
Recovery in the context of post-stroke aphasia: A concept analysis
Abstract
BACKGROUND:
The term ‘recovery’ frequents the literature relating to aphasia, however there has been limited research directly investigating the concept (or meaning) the term represents.
OBJECTIVE:
To present a concept analysis of ‘recovery’ in the context of post-stroke aphasia and investigate the consistency in meaning, use and interpretation of the concept, in relation the International Classification of Functioning, Disability and Health (ICF) and the Life Participation Approach to Aphasia (LPAA).
METHODS:
Rodgers’ evolutionary method of concept analysis was used to analyse the studies retrieved through a systematic search of PubMed and CINAHL bibliographic databases and a journal search of Aphasiology. The International Classification of Functioning, Disability and Health (ICF) and the Life Participation Approach to Aphasia (LPAA) were used as frameworks to explore the correspondence of the concept of ‘recovery’ with current speech and language therapy service delivery approaches.
RESULTS:
Seventy-one papers were retrieved and analysis revealed six core attributes of the concept; recovery as (1) a process (2) variable dependant (3) existing on a spectrum (4) facilitated (5) quantifiable (6) subject to deceleration. The concept of recovery was found to be impairment-oriented, demonstrating a poor overall correspondence with current frameworks underpinning service delivery.
CONCLUSIONS:
Facilitating recovery in the context of post-stroke aphasia is a widely discussed therapeutic priority, yet the concept of recovery itself remains ambiguous. Clarification of the current conceptual status of recovery is necessary to ensure consistency in meaning, use and interpretation of the concept, in recognition of its potential implications on research and service delivery.
1Introduction
The term ‘recovery’ frequents the literature relating to aphasia rehabilitation, across disciplines and contexts. There has been limited research published on how clinicians frame the concept of recovery in clinical practice, however recent discussions identified in grey literature (Worrall, 2020) suggest that a typical activity in speech and language therapy practice is to facilitate the explanation of recovery through drawing a ‘recovery curve’. This is a graph that depicts the recovery process as the relationship between time on the X-axis and improvement (typically in impairment) on the Y-axis. Clinicians have described variations in the way they illustrate the ‘recovery curve’, reporting variations in slope steadiness, linearity, and timespan, but overall depicting an uphill curve followed by a plateau in improvement (Worrall, 2020). Despite a strong universal theme in the literature there is a vague conceptualisation of recovery in the context of post-stroke aphasia, appearing to be restricted by criteria laid out on a case-by-case basis and applied to the context in which it is being used.
Why does a vague conceptualisation of recovery matter, and what difference would it make to the field of aphasiology if this central concept was more robustly interrogated? The absence of conceptual clarity makes it challenging to synthesise findings from different studies, approaches, and models and risks misunderstanding between clinicians and clients when talking about prognosis. The re-conceptualisation of recovery in mental health services, undertaken in the last two decades, provides a clear example of the positive impact of conceptual clarity. Since the early 2000 s recovery in the context of mental health disorders has evolved to from implying a “cure” or a “return to normal”, to being defined as “a nonlinear process of self-organization and adaptation that offsets the personal disintegration of mental illness and enables the individual to reconceive his or her sense of self and well-being on all biopsychosocial levels” (ibid, p.654). Ultimately the articulation of the meaning of recovery led to a shift in delivery of services to people with MHD’s, with recovery-oriented services considered the gold-standard. The lessons learned from the field of mental health shows that ‘unpacking’ the concepts in taken-for-granted terms such as recovery can lead to advancements in service delivery. In addition, conceptual clarity between clinicians and people with aphasia should allow for more nuanced discussions around prognosis (what kind of ‘recovery’ do we mean with the recovery curve; how, in the context of persistent symptoms, is recovery possible) and reinforce join-ownership of the therapeutic process and its outcomes.
Therefore, this paper seeks to address the following research questions: 1) How is the concept of ‘recovery’ understood in aphasia literature from a concept analysis perspective? 2) Does the conceptual consensus correspond with current philosophies and frameworks of service delivery when working with PWA, from a Speech and Language Therapy perspective.
2Materials and methods
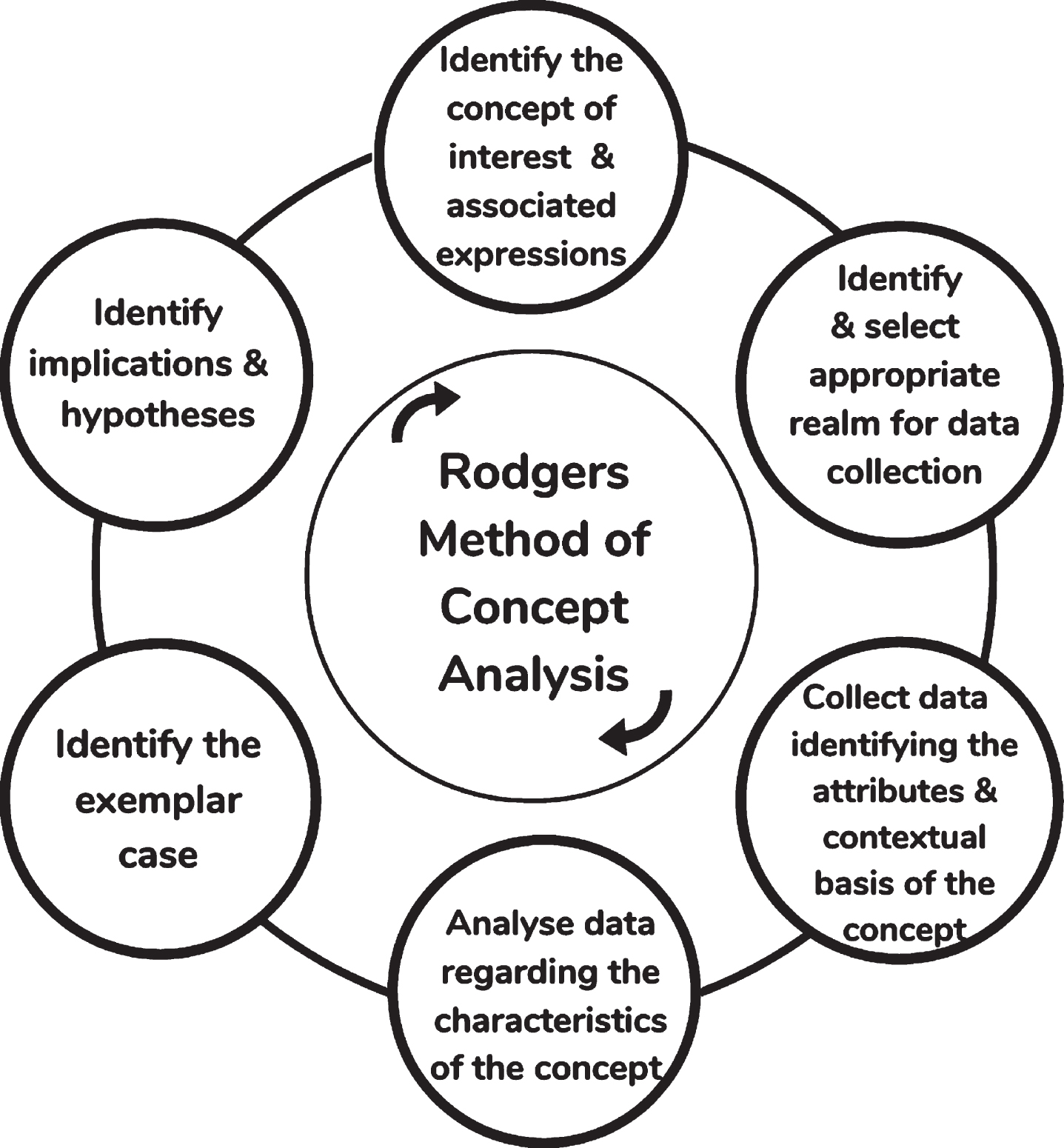
Concept analyses are a group of approaches used to investigate complex or ambiguous concepts, allowing for the establishment of a conceptual consensus at a point in time, and identifying possible areas for growth and development. Rodgers evolutionary method of concept analysis (Rodgers & Knafl, 2000), used in this study, proposes that a concept is a mental construct behind a word that alters across time and contexts. The method is composed of six primary activities, illustrated in Fig. 1, and the analysis occurs in a cyclical as opposed to a linear manner (Rodgers and Knafl, 2000).
