns of the person being assessed.
The application of this argument scheme in the design of OPERA has been facilitated by a series of factors. Generally speaking, an argumentative structure like OPERA can be instantiated only if it can answer to the critical questions that are appropriate when evaluating an argument from authority (van Eemeren and Grootendorst 2004).
First of all, the institution acting as a source has to be recognised as an expert in the field. Given the national and international recognition of Cancer-backup, this aspect was less problematic.
Second, problems might arise when there is disagreement among several experts over an issue. When disagreement occurs, it is difficult for a layperson to arrive at a reasoned opinion or decision about the issue. Here, again, being OPERA based on the NICE guidelines, the coherence of the body of knowledge offered is guaranteed. Doubts might arise on whether the programme, being online, is used by non-UK people from countries that apply different national guidelines.
Another important factor is that the interpretation of the expert's opinion by the layperson has to be carefully guided. To be useful, an expert opinion has to be in a form that is clear and intelligible. But, especially in dealing with genomics, the jargon can be technical and resists translation into accessible layman's terms. We had to face the issue of how to transmit clinical guidelines to the lay people. With OPERA, we answered to this aspect by designing the wording together with genetic counsellors who had a live experience on the way people react to their words and their letters during or after consultation.
Further studies will have to address some of the important limitations of this study. First of all, in the recruitment of our sample, we did not fully take into account users’ previous knowledge. In our analysis we relied on users’ declaration on whether or not they have learned from the test. More effort is needed to specify the impact of OPERA according to different levels of pre-existing knowledge on hereditary breast cancer and personal risk.
Another limitation is that in the study, we did not evaluate the contribution of argumentation to the desired outcome, an aspect that, however, we plan to address through more refined experimental design and after the revision of the pilot version of OPERA.
Finally, the argument model used in this current version of OPERA is that all knowledge in the program is stored as pre-compiled arguments, assessed with an a priori screening of users’ informational needs. This is an approach that has the clear advantage of being simple, but it presupposes an anticipation of all possible arguments.
At this stage, we have worked on the assumption that the authority of the scientific guidelines is sufficient enough to meet the range of users’ emotional concerns. More complex argumentative structures, performing a higher level of dialoguing interaction with users, are difficult to implement.
We are currently exploring how theories of argumentation based on the critical discussion of arguers – in particular, the pragma-dialectical theory developed by van Eemeren and Grootendorst (2004) and current models of persuasion (O'Keefe 2002) – can advance theory and practice of this phenomenon. One promising attempt has been made by Grasso, Cawsey, and Jones (2009) who have formalised an agent, Daphne, that advices on controversial issues by using dialectical argumentative strategies. Daphne, however, does not recognise the opponent's argumentative schema and this risks limiting the actual resolution of eventual differences of opinion.
Acknowledgements
We would like to thank Dr James Mackay and Dr Andrea Pithers for the work done together and King's Fund for having supported the creation of OPERA. Our special thanks also go to the reviewers of Argument & Computation who have provided very pertinent and constructive criticism.
References
1 | Bennet, P. and Calman, K. (1999) . Risk Communication and Public Health, Oxford: Oxford University Press. |
2 | Bennett, P., Wilkinson, C., Turner, J., Brain, K., Edwards, R.T., Griffith, G., France, B. and Gray, J. (2008) . Psychological Factors Associated with Emotional Responses to Receiving Genetic Risk Information. Journal of Genetic Counseling, 17: (3): 234–241. |
3 | Bickmore, T., Giorgino, T., Green, N. and Picard, R. (2006) . Guest Editorial: Special Issue on Dialog Systems for Health Communication. Journal of Biomedical Informatics, 39: (5): 465–467. |
4 | Bosompra, K., Flynn, B.S., Ashikaga, T., Rairikar, C.J., Worden, J.K. and Solomon, L.J. (2000) . Likelihood of Undergoing Genetic Testing for Cancer Risk: A Population-based Study. Preventive Medicine, 30: (2): 155–166. |
