
The quality of clinical practice guidelines for fiberoptic endoscopic evaluation of swallowing: A systematic review
Abstract
BACKGROUND:
Clinical practice guidelines (CPGs) can act as a bridge between clinical research and everyday practice. CPGs have been generated to inform Fiberoptic Endoscopic Evaluation of Swallowing (FEES), but their quality is unclear.
OBJECTIVE:
This study aims to systematically evaluate the quality of FEES CPGs to identify their suitability for use in clinical practice.
METHODS:
A systematic review of the literature was conducted. A comprehensive search of four academic databases (Medline, Embase, CINAHL, Web of Science) and other sources was completed. Three independent researchers used the Appraisal of Guidelines for Research and Evaluation-II (AGREE-II) instrument to appraise the quality of included CPGs. CPGs were rated over 23 items across six domains. Intraclass correlation coefficients established agreement across raters.
RESULTS:
Four FEES CPGs were included. Individual CPG scores ranged from 0% to 89% across AGREE-II domains. Median domain scores were “Scope and Purpose” 66%; “Stakeholder Involvement” 47%; “Rigour of Development” 29%; “Clarity of Presentation” 60%; “Applicability” 13% and “Editorial Independence” 0%. None of the CPGs included sufficient detail regarding their development methodology and supporting evidence. No CPG was recommended to guide practice in their current state. Only 1 CPG was recommended for use, upon appropriate modifications.
CONCLUSION:
CPGs are highly influential tools that play a vital role in guiding clinical practice. Study findings highlight a scarcity of high-quality FEES CPGs to inform dysphagia practice. Superior FEES CPGs are required to ensure individuals with dysphagia are benefiting from high-quality research emerging internationally.
1Introduction
Since initially described in 1988, Fiberoptic Endoscopic Evaluation of Swallowing (FEES) has become a widely employed dysphagia evaluation tool (Langmore, Schatz, & Olsen, 1988). It involves the trans-nasal insertion of a flexible nasendoscope to directly visualise the nasopharynx, oropharynx, laryngeal structures, sensory responses and secretions during swallowing (Wallace et al., 2020). The assessment incorporates the anatomical-physiological evaluation of structural movements, pharyngeal mucosa, vocal cord adduction and salivary management. A formal assessment of swallowing ability across different consistencies and trial of compensatory or rehabilitation strategies can also be incorporated to inform treatment (Dziewas et al., 2014; Miller, Schroeder Jr, & Langmore, 2020).
Research suggests that both FEES and videofluoroscopic swallow study (VFSS) are reference standard instrumental dysphagia evaluations, with FEES being sensitive to the presence and severity of pharyngeal residue (Langmore, 2017). The demand for FEES has increased as it does not involve radiation and it can be used in intensive care settings and outpatient clinics (Miller et al., 2020). Furthermore, it can monitor fatigue during meals and act as a biofeedback tool in therapy (Dziewas et al., 2017; Miller et al., 2020).
Staffing models for FEES vary across settings with trained speech and language therapists (SLTs) often completing FEES examinations independently without an ear, nose and throat (ENT) surgeon or medical professional present. However, FEES is a procedure with potential adverse events including epistaxis, laryngospasm and vasovagal events (Dziewas et al., 2019). Therefore, high-quality guidance is required to ensure assessments are completed safely and accurately (Dziewas et al., 2017).
FEES has evolved considerably over the last thirty years (Langmore, 2017). As well as technological developments, high-quality research has advanced the FEES protocol (Baijens, Speyer, Pilz, & Roodenburg, 2014; Fuller, Leonard, Aminpour, & Belafsky, 2009; Kaneoka, Krisciunas, Walsh, Raade, & Langmore, 2015; Warnecke et al., 2009). Novel analysis methods are also being established to facilitate FEES interpretation and guide treatment (Curtis et al., 2021; Pisegna, Kaneoka, Leonard, & Langmore, 2018). Given these advances, there is significant potential for variability in FEES protocols and analysis methods across clinical settings and a distinct possibility that robust research is not being integrated into clinical practice. A proactive approach is required to standardise and advance FEES evaluation and to ensure practice represents the evidence base.
Clinical practice guidelines (CPGs) are highly influential and useful tools that provide evidence-informed recommendations to guide clinical practice and reduce unwarranted variation (Boaden, Nightingale, Bradbury, Hives, & Georgiou, 2020; Chong, 2018). They are a way of bridging the gap between research findings and clinical practice and can improve quality of care and patient outcomes (Sekercioglu et al., 2017). They reduce preventable adverse events and integrate policy, best practice, local settings and patient preference (Kredo et al., 2016). The definition of CPGs describes them as recommendations guided by a systematic review of the evidence and an assessment of the benefits and harm of various care options (Institute of Medicine, 2011). This definition reflects the emphasis on methodological rigour in the development process (Kredo et al., 2016). The potential of CPGs to promote patient outcomes depends on the quality of the guidelines themselves, the availability of the evidence and their uptake in practice (Gillespie et al., 2018).
Research evaluating the standards of CPGs has concluded that inconsistency of CPG quality has been identified across healthcare disciplines (Boaden et al., 2020; Kredo et al., 2016; Yang et al., 2018; Zafra-Tanaka, Goicochea-Lugo, Villarreal-Zegarra, & Taype-Rondan, 2019). Likewise, discrepancies among recommendations provided have also been highlighted (Andrade, Pereira, van Cingel, Staal, & Espregueira-Mendes, 2020; Boaden et al., 2020; Quintyne & Kavanagh, 2019). The Appraisal of Guidance for Research & Evaluation-II (AGREE-II) instrument evaluates the quality and guides the future formulation of CPGs (Brouwers et al., 2010). It has allowed for feasible quality measurement and has informed practitioners about the relevance of CPG implementation across disciplines (Andrade et al., 2020; Boaden et al., 2020; Gillespie et al., 2018; Lin et al., 2020; Yang et al., 2018; Zafra-Tanaka et al., 2019). Evidence-based practice is reliant on high-quality and up-to-date research to identify information regarding diagnostics, risk factors, treatment outcomes and patterns of care, which can in turn promote positive patient outcomes (Black, Balneaves, Garossino, Puyat, & Qian, 2015).
In a recent study carried out by Boaden and colleagues (2020), CPGs for VFSS were appraised using the AGREE-II instrument. Findings addressed both the lack of rigorous development and inclusion of high-quality evidence to inform recommendations. No VFSS CPG was recommended for use without modifications and multiple shortcomings were highlighted. These findings are essential to portray areas of need for the future development of CPGs for VFSS, which are urgently required. The same investigation into CPG quality is warranted for other instrumental dysphagia assessments including FEES.
Whilst FEES CPGs developed to date have played a crucial role in informing FEES services worldwide, their quality to guide clinical practice is unclear. High-quality CPGs for FEES are fundamental to ensure standardisation of care, to reduce variation in practice and maintain an objective tool for the diagnosis and management of dysphagia. This study critically appraises FEES CPGs using the AGREE-II instrument to assess their ability to effectively guide clinical practice. The primary research question was; what is the quality of all international FEES CPGs for SLTs to refer to in clinical practice, according to the AGREE II criteria?
The authors hypothesised that the quality of CPGs for FEES would be limited. This is based on findings in recent research evaluating the quality of CPGs for VFSS (Boaden et al., 2020), given that VFSS is another gold standard procedure for dysphagia assessment and management. Findings from this study can therefore inform the future development of high-quality CPGs for FEES.
2Methods
2.1Research design
A systematic review of the literature was completed to identify and appraise international FEES CPGs, to establish their ability to effectively guide clinical dysphagia practice. This systematic review is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. Ethical approval was not required as this study did not involve human or animal participants.