Fig. 1
The cyclical process of a Rodgerian concept analysis.
A systematic search strategy was implemented to identify appropriate literature in which to conduct data collection, rather than following Rodger’s traditional approach of probability sampling from the identified indexed literature. The systematic search was confined to two bibliographic databases (PubMed and CINAHL) which index the journals most highly cited in relation to stroke and aphasia. This approach allowed us to capture the research which appears most widely read and therefore influential in shaping the concept of recovery in aphasia. Additionally, early online articles from the journal Aphasiology were searched for relevant studies. Papers published in English, between the years 2010 through 2020 inclusive were eligible for inclusion. The time period was selected in order to support the extraction of data relevant to the current status of the concept of recovery, while accounting for the influential introduction of the ‘Life Participation Approach to Aphasia’ (LPAA) (Chapey et al., 2000), discussed below. A sample search strategy is available in Supplementary File 1.
Data was extracted from each paper using three frameworks, independent of one another, the first being the traditional features of concept analysis (i.e., attributes, antecedents, consequences, and references). The second framework, ‘The International Classification of Functioning, Disability and Health’ (ICF) (WHO, 2001) was applied deductively using the ICF checklist version 2.1A, due to its standing as a globally recognised framework, which accounts for disability as an interaction between the impairment and barriers in the environment resulting to the functional limitations and participation restrictions. The third and final framework applied was that of the five articulated values of the LPAA1 (Chapey et al., 2000). The LPAA is a person-centred philosophy of service delivery for PWA, widely considered to be a favourable approach within the Speech & Language Therapy discipline that highlights the importance of supporting PWA to actively collaborate in their recovery process. Its application allowed the data extraction process to account for the literature’s representation of these factors. A second researcher reviewed a randomised 10% of papers at this point using the data extraction protocol, to monitor for bias at this stage of the study.
Data was extracted and managed in Microsoft Excel 2016, through use of an extraction protocol designed to elicit data relevant to the concept’s attributes, contextual basis, and parallels with selected philosophies/frameworks. Each paper was read in full prior to extracting any data and was then classified according to the tone of the study (impairment focus / psychosocial / combination). The contextual factors included in the extraction protocol for this analysis were: disciplinary features (e.g., speech and language therapy, neurology, nursing), antecedents, consequences, and surrogate terms as they have the capacity to elucidate answers to the first research question posed (see Table 1 for an explanation of terms). Identification of the attributes of a concept is a core component of concept analysis, with these attributes collectively constituting the ‘real’ definition of a concept (Rodgers and Knafl, 2000).
Table 1
Terminology in Rodger’s approach to concept analysis
| Term | Explanation |
| Tone | The underlying attitudes and/or message of a paper, inferred by authors through selection of terms and phrases used. |
| Concept | A concept encompasses ideas, dimensions or a series of attributes that are expressed through use of a term. Therefore, words are used to express concepts, but they are not concepts themselves e.g., the term grief is associated with sadness, loss etc. The concept referred to through this paper is ‘the concept of recovery in post-stroke aphasia’ |
| Surrogate Terms | A concept can be represented by more than one term i.e., multiple terms are used interchangeably to express a singular concept. In this case, the terms used are called surrogate terms. |
| Related Concepts | Occasionally, a term can represent more than one concept. These concepts tend to be closely related but can be differentiated by core attributes. These are referred to as related concepts. |
| Attributes | Attributes are the core, defining characteristics of a concept. Identification of a concepts attributes is the primary goal of concept analysis. |
| Antecedents | Antecedents are events/situations that precede a concept. |
| Consequences | Consequences are events/situations that occur as a result of the concept. |
As advised in Rodger’s approach (2000) analysis of the concept was delayed until the data extraction process was complete. The data extracted was analysed as two separate sets of data; the first relating to traditional features of concept analysis (i.e. attributes, antecedents, consequences, and references), the second relating to the additional data extracted for the purposes of this analysis (i.e., ICF codes and LPAA values). The first analysis of the data was conducted according to traditional thematic analysis procedures, using a combination of a deductive approach guided by the framework of concept analysis and an inductive processes to identify the specific themes related to attributes, antecedents etc. The results of the two data sets were then merged to deductively evaluate how the conceptual consensus corresponded with the ICF and LPAA. Following this, the data was segregated across disciplines to be examined for inter-disciplinary similarities/differences. All included articles and their references were then evaluated for the presence of an exemplar case, as Rodger’s method disallows the independent construction of one. In this approach, the exemplar of a concept serves to further consolidate conceptual clarity, through its application to a practical context.
