
Speech and language therapy service provision to UK intensive care units: A national survey
Abstract
BACKGROUND:
The role of Speech and Language Therapists (SLTs) in intensive care units (ICUs) has become increasingly recognised. This survey was developed in response to concern amongst UK SLTs that service provision was insufficient.
OBJECTIVE:
The primary objective was to benchmark and describe UK pre-pandemic SLT ICU service provision. Secondary objectives included: identifying factors which might explain differences in SLT service provision, identifying unmet needs and good practice, and informing recommended SLT staffing levels.
METHODS:
An online survey was distributed through UK SLT networks and social media. Quantitative data were reported descriptively, and content analysis was conducted with qualitative data.
RESULTS:
Responses were received from 64 hospitals, representing three paediatric services and 61 adult services. Average staffing ratios of 0.03 and 0.01 whole time equivalent (WTE) were reported for these respectively. Most services (77&) received no funding from their ICU for SLT staffing. Few reported an adequate SLT service for communication (12&), swallowing (16&) and tracheostomy weaning interventions (11&). Compliance with national guidance for SLT-led communication and swallowing input for all tracheostomised patients was achieved by 27& of sites.
CONCLUSIONS:
Staffing levels at many sites were insufficient to provide a consistent and responsive service. The findings contributed to a recommendation of 0.1 WTE SLT per ICU bed, which was incorporated into Edition 2 of the Guidelines for the Provision of Intensive Care Services. This survey identified barriers and facilitators to providing an adequate SLT service for critically ill patients that may assist service development initiatives and guide further research.
1Introduction
The role of Speech and Language Therapists (SLTs) in intensive care units (ICUs) has developed over the last two decades (McRae et al., 2019). SLTs provide crucial interventions for swallowing, communication, and tracheostomy weaning (McGrath & Wallace, 2014). Post-extubation dysphagia, laryngeal injury, and dysphonia are common (41% 83% and 76% respectively) (Brodsky et al., 2018; McIntyre et al., 2020; Skoretz et al., 2010). SLTs play an important role in identifying and treating these patients. SLT-led Fibreoptic Endoscopic Evaluation of Swallowing (FEES) provides objective information regarding swallowing function, saliva management, and laryngeal function which can guide swallowing rehabilitation, tracheostomy weaning, laryngeal rehabilitation, and early resumption of oral intake (Hafner et al., 2008; Hales et al., 2008; Wallace & McGrath, 2021). Voicelessness in ICU can have a devastating psychological impact on patients (Happ, 2000). SLTs play a vital role in providing laryngeal rehabilitation through the use of one-way valves, communication aids, therapy exercises and ICU staff training (Freeman-Sanderson et al., 2016; Zaga et al., 2019). Despite the growing body of evidence of the value of SLT in ICU, a recent study found that only 55% (n = 137/251) of SLTs internationally are involved in cuff deflation and one-way valve trials in ventilator-dependent patients, and that 14% of ICU FEES services do not include SLTs (Rowland et al., 2022).
Prior to the development of this study, research investigating the UK SLT workforce and service delivery in ICU had been lacking. However, since this survey was disseminated several international studies have explored the ICU SLT workforce and service delivery (Cardinal et al., 2020; Rowland et al., 2022; Spronk et al., 2022; Twose et al., 2022).
An expert committee of the UK-wide body representing SLTs working within ICU (the Royal College of Speech and Language Therapy Tracheostomy Clinical Excellence Network, RCSLT Tracheostomy CEN) was aware of significant issues relating to SLT service provision in ICUs in the UK from communication from RCSLT Trache CEN members. Concerns included a national shortage of appropriately trained and competent SLTs within ICU, variation in SLT service provision, and inability to meet best practice as outlined in national guidance (GPICS, 2015; National Institute for Health and Clinical Excellence (NICE), 2009; NCEPOD, 2014; RCSLT, 2014; Royal College of Speech & Language Therapists, 2014). At the time of conducting this study, national guidance recommended:
• Early intervention for communication and swallowing and for all patients with tracheostomies
• A minimum of 45 minutes daily therapy, Monday to Friday, with SLT
• SLT should be a key and fully integrated member of the ICU multi-disciplinary team (MDT)
The primary objective of this study was to benchmark and describe UK SLT ICU service provision. Secondary objectives included: identifying factors which might explain differences in SLT service provision, identifying unmet needs and good practice, and informing SLT staffing levels for revised versions of the Guidelines for the Provision of Intensive Care Services (GPICS); a multi-disciplinary document that is considered the ‘definitive reference source for planning and delivery of UK Intensive Care Services’ (GPICS, 2019).
2Methods
This descriptive, observational study used a cross-sectional, online, single-event survey to evaluate SLT service provision to adult and paediatric ICUs in the UK. Ethical approval was obtained from the School of Medicine Research Ethics Committee at the University of Leeds on 23 November 2018 (MREC: 18-007). This study conforms with the Code of Ethics of the World Medical Association (Declaration of Helsinki) and was undertaken with the understanding and written consent of each subject. The open, online survey was developed and compiled by the RCSLT Tracheostomy CEN committee using Jisc Online Surveys as required by the University of Leeds. The survey was piloted by three, ICU SLTs and the final survey comprised 42 questions exploring: service demographics, response times and access to SLT, referral and assessment, patient management, MDT collaboration, best practice and service improvement and innovation. The survey included both closed questions (multiple choice and Likert scales) and open, free text questions. Items were not randomised or alternated and adaptive questioning was not employed and mandatory questions were avoided, as they disregard the voluntary nature of a survey (Dillman, 1999). Participants were able to review and edit their responses and save and complete the survey later. In order to protect participants’ anonymity cookies, log files, and IP addresses were not recorded, which also prevented calculation of unique site visitors and view rate. Participant registration was not required, and timestamps were not recorded. Duplication of survey completion could be analysed via the name of the hospital and Trust provided by participants. Supplemental Appendix A presents the survey and embedded participation information sheet.