2.2Search strategy
A search strategy was developed to search across four bibliographic databases, including PubMed (Medline), Embase (Scopus), CINAHL and Web of Science. This search strategy was reviewed by a subject librarian and performed on 10/10/20. The timeframe was from inception of the database to October 2020. Other sources were searched on 11/10//20, including The National Institute for Health & Care Excellence (NICE) Guidance, Prospero- The International Prospective Register of Systematic Reviews, Google Search and through the manual searching of national SLT professional associations’ websites. The search of the academic databases and Prospero included 3 search strings. Search terms were customised for each database but included similar variations of ‘dysphagia’, ‘FEES’ and ‘practice guidelines’ for the controlled vocabulary and title/abstract terms of the three respective search strings. The full search strategy is presented in Supplementary Information Table 1.
Websites from the following professional associations were manually searched on 11/10/20 to identify publications of potential relevance: Royal College of Speech & Language Therapists (RCSLT); Speech Pathology Australia (SPA); American Board for Swallowing & Swallowing Disorders; American Speech-Language Hearing Association (ASHA); New Zealand Speech-Language Therapists’ Association (NZSTA); Dysphagia Research Society; Japanese Society of Dysphagia Rehabilitation (JSDR); European Society for Swallowing Disorders (ESSD) and Hong Kong Association of Speech Therapists. NICE Guidance and Google were also searched in this manner. Search terms used within these websites were ‘fiberoptic endoscopic evaluation of swallowing’ or ‘flexible endoscopic evaluation of swallowing’. An additional search was carried out on 05/09/21 to ensure that no other CPGs were published more recently.
2.3Eligibility criteria
2.3.1Inclusion criteria
Included CPGs were those defined as documents that aimed to outline recommendations, according to the following criteria: 1) national or professional SLT association guidance documents, 2) full texts available in English, 3) CPGs focused solely on FEES within the context of dysphagia assessment across all age groups, 4) where two or more versions of the CPG existed, only the most recent version was included. For the purposes of this study, guidance documents (including position papers and practice standards) developed to guide clinical FEES evaluations were included. This was due to the very limited number of CPGs for FEES developed to date. This broad inclusion criterion has also been observed in recent research investigating the quality of CPGs for VFSS, whereby limited CPGs were available internationally to guide clinicians also (Boaden et al., 2020).
2.3.2Exclusion criteria
Studies were excluded if 1) they were focused on overall dysphagia assessment and not specific to the FEES procedure, 2) developed in the context of a global pandemic e.g., COVID-19, 3) they were designed as local evidence-based protocols for specific institutions. For any CPG that was identified in languages other than English, a translated version was searched for and contact was made with the author to request an English-translated version. A CPG was identified from JSDR, however, as there was no English translation available upon request, it was excluded.
2.4Selection process
The search results were stored in EndNote X9 and uploaded to the Covidence Systematic Review Software, where duplicates were removed and the title/abstract screen was completed. Reference lists of selected studies from the search of databases and other sources were screened to locate publications of potential relevance. Four studies were identified in this manner and were included in the full text review. Worldwide experts in the area of FEES and relevant professional associations were contacted via email regarding their knowledge of any additional CPGs available. No further publications were identified in this manner.
2.5Data extraction
Abstract screening was carried out by two independent reviewers (LMS and RB). Abstracts were discussed collectively using the eligibility criteria if any disagreements occurred. If uncertainty remained, the full text would be retrieved and reviewed to arbitrate the disagreement, but this did not occur. Full consensus was required for abstracts to be included for full text review.
Data was extracted and reviewed by two researchers (LMS and JR) using a pre-developed data extraction table on Microsoft Excel. Data extraction tables were developed to extract CPG characteristics and AGREE-II appraisal scores. The following data was extracted to identify characteristics from the included studies; professional association, year published, CPG title, development method included, systematic review included, external review included, grading system included, service user involvement, search strategy included, target group outlined and potential candidates for FEES discussed. The AGREE-II individual domain scores and rationale for scores for each appraiser were documented in a data extraction table also. All data was then combined and tabulated to facilitate the descriptive analysis of results.
2.6AGREE-II training and rating
The four CPGs underwent a quality assessment using the AGREE-II tool, which was rated by 3 independent researchers (LMS, SL and JR). The AGREE-II instrument evaluates the methodological rigour and transparency of CPG development. (Brouwers et al., 2010) The tool consists of 23 items organised into six domains: 1) Scope and Purpose, 2) Stakeholder’(s) Involvement, 3) Clarity of Presentation, 4) Rigour of Development, 5) Applicability and 6) Editorial Independence. Each item is assessed using a 7-point Likert scale (1- “strongly disagree” to 7- “strongly agree”) based on the criteria provided. This instrument was chosen as it is the most common tool to specifically evaluate CPGs. (Boaden et al., 2020)
The AGREE Enterprise website (www.agreetrust.org/), provides an AGREE training module, which was completed by the researchers and the user’s manual was examined before the employment of the instrument. Items were rated with reference to these resources and rationale for the scores issued were recorded in the comments section.
Overall scores for each domain were calculated in accordance with the algorithm discussed in the AGREE-II manual (as seen on www.agreetrust.org/). A domain score of 60% or above was deemed as good quality. This score was taken from previous research evaluating the quality of CPGs (Boaden et al., 2020; Hurkmans, Jones, Li, & Vliet Vlieland, 2011; Johnston et al., 2018; Lucendo et al., 2017). The AGREE-II does not provide specific scores to classify as adequate quality, and states that this should be decided by the user and guided by the context in which they are used. The same cut-off point was used for each domain. Two overall assessments of the CPGs were also completed within the AGREE-II checklist. These consider the overall quality score and recommendation for use in clinical practice, taking into account the criteria considered during the critical appraisal. The total score of the AGREE-II domains for each CPG was not calculated as recommended by the AGREE protocol, given that domains may not be weighted equally. Reviewers met to agree final scores if any disagreement occurred on these items.
2.7Data analysis
Data was analysed to compare common characteristics and quality appraisal scores. The level of agreement between AGREE-II appraisers across the four CPGs was evaluated to assess reliability between appraisers. This was identified by calculating the percentage agreement in appraisers’ scores of the 23 individual AGREE-II items assessed across the four CPGs. An intraclass correlation coefficient (ICC) was calculated using SPSS v.26 to measure inter-rater reliability of the three appraisers’ scores for each CPG evaluated.