3Results
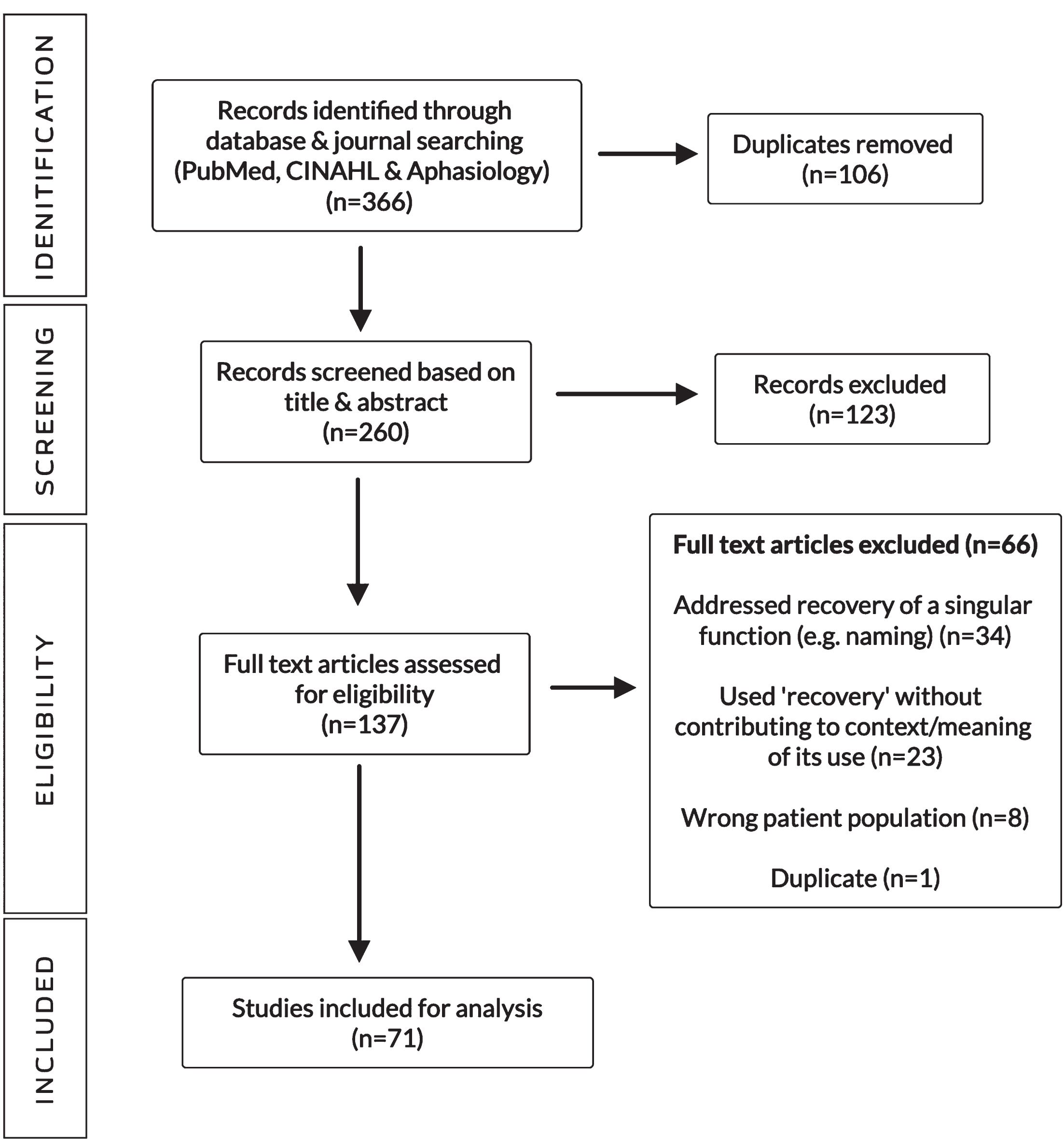
A total of 366 papers were retrieved: 133 from PubMed, 210 from CINAHL and 23 from the journal Aphasiology. Covidence identified 106 duplicates, leaving 260 articles for review. After exclusion based on the title, abstract, and full-text review (Fig. 2), 71 papers were included in this analysis (Supplementary File 2). No extraction discrepancies were identified in the second researcher’s review of the data extraction phase.
Fig. 2
PRISMA flowchart.
3.1Associated expressions: Tone, definitions, surrogate terms, and related concepts
When analysed regarding overall tone, 59 of the included papers demonstrated an impairment focus, 4 on psychosocial considerations, and the tone of 8 papers alluded to both factors. A limited number of explicit definitions of the concept were identified, a finding which is typical in concept analysis. Recovery was instead discussed in reference to measurements of symptom improvement. Any attempted definitions were constructed on an operational basis specific to the study, for example, “...recovery from aphasia was defined as a score of 1 at baseline (Day 0) followed by a score of 0 on the appropriate NIHSS domain at three-months” (Ali, Lyden & Brady, 2015, p.401). Several surrogate terms were identified, namely ‘language recovery’, ‘speech recovery’ and ‘functional recovery’. The surrogate ‘language recovery’ was decidedly the most prevalent term observed, present in 67.6% of papers analysed. Not only were these terms used interchangeably but so too were the concepts they represented. This finding was supported by evidence of subtle differences in use of terms throughout a paper, monitoring for repeated extension of term to concept through use of the context provided. For example;
. . . we found no significant difference in language recovery between poststroke aphasia patients carrying a Met allele compared to noncarriers. Therefore, the present results suggest that the BDNF polymorphism does not significantly influence aphasia recovery through SLT after stroke. (de Boer et al., 2017, p.856, emphasis added)
3.2Attributes of ‘recovery’
Through use of an inductive analytical approach, 6 core attributes were identified: (1) recovery as a process, (2) recovery as variable dependant, (3) recovery’s existence on a spectrum, (4) recovery as facilitated, (5) recovery as quantifiable and (6) recovery as being subject to deceleration. Each attribute is discussed in more detail below and presented in Table 2 listed in descending order of frequency of occurrence.
Table 2
Core attributes of the concept of recovery in post-stroke aphasia
| Core attributes | Number of | % |
| of recovery | studies | |
| Process | 64 | 90.1% |
| Variable Dependant | 60 | 84.5% |
| Facilitated | 60 | 84.5% |
| Existence on a Spectrum | 59 | 83.1% |
| Quantifiable | 34 | 47.9% |
| Deceleration | 16 | 22.5% |
The attribute process identifies that the concept of recovery in the context of aphasia is an interactive, long-term entity as opposed to an endpoint. Dynamicity proved intrinsic to this attribute, with studies describing the process as unpredictable and non-linear (Berthier et al., 2011). Across disciplines, frequent reference was made to the advancement of recovery through phases/stages (Furlanis et al., 2018; Meier, Johnson, Pan and Kiran, 2019; Stefaniak, Halai and Lambon Ralph, 2020). Considerable obscurity was noted across the data sample regarding the timeframe attributed to the process. Each study presenting this attribute made reference to ‘stages of recovery,’ however within this consensus considerable variance was observed in the periods recognised as the acute, sub-acute and chronic phases. To illustrate the disparity across the data sample, the reported duration of the chronic phase of recovery ranged from 1 year, (Geranmayeh, Brownsett & Wise, 2014) to 25 years (Smania et al., 2010), to lifelong and ongoing (Wortman-Jutt & Edwards, 2017). Despite this, there is a clear recognition of the enduring nature of recovery, and a portrayal of the fluctuating periods inherent in the process.
The attribute variable dependant refers to the diverse range of variables considered to be intrinsic to the phenomenon of recovery, and the extent to which they facilitate or impede the concept’s occurrence. Variables identified pertained to three main themes: personal, neural, and external. The personal variables observed ranged from an individual’s age and gender to their inherent resilience and motivation (Gilbert, Gilbert, Culpepper & Wilkinson, 2013). External variables included familial support and finance (Pringle, Hendry, Mc Lafferty & Drummond, 2010), services, intervention received, and dosage of the intervention (Marangolo & Caltagirone, 2014), whereas neural variables made reference to lesion site/size (Watila & Balarabe, 2015) and residual fibres (McKinnon et al., 2017). Disagreements surrounding the impact and/or relevance of specific variables were widely observed, however, a distinct consensus existed in the portrayal that different variables are an attribute intrinsic to the concept.
The attribute of recovery as facilitated was a frequently identified attribute. This attribute suggests that recovery can be supported by products (e.g. Gilbert, Gilbert, Culpepper, and Wilkinson, 2013), people, whether it be family/friends (Zhou et al., 2018) or healthcare professionals (Fonseca, Raposo and Martins, 2018) and/or services and systems (Watila and Balarabe, 2015). All studies originating from the discipline of speech and language therapy and 82% of the papers from the discipline of neurology, portrayed recovery as facilitated.