Convenience sampling was employed, with distribution via social media and through UK SLT networks, between December 2018 and March 2019. The survey targeted SLTs working in adult, paediatric and neonatal ICUs and respondents were asked to complete one survey per SLT service. Survey completion was voluntary, with no incentives offered. See Appendix B for the survey adverts used.
All data were analysed, including incomplete responses, with omissions of questions recorded as ‘no response’. Quantitative data were analysed using Microsoft Excel® (2016) and reported descriptively with percentages (n, %) and ranges, with no statistical analysis or correction. In order to identify any good practice that might be associated with better staffing, a sub-analysis was conducted on three adult services with the highest staffing levels. Inductive, content analysis of the qualitative data was carried out using NVivo® version 12 (QSR International). Qualitative data were coded by members of the study team (CM, SW, CI, HN) with a minimum of 3 people independently coding each question. Discrepancies were resolved through discussion and a consensus decision was made. In order to contribute recommended staffing levels to the revised GPICS guidance, a committee review of the participant estimated staffing requirements for an adequate 5-day service responses was conducted. The survey was reported in line with the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) (Eysenbach, 2004) including recommended reporting of participation and completion rates, rather than response rate. See supplemental Appendix C for the complete CHERRIES checklist.
3Results
3.1Response sources
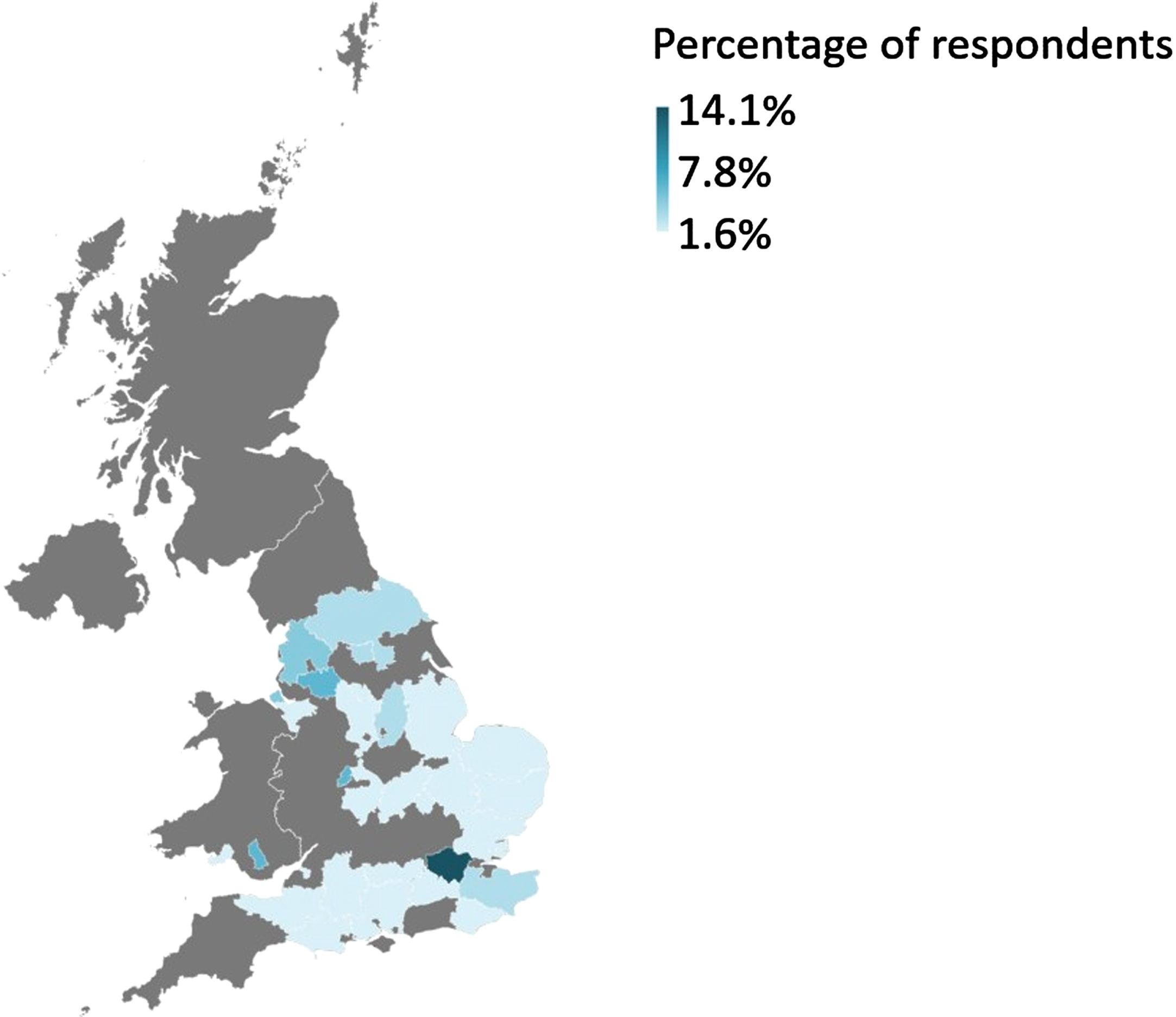
Sixty-four responses were received from a range of university teaching (n = 30, 47%), district general (n = 29, 45%), and specialist (n = 5, 8%) hospitals. Three paediatric and 61 adult services were represented, with no duplicate responses. The distribution of responses across the UK is shown in Fig. 1. The participation rate –the percentage of visitors to the online survey webpage who participated in the survey –was 11%. The completion rate of those participating in the survey was 100%. The UK response rate for Trusts/Health Boards was 35% (based on the figure of 160 Trusts/Health Boards (Health and Social Care Online, 2021; NHS Improvement, 2019; NHS Inform, 2021; NHS Wales, 2006).
Fig. 1
Map of the distribution of hospital or NHS Trust respondents by region of the UK.