3Results
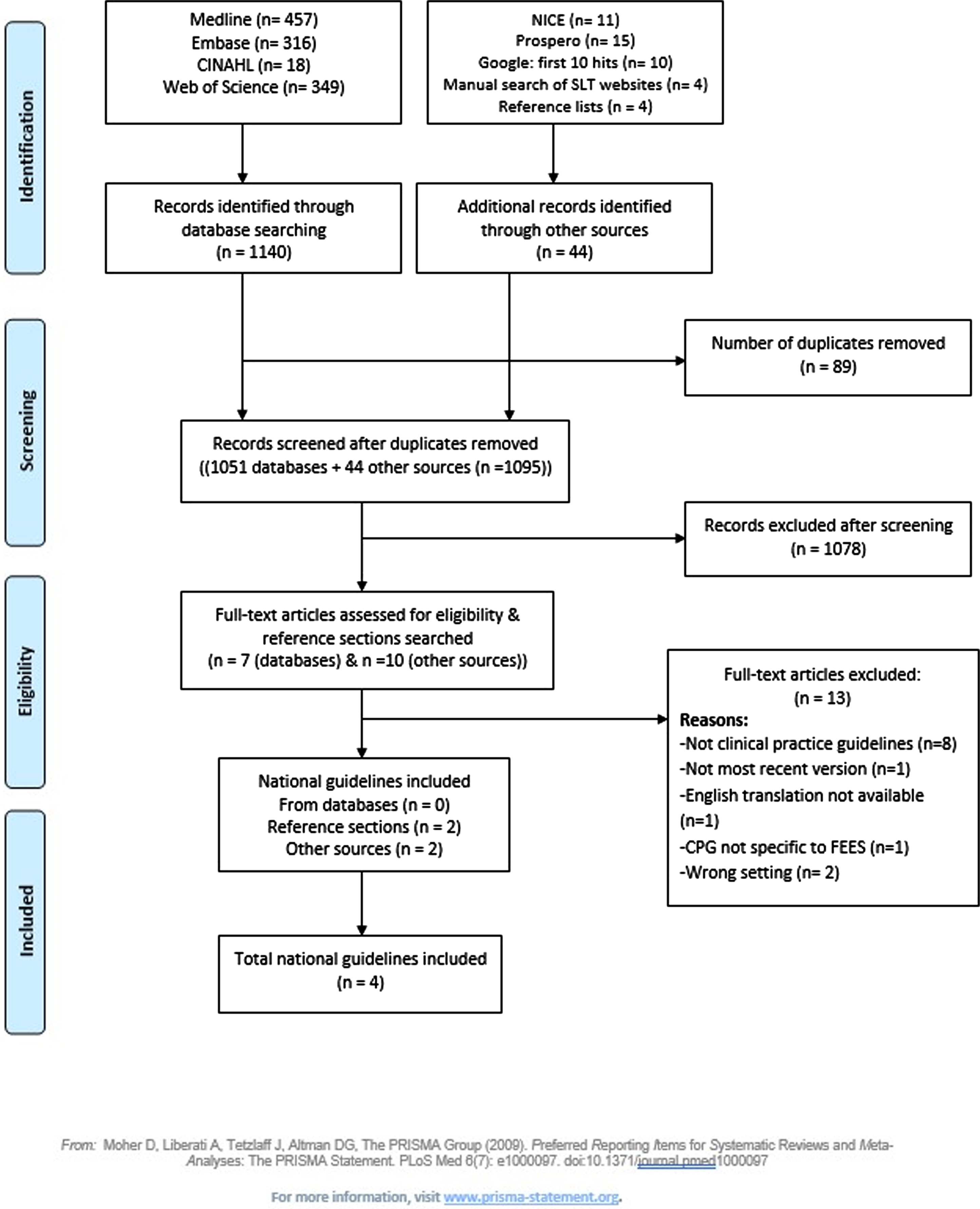
The search of academic databases identified 1140 studies and 44 were located from other sources. Following the removal of duplicates and the title/abstract screening, 17 studies underwent a full text review. Eligible studies underwent a full text review, whereby 13 were excluded with reasons listed in Fig. 1. There was 100% agreement between reviewers during the full text review. Four texts met the eligibility criteria and were included in this review. Two of the included CPGs (ASHA, 2004; SPA, 2019) were accessed behind a paywall.
Fig. 1
PRISMA flow diagram for the study identification process.
3.1Characteristics of included CPGs
The international guidelines represented national SLT professional associations across four countries: Australia, United Kingdom, United States and New Zealand. Three of the CPGs were published between 2018 and 2020, with one published less recently in 2004. All of the included CPGs were written in English.
Discrepancies were established in terms of characteristics such as their development method, grading systems included and service user involvement in the development process. Additional characteristics are outlined in Table 1.
Table 1
Characteristics of Included Clinical Practice Guidelines
| Professional Association and Year Published | Country | Guideline Title | CPG Development Method | Included Systematic Review of Evidence | Externally Reviewed | Grading System Included | Service User Involvement in CPG Development | Search Strategy | Target Group Outlined | Potential Candidates for FEES Discussed |
| The Speech Pathology Association of Australia Limited 2019 | Australia. | Clinical Guideline: Flexible Endoscopic Evaluation of Swallowing. | Not discussed. | No. | No. | Yes- Based on NHMRC levels of evidence and grades of recommendation (NHMRC, 2009). | No. | Not included. | SLTs in Australian healthcare contexts. | No. Patient selection discussed but no specific populations named. |
| Royal College of Speech &Language Therapists 2020 | United Kingdom. | Fiberoptic Endoscopic Evaluation of Swallowing: The Role of Speech and Language Therapy. RCSLT Position Paper. | Brief method description. Literature review carried out. Criteria for studies: validity, reliability, clinical groups, efficacy and utility, safety and outcomes. | No. | Consultation period with dysphagia advisors, international FEES experts, stakeholders (eg. ENT UK) and service users. Lacks details about process. | No. | Yes. Patients included within the consultation period. Lacks detail regarding methods. | Not included. | SLTs working in the field of dysphagia, ENT surgeons, respiratory consultants, neurologists, service managers, commissioners of service involving people with dysphagia. | Yes. List of typical clinical groups included. |
| The New Zealand Speech-Language Therapists’ Association 2018 | New Zealand. | NZSTA Practice Standards: Flexible Endoscopic Evaluation of Swallowing in Adults &Children in New Zealand. | Not discussed. | No. | Yes- externally reviewed by NZSTA Executive Committee and NZSTA Health Leaders Forum. Lacks details about process. | No. | No. | Not included. | SLTs working with FEES. | Yes. Lists high risk and complex patient groups only. |
| American Speech-Language-Hearing Association 2004 | United States. | Role of the Speech-Language Pathologist in the Performance and Interpretation of Endoscopic Evaluation of Swallowing: Guidelines. | Not discussed. | No. | No. | No. | No. | Not included. | SLTs. | Yes. List of potential candidates for FEES included. |
NHMRC, National Health and Medical Research Council (Australia). ENT Surgeon, ear nose and throat surgeon. CPG, clinical practice guideline. SLT, speech and language therapist. FEES, fiberoptic endoscopic evaluation of swallowing. NZSTA, The New Zealand Speech-Language Therapists’ Association.
3.2CPG quality appraisal
The domain scores for each CPG are demonstrated in Table 2 and Fig. 2. Table 2 displays a summary of the scores for each AGREE-II domain, including the median and range. A wide range of scores are depicted between domains. Four out of six domains achieved a median score of below 60% and no CPG scored above the 60% threshold in more than three domains.
Table 2
Summary of domain, median and range scores for AGREE-II appraisal
| Domain | AGREE-II Definition | SPA | RCSLT | NZSTA | ASHA | Median | Range in |
| (2019) | (2020) | (2018) | (2004) | Domain | Domain | ||
| Score | Scores | ||||||
| 1.Scope &Purpose | The overall aim of the CPG, specific health questions &target population. (Item 1–3). | 63% | 89% | 69% | 50% | 66% | 50–89% |
| 2.Stakeholder Involvement | The extent to which the CPG was developed by appropriate stakeholders &represents views of intended user. (Item 4–6). | 50% | 78% | 44% | 35% | 47% | 35–78% |
| 3.Rigour of Development | Process used to gather &synthesise the evidence, methods to formulate &update recommendations. (Item 7–14). | 32% | 59% | 24% | 25% | 29% | 24–59% |
| 4.Clarity of Presentation | Deals with language, structure, and format of the CPG. (Item 15–17). | 63% | 78% | 33% | 57% | 60% | 33–78% |
| 5.Applicability | The likely barriers &facilitators to implementation, strategies to improve uptake &resource implications of applying the CPG. (Item 18–21). | 15% | 26% | 8% | 11% | 13% | 8–26% |
| 6.Editorial Independence | Ensures that the formulation of recommendations is not unduly biased with competing interests. (Item 22–23). | 0% | 0% | 0% | 0% | 0% | 0% |
| Overall Quality Assessment Score | Overall quality of the CPG, considering all items from the assessment process. | 4 | 5 | 2 | 2 | ||
| Recommended for Use in Clinical Practice | No. | Yes, with | No. | No. | |||
| modifications |
CPG, clinical practice guideline. SPA, Speech Pathology Australia. RCSLT, The Royal College of Speech and Language Therapists. NZSTA, The New Zealand Speech-Language Therapists’ Association. ASHA, American Speech-Language-Hearing Association.
Fig. 2
AGREE-II domain scores across the appraised clinical practice guidelines.