Quantifiable was identified as a further core attribute of the concept with studies describing this characteristic further analysed in terms of tools used to quantify recovery (Table 3). Other papers directly stated their measures of recovery, such as van Oers and colleagues (2010) who described that “For each patient, the difference between the subacute and chronic stage Z -scores was calculated as a measure of recovery” (van Oers et al., 2010, p.887) and “aphasia recovery measured as absolute change in global AAT score” (Thiel et al., 2013, p.2241). As the related concepts ‘aphasia recovery’ and ‘language recovery’ have been used interchangeably, this demonstrates that this attribute makes specific reference to “recovery of language function” (Yagata et al., 2016, p.3) and the “absence of limitation of communication” (Glize et al., 2019, p.109). Other studies analysed however directly contraindicate ‘quantifiable’ as an attribute of the concept; “...one never recovers from aphasia; one recovers with aphasia” (Sarno as cited by Wortman-Jutt & Edwards, 2017, p.820). This illustrates the consequences of related concepts being used interchangeably in literature. Interdisciplinary analysis demonstrated that quantifiable as an attribute of recovery was most evident in publications from the discipline of neurology.
Table 3
Most frequently used data collection tools across studies portraying the attribute ‘quantifiable’
| Data Collection Tools | Number of Studies |
| Western Aphasia Battery-Revised (WAB-R), Western Aphasia Battery (WAB), Korean Western Aphasia Battery (KWAB) | 10 |
| Functional Magnetic Resonance Imaging (fMRI) | 7 |
| Boston Naming Test (BNT) | 6 |
| The Token Test (TT) | 6 |
| Aachen Aphasia Test (AAT) | 5 |
| A clinical language test for aphasia (unspecified) | 4 |
| Boston Diagnostic Aphasia Examination (BDAE) | 3 |
| National Institutes of Health Stroke Scale (NIHSS) | 2 |
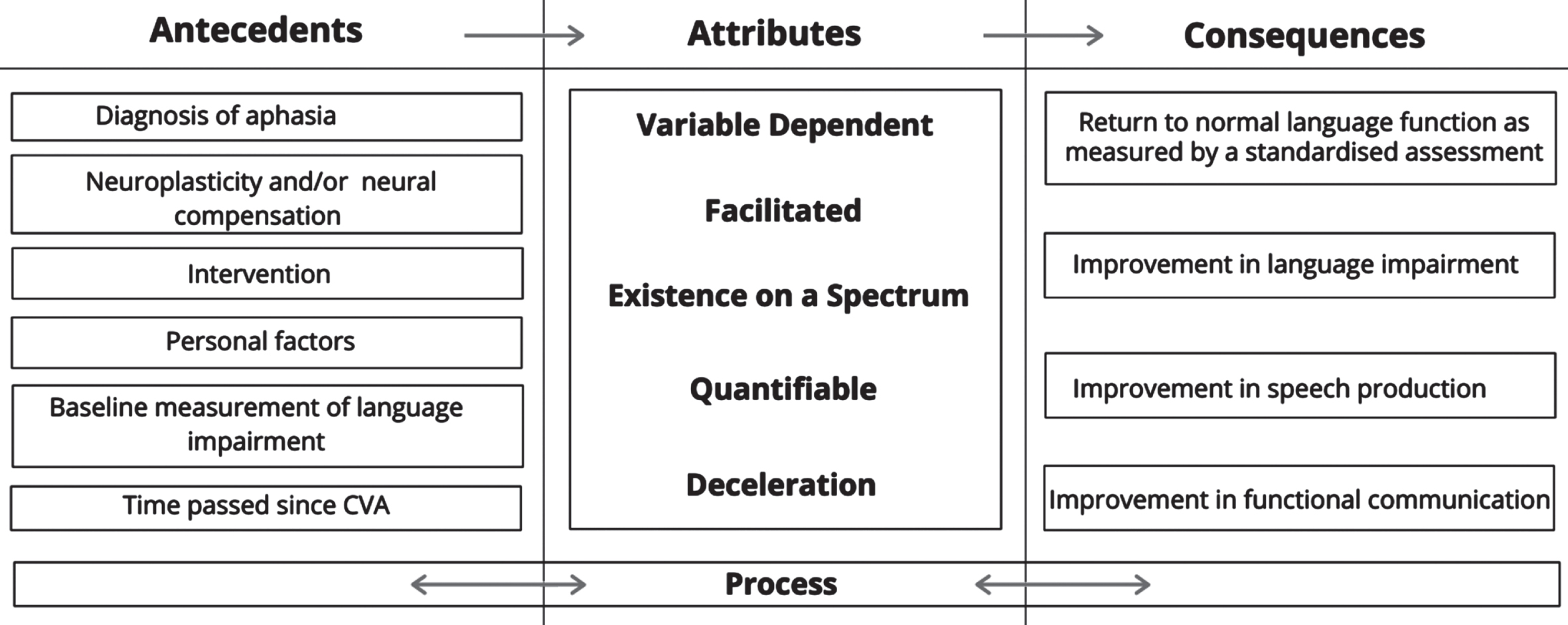
Finally, deceleration is an attribute suggesting a fluctuating timeline as characteristic of recovery. The attribute of deceleration complements the attribute of recovery as a process but corresponds to the related, more specific concept of ‘language recovery’. It is through this understanding of the interchangeable use of related concepts by authors within/across papers that the differentiation between the attributes of ‘process’ and ‘deceleration’ can be clearly defined. The attribute of ‘process,’ as previously discussed, occurs in a large number of papers identifying recovery as a process opposed to an endpoint. This attribute can be applied to either the concept of recovery in the context of language impairment or recovery in the context of aphasia. The attribute ‘deceleration’ however, can only be applied to the concept in the context of improvement of language impairment. Consequently, ‘deceleration’ can occur even in absence of the attribute of ‘process’ and is therefore considered a core attribute. Typically, authors of studies possessing the ‘deceleration’ attribute discussed rapid improvement of language impairment in the initial days/weeks post-stroke, prior to a deceleration in regain of language function; “after the second week it is clear that recovery slows dramatically”, (Wilson et al., 2019, p.727), hence interpreting this as a reduction in recovery rate. Interdisciplinary analysis revealed this characteristic to be recognised across each discipline, however papers from the discipline of neurology accounted for a substantial portion of the attribute’s presence, accounting for 81.3% of papers, as opposed to just 12.5% in the papers from the discipline of speech and language therapy. Figure 3 illustrates a summary of the conceptual model of recovery as defined by the core attributes and the related contextual features.
Fig. 3
Recovery: Summary of Antecedents, Attributes and Consequences.
3.3Contextual features of recovery: Antecedents and consequences
Analysis of the antecedents, testified to a relative consensus across the literature regarding situations that precede the concept of recovery. They are closely interrelated with the concept’s attributes due to the necessity of their presence for recovery to occur. The antecedents of recovery demonstrated six themes; the obtainment of a diagnosis of aphasia, time passed since cerebrovascular accident (CVA), the occurrence of neuroplasticity and/or neural compensation, intervention received, and personal factors. Qualifiers (or secondary antecedents) such as treatment dosage were also frequently referred to across papers and disciplines. Inter-disciplinary discrepancy was identified in the emphasis placed upon antecedents, the most prominent being the significance placed on the nature of intervention. While each discipline alluded to the various form’s intervention may take, medical interventions were referred to at a higher frequency and in greater detail in the discipline of neurology, whereas speech and language therapy was the most prevalent intervention referred to in the disciplines of rehabilitation medicine, nursing and speech and language therapy.