3.2Staffing
The reported median SLT staffing ratio (the number of staff per ICU bed) for paediatrics and neonatal services was 0.03 (range: 0.01–0.04) whole time equivalent (WTE), and 0.01 (range: 0.001–0.05) WTE for adults. Seventeen services (27%) employed a band 8a (Clinical Specialist or Clinical Lead) or 8b (Consultant) SLT. Of these, 94% (n = 16/17) were either employed in management roles or part-time and not routinely clinical in ICU (Table 1). The majority of services were unable to provide daily (n = 44/66, 69%), weekend (n = 62/64, 97%) or bank holiday cover (n = 60/63, 94%). Reasons given for insufficient resources included: lack of funding (n = 32/59, 54%), business cases for staffing being declined (n = 6/59, 10%), historical staffing levels not increased with changing role or demand (n = 5/59, 8%), increased demand from increased referrals (n = 5/59, 8%), skill limitation (n = 5/59, 8%), service pressures elsewhere (n = 3/59, 5%) and a perceived lack of MDT understanding of SLT role (n = 3/59, 5%). The majority of services received no ring-fenced funding from their ICU for SLT (shown in Fig. 2). Thirty respondents (47%) stated that their SLT service in ICU was provided by in-reach from the generic hospital SLT cover (which may or may not have included SLTs with ICU skills), and 16 (25%) specifically stated that their service was provided by non-ICU specialist SLTs. In the two years
Fig. 2
Percentage of ICU SLT staffing funded directly by ICU.
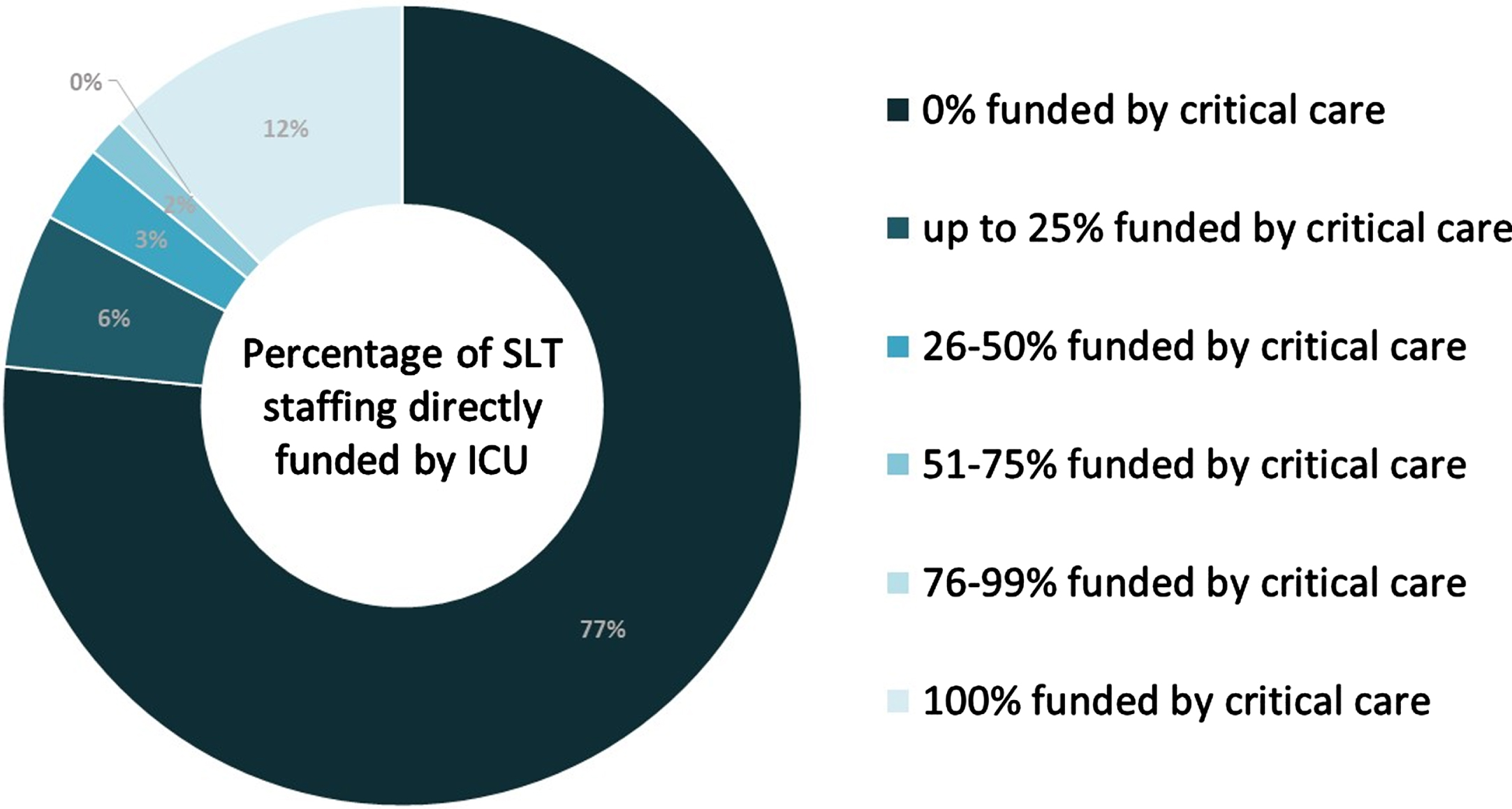
Table 1
Banding of staff
| Banding of Staff | Number of Services with Staff at Banding (%) |
| 8c (Consultant) | 0 (0%) |
| 8b (Consultant/Head of Service) | 2 (3%) |
| 8a (Clinical Specialist/Clinical Lead) | 15 (23%) |
| 7 (Highly Specialist) | 52 (81%) |
| 6 (Specialist) | 27 (42%) |
| 5 (Basic Grade) | 2 (3%) |
| 4 (Technical Instructor/Assistant) | 1 (2%) |
| 3 (Assistant) | 0 (0%) |
Various potential risks were felt to be associated with inadequate staffing (see Table 2). Respondents also identified a range of facilitators to improving SLT service provision, including management support improving relationships “presence on ICUs combined with good working relationships with the wider MDT”, and funding for posts “dedicated funding for a full time Band 7 SLT”.