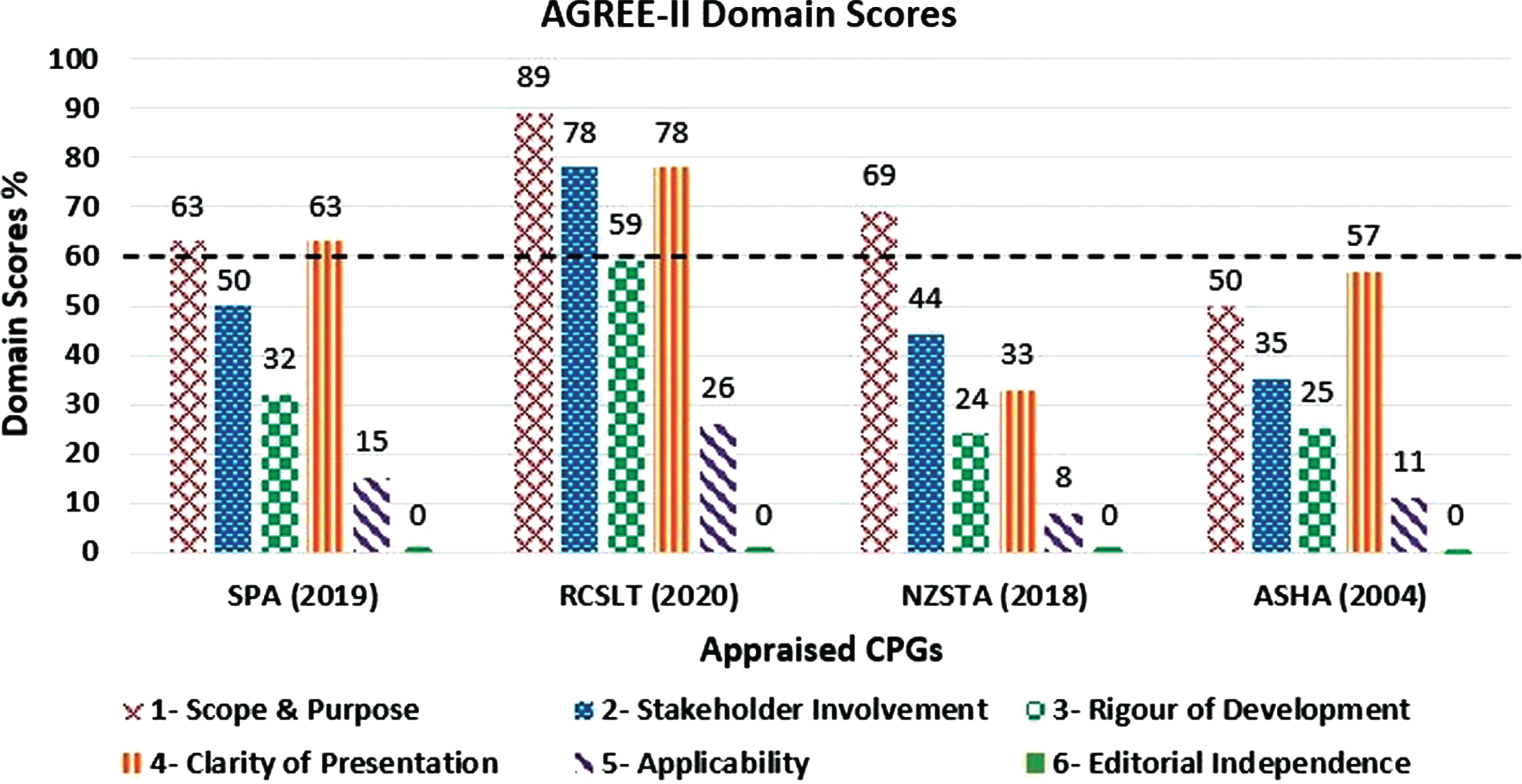
The highest median domain score (66%) was achieved in domain 1 “Scope and Purpose”. Three out of four CPGs scored above 60% (range 50–89%) in this domain. A median score of 60% or less was achieved in all other domains. However, two out of four CPGs scored above 60% in domain 4 “Clarity of Presentation” (median 60%; range 33–78%). In domain 2 “Stakeholder Involvement”, one CPG scored above 60% (median 47%; range 35–78%).
No CPG achieved a score above 60% in the following domains: “Rigour of development” (median 29%; range 24–59%), “Applicability” (median 13%; range 8–26%), and “Editorial Independence” (median 0%; range 0%). All median scores in these domains were below 30%.
3.3Overall assessment
The overall assessment was rated on a Likert scale of 1–7, considering the CPGs quality over the various domains. Table 2 states whether the CPG was recommended for use in clinical practice based on these scores. A CPG was considered to be “recommended for clinical practice” if a score of 60% was achieved in at least 4 domains. CPGs were “recommended with modifications” if a score of 60% was achieved in three domains. CPGs were “not recommended for use in clinical practice” if at least four domains scored less than 60%.
3.4Appraiser’s consistency
The ICCs calculated for all CPGs were above 0.90, indicating excellent inter-rater reliability, as displayed in Table 3. These scores demonstrate strong agreement and little variation between appraisers’ scores across CPGs (O’Donnell, Allison, Melikian, & Iafrati, 2020).
Table 3
Inter-rater reliability for appraisal of clinical practice guidelines
| CPG | Intraclass Correlation | 95% Confidence |
| (year published) | Coefficient | Interval |
| SPA (2019) | 0.983 | 0.965 – 0.992 |
| RSCLT (2020) | 0.943 | 0.886 – 0.974 |
| NZSTA (2018) | 0.960 | 0.920 – 0.982 |
| ASHA (2004) | 0.966 | 0.932 – 0.984 |
CPG, clinical practice guideline. SPA, Speech Pathology Australia. RCSLT, The Royal College of Speech and Language Therapists. NZSTA, The New Zealand Speech-Language Therapists’ Association. ASHA, American Speech-Language-Hearing Association.
4Discussion
4.1Main findings
To the authors’ knowledge, this is the first study to systematically appraise the quality of FEES CPGs. Study findings were consistent with the original hypothesis, conveying the scarcity of FEES CPGs worldwide and their inferior quality. The majority of CPGs omitted relevant detail within their recommendations or the development process. Based on the critical appraisal using the AGREE-II instrument, none of the included CPGs are recommended for use in clinical practice. However, one CPG by RCSLT, was recommended for use with modifications, based on the domain scores achieved. Standardisation of FEES CPGs is urgently required to provide reliable and high-quality care to service users. Authors acknowledge that other multi-disciplinary team (MDT) members such as ENT specialists, otolaryngologists, or neurologists may carry out FEES. This review was focused solely on CPGs for SLTs carrying out the procedure.
4.2Variance among CPG characteristics
Information regarding the development process, search strategies or included evidence to support recommendations was not sufficiently included in the evaluated CPGs. Details were omitted regarding grading systems used to rate their evidence, service user involvement in the development process or the inclusion of an external review by an expert team. The above characteristics are considered crucial features required to develop a document of evidence-based recommendations with a transparent methodology (Zafra-Tanaka et al., 2019).
CPG development processes varied widely. No CPG included a systematic review of the evidence or discussed any methodology by which they reached their recommendations, with the exception of RCSLT’s CPG, including a brief discussion only. Similarly, service user and MDT involvement were solely mentioned in RCSLT’s CPG, but not sufficiently discussed. Given that CPGs are developed to optimise patient care, it is indispensable that service users are consulted during the guideline development process to promote implementation of CPGs in a way that service users deem advantageous (Armstrong, Mullins, Gronseth, & Gagliardi, 2018).
Recommendations were often provided in the form of generalised statements, without a clearly stated rationale or supporting evidence, which reduces the recommendations’ applicability. Recommendations should have a key action statement, elaborated by text, evidence and strength of recommendation ratings (Institute of Medicine, 2011). Whilst only one CPG graded their practice statements, most were graded as “GP”, abbreviated for “good practice based on clinical experience and expert opinion” rather than trusted evidence, which would be graded as “A”. (SPA, 2019). No recommendation was graded as trusted evidence and 26 out of 32 recommendations made in the CPG were given the grading “GP”. This could imply that these recommendations were graded as “GP” due to the fact that there is limited evidence available to support the recommendation, and thus developers are relying more on clinical practice and expert opinion. Additionally, ambiguity in recommendations can signify a limited evidence base (Institute of Medicine, 2011). Further high-quality research in areas of dysphagia assessment may be beneficial to ensure that recommendations can be supported by appropriate evidence, in addition to expert opinions, in order for superior CPGs to be produced. (Koidou, Kollias, Sdravou, & Grouios, 2013; Plowman, Mehdizadeh, Leder, Martino, & Belafsky, 2013).