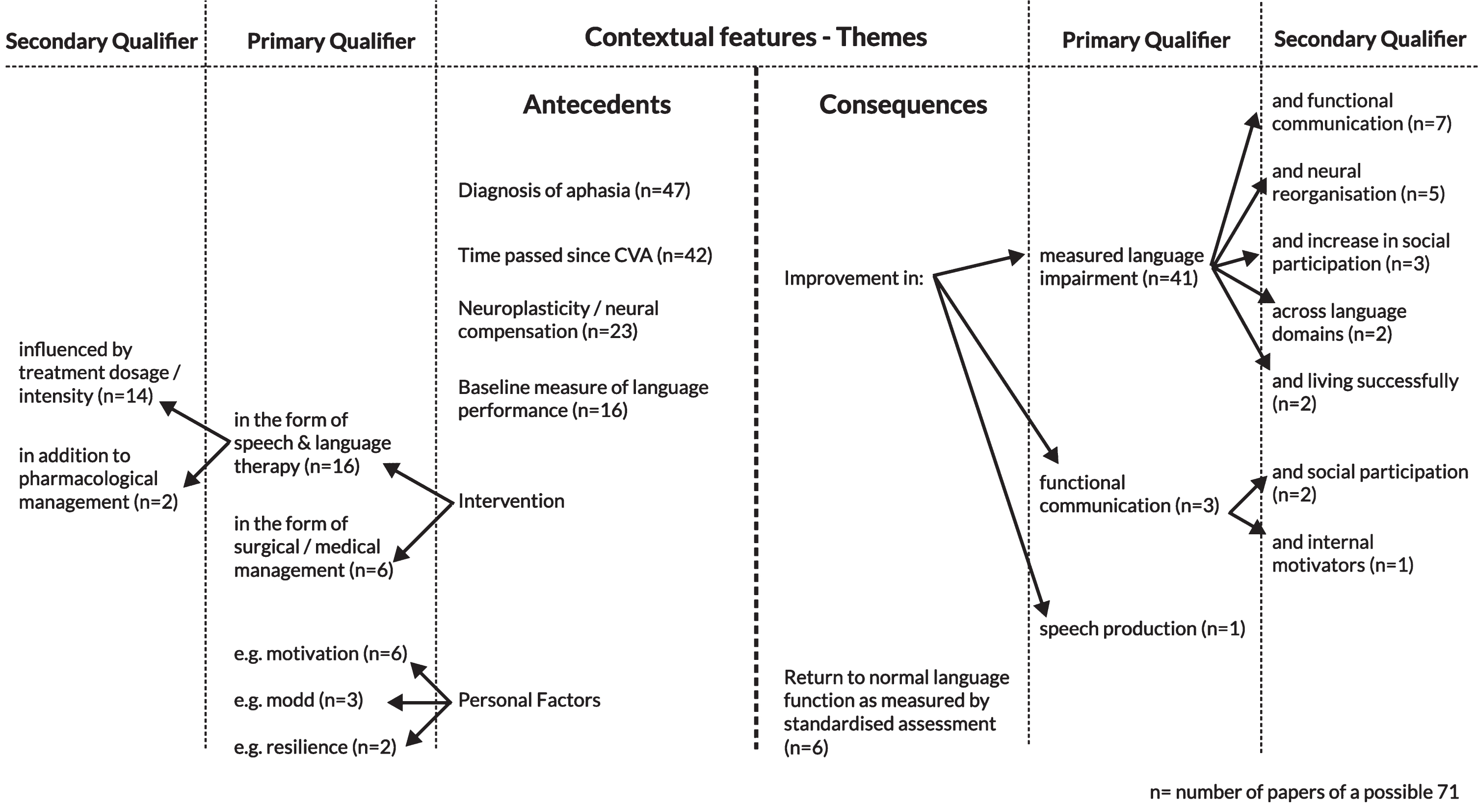
The consequences, or the resulting behaviours, actions, and/or situations that follow the presence of the concept, demonstrated two themes; improvement, and return to normal language function as measure by standardised assessment. Several qualifiers to the theme were similarly revealed, with the principal qualifier being ‘(improvement in) measured language impairment,’ as measured by the data collection tools outlined in Table 3. Across the data set three primary qualifiers and seven secondary qualifiers were identified, as represented in Fig. 4.
Fig. 4
Contextual features of the concept of recovery: Themes and Qualifiers.
3.4Exemplar case of the concept of ‘recovery’
In situations where there is wide variation in the use of a concept, as was the case in this analysis, the exemplar does not serve as an ‘ideal’ or ‘model’ case and instead portrays a “real life” example of the concepts’ contextual applications. An exemplar of the concept was identified in a case report by Kunst and colleagues (2013) and has been summarised and presented below. The paper in which the exemplar is demonstrated was not identified by the bibliographic database search or through citation tracing, a situation not uncommon in concept analysis.
D suffered an ischemic stroke in the left hemisphere in January 2009. He was admitted to hospital for three days presenting with “oral expressive language impairment.” D lives with his wife who has become his primary caregiver. He started attending speech therapy approximately two weeks after he was discharged from hospital. Up until this point, he could communicate with some effectiveness, but he “had many episodes of anomia and phonemic changes”. It was noted that the extent of the lesion seemed to play the biggest role in predicting D’s recovery from aphasia and that “the involved variants in the recovery of aphasia should be considered, ranging from clinical aspects to psychosocial ones”. He was described to be a diligent and active participant in therapy. Baseline measurements of D’s language abilities were taken through use of the Token Test. Other assessments included “neurological, brain CT scan and ultrasound”. D was diagnosed with expressive aphasia affecting both verbal and written modalities at this point. Since beginning therapy, improvements in linguistic function were noted. Recovery of aphasia occurred gradually, especially in the first month’s post-stroke. D is now able to communicate “in a satisfactory way” and has “presented a very positive recovery” (Kunst, Oliveira, Costa, Wiethan & Mota, 2013, pp.1713-1715).
This account was selected as the exemplar case due to its possession of the defining attributes, antecedents, and consequences of the concept, identified in the earlier stages of the analysis. The concept’s existence on a spectrum is reflected in how the authors describe D’s recovery as ‘positive’. The process of recovery is referred to in the timespan across which the case is described, whereas the variable dependent attribute is stated directly. The attribute of deceleration was shown in the sentence “recovery of aphasia occurred gradually, especially in the first months”. Finally, the facilitated and quantifiable attributes were reflected in the familial and rehabilitation service supports noted and the assessment used as a measure of D’s recovery. Further illuminating the concept is the presence of antecedents such as diagnosis, a baseline measure of language and time since stroke, accompanied by the consequences improvement in language impairment and functional communication.