Table 2
Potential risks associated with insufficient SLT staffing
| Risk | Number of Services (%) |
| Increased length of stay | 20 (53%) |
| Increased frequency of aspiration or aspiration pneumonia | 24 (42%) |
| Difficulty communicating with staff/family | 17 (30%) |
| Negative impact on patients’ psychological well-being | 17 (30%) |
| Lack of support for communication difficulties | 15 (26%) |
| Increased days with tracheostomy | 13 (23%) |
| Increased duration of requiring enteral nutrition | 12 (21%) |
| Slow SLT response times | 12 (21%) |
| Little or no rehabilitation for swallowing/communication difficulties | 11 (19%) |
| Delayed commencement of oral intake | 10 (18%) |
| Delayed weaning | 10 (18%) |
| Negative impact on patient outcomes | 10 (18%) |
| Poor swallowing management | 7 (12%) |
| Difficulty for patients to participate in care decisions and treatment | 7 (12%) |
| Reduced quality of life for patients | 7 (12%) |
| Other professional taking on SLT roles | 6 (11%) |
| Risks associated with dysphagia | 6 (11%) |
| Under-diagnosed dysphagia | 6 (11%) |
3.3Clinical service provision
Response times to referrals varied greatly; 16% (n = 10/64) reported patients were seen on the same working day, 45% (n = 29/64) within one working day, and 23% (n = 15/64) reported waits of up to two working days. Few respondents reported an adequate SLT service for communication (n = 8/64, 12%), swallowing (n = 10/64, 16%), and tracheostomy weaning (n = 7/64, 11%). Access to FEES occurred in 58% of sites (n = 37/64), however, waiting times varied. Sixty percent of services (n = 22/37) conducted 1–5 FEES per month, 14% (n = 5/37) conducted 6–20 per month, with one service providing 31 –35 FEES per month. A wait time of 1–3 days for FEES was reported by 70% of services (n = 26/37), while 11% (n = 4/37) had a wait of ≥7 days. Barriers to delivering a FEES service in ICU were funding “not able to secure funding for the equipment”, and skill-mix based “no-one trained in FEES, no funding to train”.
Less than a third of SLTs reported being often (n = 19/64, 32%) or always (n = 10/64, 17%) involved in trials of Passy Muir Valves (PMV); a key aspect of laryngeal assessment and weaning in tracheostomised patients (Wallace et al., 2022). SLT involvement in identifying Augmentative and Alternative Communication (AAC) techniques was even less frequent (often: n = 15/64, 23%; always: n = 8/64, 13%). Compliance with the GPICS guidance of SLT-led communication and swallowing input for all patients with a tracheostomy was reportedly achieved at 27% (n = 17/64) of sites. Ability to meet the GPICS guidelines (GPICS, 2015) of 45 minutes of SLT rehab 5 days a week was rare (n = 2/64, 3%), with 84% (n = 52/62) of respondents citing staffing as a barrier to achieving this.
3.4Referrals
Eighty percent of respondents (n = 51/64) felt under-referral to SLT was a problem and half of respondents (n = 33/64, 52%) reported that there was an issue with timeliness of referrals. Reasons identified for this included a perceived lack of MDT understanding of the SLT role and impact, lack of awareness of a problem (particularly relating to post-extubation dysphagia), MDT perception of lack of SLT service capacity to respond to referrals, and lack of understanding when to refer, and a lack of SLT presence on ICU. Referrals came from a wide range of professions with nursing as the most common referral source (n = 54/64; 84%) followed by physiotherapy (n = 34/64; 53%).
3.5Multi-disciplinary team integration
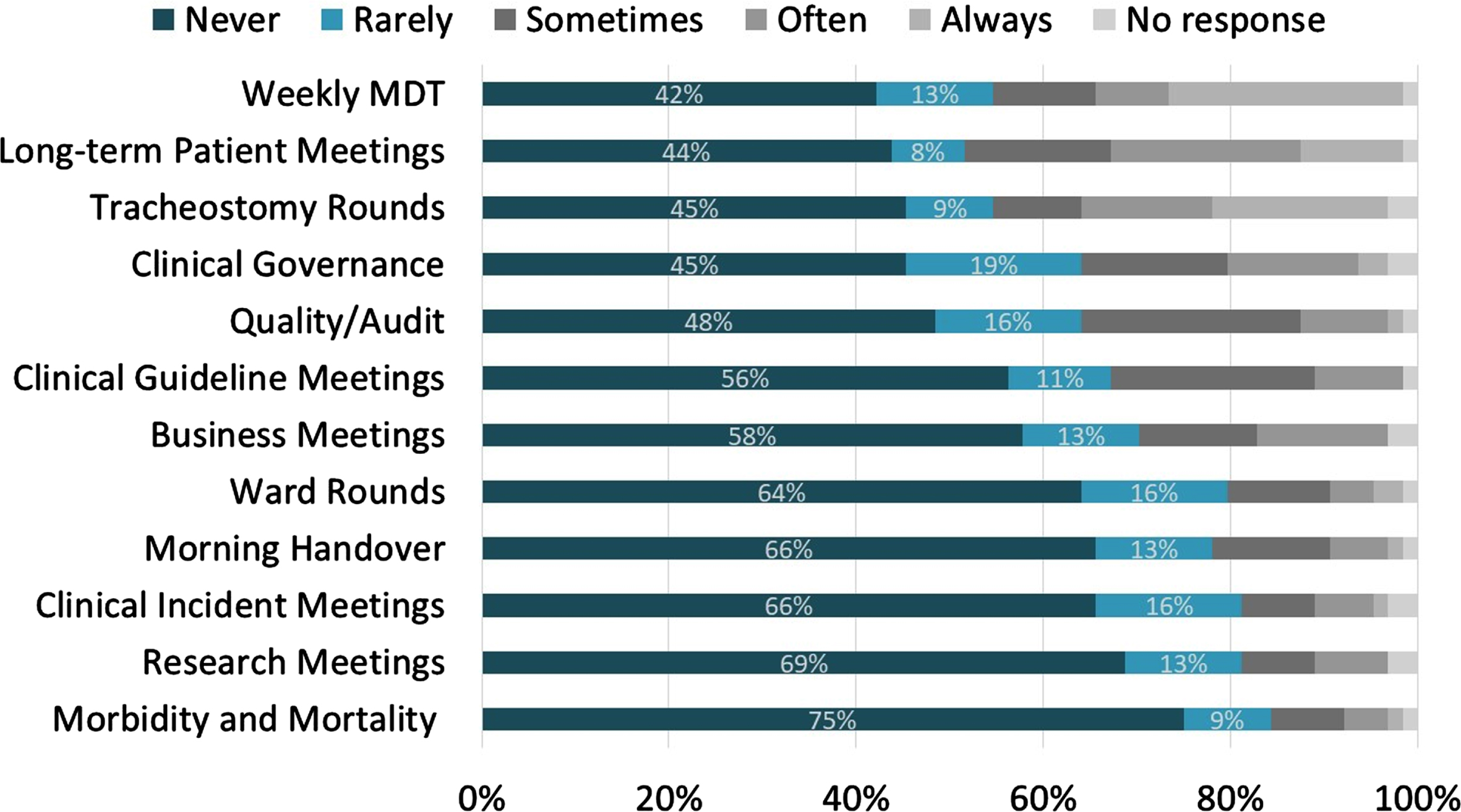
Respondents reported limited attendance at MDT meetings, with weekly MDT meetings the most frequently attended (n = 16/64, 25% ‘always’) and 75% (n = 48/65) of respondents reported never having capacity to attend morbidity and mortality meetings (shown in Fig. 3). Whilst 88% (n = 56/64) of sites reported involvement in teaching and training staff, 63% (n = 35/56) also reported this occurred only a few times a year.
Fig. 3
SLT attendance at intensive care unit meetings.
3.6Audit and research
Thirty-three percent (n = 21/64) reported involvement in ICU-related audit or research, including: audit (n = 12/21, 57%), service evaluation (n = 3/21, 14%), Global Tracheostomy Collaborative data collection (n = 3/21, 14%) and clinical research (n = 2/21, 11%).
3.7Good practice sub-analysis
Sub-analysis of three adult services with the highest staffing levels revealed that all were able to provide a daily service, five days per week. Two services were able to meet the GPICS guidance for all tracheostomised patients to be seen, two services were 100% funded by ICU and the third service received partial funding from ICU (1–25%). All services reported that referrals were timely and appropriate, and patients were seen within one working day of referral by one service, and within 4–15 hours for the two other services. All services were often involved in PMV assessment, and all services were involved in AAC identification. Two services were conducting research, and all were providing teaching for the MDT. However, one service had wait times of 5 days for FEES and MDT training only occurred a few times per year. Two services reported that their staffing had improved in the past 2 years, due to additional funding for extra beds and service re-configuration.