4.3Limited CPG quality
The AGREE-II critical appraisal concluded that no CPG is suitable for use in clinical practice without modifications. The most recently published CPG by RCSLT, was recommended for use in clinical practice with modifications, achieving an overall quality score of 5. However, even this CPG scored inadequately in certain domains (“Rigour of development”, “Applicability”, “Editorial Independence”).
Higher scoring domains across the appraised CPGs included “Scope and Purpose” and “Clarity of Presentation”. Some adequate scores in these domains indicates effective reporting of the objective, target population and specific health question, as well as a clear structure and format within the CPG. Only one CPG scored adequately in Domain 2 “Stakeholder Involvement”, meaning that all other CPGs did not include relevant patient, carer or professional involvement in the development process.
All median domain scores in “Rigour of Development”, “Applicability” and “Editorial Independence” were below 30%, indicating very poor quality. These scores depict an absence of systematic methods used to develop and update recommendations, as well as a critical evaluation of the evidence supporting the recommendations. These scores also reflect a lack of advice to put the recommendation into practice, discussion of the resource implications in doing so, and an omission of declarations of competing interests or statements relating to the funding bodies.
“Rigour of development” is the largest domain of the AGREE-II instrument and plausibly one of the most important domains in the assessment (Amer et al., 2019; Zafra-Tanaka et al., 2019). It is therefore concerning that three of the four CPGs scored very poorly in this domain (below 30%), due to a lack of transparent and robust methodology.
4.4Comparison to existing research
Findings relating to the quality of FEES CPGs can be compared to VFSS CPGs, researched by Boaden and colleagues (2020). Figure 3 highlights that areas of strength and downfall exist in the same domains of the AGREE-II for FEES and VFSS CPGs. Considerations can therefore be made regarding improvements in guideline formulation and quality with particular focus on the lower scoring domains displayed in Fig. 3.
Fig. 3
Trend in median domain scores of AGREE-II in FEES vs VFSS CPGs. Blue represents the median domain scores for FEES CPGs. Orange represents the median domain scores for VFSS CPGs. VFSS data adapted from Boaden et al., 2020.
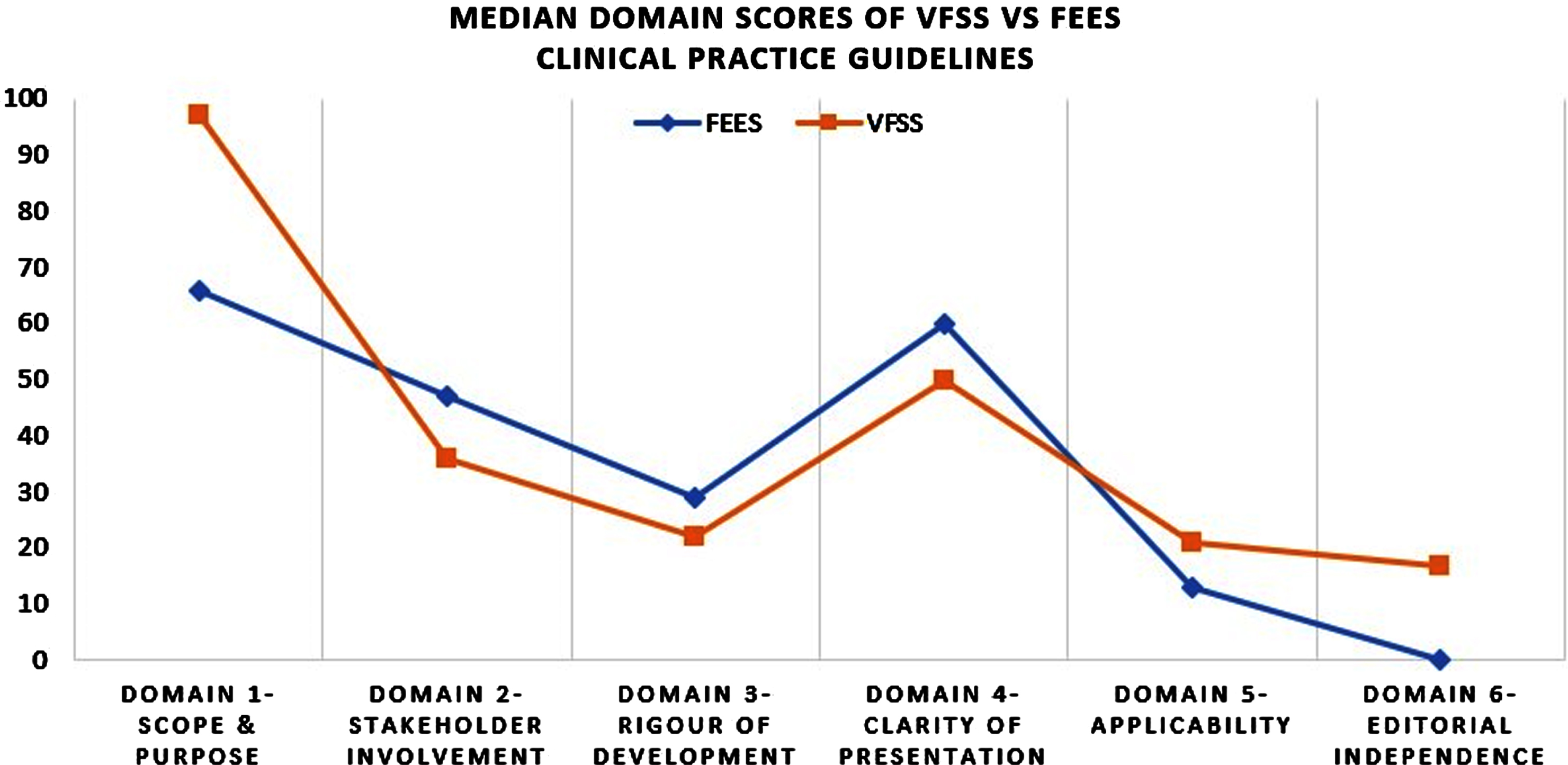
The lowest scoring domains for both VFSS and FEES were the following: “Rigour of Development”, “Applicability” and “Editorial Independence” respectively, whereby no CPG scored above the 60% threshold in either study. With a lack of focus on these domains, CPGs are omitting crucial steps in formulating recommendations using systematic methods and high-quality evidence and reducing the ability for clinicians to apply the CPGs to practice. They are also failing to state competing interests or information regarding funding bodies.
Lower scores in these domains have been noted across healthcare disciplines, including CPGs for the treatment of tic disorders, depression in adults and chronic kidney disease (Boaden et al., 2020; Coronado Daza, Vernooij, Salas, Osorio, & Urrútia Cuchí, 2019; Yang et al., 2018; Zafra-Tanaka et al., 2019).
4.5Clinical implications
This study’s findings carry clinical significance as it highlights the gaps that exist in the provision of optimum patient care. Prior to this study there was limited information surrounding the nature of FEES CPGs, a resource frequently adopted to guide numerous assessment and management plans for SLTs worldwide. As the primary role of CPGs is to promote evidence-based practice, poor-quality CPGs are potentially detrimental to patient outcomes.
As the demand for FEES is growing and will continue to increase as the prevalence of dysphagia rises (Adkins et al., 2020; Madhavan, Lagorio, Crary, Dahl, & Carnaby, 2016; Smithard, 2018), these findings are crucial to allow clinicians to make decisions about their use of CPGs in practice. This research portrays the nature and quality of such resources and the need for additional CPG development.