5 | Bottorff, J., Ratner, P., Johnson, J., Lovato, C. and Joab, A. (1998) . Communicating Cancer Risk Information: The Challenges of Uncertainty. Patient Education & Counseling, 33: (1): 67–81. |
6 | Bowen, D.J., Burke, W., McTiernan, A., Yasui, Y. and Andersen, M. (2004) . Breast Cancer Risk Counseling Improve Women's Functioning. Patient Education and Counseling, 53: (1): 79–86. |
7 | Cawsey, A.J., Webber, B.L. and Jones, R.B. (1997) . Natural Language Generation in Health Care. Journal of the American Medical Informatics Association, 4: (6): 473–482. |
8 | Contegiacomo, A., Pensabene, M., Capuano, I., Tauchmanova, L., Federico, M., Turchetti, D., Cortesi, L., Marchetti, P., Ricevuto, E., Cianci, G., Venuta, S., Barbieri, V., Silingardi, V. and Italian Network on Hereditary Breast Cancer. (2004) . An Oncologist-based Model of Cancer Genetic Counseling for Hereditary Breast and Ovarian Cancer. Annals of Oncology, 15: (5): 726–732. |
9 | Cosmides, L. and Tooby, J. (1996) . Are Humans Good Intuitive Statisticians After All? Rethinking Some Conclusions from the Literature on Judgment under Uncertainty. Cognition, 58: (1): 1–73. |
10 | Croyle, R.T. and Lerman, C. (1999) . Risk Communication in Genetic Testing for Cancer Susceptibility. Journal of the National Cancer Institute. Monographs, 25: : 59–66. |
11 | De Grève, J., Sermijn, E., De Brakeleer, S., Ren, Z. and Teugels, E. (2008) . Hereditary Breast Cancer: From Bench to Bedside. Current Opinion in Oncology, 20: (6): 605–613. |
12 | Dillard, A.J., McCaul, K.D., Kelso, P.D. and Klein, W.M. (2006) . Resisting Good News: Reactions to Breast Cancer Risk Communication. Health Communication, 19: (2): 115–123. |
13 | Edwards, A., Gray, J., Clarke, A., Dundon, J., Elwyn, G., Gaff, C., Hood, K., Iredale, R., Sivell, S., Shaw, C. and Thornton, H. (2008) . Interventions to Improve Risk Communication in Clinical Genetics: Systematic Review. Patient Education and Counseling, 71: (1): 4–25. |
14 | Edwards, S., Sivell, S., Dundon, J., Elwyn, G., Evans, R., Gaff, C., Iredale, R., Shaw, C., Thornton, H., Gray, J., Clarke, A. and Atkinson, P. (2006) . “Effective Risk Communication in Clinical Genetics – A Systematic Review”. Report to: Department of Health, Genetics Research Program – Health Services Research Cardiff Centre for Health Sciences Research |
15 | van Eemeren, F.H. and Grootendorst, R. (2004) . A Systematic Theory of Argumentation. The Pragma-dialectical Approach, Cambridge: Cambridge University Press. |
16 | van Eemeren, F.H. (2010) . Strategic Maneuvering in Argumentative Discourse, Philadelphia, PA: John Benjamins Publishing Company. |
17 | Entman, R. (1993) . Framing: TOWARD a Clarification of a Fractured Paradigm. Journal of Communication, 43: (4): 51–58. |
18 | Fransen, M., Meertens, R. and Schrander-Stumpel, C. (2006) . Communication and Risk Presentation in Genetic Counseling Development of Checklist. Patient Education and Counseling, 61: (1): 126–133. |
19 | Glasspool, D.W., Fox, J., Coulson, A.S. and Emery, J. (2001) . Risk Assessment in Genetics: a Semi-quantitative Approach. Studies in Health Technology and Informatics, 84: (Pt1): 459–463. |
20 | Grasso, F., Cawsey, A. and Jones, R. (2000) . Dialectical Argumentation to Solve Conflicts in Advice Giving: A Case Study in the Promotion of Healthy Nutrition. International Journal of Human-Computer Studies, 53: (6): 1077–1115. |
21 | Green, N. Generation of Biomedical Arguments for Lay Readers. Proceedings of the Fourth International Natural Language Generation Conference. July (2006) , Sydney. pp. 114–121. |
22 | Green, M.J., Peterson, S.K., Baker, M.W., Harper, G.R., Friedman, L.C., Rubinstein, W.S. and Mauger, D.T. (2004) . Effect of a Computer-based Decision aid on Knowledge, Perceptions, and Intentions about Genetic Testing for Breast Cancer Susceptibility: A Randomized Controlled Trial. Journal of the American Medical Association, 292: (4): 442–452. |
23 | Hallowell, N. and Murton, F. (1998) . The Value of Written Summaries of Genetic Consultations. Patient Education and Counseling, 35: (1): 27–34. |
24 | Honda, K. and Neugut, A.I. (2004) . Associations Between Perceived Cancer Risk and Established Risk Factors in a National Community Sample. Cancer Detection and Prevention, 28: (1): 1–7. |
25 | Hopwood, P., Shenton, A., Lalloo, F., Evans, D.G.R. and Howell, A. (2001) . Risk Perception and Cancer Worry: An Exploratory Study of the Impact of Genetic Risk Counseling in Women with a Family History of Breast Cancer. Journal of Medical Genetics, 38: (2): 139–142. |
26 | Huiart, L., Eisinger, F., Stoppa-Lyonnet, D., Lasset, C., Noguès, C., Vennin, P., Sobol, H. and Julian-Reynier, C. (2002) . Effects of Genetic Consultation on Perception of a Family Risk of Breast/Ovarian Cancer and Determinants of Inaccurate Perception after the Consultation. Journal of Clinical Epidemiology, 55: (7): 665–675. |