4Discussion
This is the first UK survey detailing ICU SLT workforce and service provision. Findings indicated insufficient SLT staffing to provide a consistent and responsive expert service to meet ICU patients’ needs or achieve UK national guidance.
4.1Staffing
Average SLT staffing in ICUs was very low and slightly greater for paediatric and neonatal services, although the sample size for this group was very low (n = 3). Staffing tended to be Band 6 and 7 with fewer than a third of services having staff at band 8a (Clinical Specialist or Clinical Lead) or 8b (Consultant) level. This lack of ring-fenced funding may have contributed to low SLT staffing provision across the UK and many services providing a non-specialist service from their generic SLT hospital cover. In the National Health Service there is an expectation that an equitable service be provided to all patients, which may lead to diluting of staffing across service areas and to the use of generic and non-ICU specialist staff, as observed in these results.
There are a number of UK SLT competencies to support development of ICU-specific skills such as: the RCSLT Tracheostomy competencies (RCSLT, 2014), the Intensive Care Society (ICS) Allied Health Professionals Critical Care Professional Development Framework ( Allied Health Professionals: Critical Care Professional Development Framework, 2018), the ICS SLT Pillar ( The Speech and Language Therapy Pillar: A Supplementary Resource of the Allied Health Professionals (AHP) Critical Care Professional Development Framework (CCPDF), 2021). However, completing these competencies requires access to appropriately trained supervisors, which can be problematic, and may contribute to the reliance on non-specialist SLT staff providing services to ICUs in the UK.
The findings of limited SLT staffing are consistent with other international data. Cardinal et al. found that 71% of participants reported that they provided a service to ICU of≤10 hours per week and dedicated funding was available in 23% of services (Cardinal et al., 2020). The UK critical care workforce survey reported that SLT were the least funded of all professional groups, at 23% (Twose et al., 2022). This study reported SLT staffing ratios of 1 WTE per 30 ICU beds in services with ring-fenced funding, and 1 WTE per 158 ICU beds in services without dedicated funding (Twose et al., 2022). The UK data (sample size = 52 ICUs) from the Dysphagia in Intensive Care Evaluation (DICE) study, conducted between November 2017 and June 2019, reported similar findings with 98% of services having SLT provision to ICU, but just 13% of this provision was dedicated solely to ICU (Spronk et al., 2022). However, the DICE study also presents Australian data where 100% of ICUs (n = 12/12) had SLT provision, with 92% (n = 11/12) of this dedicated to ICU (Spronk et al., 2022). This presents a very different picture to the focused Australian study with a larger sample size of 165 sites (Cardinal et al., 2020). An international survey of SLTs found that 10% were working exclusively in ICU (Rowland et al., 2022). It also suggests that UK provision is much better than many countries in Europe where a high proportion of services had no SLT provision: Greece (n = 36/36, 100%), Turkey (n = 36/39, 92%), Slovakia (n = 16/19, 84%), Spain (n = 24/36, 67%), Italy (n = 29/46, 63%), Norway (n = 14/31, 45%) (Spronk et al., 2022). However, staffing levels in the UK were not improving at the same rate as other countries, with international reports of 35% improvement in the previous 3 years compared with 20% found in this study (Rowland et al., 2022). This situation seems to have reversed more recently, potentially as a result of the COVID-19 pandemic, and increasing awareness of the value of SLT in ICU (Mills et al., Manuscript submitted for publication). The sub-analysis of the three services with the highest staffing levels shows they were able to provide a better service in various areas and highlights the importance of continuing to work towards improving SLT staffing in ICU. The secondary aim of this study was to provide evidence to support decision-making regarding recommended SLT staffing ratios for ICU. Participants were asked to estimate what staffing they required to provide an adequate 5-day service. However, these were not uniformly described, perhaps due to the wording of the question and free text responses, and could not be reported. However, after thorough analysis of the complete dataset the RCSLT Tracheostomy CEN’s committee agreed on a recommendation of 0.1 WTE SLT per ICU bed, which was incorporated into Edition 2 of GPICS (GPICS, 2019).