4.6Limitations and future directions
The authors acknowledge certain limitations. Given the broad definition of CPGs employed in this study, it could be argued that some included documents should not be measured using the AGREE-II tool. However, each of the documents included were developed with the intention to guide clinical practice and are the source of guidance for SLTs carrying out FEES procedures. Additionally, similar broad definitions have been used in other CPG research (Boaden et al., 2020).
All CPGs included were published in English. Findings did not capture CPGs that were published in other languages. Quality ratings were based on authors’ reports of the completion of certain steps within the development process. For example, if CPG developers did not report the systematic methods used to formulate recommendations, a transparent methodology is not evident and a lower score will be assigned to that item.
The ‘overall guidelines assessment’ at the end of each AGREE-II assessment requires the reviewer to assign a score between one and seven of the overall CPG quality based on the scored domains. Whilst there were no large disagreements on this item between reviewers, the authors found this section somewhat subjective with no outlined criteria to designate a score. Additionally, whilst the AGREE-II provides explicit criteria allowing the authors to effectively evaluate the quality of CPGs, the involvement of an epidemiologist with expertise in CPG development would have added value to the critical analysis of the international CPGs included in this study.
In order for direct improvements to be made to FEES CPGs, particular focus needs to be placed on the following measures: including systematic methods within the development process; incorporating service users and other relevant stakeholders’ views and preferences in the development process; the provision of advice and tools to put the recommendations into practice; and statements regarding the views of funding bodies and competing interests.
Any future FEES CPG developers should be advised to closely follow the AGREE-II reporting checklist outlined by Brouwers and colleagues (2016), as one of its primary functions is to guide CPG development. By doing so, all necessary components of high-quality and standardised CPGs can be formulated efficiently. Particular focus on the aforementioned lower scoring domains (“Rigour of development”, “Applicability” and “Editorial Independence”) in FEES CPGs will assist developers to overcome common errors and omissions. Future developers should also be advised to ensure all steps within the development process are reported within the CPG. This study’s findings convey that an omission of this information often leads to an inadequate quality score in some domains.
5Conclusion
This study highlights the scarcity of comprehensive FEES CPGs available for dysphagia clinicians to refer to in clinical practice internationally. Up-to-date and evidence-based CPGs for FEES are urgently required to provide clinicians with sufficient guidance and patients with optimum care. Findings from this study can serve as a basis for future research and the development of additional FEES CPGs, by highlighting important areas requiring improvement, in order to promote patient safety and enhance clinical practice.
Acknowledgments
With thanks to Isolde Harpur, Faculty Librarian, Trinity College Dublin, for her assistance in reviewing the database searches.
Conflict of interest
The authors declare no conflicts of interest. Given her role as co-Editor-in-Chief, Julie Regan had no involvement in the peer review of this article.
References
[1] | Adkins, C. , Takakura, W. , Spiegel, B.M.R. , Lu, M. , Vera-Llonch, M. , Williams, J. , … Almario, C.V. ((2020) ) Prevalence and characteristics of dysphagia based on a population-based survey. Clinical Gastroenterology and Hepatology, 18: ((9)), 1970–e1972. https://doi.org/https://doi.org/10.1016/j.cgh.2019.10.029 |
[2] | Amer, Y.S. , Al-Joudi, H.F. , Varnham, J.L. , Bashiri, F.A. , Hamad, M.H. , Al Salehi, S.M. , … Albatti, T.K. ((2019) ) Appraisal of clinical practice guidelines for the management of attention deficit hyperactivity disorder (ADHD) using the AGREE II Instrument: A systematic review. PloS One, 14: ((7)), e0219239https://doi.org/10.1371/journal.pone.0219239 |
[3] | Andrade, R. , Pereira, R. , van Cingel, R. , Staal, J.B. , … Espregueira-Mendes, J. ((2020) ) How should clinicians rehabilitate patients after ACL reconstruction? A systematic review of clinical practice guidelines (CPGs) with a focus on quality appraisal (AGREE II). British Journal of Sports Medicine, 54: ((9)), 512–519. https://doi.org/10.1136/bjsports-2018-100310 |
[4] | Armstrong, M.J. , Mullins, C.D. , Gronseth, G.S. , … Gagliardi, A.R. ((2018) ) Impact of patient involvement on clinical practice guideline development: A parallel group study. Implementation Science, 13: ((1)), 55. https://doi.org/10.1186/s13012-018-0745-6 |
[5] | American Speech-Language-Hearing Association (ASHA).. ((2004) ) Role of the speech-language pathologist in the performance and interpretation of endoscopic evaluation of swallowing: Guidelines. Retrieved from Role of the Speech-Language Pathologist in the Performance and Interpretation of Endoscopic Evaluation of Swallowing_ Guidelines (1).pdf. |
[6] | Baijens, L.W. , Speyer, R. , Pilz, W. , … Roodenburg, N. ((2014) ) FEES protocol derived estimates of sensitivity: Aspiration in dysphagic patients. Dysphagia, 29: ((5)), 583–590. https://doi.org/10.1007/s00455-014-9549-2 |
[7] | Black, A.T. , Balneaves, L.G. , Garossino, C. , Puyat, J.H. , … Qian, H. ((2015) ) Promoting evidence-based practice through a research training program for point-of-care clinicians. The Journal of Nursing Administration, 45: ((1)), 14–20. https://doi.org/10.1097/NNA.0000000000000151 |
[8] | Boaden, E. , Nightingale, J. , Bradbury, C. , Hives, L. , … Georgiou, R. ((2020) ) Clinical practice guidelines for videofluoroscopic swallowing studies: A systematic review. Radiography (Lond), 26: ((2)), 154–162. https://doi.org/10.1016/j.radi.2019.10.011 |
[9] | Brouwers, M.C. , Kerkvliet, K. , … Spithoff, K. ((2016) ) The AGREE Reporting Checklist: A tool to improve reporting of clinical practice guidelines. BMJ, 352: , i1152. https://doi.org/10.1136/bmj.i1152 |
[10] | Brouwers, M.C. , Kho, M.E. , Browman, G.P. , Burgers, J.S. , Cluzeau, F. , Feder, G. ..., … Zitzelsberger, L. ((2010) ) AGREE II: Advancing guideline development, reporting and evaluation in health care. Canadian Medical Association Journal, 182: ((18)), E839–E842. https://doi.org/10.1503/cmaj.090449 |
[11] | Chong, C. ((2018) ) Pros and cons of clinical practice based on guidelines. Hong Kong Medical Journal=Xianggang Yi Xue Za Zhi, 24: ((5)), 440–441. https://doi.org/10.1503/cmaj.090449 |
[12] | Coronado Daza, J. , Vernooij, R.W.M. , Salas, K. , Osorio, D. , … Urrútia Cuchí, G. ((2019) ) Quality assessment of clinical practice guidelines for chronic kidney disease: A systematic review. BMC Nephrology, 20: ((1)), 192. https://doi.org/10.1186/s12882-019-1387-x |