3.5Alignment of the conceptual consensus of ‘recovery’: ICF and LPAA mapping
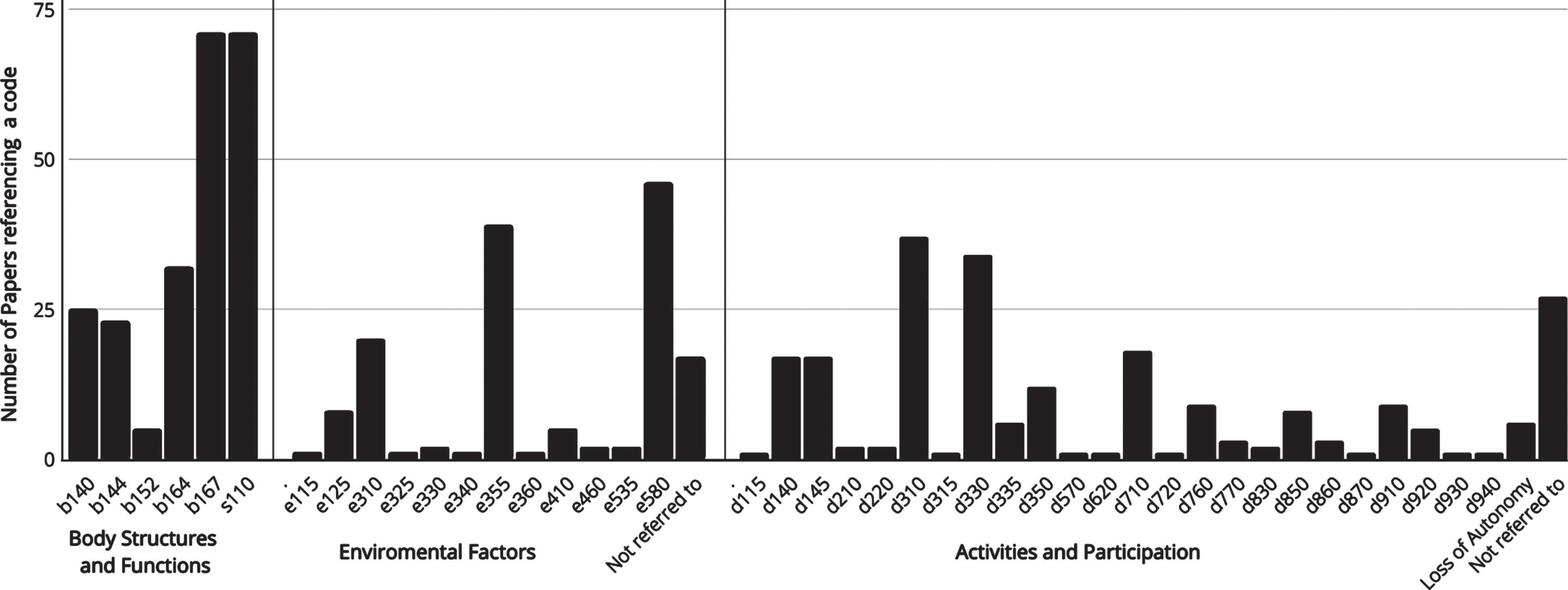
Analysis of the presence (inferred or stated) of codes across all domains of the ICF and the values of the LPAA, offered the opportunity to compare the conceptualisation of recovery in the literature against frameworks advocating for a holistic approach to intervention. Frequency counts in relation to the ICF are displayed in Fig. 5, identifying the number of papers in which a code was identified. The findings demonstrate the research weight attributed to codes residing in the Body Functions and Structures domain. However, the nature and spread of the identified codes demonstrate the extensive spectrum of factors contributing to recovery in the context of aphasia. This finding indicates that while a range of codes are perceived to be relevant to the recovery process, they remain concealed in the research bulk in which ‘aphasia recovery’ is conflated with ‘language recovery’.
Fig. 5
Frequency of ‘International Classification of Functioning, Disability and Health’ codes mentioned or inferred across papers.
The alignment of the conceptual consensus to the values of the rehabilitative philosophy Life Participation Approach to Aphasia demonstrated that the majority included studies (n = 44, 62%) did not allude to any of the LPAA values. Of the remaining papers, 13 aligned with one value, 6 aligned with two values, 3 papers aligned with three values, and a further 3 papers identified four ‘Life Participation Approach to Aphasia’ values. Just 2 studies aligned with all five values of the approach, one of which originated from the discipline of neurology and one from the discipline of speech and language therapy. Value five ‘emphasis on availability of services as needed at all stages of aphasia’ was the most commonly noted in the data sample, corresponding to the attributes ‘process’ and ‘facilitated’.
4Discussion
Through the use of Rodger’s method of concept analysis (2000), the literature’s portrayal of recovery and its conceptual boundaries was found to be vague, to the extent that overlap was identified between the related concepts of ‘language recovery’ and ‘aphasia recovery’, resulting in inconsistencies in the manner in which the concept is expressed in research. The full range of ICF codes and LPAA values identified do not occur frequently enough in the literature to contribute to the core attributes of the concept yet offer an insight into the full scope of factors pertaining to recovery. Hence, while consideration is given to the psychosocial aspects of the concept in the literature, it is to a lesser degree than the focus on linguistic recovery.
Distinguishing recovery in the context of aphasia as a ‘process’ is an important finding as it accounts for the complexities, fluctuations and unknowns associated with the disorder and its impacts on an individual. Complications arise however in the literature’s passive use of the term ‘recovered’ when signifying the endpoint of the recovery ‘process’. There has been no definitive consensus point found in the research as to when an individual progresses from being in the process of recovery to the point of being classed as ‘recovered’, despite frequent use of the term (e.g. Bullier et al., 2020). Furthermore, the consequences of recovery discovered through this analysis are heavily focused on language outcomes, citing ‘improvements in’ or even ‘a return to normal language function.’ Furthermore, relating to the ‘quantifiable’ finding, a consensus document published by the Stroke Recovery and Rehabilitation Roundtable proposed that a test of speech or language production is the optimal measure of aphasia recovery (Bernhardt et al., 2017). Such a consensus suggests that measures of impairment are the near-exclusive outcome of the process of recovery, raising the question as to whether the literature’s conceptualisation of recovery is indeed reflective of the rhetoric of the ICF and LPAA.
How recovery is defined has a marked impact on research and practice –evident in the response to the evolving definition of recovery in the field of mental health. The disparate ways of conceptualising recovery in the context of mental health disorders led to a response in which the understanding of recovery was progressed beyond the remission of symptoms, instead focusing on reintegration of oneself in life and society despite ongoing illness/symptoms. This field-wide shift in understanding of the nature of recovery and the manner in which it is discussed has led to a redirection of research priorities, resulting in more meaningful service provision. We suggest that the concepts raised in this analysis could be brought to people with aphasia for further specification and nuance, ultimately yielding a broad definition of recovery as an umbrella term, in a similar manner as the field of mental health has achieved. This umbrella term should capture highly personal, individual and nonlinear process that appears to be multifactorial. An alternative, or perhaps complementary, approach to generating a single broad definition of such an all-encompassing term in the case of aphasiology, may be to move towards conscientious use of distinct, meaningful terms. Differentiation in the expression of the concept would lead to greater specificity of purpose across the relevant literature, directing readers, researchers or clinicians towards the specific aspect of recovery being referred to or measured; be it language recovery, neuroplastic recovery, personal recovery, etc. Avoiding the use of the singular term ‘aphasia recovery’ to express the entirety of the concept acknowledges the multi-faceted nature of recovery in this context and would support the reorientation of its currently impairment focused status. This specification may similarly support interdisciplinary communication and interpretation of the concept, facilitating recognition of service delivery priorities through increased clarification.