4.2Clinical service provision
Most respondents stated that their service provision for communication, swallowing and tracheostomy weaning was inadequate. There was considerable variety in referral response times, although most services reported that patients were seen within two working days. Less than a third of respondents reported that all patients with a tracheostomy were assessed by SLT for both communication and swallowing. Similarly, 30% of international respondents reported that all patients with a tracheostomy are seen by SLT (Rowland et al., 2022). The DICE study reported that dysphagia assessment was completed for tracheostomised patients > 50% of the time (Spronk et al., 2022).
More than half of respondents were able to access FEES, and wait times were 1–3 days for the majority of these services. UK access to FEES appears to be much better than in some other countries, with Australian SLTs reporting 36% of services able to access FEES (Cardinal et al., 2020). Thirty-nine percent of Irish SLTs were able to access FEES, and 60% of other international services were able to access FEES, though this was not always SLT-led (Rowland et al., 2022). The DICE international study reported that more than 30% of services did not have access to FEES or were not familiar with it (Spronk et al., 2022). Reliable and regular access to FEES is important for tracheostomy weaning, decannulation, and patients’ early safe return to oral intake (Hafner et al., 2008; Hales et al., 2008; McGowan et al., 2007; Wallace & McGrath, 2021).
Most SLTs had limited input into tracheostomy weaning, PMV trials, and the identification of AAC. Comparatively, 55% of international SLTs reported involvement in PMV trials and 35% reported that all non-speaking patients were referred to SLT (Rowland et al., 2022). Inconsistency of communication input for tracheostomised patients means patients are more likely to be voiceless for longer, leading to higher levels of psychological distress (Happ, 2000). Irregularity of involvement with PMV trials may mean missed identification of vocal fold dysfunction or other functional impairments in the upper airway (McRae et al., 2019). Likewise, the provision of daily rehabilitation was rare, with poor compliance of the GPICS recommendation for rehabilitation, and this may delay restoration of communication and swallowing function and contribute to lower patient quality-of-life. This recommendation has since been removed in the updated guidelines due to lack of supporting evidence, which highlights the need for further research to establish the rehabilitation needs of ICU patients (GPICS, 2019).
4.3Referrals
Under-referral and untimely referrals were a problem in most services. These issues were also identified in the National Confidential Enquiry into Patient Outcome and Death report conducted in 2013 (NCEPOD, 2014). Untimely referrals appear to be more of a problem in the UK than internationally, where 36% reported an issue (Rowland et al., 2022). Increasing the SLT presence on ICU could help to improve MDT education regarding the SLT role and the nature of ICU-related dysphagia and communication impairment, and identification of problems and consequently improve referrals.
4.4Multi-disciplinary team integration
There was a lack of integration within ICU MDTs, with most respondents unable to attend unit meetings. This appears to be worse in the UK than in Australia where 32% had no involvement (Cardinal et al., 2020). Frequency of attendance at MDT meetings is considerably lower for SLTs than for physiotherapists or dietitians (Twose et al., 2022). Most respondents were able to provide teaching and training on their ICUs, but this was limited in most cases to a few times per year. These figures are similar to that seen in Australia where 90% of respondents were able to provide training to nursing staff (Cardinal et al., 2020). Improving SLT integration within the MDT and participation in unit activities would improve awareness of communication and swallowing impairment.
4.5Audit and research
A third of respondents were involved in ICU-related audit and research, and this is likely due to the limited staffing available in most centres. Research has demonstrated that there is an association between the level of clinician-engagement in research and improved patient outcomes and care processes (Boaz et al., 2015). Additionally, patients that are admitted to hospitals with higher levels of research activity have greater confidence in staff, receive better quality information about their care, and have a better inpatient experience (Jonker et al., 2020). Improving SLT staffing to allow increased participation in collaborative research in ICU has the potential to have substantial positive effects for services and patients.
4.6Implications for clinicians, service providers, and researchers
A lack of direct funding for dedicated ICU SLTs often results in inexperienced SLTs from other clinical areas providing input into ICU. This poses a risk for the quality and safety of the service provided, and working relations with other MDT members (Cardinal et al., 2020; McGrath et al., 2020). It can also lead to reduced service provision in other areas of the hospital. Insufficient staffing, in terms of expertise and numbers of SLTs, is likely to contribute to a lower standard of service provision and worse patient outcomes. Research supports positive patient outcomes and financial benefits of having an integrated, experienced SLT service in ICU (McGrath et al., 2020; McGrath & Wallace, 2014). However, with increasing financial pressures within the UK National Health Service, more evidence is needed to support the cost-effectiveness of SLT services in ICU. On the basis of our findings, specific areas for focus include: the impact of increased SLT staffing (e.g. MDT knowledge and awareness of the SLT role and dysphagia and communication impairment; patient outcomes, including early restoration of voice and oral intake; and patient quality-of-life), the impact of improved patient access to communication, the impact of improved access to FEES (including the impact on tracheostomy weaning), and the impact of early and daily rehabilitation. Local and national service evaluation, quality improvement projects, as well as larger scale research would all help to improve evidence base in these areas. Improving the evidence base will help to: ensure that cost-effective interventions are implemented, provide more support for increased funding for SLT staffing, and ensure that patients receive an optimal service.