[13] | Curtis, J.A. , Borders, J.C. , Perry, S.E. , Dakin, A.E. , Seikaly, Z.N. , … Troche, M.S. ((2021) ) Visual analysis of swallowing efficiency and safety (VASES): A standardized approach to rating pharyngeal residue, penetration, and aspiration during FEES. Dysphagia, 1–19. https://doi.org/10.1007/s00455-021-10293-5 |
[14] | Dziewas, R. , auf dem Brinke, M. , Birkmann, U. , Bräuer, G. , Busch, K. , Cerra, F. , … Warnecke, T. ((2019) ) Safety and clinical impact of FEES – results of the FEES-registry. Neurological Research and Practice, 1: ((1)), 16. https://doi.org/10.1186/s42466-019-0021-5 |
[15] | Dziewas, R. , Baijens, L. , Schindler, A. , Verin, E. , Michou, E. , … Clave, P. , European Society for Swallowing, Disorders.. ((2017) ) European society for swallowing disorders FEES accreditation program for neurogenic and geriatric oropharyngeal dysphagia. Dysphagia, 32: ((6)), 725–733. https://doi.org/10.1007/s00455-017-9828-9 |
[16] | Dziewas, R. , Glahn, J. , Helfer, C. , Ickenstein, G. , Keller, J. , Lapa, S. , … Busse, O. ((2014) ) FEES für neurogene dysphagien. Der Nervenarzt, 85: ((8)), 1006–1015. https://doi.org/10.1007/s00115-014-4114-7 |
[17] | Fuller, S.C. , Leonard, R. , Aminpour, S. , … Belafsky, P.C. ((2009) ) Validation of the pharyngeal squeeze maneuver. Otolaryngology and Head and Neck Surgery, 140: ((3)), 391–394. https://doi.org/10.1016/j.otohns.2008.12.015 |
[18] | Gillespie, B.M. , Bull, C. , Walker, R. , Lin, F. , Roberts, S. , … Chaboyer, W. ((2018) ) Quality appraisal of clinical guidelines for surgical site infection prevention: A systematic review. PloS One, 13: ((9)), e0203354. https://doi.org/10.1371/journal.pone.0203354 |
[19] | Hurkmans, E.J. , Jones, A. , Li, L.C. , … Vliet Vlieland, T.P.M. ((2011) ) Quality appraisal of clinical practice guidelines on the use of physiotherapy in rheumatoid arthritis: A systematic review. Rheumatology, 50: ((10)), 1879–1888 https://doi.org/10.1093/rheumatology/ker195. |
[20] | Institute of Medicine. ((2011) ) Institute of Medicine Committee on Standards for Developing Trustworthy Clinical Practice, Guidelines. In Graham, R. Mancher, M. , Miller Wolman, D. , Greenfield, S , & Steinberg, E. (Eds.), Clinical Practice Guidelines We Can Trust. Washington (DC): National Academies Press (US) https://doi.org/10.17226/13058 |
[21] | Johnston, A. , Hsieh, S.C. , Carrier, M. , Kelly, S.E. , Bai, Z. , Skidmore, B. , … Wells, G.A. ((2018) ) A systematic review of clinical practice guidelines on the use of low molecular weight heparin and fondaparinux for the treatment and prevention of venous thromboembolism: Implications for research and policy decision-making. PloS One, 13: ((11)), e0207410. https://doi.org/10.1371/journal.pone.0207410 |
[22] | Kaneoka, A. , Krisciunas, G.P. , Walsh, K. , Raade, A.S. , … Langmore, S.E. ((2015) ) A comparison of 2 methods of endoscopic laryngeal sensory testing: A preliminary study. Annals of Otology, Rhinology and Laryngology, 124: ((3)), 187–193. https://doi.org/10.1177/0003489414550241 |
[23] | Koidou, I. , Kollias, N. , Sdravou, K. , … Grouios, G. ((2013) ) Dysphagia: A short review of the current state. Educational Gerontology, 39: ((11)), 812–827. https://doi.org/10.1080/03601277.2013.766518 |
[24] | Kredo, T. , Bernhardsson, S. , Machingaidze, S. , Young, T. , Louw, Q. , Ochodo, E. , … Grimmer, K. ((2016) ) Guide to clinical practice guidelines: the current state of play. International Journal for Quality in Health Care, 28: ((1)), 122–128. https://doi.org/10.1093/intqhc/mzv115 |
[25] | Langmore, S.E. ((2017) ) History of fiberoptic endoscopic evaluation of swallowing for evaluation and management of pharyngeal dysphagia: Changes over the years. Dysphagia, 32: ((1)), 27–38. https://doi.org/10.1007/s00455-016-9775-x |
[26] | Langmore, S.E. , Schatz, K. , … Olsen, N. ((1988) ) Fiberoptic endoscopic examination of swallowing safety: A new procedure. Dysphagia, 2: ((4)), 216–219. https://doi.org/10.1007/bf02414429 |
[27] | Lin, I. , Wiles, L. , Waller, R. , Goucke, R. , Nagree, Y. , Gibberd, M. , … O’Sullivan, P.P.B. ((2020) ) What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. British Journal of Sports Medicine, 54: ((2)), 79. https://doi.org/10.1136/bjsports-2018-099878 |
[28] | Lucendo, A.J. , Molina-Infante, J. , Arias, Á. , von Arnim, U. , Bredenoord, A.J. , Bussmann, C. , … Attwood, S.E. ((2017) ) Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterology Journal, 5: ((3)), 335–358. https://doi.org/10.1177/2050640616689525 |
[29] | Madhavan, A. , Lagorio, L.A. , Crary, M.A. , Dahl, W.J. , … Carnaby, G.D. ((2016) ) Prevalence of and risk factors for dysphagia in the community dwelling elderly: A systematic review. The Journal of Nutrition, Health … Aging, 20: ((8)), 806–815. https://doi.org/10.1007/s12603-016-0712-3 |
[30] | Miller, C.K. , Schroeder J.W. Jr. , … Langmore, S. ((2020) ) Fiberoptic endoscopic evaluation of swallowing across the age spectrum. American Journal of Speech-Language Pathology, 29: ((2S)), 967–978. https://doi.org/10.1044/2019_AJSLP-19-00072. |
[31] | National Health and Medical Research Council in Australia (NHMRC). ((2009) ) Guidelines. Retrieved from https://www.nhmrc.gov.au/health-advice/guidelines |
[32] | The New Zealand Speech-language Therapists’ Association (NZSTA). ((2018) ) Flexible Endoscopic Evaluation of Swallowing (FEES) in adults and children in New Zealand. [Practice Standards]. Retrieved from https://speechtherapy.org.nz/wp-content/uploads/2018/06/NZSTA-Practise-standards_FEES-final.pdf |
[33] | O’Donnell, T.F. , Allison, G.M. , Melikian, R. , … Iafrati, M.D. ((2020) ) A systematic review of the quality of clinical practice guidelines for lymphedema, as assessed using the Appraisal of Guidelines for Research and Evaluation II instrument. Journal of Vascular Surgery: Venous and Lymphatic Disorders, 8: ((4)), 685–692. https://doi.org/https://doi.org/10.1016/j.jvsv.2020.04.008 |
[34] | Pisegna, J.M. , Kaneoka, A. , Leonard, R. , … Langmore, S.E. ((2018) ) Rethinking residue: Determining the perceptual continuum of residue on FEES to enable better measurement. Dysphagia, 33: ((1)), 100–108. https://doi.org/10.1007/s00455-017-9838-7 |
[35] | Plowman, E.K. , Mehdizadeh, O. , Leder, S.B. , Martino, R. , … Belafsky, P.C. ((2013) ) A bibliometric review of published abstracts presented at the dysphagia research society. Dysphagia, 28: ((2)), 123–130. https://doi.org/10.1007/s00455-012-9420-2 |
[36] | Quintyne, K.I. , … Kavanagh, P. ((2019) ) Appraisal of international guidelines on smoking cessation using the AGREE II assessment tool. Irish Medical Journal, 112: ((2)), 867. |
[37] | Sekercioglu, N. , Al-Khalifah, R. , Ewusie, J.E. , Elias, R.M. , Thabane, L. , Busse, J.W. , … Guyatt, G.H. ((2017) ) A critical appraisal of chronic kidney disease mineral and bone disorders clinical practice guidelines using the AGREE II instrument. International Urology and Nephrology, 49: ((2)), 273–284. https://doi.org/10.1007/s11255-016-1436-3 |
[38] | Smithard, D.G. ((2018) ) Dysphagia: A growing concern? A personal view. Gastroenterology & Hepatology: Open Access, 9: ((4)), 142–144. https://doi.org/https://doi.org/10.15406/ghoa.2018.09.00313 |