Additionally, furthering the understanding of recovery as a process opposed to an end goal supports the prioritisation of research outside of the acute stages of post-stroke aphasia. Recovery is inevitably a highly individualised process. Providing clarity about what is meant by recovery may ensure that in conversations about prognosis, goals or progress, the client and clinician are both talking about the same idea, and also considering the multiplicity of forms that recovery may take. Therefore, this analysis re-emphasises the LPAA’s call for the re-focusing of research priorities surrounding the consequences of aphasia (Chapey et al., 2000).
The concept analysis presented is not without its limitations. Data was gathered exclusively from electronic databases, as influenced by Rodgers (2000). This meant that books, grey literature, and other data sources were excluded from the analysis, possibly limiting the data sample included. Similarly, the inclusion of English language papers/only papers with a readily available translation may have been a further limiting factor. In order for this research to be truly reflective of the concept and responsive to PWA’s recovery priorities, they themselves must play an active role in influencing recovery’s conceptualisation. Interview-based studies comparing the conceptual characteristics identified in this analysis with the perspectives of service users and the practices of clinicians, would offer valuable insight into the expression of the concept. Similarly, such research would address the methodological critiques of concept analysis through the generation of empirical evidence, thus offering the opportunity for reformulation of service delivery as guided by PWA’s needs. We suggest that the findings of this concept analysis may be a useful starting point for interviews with people with aphasia and their family members.
Concepts are ever developing and evolving phenomena. Side by side comparisons of the concept with frameworks such as the ICF and the LPAA demonstrate that the conceptual consensus is still emerging in the literature, portraying an impairment-oriented conceptualisation of recovery. Intrinsic to Rodgers methodology however, is the recognition that concepts evolve over time. Active and purposeful advancement of the conceptualisation of recovery will facilitate services to offer the highest standard of care to PWA.
Acknowledgments
The authors have no acknowledgements.
Conflict of interest
The authors report there are no competing interests to declare.
Funding
This paper is based on the unpublished undergraduate thesis of Laoighse Gleeson, supervised by Caroline Jagoe. Laoighse Gleeson was a recipient of a Tavistock Trust for Aphasia Student Prize in 2021 for this work, but the project itself was unfunded.
SUPPLEMENTARY MATERIAL
{ label (or @symbol) needed for fn } The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/ACS-220013.
References
1 | Ali, M. , Lyden, P. , Brady, M. ((2015) ) Aphasia and Dysarthria in Acute Stroke: Recovery and Functional Outcome. Int J Stroke, 10: (3), 400–406. https://doi.org/10.1111/ijs.12067. |
2 | Bernhardt, J. , Hayward, K. S. , Kwakkel, G. , Ward, N. S. , Wolf, S.L. , Borschmann, K. , Cramer, S. C. ((2017) ) Agreed definitions anda shared vision for new standards in stroke recovery research: TheStroke Recovery and Rehabilitation Roundtable taskforce. Int JStroke, 12: (5), 444–450. https://doi.org/10.1177/1747493017711816. |
3 | Berthier, M. L. , García-Casares, N. , Walsh, S. F. , Nabrozidis, A. , Ruíz de Mier, R. J. , Green, C. , Pulvermüller, F. ((2011) ) Recovery from post-stroke aphasia: lessons from brain imaging and implications for rehabilitation and biological treatments. Discov Med, 12: (65), 275–289. |
4 | Borkin, J. R. , Steffen, J. J. , Ensfield, L. B. , Krzton, K. , Wishnick, H. , Wilder, K. , Yangarber, N. ((2000) ) RecoveryAttitudes Questionnaire: Development and evaluation. Psychiatric Rehabilitation Journal, 24: (2), 95–102. https://doi.org/10.1037/h0095112. |
5 | Brown, K. , Worrall, L. E. , Davidson, B. , Howe, T. ((2012) ) Livingsuccessfully with aphasia: A qualitative meta-analysis of theperspectives of individuals with aphasia, family members, andspeech-language pathologists. International journal of speech language pathology, 14: (2), 141–155. |
6 | Bullier, B. , Cassoudesalle, H. , Villain, M. , Cogn,é M. , Mollo, C. , De Gabory, I. , Glize, B. ((2020) ) New factors thataffect quality of life in patients with aphasia. Annals of physical and rehabilitation medicine, 63: (1), 33–37. https://doi.org/10.1016/j.rehab.2019.06.015. |
7 | Chapey, R. , Duchan, J. F. , Elman, R. J. , Garcia, L. J. , Kagan, A. , Lyon, J. G. , Simmons Mackie, N. ((2000) ) Life participationapproach to aphasia: A statement of values for the future. The ASHA Leader, 5: (3), 4–6. https://doi.org/10.1044/leader.FTR.05032000.4. |
8 | de Boer, R. G. A. , Spielmann, K. , Heijenbrok-Kal, M. H. , van derVliet, R. , Ribbers, G. M. , van de Sandt-Koenderman, W. M. E. ((2017) ) The Role of the BDNF ValMet Polymorphism in Recovery ofAphasia After Stroke. Neurorehabil Neural Repair, 31: (9), 851–857. https://doi.org/10.1177/1545968317723752. |
9 | Farkas, M. ((1996) ) Recovery, rehabilitation, reintegration: Wordsvs. meaning. World Association of Psychosocial Rehabilitation 683 Bulletin, 8: (4), 6–8. |
10 | Fonseca, J. , Raposo, A. , Martins, I. P. ((2018) ) Cognitiveperformance and aphasia recovery. Topics in Stroke Rehabilitation, , 25: (2), 131–136. https://doi.org/10.1080/10749357.2017.1390904. |
11 | Furlanis, G. , Ridolfi, M. , Polverino, P. , Menichelli, A. , Caruso, P. , Naccarato, M. , Manganotti, P. ((2018) ) Early Recovery of Aphasia through Thrombolysis: The Significance of Spontaneous Speech. J Stroke Cerebrovasc Dis, 27: (7), 1937–1948. https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.02.043. |
12 | Geranmayeh, F. , Brownsett, S. L. E. , Wise, R. J. S. ((2014) ) Task-induced brain activity in aphasic stroke patients: what isdriving recovery. Brain: A Journal of Neurology, 137: (10), 2632–2648. https://doi.org/10.1093/brain/awu163. |
13 | Gilbert, T. T. , Gilbert, M. R. , Culpepper, L. , Wilkinson, J. E. ((2013) ) Voices of recovery: a family physician’s experience ofaphasia. Fam Med, 45: (3), 201–204. |