27 | Kwate, N.O.A., Thompson, H.S., Valdimarsdottir, H.B. and Bjovberg, D.H. (2005) . Etiological Attributions for Breast Cancer among Healthy African American and European American Women. Psycho-oncology, 14: (5): 421–425. |
28 | Kuhn, D. (1993) . Science as Argument: Implications for Teaching and Learning Scientific Thinking. Science Education, 77: (3): 319–337. |
29 | Lerman, C., Lustbader, E., Rimer, B., Daly, M., Miller, S., Sands, C. and Calshem, A. (1995) . Effects of Individualized Breast Cancer Risk Counseling: A Randomized Trial. Journal of the National Cancer Institute, 87: (4): 286–292. |
30 | Lipkus, I.M., Klein, W.M. and Rimer, B.K. (2001) . Communicating Breast Cancer Risks to Women Using Different Formats. Cancer Epidemiology, Biomarkers & Prevention, 10: (8): 895–898. |
31 | Lobb, E.A., Butow, P.N., Barratt, A., Meiser, B., Gaff, C., Young, M.A., Haan, E., Suthers, G., Gattas, M. and Tucker, K. (2004) . Communication and Information-giving in High-risk Breast Cancer Consultations: Influence on Patient Outcomes. British Journal of Cancer, 90: (2): 321–327. |
32 | Lobb, E., Butow, P., Moore, A., Barratt, A., Tucker, K., Gaff, C., Kirk, J., Dudding, T. and Butt, D. (2006) . Development of a Communication Aid to Facilitate Risk Communication in Consultations with Unaffected Women from High Risk Breast Cancer Families: A Pilot Study. Journal of Genetic Counseling, 15: (5): 393–405. |
33 | Mackay, J., Schulz, P.J., Rubinelli, S. and Pithers, A. (2007) . Online Patient Education and Risk Assessment: Project OPERA from Cancerbackup. Patient Education and Counseling, 67: (3): 261–266. |
34 | Natter, H. and Berry, D. (2005) . Effects of Active Information Processing on the Understanding of Risk Information. Applied Cognitive Psychology, 19: : 123–135. |
35 | O'Doherty, K and Suthers, G.K. (2007) . Risky Communication: Pitfalls in Counseling about Risk, and How to Avoid Them. Journal of Genetic Counseling, 16: (4): 409–417. |
36 | O'Keefe, O. (2002) . Persuasion. Theory & Research, London: Sage Publication. |
37 | Perelman, C. and Olbrecht-Tyteca, L. (1958) . Traité de l'argumentation. La nouvelle rhétorique, Paris: Presses Universitaires de France. |
38 | Phelps, C., Platt, K., France, L., Gray, J. and Iredale, R. (2004) . Delivering Information about Cancer Genetics Via Letter to Patients at Low and Moderate Risk of Familial Cancer: A Pilot Study in Wales. Familial Cancer, 3: (1): 55–59. |
39 | Rees, G., Fry, A. and Cull, A. (2001) . A Family History of Breast Cancer: Women's Experiences from a Theoretical Perspective. Social Science and Medicine, 52: (9): 1233–1240. |
40 | Reiter, E., Robertson, R. and Osman, L.M. (2003) . Lessons from a Failure: Generating Tailored Smoking Cessation Letters. Artificial Intelligence, 144: (1): 41–58. |
41 | Rubinelli, S. and Schulz, P.J. (2006) . Let Me Tell You Why! When Argumentation in Doctor–patient Interaction Makes a Difference. Argumentation, 20: (3): 353–375. |
42 | Rubinelli, S., Bolchini, D., Paolini, P. and Schulz, P.J. Designing Tailored Arguments in Online Risk Assessment Tools. Proceedings of the 11th International Conference on User Modeling, Personalisation for e-Health. pp. 57–60. |
43 | Schulz, P.J. and Rubinelli, S. (2006) . Healthy Arguments for Literacy in Health. : 86–95. AAAI Spring Symposium Technical Report |
44 | Schulz, P.J. and Rubinelli, S. (2008) . Arguing for the Patient. Informed Consent and Strategic Maneuvering in Doctor–patient Interaction. Argumentation, 22: (3): 423–432. |
45 | Skinner, C.S.S., Berry, J.M., Calingaert, D., Marcom, B., Sugarman, P.K., Winer, J., Stefanek, M., Vogel, V. and Lerman, C. (2002) . Pre-counseling Education Materials for BRCA Testing: Does Tailoring Make a Difference?. Genetic Testing, 6: (2): 93–105. |
46 | Souka, M. and Yoshida, K. (2005) . Health Risk Appraisal Using Internet Technology. Methods of Information in Medicine, 44: (2): 310–314. |
47 | Toulmin, S. (1958) . The Uses of Argument, Cambridge: Cambridge University Press. |
48 | Voss, J.F. (1991) . Learning to Reason via Instruction in Argumentation. Learning & Instruction, 1: (4): 337–350. |
49 | Wadey, V. and Frank, C. (1997) . The Effectiveness of Patient Verbalization on Informed Consent. Canadian Journal of Surgery, 40: (2): 124–128. |
50 | Wold, K.S., Byers, T., Crane, L.A. and Ahnen, A. (2005) . What Do Cancer Survivors Believe Causes Cancer? (United States). Cancer Causes Control, 16: (2): 115–123. |
51 | Zeidler, D.L. (1997) . The Central Role of Fallacious Thinking in Science Education. Science Education, 81: (4): 483–496. |