[39] | Speech Pathology Association of Australia Limited (SPA). ((2019) ) Flexible Endoscopic Evaluation of Swallowing (FEES). Clinical guideline. Retrieved from https://www.speechpathologyaustralia.org.au/SPAweb/Members/Clinical_Guidelines/spaweb/Members/Clinical_Guidelines/Clinical_Guidelines.aspx |
[40] | Wallace, S. , McLaughlin, C. , Clayton, J. , Coffey, M. , Ellis, J. , Haag, R. , Howard, A. , Marks, H. , … Zorko, R. ((2020) ) Fibreoptic Endoscopic evaluation of Swallowing (FEES): The Role of Speech and Language Therapy. London: Royal College of Speech and Language Therapists, Position Paper. Retrieved from https://www.rcslt.org/wp-content/uploads/media/RCSLT_FEES-Position-paper.pdf?la=en…hash=652C2876A5C13FF034A5068D08760652276EF257 |
[41] | Warnecke, T. , Ritter, M.A. , Kroger, B. , Oelenberg, S. , Teismann, I. , Heuschmann, P.U. , … Dziewas, R. ((2009) ) Fiberoptic endoscopic Dysphagia severity scale predicts outcome after acute stroke. Cerebrovascular Diseases, 28: ((3)), 283–289. https://doi.org/10.1159/000228711 |
[42] | Yang, C. , Zhang, Z. , Zhang, L. , Tian, J. , Yu, D. , Wang, J. , … Yang, J. ((2018) ) Quality assessment of clinical practice guidelines on tic disorders with AGREE II instrument. Psychiatry Research, 259: , 385–391. https://doi.org/https://doi.org/10.1016/j.psychres.2017.08.060 |
[43] | Zafra-Tanaka, J.H. , Goicochea-Lugo, S. , Villarreal-Zegarra, D. , … Taype-Rondan, A. ((2019) ) Characteristics and quality of clinical practice guidelines for depression in adults: a scoping review. BMC Psychiatry, 19: ((1)), 76. https://doi.org/10.1186/s12888-019-2057-z |
Appendices
Appendix -
Search Strategies for CPGs for FEES
| Source | Link | Search terms used |
| Pubmed (Medline) | https://pubmed.ncbi.nlm.nih.gov/ | (“practice standard*”[Title/Abstract] OR “practice guideline*”[Title/Abstract] OR “clinical guideline*”[Title/Abstract] OR “clinical protocol*”[Title/Abstract] OR “clinical polic*”[Title/Abstract] OR “clinical pathway*”[Title/Abstract] OR “critical pathway*”[Title/Abstract] OR guideline[Title/Abstract] OR “Clinical Protocols”[Mesh] OR “Critical Pathways”[Mesh] OR “Practice Guidelines as Topic”[Mesh] OR “Practice Guideline” [Publication Type]) AND (“Endoscopy”[Mesh] OR “Fiber Optic Technology”[Mesh] OR nasendoscop*[Title/Abstract] OR endoscop*[Title/Abstract] OR “fiber optic technology”[Title/Abstract] OR “endoscopic evaluation of swallowing”[Title/Abstract] OR “flexible endoscopic evaluation of swallowing”[Title/Abstract] OR “fibreoptic endoscopic evaluation of swallowing”[Title/Abstract] OR “fiberoptic endoscopic evaluation of swallowing”[Title/Abstract] OR “FEES”[Title/Abstract]) AND (Deglutition[Title/Abstract] OR “deglutition disorder*”[Title/Abstract] OR swallow*[Title/Abstract] OR dysphagi*[Title/Abstract] OR “Deglutition”[Mesh] OR “Deglutition Disorders”[Mesh]) |
| Cinahl, Prospero | https://www.ebsco.com/products/research-databases/cinahl-complete https://www.crd.york.ac.uk/prospero/ | (“practice standard*”[Title/Abstract] OR “practice guideline*”[Title/Abstract] OR “clinical guideline*”[Title/Abstract] OR “clinical protocol*”[Title/Abstract] OR “clinical polic*”[Title/Abstract] OR “clinical pathway*”[Title/Abstract] OR “critical pathway*”[Title/Abstract] OR guideline[Title/Abstract] OR “Clinical Protocols”[Mesh] OR “Critical Pathways”[Mesh] OR “Practice Guidelines as Topic”[Mesh] OR “Practice Guideline” [Publication Type]) AND (“Endoscopy”[Mesh] OR “Fiber Optic Technology”[Mesh] OR nasendoscop*[Title/Abstract] OR endoscop*[Title/Abstract] OR “fiber optic technology”[Title/Abstract] OR “endoscopic evaluation of swallowing”[Title/Abstract] OR “flexible endoscopic evaluation of swallowing”[Title/Abstract] OR “fibreoptic endoscopic evaluation of swallowing”[Title/Abstract] OR “fiberoptic endoscopic evaluation of swallowing”[Title/Abstract] OR “FEES”[Title/Abstract]) AND (Deglutition[Title/Abstract] OR “deglutition disorder*”[Title/Abstract] OR swallow*[Title/Abstract] OR dysphagi*[Title/Abstract] OR “Deglutition”[Mesh] OR “Deglutition Disorders”[Mesh]) (Exclude Medline). |
| Embase (Scopus) | https://www.embase.com/login | (’dysphagia’/exp OR ‘swallowing’/exp OR dysphagi*:ab,ti OR swallow*:ab,ti OR deglutition:ab,ti OR ‘deglutition disorder*’:ab,ti) AND (’nasendoscope’/exp OR ‘endoscopy’/exp OR ‘fiber optics’/exp OR ‘fiberoptic endoscopic evaluation of swallowing’/exp OR ‘flexible endoscopic evaluation of swallowing’/exp OR nasendoscop*:ab,ti OR endoscop*:ab,ti OR ‘fiber optics’:ab,ti OR ‘endoscopic evaluation of swallowing’:ab,ti OR ‘flexible endoscopic evaluation of swallowing’:ab,ti OR ‘fibreoptic endoscopic evaluation of swallowing’:ab,ti OR ‘fiberoptic endoscopic evaluation of swallowing’:ab,ti OR ‘fees’:ab,ti) AND (’practice guideline’/exp OR ‘clinical protocol’/exp OR ‘clinical pathway’/exp OR ‘practice guideline’:ab,ti OR ‘practice standard*’:ab,ti OR ‘clinical guideline*’:ab,ti OR ‘clinical protocol*’:ab,ti OR ‘clinical polic*’:ab,ti OR ‘clinical pathway*’:ab,ti OR ‘critical pathway*’:ab,ti OR ‘guideline’:ab,ti) AND [embase]/lim NOT ([embase]/lim AND [medline]/lim) |
| Web of Science | https://login.webofknowledge.com/ | TOPIC: (Deglutition OR “deglutition disorder*” OR swallow* OR dysphagi*) AND (nasendoscop* OR endoscop* OR “fiber optic technology” OR “endoscopic evaluation of swallowing” OR “flexible endoscopic evaluation of swallowing” OR “fibreoptic endoscopic evaluation of swallowing” OR “fiberoptic endoscopic evaluation of swallowing” OR “FEES”) AND (“practice standard*” OR “practice guideline*” OR “clinical guideline*” OR “clinical protocol*” OR “clinical polic*” OR “clinical pathway*” OR “critical pathway*” OR guideline) |
| NICE Guidance | https://www.nice.org.uk/guidance | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| Royal College of Speech &Language Therapists | https://www.rcslt.org/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| Speech Pathology Australia | https://www.speechpathologyaustralia.org.au/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| American Board of Swallowing and Swallowing Disorders | https://www.swallowingdisorders.org/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| American Speech-Language-Hearing Association | https://www.asha.org/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| New Zealand Speech-Language Therapists’ Association | https://speechtherapy.org.nz/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| Dysphagia Research Society | https://www.dysphagiaresearch.org/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| Japanese Society of Dysphagia Rehabilitation | https://www.jsdr.or.jp/english/english_about.html | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| European Society for Swallowing Disorders | http://www.myessd.org/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| Hong Kong Association of Speech Therapists | https://www.speechtherapy.org.hk/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” |
| Google Search | https://www.google.com/ | “Flexible endoscopic evaluation of swallowing” OR “Fiberoptic endoscopic evaluation of swallowing” OR practice guidelines OR practice standards (first 10 hits). |