4.7Strengths and limitations
There was high survey completion rate (100%), with no drop out, implying that the survey was an appropriate length. Both participation rate (11%) and response rate (35%) were relatively low. A low participation rate is to be expected with online surveys, as it includes all visits to the initial page of the website in the denominator. It is typical for many individuals to click on the survey link to find out more information. The numbers visiting the initial page may have been further increased by individuals clicking on the survey link from a mobile device but choosing to complete the survey later on a computer, as well as multiple individuals from the same team viewing the survey. The relatively low response rate may be due to the dissemination approach via SLT professional networks and social media. Units whose SLT staff were not part of these networks may have been unaware of the survey. This may particularly have been the case for the lack of respondents from Scotland and Northern Ireland, where there is currently no representation from these countries on the committee and minimal representation in the membership. Additionally, units with no SLT service may not have been aware of the survey. Moreover, the results may be biased towards units with better SLT provision, therefore, and the reported findings may provide an overly optimistic picture of service provision. This is supported by the recent UK AHP workforce survey which reported much lower staff to bed ratios in the 77% of services without dedicated funding (Twose et al., 2022). Unfortunately, estimated requirements for an adequate 5-day service were not uniformly reported, perhaps due to the wording of the question and free text responses. In future surveys, these limitations could be mitigated through more extensive piloting of the survey and distribution via the Intensive Care Society and individualICUs.
5Conclusions
This study highlights a number of areas for improvement for SLT service provision in UK ICUs. Prior to this survey, there were no recommended SLT staffing ratios for ICU. Few hospitals meet the new recommended SLT staffing ratios, developed from these data, and many fall significantly below these. Improving SLT service provision to critically ill patients will involve a number of challenges including: training and upskilling ICU specialist SLTs, funding a larger ICU SLT workforce, improving access to specialist equipment, and increasing MDT awareness of the specific roles and benefits of SLT input to improving patient outcomes and quality-of-life. In a climate of financial pressures, this will require ongoing innovative thinking, collaboration and support from a range of stakeholders (e.g. the Intensive Care Society and the Faculty of Intensive Care Medicine) to explore all options. Future research should focus on further demonstrating the benefits of SLT interventions, promoting optimised recovery of ICU patients, and the potential for cost savings. It would be beneficial to monitor progress and improvements to SLT service provision in UK ICUs working collaboratively with the MDT to address future challenges.
Acknowledgments
The authors are grateful to all the members of the RCSLT Tracheostomy Clinical Excellence Network for taking the time to complete this survey. We thank Emma Cowpe for her assistance with data analysis and Charlie McDonald and Sue McGowan for their contribution to the concept development and survey design. We are also grateful for the input of Rebecca O’Mahoney, Vicky Thorpe, and Erin Probert. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors have no conflicts of interest to declare.
Supplementary material
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/ACS-2200115.
References
1 | Allied Health Professionals: Critical Care Professional Development Framework. (2018). Intensive Care Society. https://www.ics.ac.uk/Society/Guidance/PDFs/AHP_Framework. |
2 | Boaz, A. , Hanney, S. , Jones, T. , Soper, B. ((2015) ). Does the engagement of clinicians and organisations in research improve healthcare performance: A three-stage review, BMJ Open, 5: (12), 009415. https://doi.org/10.1136/bmjopen-2015-009415. |
3 | Brodsky, M. B. , Levy, M. J. , Jedlanek, E. , Pandian, V. , Blackford, B. , Price, C. , Cole, G. , Hillel, A. T. , Best, S. R. , Akst, L. M. ((2018) ). Laryngeal injury and upper airway symptoms after oral endotracheal intubation with mechanical ventilation during critical care: A systematic review, Critical Care Medicine 46: (12), 2010–2017. https://doi.org/10.1097/CCM.0000000000003368. |
4 | Cardinal, L. A. , Freeman-Sanderson, A. , Togher, L. ((2020) ).The speech pathology workforce in intensive care units: Results from a national survey, Australian Critical Care 33: (3), 250–258.https://doi.org/10.1016/j.aucc.2020.02.003 . |
5 | Dillman, D. A. (1999). Mail and Internet Surveys: The Tailored Design Method (2nd Revised edition). John Wiley & Sons. |
6 | Eysenbach, G. ((2004) ).Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES), Journal of Medical Internet Research 6: (3), e34. https://doi.org/10.2196/jmir.6.3.e34. |
7 | Freeman-Sanderson, A. L. , Togher, L. , Elkins, M. R. , Phipps, P. R. ((2016) ).Return of Voice for Ventilated Tracheostomy Patients in ICU: A Randomized Controlled Trial of Early-Targeted Intervention, Critical Care Medicine 44: (6), 1075–1081. https://doi.org/10.1097/CCM.0000000000001610. |
8 | GPICS. (2015). Guidelines for Provision of Intensive Care Ser- vices. The Faculty of Intensive Care Medicine and the Intensive Care Society, Edition 1. |
9 | GPICS. (2019). Guidelines for the Provision of Intensive Care Services. The Faculty of Intensive Care Medicine and the Intensive Care Society, Edition 2. |