14 | Glize, B. , Bigourdan, A. , Villain, M. , Munsch, F. , Tourdias, T. , deGabory, I. , .. Sibon, I. ((2019) ) Motor evoked potential ofupper-limbs is predictive of aphasia recovery. Aphasiology, 33: (1), 105–120. https://doi.org/10.1080/02687038.2018.1444137. |
15 | Kagan, A. ((2020) ) The Life Participation Approach to Aphasia: A-Year Milestone. Perspectives of the ASHA Special Interest Groups, 5: (2), 370. https://doi.org/10.1044/2020_PERSP-20-00017. |
16 | Kakuma, R. , Hamilton, B. , Brophy, L. , Minas, H. , Harvey, C. (2017) Models of care for people with severe and enduring mentalillness, Models of care for people with severe and enduringmental illness. |
17 | Kunst, L. R. , Oliveira, L. D. , Costa, V. P. , Wiethan, F. M. , Mota, H. B. ((2013) ) Speech therapy effectiveness in a case ofexpressive aphasia resulting from stroke. Revista CEFAC, 15: (6), 1712–1717. |
18 | Lloyd, C. , Waghorn, G. , Williams, P. L. ((2008) ) ConceptualisingRecovery in Mental Health Rehabilitation. British Journal of Occupational Therapy, 71: (8), 321–328. https://doi.org/10.1177/030802260807100804. |
19 | Marangolo, P. , Caltagirone, C. ((2014) ) Options to enhancerecovery from aphasia by means of non-invasive brain stimulation andaction observation therapy. Expert Rev Neurother, 14: (1), 75–91. https://doi.org/10.1586/14737175.2014.864555. |
20 | McCauley, C. O. , McKenna, H. P. , Keeney, S. , McLaughlin, D. F. ((2015) ) Concept analysis of recovery in mental illness in youngadulthood. Journal of psychiatric and mental health nursing, 22: (8), 579–589. https://doi.org/10.1111/jpm.12245. |
21 | McKinnon, E. T. , Fridriksson, J. , Glenn, G. R. , Jensen, J. H. , Helpern, J. A. , Basilakos, A. , Bonilha, L. ((2017) ) Structural plasticity of the ventral stream and aphasia recovery. Annals of Neurology,, 82: (1), 147–151. https://doi.org/10.1002/ana.24983. |
22 | Meier, E. , Johnson, J. , Pan, Y. , Kiran, S. ((2019) ) The utility oflesion classification in predicting language and treatment outcomesin chronic stroke-induced aphasia. Brain Imaging And Behavior, 13: (6), 1510–1525. https://doi.org/10.1007/s11682-019-00118-3. |
23 | Penrod, J. , Hupcey, J. E. ((2005) ) Enhancing methodologicalclarity: principle-based concept analysis. Journal of Advanced Nursing,, 50: (4), 403–409. https://doi.org/10.1111/j.1365-2648.2005.03405.x. |
24 | Pringle, J. , Hendry, C. , McLafferty, E. , Drummond, J. ((2010) ) Stroke survivors with aphasia: personal experiences of coming home. British Journal of Community Nursing, 15: (5), 241–247. https://elib.tcd.ie/loginurl=https://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=&site=ehost-live. |
25 | Rodgers, B. L. , Jacelon, C. S. , Knafl, K. A. ((2018) ) Concept Analysis and the Advance of Nursing Knowledge: State of the Science. Journal of Nursing Scholarship, 50: (4), 451–459. https://doi.org/10.1111/jnu.12386. |
26 | Rodgers, B. , Knafl, K. ((2000) ) Concept Development in Nursing: Foundations, Techniques, and Applications (2nd ed.). Philadelphia: Saunders. |
27 | Smania, N. , Gandolfi, M. , Aglioti, S. M. , Girardi, P. , Fiaschi, A. , Girardi, F. ((2010) ) How Long Is the Recovery of Global Aphasia? Twenty-Five Years of Follow-up in a Patient With Left Hemisphere Stroke. Neurorehabilitation & Neural Repair, 24: (9), 871–875. https://doi.org/10.1177/1545968310368962. |
28 | Stefaniak, J. D. , Halai, A. D. , Lambon Ralph, M. A. ((2020) ) Theneural and neurocomputational bases of recovery from post-strokeaphasia. Nature Reviews Neurology, 16: (1), 43–55. https://doi.org/10.1038/s41582-019-0282-1. |
29 | Stewart, V. , Visser, K. , Slattery, M. ((2020) ) Supporting choice,recovery and participation: Information is the key to NDIS accessfor those with psychosocial disability. Journal of SocialInclusion,, 11: (2), 33–46. |
30 | Thiel, A. , Hartmann, A. , Rubi-Fessen, I. , Anglade, C. , Kracht, L. , Weiduschat, N. , Heiss, W.-D. ((2013) ) Effects of noninvasive brainstimulation on language networks and recovery in early poststrokeaphasia. Stroke (00392499), 44: (8), 2240–2246. https://doi.org/10.1161/STROKEAHA.111.000574. |
31 | van Oers, C. A. , Vink, M. , van Zandvoort, M. J. , van der Worp, H.B. , de Haan, E. H. , Kappelle, L. J. , Dijkhuizen, R. M. ((2010) ) Contribution of the left and right inferior frontal gyrus inrecovery from aphasia. A functional MRI study in stroke patientswith preserved hemodynamic responsiveness. Neuroimage, 49: (1), 885–893. https://doi.org/10.1016/j.neuroimage.2009.08.057. |
32 | Watila, M. M. , Balarabe, S. A. ((2015) ) Factors predictingpost-stroke aphasia recovery. J Neurol Sci, 352: (1-2), 12–18. https://doi.org/10.1016/j.jns.2015.03.020. |
33 | Wilson, J. (1963) CambridgeUniversity Press, Thinking with concepts. |
34 | Wilson, S. M. , Eriksson, D. K. , Brandt, T. H. , Schneck, S. M. , Lucanie, J. M. , Burchfield, A. S. , Kidwell. C. S. ((2019) ) Patterns of Recovery From Aphasia in the First Weeks After Stroke. Journal of Speech, Language & Hearing Research, 62: (3), 723–732. https://doi.org/10.1044/2018_JSLHR-L-18-0254. |
35 | World Health Organization. (2001). International Classification of Functioning, Disability, and Health: ICF. World Health Organization. |
36 | Worrall, L. (2020) Emeritus Professor Linda Worrall [Tweet]. Retrieved from https://twitter.com/aphasiologist1/status/1270909865955782656. |
37 | Wortman-Jutt, S. , Edwards, D. J. ((2017) ) Transcranial DirectCurrent Stimulation in Poststroke Aphasia Recovery. Stroke (00392499), 48: (3), 820–826. https://doi.org/10.1161/STROKEAHA.116.015626. |
38 | Yagata, S. A. , Yen, M. , McCarron, A. , Bautista, A. , Lamair-Orosco, G. , Wilson, S. M. ((2017) ) Rapid recovery from aphasia afterinfarction of Wernicke’s area. Aphasiology, 31: (8), 951–980. https://doi.org/10.1080/02687038.2016.1225276. |
39 | Zhou, Q. , Lu, X. , Zhang, Y. , Sun, Z. , Li, J. , Zhu, Z. ((2018) ) Telerehabilitation Combined Speech-Language and Cognitive TrainingEffectively Promoted Recovery in Aphasia Patients. Front Psychol, 9: , 2312. https://doi.org/10.3389/fpsyg.2018.02312. |
Notes
1 (1) The explicit goal is enhancement of life participation; (2) Everyone affected by aphasia is entitled to service; (3) Success measures include documented life enhancement changes; (4) Both personal and environmental factors are intervention targets; (5) Emphasis on availability of services as needed at all stages of aphasia