10 | Hafner, G. , Neuhuber, A. , Hirtenfelder, S. , Schmedler, B. , Eckel, H. E. ((2008) ).Fiberoptic endoscopic evaluation of swallowing in intensive care unit patients, European Archives of Oto-Rhino-Laryngology 265: (4), 441–446. https://doi.org/10.1007/s00405-007-0507-6. |
11 | Hales, P. A. , Drinnan, M. J. , Wilson, J. A. ((2008) ).The added value of fibreoptic endoscopic evaluation of swallowing in tracheostomy weaning, Clinical Otolaryngology 33: (4), 319–324. https://doi.org/10.1111/j.1749-4486.2008.01757.x. |
12 | Happ, M. B. ((2000) ).Interpretation of nonvocal behavior and the meaning of voicelessness in critical care, Social Science and Medicine 50: (9), 1247–1255. https://doi.org/10.1016/S0277-9536(99)00367-6. |
13 | Health and Social Care Online. (n.d.). HSC Structure — HSCNI Online. Retrieved January 12, 2021, from https://online.hscni.net/home/hsc-structure/. |
14 | Jonker, L. , Fisher, S. J. , Dagnan, D. ((2020) ).Patients admitted to more research-active hospitals have more confidence in staff and are better informed about their condition and medication: Results from a retrospective cross-sectional study, Journal of Evaluation in Clinical Practice 26: (1), 203–208. https://doi.org/10.1111/jep.13118. |
15 | McGowan, S. L. , Gleeson, M. , Smith, M. , Hirsch, N. , Shuldham, C. M. ((2007) ).A pilot study of fibreoptic endoscopic evaluation of swallowing in patients with cuffed tracheostomies in neurological intensive care, Neurocritical Care 6: (2), 90–93. https://doi.org/10.1007/s12028-007-0024-x. |
16 | McGrath, B. A. , Wallace, S. ((2014) ).The UK National Tracheostomy Safety Project and the role of speech and language therapists, Current Opinion in Otolaryngology and Head and Neck Surgery 22: (3), 181–187. https://doi.org/10.1097/MOO.0000000000000046. |
17 | McGrath, B. A. , Wallace, S. , Lynch, J. , Bonvento, B. , Coe, B. , Owen, A. , Firn, M. , Brenner, M. J. , Edwards, E. , Finch, T. L. , Cameron, T. , Narula, A. , Roberson, D. W. Improving tracheostomy care in the United Kingdom: Results of a guided quality improvement programme in diverse hospitals, December ((2020) )1–11. https://doi.org/10.1016/j.bja.2020.04.064. |
18 | McIntyre, M. , Doeltgen, S. , Dalton, N. , Koppa, M. , Chimunda, T. (2020). Post-extubation dysphagia incidence in critically ill patients: A systematic review and meta-analysis. Australian Critical Care. https://doi.org/10.1016/j.aucc.2020.05.008. |
19 | McRae, J. , Montgomery, E. , Garstang, Z. , Cleary, E. ((2019) ).The role of speech and language therapists in the intensive care unit, Journal of the Intensive Care Society 21: (4), 344–348. https://doi.org/10.1177/1751143719875687. |
20 | Mills, C. S. , Jones, G. , Wallace, S. , (Manuscript submitted for publication). The COVID-19 silver lining for speech and language therapists. |
21 | National Institute for Health and 722 Clinical Excellence (NICE). (2009) . Rehabilitation after critical illness, London National Institute for Health and Clinical Excellence. |
22 | NCEPOD. (2014). On the Right Trach? A review of the care received by patients who underwent a tracheostomy. |
23 | NHS Improvement. (2019). Consolidated NHS provider accounts 2018/19:1 April 2018—31 March 2019. |
24 | NHS Inform. (n.d.). National Contact Point: Health boards. |
25 | NHS Wales. (2006). NHS Wales: Structure. |
26 | RCSLT. (2014). RCSLT Tracheostomy Competency Framework (Issue January). |
27 | Rowland, S. , Mills, C. , Walshe, M. ((2022) ).Perspectives on speech and language pathology practices and service provision in adult critical care settings in Ireland and international settings: A cross-sectional survey, International Journal of Speech-Language Pathology 0: (0), 1–12. https://doi.org/10.1080/17549507.2022.2032346. |
28 | Royal College of Speech & Language Therapists. (2014). Position Paper: Speech and Language Therapy in Adult Critical Care. |
29 | Skoretz, S. A. , Flowers, H. L. , Martino, R. ((2010) ).The Incidence of Dysphagia Following Endotracheal Intubation: A Systematic Review, Chest137: (3), 665–673. https://doi.org/10.1378/chest.09-1823. |
30 | Spronk, P. E. , Spronk, L. E. J. , Egerod, I. , McGaughey, J. , McRae, J. , Rose, L. , Brodsky, M. B. , Brodsky, M. B. , Rose, L. , Lut, J. , Clavé, P. , Nanchal, R. , Inamoto, Y. , van der Hoeven, J. I. , Spronk, P. E. , Freeman-Sanderson, A. , Hiesmayr, M. , Veraar, C. , Hickmann, C. E. ,the DICE study investigators. (2022). Dysphagia in Intensive Care Evaluation (DICE): An International Cross-Sectional Survey. Dysphagia. https://doi.org/10.1007/s00455-021-10389-y. |
31 | The Speech and Language Therapy Pillar: A supplementary resource of the Allied Health Professionals (AHP) Critical Care Professional Development Framework (CCPDF). (2021). Intensive Care Society. https://www.ics.ac.uk/Society/Guidance/PDFs/SLT_Pillar. |
32 | Twose, P. , Terblanche, E. , Jones, U. , Bruce, J. , Firshman, P. , Highfield, J. , Jones, G. , Merriweather, J. , Newey, V. , Newman, H. , Rock, C. , Wallace, S. (2022). Therapy professionals in critical care: A UK wide workforce survey. Journal of the Intensive Care Society, 17511437221100332. https://doi.org/10.1177/17511437221100332. |
33 | Wallace, S. , McGowan, S. , Sutt, A.-L. (2022). Benefits and options for voice restoration in mechanically ventilated intensive care unit patients with a tracheostomy. Journal of the Intensive Care Society, 17511437221113162. https://doi.org/10.1177/17511437221113162. |
34 | Wallace, S. , McGrath, B. A. Laryngeal complications after tracheal intubation and tracheostomy, BJA Education ((2021) ) 21: (7), 250–257. |
35 | Zaga, C. J. , Berney, S. , Vogel, A. P. ((2019) ).The feasibility, utility, and safety of communication interventions with mechanically ventilated intensive care unit patients: A systematic review, American Journal of Speech-Language Pathology 28: (3), 1335–1355. https://doi.org/10.1044/2019_AJSLP-19-0001. |


